
Modeling Subcutaneous Microchip Implant Acceptance in the General Population: A Cross-Sectional Survey about Concerns and Expectations




Abstract
:1. Introduction
2. Literature Review
3. Materials and Methods
3.1. Study
- RQ 1: What are the public’s major concerns about microchip implants?
- RQ 2: How are these concerns represented in various demographics?
- RQ 3: What are the public’s positive expectations (hopes) about microchip implants?
- RQ 4: How are these hopes represented in various demographics?
3.2. Methods
3.3. Survey Design
3.4. Participants
3.5. Data Analysis
4. Results
4.1. RQ 1: Concerns about Microchip Implants
“Invasion of privacy, issues with who controls the microchip, cyber-security concerns, overall creepiness factor.” (White Female, 65–79 years, with medical condition(s), but no disability).
“Unethical use of the microchip by government, business owners and society members. Additionally, right now the microchip seems to have limited capabilities (for example: turning on lights and opening doors). My concern is more would be tracked than is communicated.” (White Female, 30–49 years, no medical condition and no disability).
“My main concern with microchip implants is that the data acquired from the implants could get into the wrong hands and become misused and abused. I think companies would use this data for their own financial gain by exploiting the people who have chips in them. I also think the “big brother” aspect comes into play if the government were to require people to have microchips. I do not think the government should be so heavily involved that they require people to have a device in them that tracks their data, what they are doing, and where they are at all times.” (Asian or Pacific Islander Female, 18–29 years, mo medical condition and no disability).
“I am concerned that microchips will cause heavy dependence on technology and will not allow humans to think naturally. ” (Asian or Pacific Islander Female, 50–64 years, with medical condition(s), but no disability).
“My only concern would be if it had a long-term health risk to you …” (White Female, 50–64 years, with medical condition(s), but no disability).
“Regarding microchip implants my concerns include adverse tissue reactions, …” (White Female, 65–79 years, with no medical condition and no disability).
“Side effects to my immune system. Will my body think it is a foreign substance, fight it and lose? What types of infections can it cause?” (White Female, 30–49 years, with medical condition(s) and disability).
“Does not sound right. Insufficient science. No compelling reason to face its risks.” (African American or Black Female, 18–29 years, with medical condition(s), but no disability).
“There would need to be a lot of trial and error in testing subjects for me to not be concerned about the use of microchips in humans. I believe we would need years and years of observing this practice before something come on the market and people agreed to buy it and use it. Eventually, personal stories from people who have the implant and their pros and cons would be helpful to know.” (White, Female, 30–49 years, no medical condition or disability).
“I fear having anything implanted in my body.” (White Female, 30–49 years, with medical condition(s) and disability).
“… if it is implanted in the brain that could be very scary if something were to go wrong.” (White Female, 18–29 years, with no medical condition and no disability).
“… Also a malfunction could leave me worst off with me not being able to complete many tasks.” (White Female, 18–29 years, with no medical condition and no disability).
“Regarding microchip implants my concerns include… incompatibility with medical equipment such as MRIs, which would prevent me from going through airport scanners or getting diagnostic tests.” (White Female, 65–79 years, with no medical condition and no disability).
“With the implants, the lines get sticky when people start talking about bringing in church and state. While the video just did a quick skip over the two, this topic has been a hotbed in my church for as long as I can remember. The mark of the beast, never let them implant you with anything. I am in my fifties now and have been hearing this at just about any church I have gone to since I was a kid. So why now? With the state of the world that it is, why would I be comfortable now? And as far as the government, the same thing. We have been told, never give them too much power over you. And here we are. My problem is I literally just found out that the pain pump that I have installed is most likely indeed microchipped already. Something I did not particularly feel positively having for myself. ” (White Female, 50–64 years, not reported medical condition, but no disability).
“My only concern would be if it had a long-term health risk to you, or if the cost of it was astronomical.” (White Female, 50–64 years, with medical condition(s), but no disability).
“Who pays for the surgery and what will costs entail?” (White Female, 30–49 years, with medical condition and disability).
“Funding issue: who is funding this research and why; I am aware of the business interests behind medical industry and drug companies. Their priorities are not ethically in the right place. If they need to choose between profit and well-being of the patients, they choose the former.” (White Female, 65–79 years, with medical condition(s), but no disability).
“My concerns are government control, control from business or people in power, being black” (African American or Black Male, 18–29 years, with medical condition(s), but no disability).
“What if Trump or his ilk were president and got the idea to control the vote or other things via microchip.” (White Female, 30–49 years, with medical condition(s), but no disability).
4.2. RQ 2: Prevalence of Identified Concerns in Various Demographics
4.3. RQ 3: Participants’ Positive Expectations (Hopes) Regarding Microchip Implants
“I was diagnosed with cancer last year, if it could monitor certain levels within the body that would be great, also monitoring temperature could be helpful. In addition, getting vaccines or other life-saving medication could be a great use. Hospitals could also download health info immediately if patient is unresponsive. Maybe could also monitor certain chemical levels in the body to give information on patient’s mental health.” (White Female, 50–64 years, with medical condition(s) and disability).
