1. Introduction
As a consequence of technological developments and medical advances, human life expectancy has continued to rise in recent decades. There is a need to predict and monitor the evolution of future mortality levels in fields such as pension planning, insurance, public health and government policy. Researchers and practitioners have proposed various mortality forecasting models to accommodate different needs. For instance,
Lee and Carter (
1992) introduced a parsimonious mortality model with age and time effects, which can readily be estimated using singular vector decomposition. The Lee-Carter model is one of the most popular models in the extrapolative family whose members assume a continuation of past patterns. In the application of such models, the choice of the sample period can have a significant impact on forecast accuracy (
Booth et al. 2006).
On the one hand, adopting only the recent data may overlook historical features that are pivotal for prediction. Also, as mortality data are usually available by single year, too short a calibration period may lead to unstable parameter estimates. On the other hand, longer estimation periods do not necessarily produce more accurate forecasts, as there may exist certain structural changes in the sample. In the current literature, time effects in mortality models (e.g., the pace of mortality reductions) are often captured by random walk with drift (RWD), which may not be appropriate in the presence of structural changes (
van Berkum et al. 2013). For example, when a RWD is fitted to the mortality index in the Lee-Carter model, the drift term is determined only by the beginning and ending values, ignoring potential signals of structural changes within the sample period. Consequently, the predicted mortality rates will ignore structural shifts that could impact forecast trends, and may yield results that are highly sensitive to the estimation period.
Approaches to incorporate the effect of structural changes can be considered in three broad categories, the regime-switching model, broken-trend stationary (
Perron 1989) and difference stationary processes with breakpoints (
van Berkum et al. 2013).
Milidonis et al. (
2011) argued that regime-switching models can be employed to describe different mortality states. Specifically, they allowed the error term of the mortality index in the Lee-Carter model to switch between two states with different means and variances and suggested potential deviations from the normality of the error term. The main criticism of regime-switching models is that one may not expect influences on human mortality from developments such as medical advances to be reversed over time (
van Berkum et al. 2013), which makes the model somewhat unrealistic. It is also difficult to estimate the switching frequencies as there are only a few major structural changes in the last century.
The other two categories focus on the existence of potential structural changes and unit roots in the time series processes of mortality models.
Sweeting (
2011) proposed a broken-trend stationary model to detect multiple structural changes using the Cairns-Blake-Dowd model (
Cairns et al. 2006) as a base.
Li et al. (
2011) applied a trend stationary model to the mortality index in the Lee-Carter model using data from England and Wales and the United States, allowing a structural change to occur at a breakpoint. They also pointed out that this approach produces rather narrow prediction intervals, which may not be adequate to capture uncertainties of future mortality rates. For difference stationary models, the most common choice is a (multi-dimensional) random walk with drift (e.g.,
Cairns et al. 2009;
Dowd et al. 2010). Nonetheless, several studies have expressed concerns about the appropriateness of assuming a constant drift. For instance,
O’Hare and Li (
2015) applied a random walk with drift process to the mortality index in the Lee-Carter model and detected changes in the drift term over time based on the mortality data of Australia, the Netherlands, the United Kingdom and the United States. Similar to applications of the broken-trend stationary model, multiple breaks are also analyzed under the difference stationary model in
van Berkum et al. (
2013,
2016).
To date, most attention has been paid to investigating structural shifts via the time effects of mortality models, neglecting the evolution of age effects. It is often assumed that the age response to mortality changes remains constant over time.
Carter and Prskawetz (
2001) estimated the parameters of the Lee-Carter model using different subsamples with a fixed length. They found that the pattern of age response changed significantly for the Austrian population over the sample period 1947–1999. Nevertheless, their paper did not propose a readily applicable method to predict future age patterns.
Li et al. (
2013) rotated the shape of the Lee-Carter age response to depict the acceleration (deceleration) of mortality improvements at older (younger) ages. The life expectancy at birth is employed as an indicator for the occurrence of the rotation in age patterns, which involves the projection of future life expectancy. Despite the subtleness of the rotation approach, they emphasized the importance of incorporating the changing age patterns into mortality predictions. In the recent work of
Li and Wong (
2020), the authors attempted to capture the movements of age patterns by analyzing the age response in the Lee-Carter model from (relatively) homogeneous subperiods. They suggested three ways to estimate future age responses, including assuming a continuation of the latest patterns, fitting a modified
Heligman and Pollard (
1980) curve and applying principal components analysis. Specifically, estimated parameters of the fitted curve and principal components over successive subperiods can be extrapolated via linear regression to compute the age sensitivity parameter for a future period. Their study emphasized the importance of considering the changing age patterns of structural changes in mortality predictions.
In light of the findings of time-varying age effects, this paper proposes a method to fit and forecast the evolution of the age sensitivity factor under the Lee-Carter model, integrating for the first time structural changes in both age and time effects. The method is applied to mortality data for the male population aged 0 to 89 from 1950 to 2016
1 of Australia, Canada, New Zealand, Sweden, the United Kingdom and the United States, from the Human Mortality Database (
Human Mortality Database 2019).
Inspired by the findings in
Carter and Prskawetz (