“I would hope to get answers to different health conditions I suffer with, and I would want to be able to better my illnesses or quality of life.” (White Female, 50–64 years, with medical condition(s) and disability).
“That it could help many people, including research communities, understand the human body and psyche better.” (Asian or Pacific Islander Female, 65–79 years, no medical condition or disability).
“… ability to find someone who has been kidnapped or someone with dementia” (White Female, 50–64 years, with medical condition(s) and disability).
“… better control and stop crimes in society.” (White Female, 30–49 years, without any medical condition and disability).
“I hope the information on microchip implants can one day be controlled by the patient and the patient only with a guarantee of no data leaks.” (White Female, 65–79 years, without any medical condition and disability).
“Able to encrypt data and only able to access certain portions for certain reasons.” (White Male, 30–49 years, with medical condition(s) but no disability).
“It could be made in a way where it will be actually part of a body not some foreign object implanted inside.” (Asian or Pacific Islander Male, 18–29 years, without any medical condition and disability).
“With respect to microchip implants, one hope is that if they became an option in the future, that they would enhance performance (physical and mental). However, it could be seen as an unfair advantage to those who do not have one. I also hope that they can be used to improve diseases and conditions in people, if and only if that is what they are used for.” (White Male, 30–49 years, without any medical condition and disability).
“Lots of interesting possibilities for use to enhance one’s innate abilities” (White Female, 30–49 years, with medical condition(s) but no disability).
“I hope that it doesn’t get regulated and mandated by the government because it’s another form of tracking and hindering citizens of privacy.” (African American or Black Male, 18–29 years, without any medical condition and disability).
“To make the implantation easy and temporary with lowering the cost and ensure that it has no negative impact on human life.” (African American or Black Male, 50–64 years, without any medical condition and disability).
“That microchips will be publicly funded or covered by insurance for individuals who would benefit most from the technology (e.g., individuals with disabilities, cancer patients).” (White Female, 30–49 years, with medical condition(s) but no disability).
“That people stand up against it unless it is done to help with severe medical conditions.” (White Female, 50–64 years, with medical condition(s) but no disability).
“That they don’t become widely used.” (White Female, 30–49 years, with medical condition(s) and disability).
4.4. RQ 4: Prevalence of Identified Expectations in Various Demographics
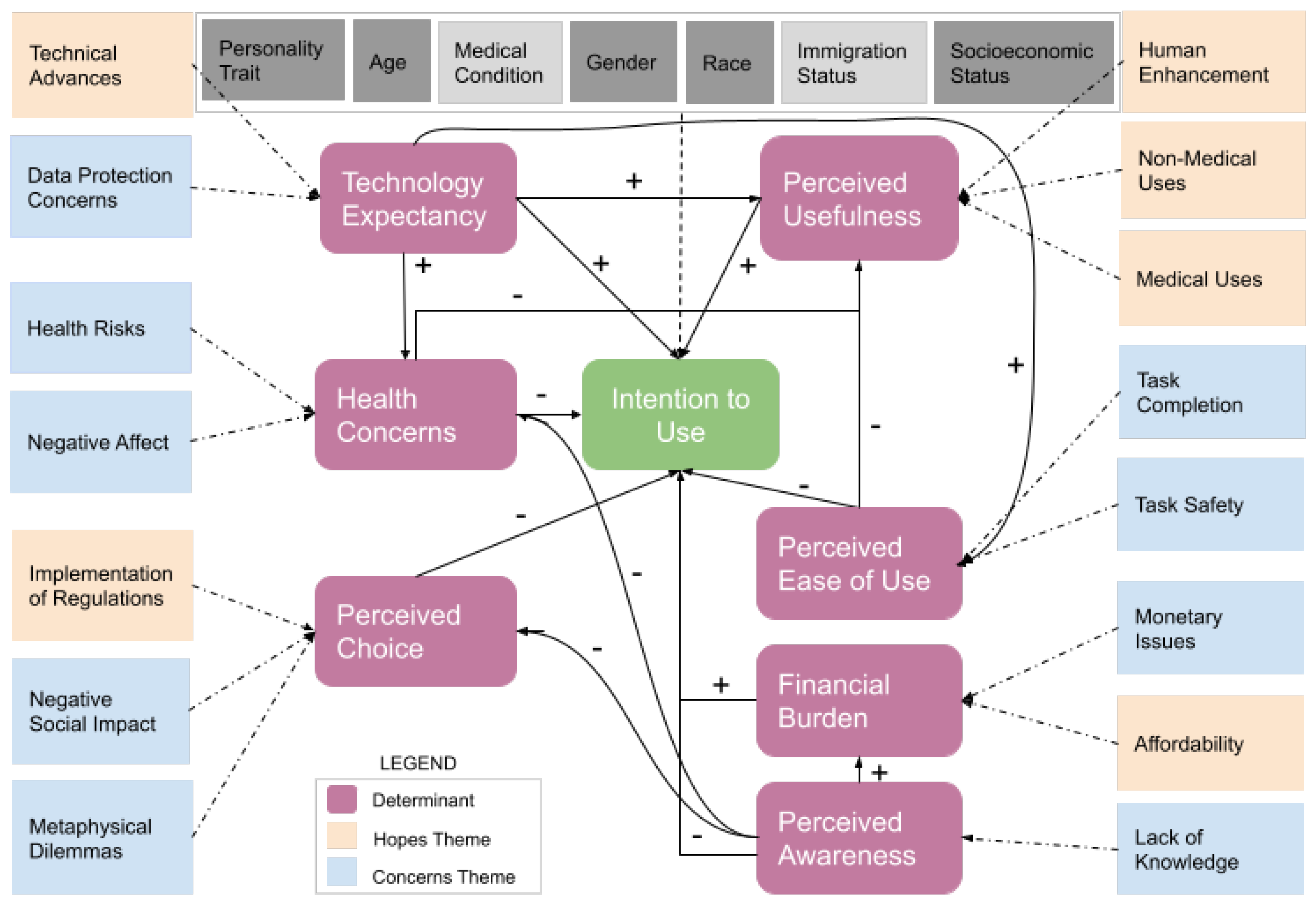
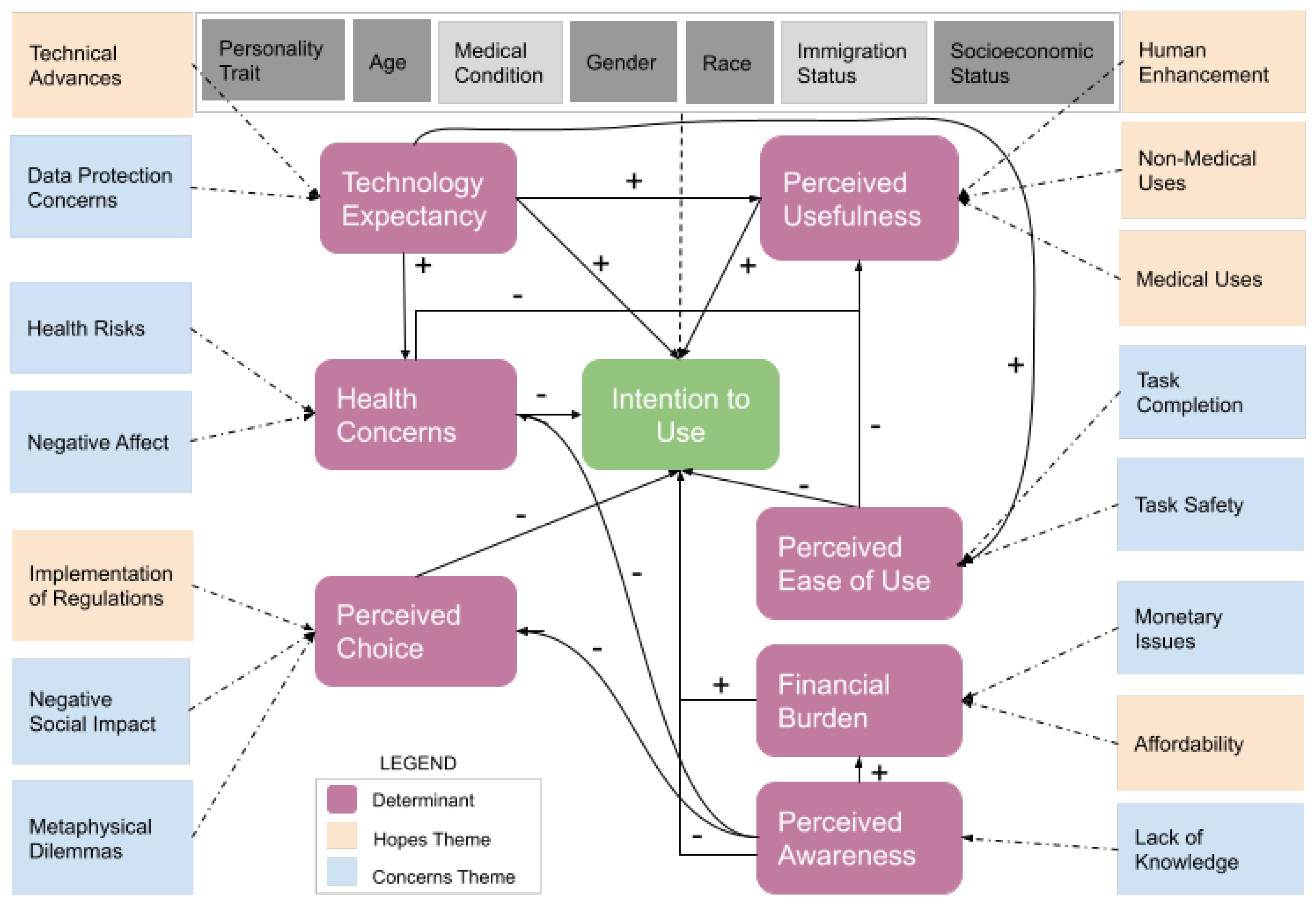
5. Discussion
5.1. Determinants of Acceptance
5.1.1. Perceived Usefulness
5.1.2. Perceived Ease of Use
5.1.3. Technology Expectancy
5.1.4. Health Concerns
5.1.5. Financial Burden
5.1.6. Perceived Awareness
5.1.7. Perceived Choice
5.2. Predictor Variables
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| US | United States |
| RFID | Radio Frequency Identification Device |
| SM | Subcutaneous Microchip |
| NFC | Near Field Communication |
| RQ | Research Question |
| TAM | Technology Acceptance Model |
| GPS | Geographical Positioning System |
| MRI | Magnetic Resonance Imaging |
References
- Nsanze, F. ICT implants in the human body-A review. In The European Group on Ethics in Science and New Technologies to the European Commission; European Communities: Luxembourg, 2005. [Google Scholar]
- Moessner, M. Secure Authentication Scheme for Passive C1G2 RFID Tags. Comput. Netw. 2012, 56, 273–286. [Google Scholar] [CrossRef]
- Microchip Implant (Human)—Wikipedia. Available online: https://en.wikipedia.org/wiki/Microchip_implant_human (accessed on 19 November 2021).
- Is Human Chip Implant Wave of the Future? Available online: http://edition.cnn.com/TECH/computing/9901/14/chipman.idg/ (accessed on 14 January 2022).
- Werber, B. Factors affecting the intentions to use RFID subcutaneous microchip implants for healthcare purposes. Organizacija 2018, 51, 121–133. [Google Scholar] [CrossRef] [Green Version]
- Microchip Developed by Pentagon to Detect Covid-19. Available online: https://nypost.com/2021/04/12/microchip-developed-by-pentagon-to-detect-covid-19/ (accessed on 27 January 2022).
- Carr, N.K. As Society Strives for Reduced Contact During the Pandemic, How Can Human Microchipping Help? Villanova Law Rev. Online 2020, 65, 46. [Google Scholar]
- Tzeng, S.-F.; Chen, W.-H.; Pai, F.-Y. Evaluating the business value of RFID: Evidence from five case studies. Int. J. Prod. Econ. 2008, 112, 601–613. [Google Scholar] [CrossRef]
- Eltorai, A.E.M. Microchips in medicine: Current and future applications. BioMed Res. Int. 2016, 2016, 1743472. [Google Scholar] [CrossRef] [Green Version]
- Perakslis, C.; Michael, K. Indian Millennials: Are microchip implants a more secure technology for identification and access control? In Proceedings of the 2012 IEEE Conference on Technology and Society in Asia, T and SA, Singapore, 27–29 October 2012. [Google Scholar]
- Tech Company Workers Agree to Have Microchips Implanted in Their Hands. Available online: https://abcnews.go.com/Technology/tech-company-workers-agree-microchips-implanted-hands/story?id=48818529 (accessed on 27 January 2022).
- Work 2035: How People and Technology Will Pioneer New Ways of Working. Available online: www.citrix.com/fieldwork/employee-experience/new-ways-of-working-2035.html (accessed on 29 January 2022).
- Michael, K.; Aloudat, A.; Michael, M.G.; Perakslis, C. You Want to Do What with RFID?: Perceptions of radio-frequency identification implants for employee identification in the workplace. IEEE Consum. Electron. Mag. 2017, 6, 111–117. [Google Scholar] [CrossRef]
- Gauttier, Stéphanie, ‘I’ve got you under my skin’–The role of ethical consideration in the (non-) acceptance of insideables in the workplace. Technol. Soc. 2019, 56, 93–108. [CrossRef] [Green Version]
- Michael, K.; Michael, M.G.; Galliot, J.C.; Nicholls, R. Socio-Ethical Implications of Implantable Technologies in the Military Sector. IEEE Technol. Soc. Mag. 2017, 36, 7–9. [Google Scholar] [CrossRef]
- Michael, K. RFID/NFC implants for bitcoin transactions. IEEE Consum. Electron. Mag. 2016, 5, 103–106. [Google Scholar] [CrossRef]
- Half of Brits Expect to Replace Cash with New Technologies, NFC World. August 2015. Available online: http://www.nfcworld.com/2015/08/28/337345/half-of-brits-expect-to-replace-cash-with-newtechnologies/ (accessed on 26 January 2022).
- Richard Gray. The Surprising Truths and Myths about Microchip Implants. 2 August 2017. Available online: https://www.bbc.com/worklife/article/20170731-the-surprising-truths-and-myths-about-microchip-implants (accessed on 27 January 2022).
- Michael, K.; Michael, M.G.; Perakslis, C.; Abbas, R. 5 Überveillance and the Rise of Last-Mile Implantables: Past, Present, and Future. Embodied Comput. Wearables Implant. Embed. Ingestibles 2020, 97. Available online: https://www.katinamichael.com/research/2019/8/1/uberveillance-and-the-rise-of-last-mile-implantables (accessed on 27 January 2022).
- Heffernan, K.J.; Vetere, F.; Chang, S. You put what, where? Hobbyist use of insertable devices. In Proceedings of the 2016 CHI Conference on Human Factors in Computing Systems, San Jose, CA, USA, 7–12 May 2016; pp. 1798–1809. [Google Scholar]
- Khan, N.A. RFIDs chip implants and their related ethical issues. Res. Rep. 2015, unpublished. [Google Scholar] [CrossRef]
- Rotter, P.; Daskala, B.; Compano, R. RFID implants: Opportunities and and challenges for identifying people. IEEE Technol. Soc. Mag. 2008, 27, 24–32. [Google Scholar] [CrossRef]
- Yao, W.; Chu, C.-H.; Li, Z. The adoption and implementation of RFID technologies in healthcare: A literature review. J. Med. Syst. 2012, 36, 3507–3525. [Google Scholar] [CrossRef] [PubMed]
- Niemeijer, A.R. Ethical and practical concerns of surveillance technologies in residential care for people with dementia or intellectual disabilities: An overview of the literature. Int. Psychogeriatr. 2010, 22, 1129–1142. [Google Scholar] [CrossRef]
- Pelegrin-Borondo, J.; Reinares-Lara, E.; Olarte-Pascual, C. Assessing the acceptance of technological implants (the cyborg): Evidences and challenges. Comput. Hum. Behav. 2017, 70, 104–112. [Google Scholar] [CrossRef]
- Fakhr, A. Barriers and Critical Success Factors in Adoption of RFID in Healthcare Sector: Case Studies of Iranian Hospitals. Master’s Thesis, Information Security Luleå University of Technology Department of Computer Science, Electrical and Space Engineering, Lulea, Sweden, 2011. [Google Scholar]
- Wagemakers, S.; van Zoonen, L. Research about Human Chipping. 2013. Available online: http://www.imprintsfutures.org/assets/images/pdfs/ResearchaboutHumanChipping.pdf (accessed on 25 February 2022).
- Bramstedt, K.A. When microchip implants do more than drug delivery: Blending, blurring, and bundling of protected health information and patient monitoring. Technol. Health Care 2005, 13, 193–198. [Google Scholar] [CrossRef]
- Michael, K.; McNamee, A.; Michael, M.G. The emerging ethics of humancentric GPS tracking and monitoring. In Proceedings of the 2006 IEEE International Conference on Mobile Business, Copenhagen, Denmark, 26–27 June 2006; p. 34. [Google Scholar]
- Foster, K.R.; Jaeger, J. Ethical implications of implantable radiofrequency identification (RFID) tags in humans. Am. J. Bioeth. 2008, 8, 44–48. [Google Scholar] [CrossRef]
- Gadzheva, M. Getting chipped: To ban or not to ban. Inf. Commun. Technol. Law 2007, 16, 217–231. [Google Scholar] [CrossRef]
- Masters, A.; Michael, K. Lend me your arms: The use and implications of humancentric RFID. Electron. Commer. Res. Appl. 2007, 6, 29–39. [Google Scholar] [CrossRef] [Green Version]
- Čičević, S.; Samčović, A.; Dragović, M. Factors Affecting RFID Subcutaneous Microchips Usage. In Proceedings of the Sinteza 2019-International Scientific Conference on Information Technology and Data Related Research, Novi Sad, Serbia, 20 April 2019; pp. 235–243. [Google Scholar]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989, 46, 319–340. [Google Scholar] [CrossRef] [Green Version]
- Boella, N.; Gîrju, D.; Gurviciute, I. To Chip or Not to Chip? Determinants of Human RFID Implant Adoption by Potential Consumers in Sweden & the Influence of the Widespread Adoption of RFID Implants on the Marketing Mix; Lund University Publications: Lund, Sweden, 2019. [Google Scholar]
- Cristina, O.P.; Jorge, P.B.; Eva, R.L.; Mario, A.O. From wearable to insideable: Is ethical judgment key to the acceptance of human capacity-enhancing intelligent technologies? Comput. Hum. Behav. 2021, 114, 106559. [Google Scholar] [CrossRef]
- Chebolu, R.D. Exploring Factors of Acceptance of Chip Implants in the Human Body. Master’s Thesis, College of Sciences at the University of Central Florida, Orlando, FL, USA, 2021. [Google Scholar]
- John, O.P.; Srivastava, S. The Big-Five Trait Taxonomy: History, Measurement, and Theoretical Perspectives; University of California Berkeley: Berkeley, CA, USA, 1999. [Google Scholar]
- Pettersson, M. Microchip Implants and You: A Study of the Public Perceptions of Microchip Implants. Master’s Thesis, Department of Informatics Human-Computer Interaction and Social Media, UMEA University, Umea, Sweden, 2017. [Google Scholar]
- Patton, M.Q. Qualitative Evaluation and Research Methods; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 1990. [Google Scholar]
- Social Research Methods; Oxford University Press: Oxford, UK, 2016.
- Ritchie, J.; Lewis, J. Qualitative Research Practice: A Guide for Social Science Students and Researchers; Sage: London, UK, 2003. [Google Scholar]
- Reinares-Lara, E.; Olarte-Pascual, C.; Pelegrín-Borondo, J.; Pino, G. Nanoimplants that enhance human capabilities: A cognitive-affective approach to assess individuals’ acceptance of this controversial technology. Psychol. Mark. 2016, 33, 704–712. [Google Scholar] [CrossRef] [Green Version]
- Lamberg, J. Magnetic Resonance Imaging and VeriChip RFID Human Implant at 1.5 Tesla; University of Minnesota Twin Cities: Hauppauge, NY, USA, November 2005; Volume 1, p. 2010. [Google Scholar]
- Grauer, Y. A practical guide to microchip implants. Ars Tech. 2018, 3. Available online: https://arstechnica.com/features/2018/01/a-practical-guide-to-microchip-implants/ (accessed on 25 February 2022).
- Top 4 Benefits of Near Field Communication (NFC) Technology. 25 June 2019. Available online: https://www.fisglobal.com/en/insights/merchant-solutions-worldpay/article/top-4-benefits-of-near-field-communication-nfc-technology (accessed on 30 January 2022).
- Kazmeyer, M. The Advantages & Disadvantages of Implantable RFID Tags. Available online: https://itstillworks.com/rfid-technology-disadvantages-alternatives-2097.html (accessed on 5 February 2022).
- Reith, G.; Schmitz-Greven, V.; Hensel, K.O.; Schneider, M.M.; Tinschmann, T.; Bouillon, B.; Probst, C. Metal implant removal: Benefits and drawbacks–a patient survey. BMC Surg. 2015, 15, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanne, J.H. FDA approves implantable chip to access medical records. BMJ 2004, 329, 1064. [Google Scholar] [CrossRef] [Green Version]
- Implantable Chip, On Sale Now. Available online: https://www.wired.com/2002/10/implantable-chip-on-sale-now/ (accessed on 5 February 2022).
- How Can I Buy the Birth Control Implant & What Does it Cost? Available online: https://www.plannedparenthood.org/learn/birth-control/birth-control-implant-nexplanon/how-can-i-get-the-birth-control-implant:Implantremovalcancostbetween,andsomeothergovernmentprograms (accessed on 5 February 2022).
- Hague, M. Would You Implant a Microchip in Your Hand? Available online: https://www.cpacanada.ca/en/news/pivot-magazine/2019-10-31-vivokey-implants (accessed on 5 February 2022).
- Katz, J.E.; Rice, R.E. Public views of mobile medical devices and services: A US national survey of consumer sentiments towards RFID healthcare technology. Int. J. Med. Inform. 2009, 78, 104–114. [Google Scholar] [CrossRef]
- Al-Sebae, M.; Abu-Shanab, E. Big Issues for a Small Piece: RFID Ethical Issues. In Proceedings of the 7th International Conference On Information Technology (ICIT2015), Amman, Jordan, 12–14 May 2015; pp. 12–15. [Google Scholar]
- Funk, C.; Heferon, M.; Kennedy, B.; Johnson, C. Trust and Mistrust in Americans’ Views of Scientific Experts. 2021. Available online: https://www.pewresearch.org/science/2019/08/02/trust-and-mistrust-in-americans-views-of-scientific-experts/ (accessed on 15 November 2021).
- A Framework for Ethical Decision Making. Available online: https://www.scu.edu/ethics/ethics-resources/a-framework-for-ethical-decision-making/ (accessed on 3 February 2022).
- Velasquez, M.; Andre, C.; Shanks, T.; Meyer, M.J. Thinking ethically. In Issues in Ethics; Santa Clara University: Santa Clara, CA, USA, 2015; pp. 2–5. Available online: https://www.scu.edu/ethics/ethics-resources/ethical-decision-making/thinking-ethically/ (accessed on 25 February 2022).
- Mendez, K.F.; Jaremus, C. Future Employer: Are Humans with Microchips in Their Brains the Future of Work? 2021. Available online: https://www.seyfarth.com/news-insights/future-employer-are-humans-with-microchips-in-their-brains-the-future-of-work.html (accessed on 25 February 2022).
- Title VII of the Civil Rights Act of 1964. Available online: https://www.eeoc.gov/statutes/title-vii-civil-rights-act-1964 (accessed on 23 November 2021).
- Genetic Information Discrimination. Available online: https://www.eeoc.gov/genetic-information-discrimination (accessed on 23 November 2021).
- Brandtzæg, P.B.; Lüders, M.; Skjetne, J.H. Too many Facebook “friends”? Content sharing and sociability versus the need for privacy in social network sites. Int. J. Hum.-Comput. Interact. 2010, 26, 1006–1030. [Google Scholar] [CrossRef]
- Liu, Q.; Yao, M.Z.; Yang, M.; Tu, C. Predicting users’ privacy boundary management strategies on Facebook. Chin. J. Commun. 2017, 10, 295–311. [Google Scholar] [CrossRef]
- Juban, R.L.; Wyld, D.C. Would you like chips with that?: Consumer perspectives of RFID. Manag. Res. News 2004. [Google Scholar] [CrossRef]
- Ong, C.-S.; Lai, J.-Y. Gender differences in perceptions and relationships among dominants of e-learning acceptance. Comput. Hum. Behav. 2006, 22, 816–829. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G. Why don’t men ever stop to ask for directions? Gender, social influence, and their role in technology acceptance and usage behavior. MIS Q. 2000, 24, 115–139. [Google Scholar] [CrossRef]
- Smith, A.D. Gender preferences of efficiencies and ethical issues: Commercial, personal, and governmental applications of RFID-based implants and technologies. Int. J. Bus. Inf. Syst. 2013, 12, 455–492. [Google Scholar] [CrossRef]
- Katz, J.E.; Rice, R.E. Social Consequences of Internet Use: Access, Involvement, and Interaction; MIT Press: Cambridge, MA, USA, 2002. [Google Scholar]
- Socioeconomic Status. Available online: https://www.apa.org/topics/socioeconomic-status (accessed on 25 February 2022).
- Abu-Shanab, E. Income Divide: A Determinant of Technology Acceptance. Int. Arab. J. e-Technol. 2013, 3, 121–127. [Google Scholar]
- Riddell, W.C.; Song, X. The Role of Education in Technology Use and Adoption: Evidence from the Canadian Workplace and Employee Survey. IZA Discussion Papers 6377. Inst. Study Labor (IZA) 2017, 70, 1219–1253. [Google Scholar] [CrossRef]
- Durodolu, O. Technology Acceptance Model as a Predictor of Using Information System’ to Acquire Information Literacy Skills. 2016. Available online: https://digitalcommons.unl.edu/libphilprac/1450/ (accessed on 5 February 2022).
- Porter, C.E.; Donthu, N. Using the technology acceptance model to explain how attitudes determine Internet usage: The role of perceived access barriers and demographics. J. Bus. Res. 2006, 59, 999–1007. [Google Scholar] [CrossRef]

{kind=link}
| Demographic | Answer Choice |
|---|---|
| Age | 1. 18–29 years (n = 73) |
| 2. 30–49 years (n = 60) | |
| 3. 50–64 years (n = 36) | |
| 4. 65–79 years (n = 8) | |
| 5. 80 years and above (n = 1) | |
| 6. Unspecified (n = 1) | |
| Gender | 1. Male (n = 50) 2. Female (n = 126) 3. Fluid (n = 1) 4. Prefer not to disclose (n = 1) 5. Other (n = 1) |
| Race | 1. African American or Black (n = 48) 2. Asian or Pacific Islander (n = 14) 3. Hispanic/Latino (n = 6) 4. Native American or American Indian (n = 0) 5. White or Caucasian (n = 86) 6. Other (n = 18) 7. Unspecified (n = 7) |
| Immigrant? | 1. Yes (n = 72) 2. No (US national) (n = 96) 3. Unspecified (n = 11) |
| Medical Conditions? | 1. Yes (n = 78) 2. No (n = 95) 3. Unspecified (n = 6) |
| Disability? | 1. Yes (n = 26) 2. No (n = 148) 3. Unspecified (n = 5) |
| Theme | Category | Code | Code Frequency in % (n Out of 179) |
|---|---|---|---|
| Health Risks | All Health Risks | 40.8 (n = 73) | |
| Risk Type | Mental Issues | 6.7 (n = 12) | |
| Physical Issues | 5.0 (n = 9) | ||
| Risk Temporality | Long-Term Side Effects | 12.2 (n = 22) | |
| Short-Term Side Effects | 7.3 (n = 13) | ||
| Risk Nature | Generally Unnatural | 4.5 (n = 8) | |
| Data Protection | Data Misuse | Steal Data | 29.0 (n = 53) |
| Misuse Data | 31.0 (n = 55) | ||
| Organizational | 22.9 (n = 41) | ||
| Surveillance | Governmental | 6.7 (n = 12) | |
| GPS tracking | 1.1 (n = 2) | ||
| Knowledge | Side effects | 4.5 (n = 8) | |
| Inadequate | Efficacy | 1.7 (n = 3) | |
| Regulations/Limitations | 1.7 (n = 3) | ||
| General/Other | 1.1 (n = 2) | ||
| Ambiguous | Uncertainty | 5.0 (n = 9) | |
| Negative Affect | Surgery Related | Removal | 4.5 (n = 8) |
| Implantation | 6.7 (n = 12) | ||
| Usage Related | Everyday Pain | 0.6 (n = 1) | |
| Other | 1.1 (n = 2) | ||
| Metaphysical Dilemmas | Ethical and Moral | Personal Conscience | 5.6 (n = 10) |
| Religious | Belief Conflict | 6.2 (n = 11) | |
| Ease of Use | Task Completion | Malfunctions | 6.7 (n = 12) |
| Task Safety | No Control | 5.6 (n = 10) | |
| Monetary Issues | Expenses | Others | 6.7 (n = 12) |
| Maintenance Fees | 0.6 (n = 1) | ||
| Negative Social Impact | Problems | Social Inequality | 1.7 (n = 3) |
| Monetary Laundering | 0.6 (n = 1) | ||
| Absence | No Concern | Nothing | 2.3 (n = 4) |
| Theme | Medical Condition % | Immigrant? % | ||
|---|---|---|---|---|
| Yes | No | Yes | No | |
| Health Risks | 96.0 (n = 75) | 65.3 (n = 62) | 60.0 (n = 43) | 90.6 (n = 87) |
| Data Protection | 85.0 (n = 66) | 61.0 (n = 58) | 50.7 (n = 37) | 85.4 (n = 82) |
| Knowledge | 18.0 (n = 14) | 11.6 (n = 11) | 15.2 (n = 11) | 10.4 (n = 10) |
| Negative Affect | 14.1 (n = 11) | 12.6 (n = 12) | 12.5 (n = 9) | 12.5 (n = 12) |
| Metaphysical Dilemmas | 12.8 (n = 10) | 10.5 (n = 10) | 11.1 (n = 8) | 13.5 (n = 13) |
| Monetary Issues | 11.5 (n = 9) | 4.2 (n = 4) | 2.8 (n = 2) | 10.0 (n = 9) |
| Negative Social Impact | 6.4 (n = 5) | 1.0 (n = 1) | 4.2 (n = 3) | 3.1 (n = 3) |
| Absence | 0.0 (n = 0) | 4.2 (n = 4) | 2.8 (n = 3) | 2.1 (n = 2) |
| Theme | Category | Code | Code Frequency in % (n Out of 179) |
|---|---|---|---|
| Medical Uses | Corrective Uses | Solve Mental Disabilites | 8.4 (n = 15) |
| Fix Physical Disabilities | 40.2 (n = 72) | ||
| Healthcare Services | Personalized Care | 2.8 (n = 5) | |
| Health Monitoring | 14.0 (n = 24) | ||
| Enhance Quality of Life | 16.8 (n = 30) | ||
| Research | Understand Mind and Body | 1.7 (n = 3) | |
| Diagnose Diseases | 3.9 (n = 7) | ||
| Other Uses | Convenience | Replace Cash and Cards | 2.8 (n = 5) |
| Secure Entry into Buildings | 2.3 (n = 4) | ||
| Law Enforcement | Track Criminals | 0.6 (n = 1) | |
| Control Crimes | 1.1 (n = 2) | ||
| Public Awareness | Knowledge | 18.4 (n = 33) | |
| Dismissal of Microchips | No Hope | Indifference | 2.2 (n = 4) |
| No Future | 14.0 (n = 25) | ||
| Technical Advances | Improved Safety | Safe to Use | 4.7 (n = 8) |
| Better Performance | 0.6 (n = 1) | ||
| Data Protection | Security Mechanisms | 3.9 (n = 7) | |
| Privacy Controls | 2.2 (n = 4) | ||
| Surgery-Related | Not be Implantable | 1.7 (n = 3) | |
| Temporary Implant | 1.1 (n = 2) | ||
| Human Enhancement | Enhancement Uses | Mental Capabilities | 1.1 (n = 2) |
| Other Capabilities | 12.3 (n = 22) | ||
| Regulations | Affirmations | Regulate Use | 1.1 (n = 2) |
| Keep it Optional | 3.9 (n = 7) | ||
| Clarifications | Religious Verdict | 0.6 (n = 1) | |
| Safe Uses | 1.1 (n = 2) | ||
| Affordability | Reduced Cost | Maintenance and Surgery | 3.9 (n = 7) |
| Theme | Medical Conditions % | Immigrant? % | ||
|---|---|---|---|---|
| Yes | No | Yes | No | |
| Medical Uses | 98.7 (n = 77) | 78.6 (n = 75) | 63.9 (n = 46) | 90.6 (n = 87) |
| Other Uses | 28.2 (n = 22) | 24.2 (n = 23) | 26.4 (n = 19) | 22.9 (n = 22) |
| Human Enhancement | 15.4 (n = 12) | 13.7 (n = 13) | 9.7 (n = 7) | 15.6 (n = 15) |
| Affordability | 1.3 (n = 1) | 6.3 (n = 6) | 4.2 (n = 3) | 4.2 (n = 4) |
| Technical Advances | 17.9 (n = 14) | 14.7 (n = 14) | 16.7 (n = 12) | 16.7 (n = 16) |
| Regulations | 1.3 (n = 1) | 8.4 (n = 8) | 6.9 (n = 5) | 4.2 (n = 4) |
| Dismissal of Microchips | 20.5 (n = 16) | 13.7 (n = 13) | 13.9 (n = 10) | 17.7 (n = 17) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shafeie, S.; Chaudhry, B.M.; Mohamed, M. Modeling Subcutaneous Microchip Implant Acceptance in the General Population: A Cross-Sectional Survey about Concerns and Expectations. Informatics 2022, 9, 24. https://doi.org/10.3390/informatics9010024
Shafeie S, Chaudhry BM, Mohamed M. Modeling Subcutaneous Microchip Implant Acceptance in the General Population: A Cross-Sectional Survey about Concerns and Expectations. Informatics. 2022; 9(1):24. https://doi.org/10.3390/informatics9010024
Chicago/Turabian StyleShafeie, Shekufeh, Beenish Moalla Chaudhry, and Mona Mohamed. 2022. "Modeling Subcutaneous Microchip Implant Acceptance in the General Population: A Cross-Sectional Survey about Concerns and Expectations" Informatics 9, no. 1: 24. https://doi.org/10.3390/informatics9010024
APA StyleShafeie, S., Chaudhry, B. M., & Mohamed, M. (2022). Modeling Subcutaneous Microchip Implant Acceptance in the General Population: A Cross-Sectional Survey about Concerns and Expectations. Informatics, 9(1), 24. https://doi.org/10.3390/informatics9010024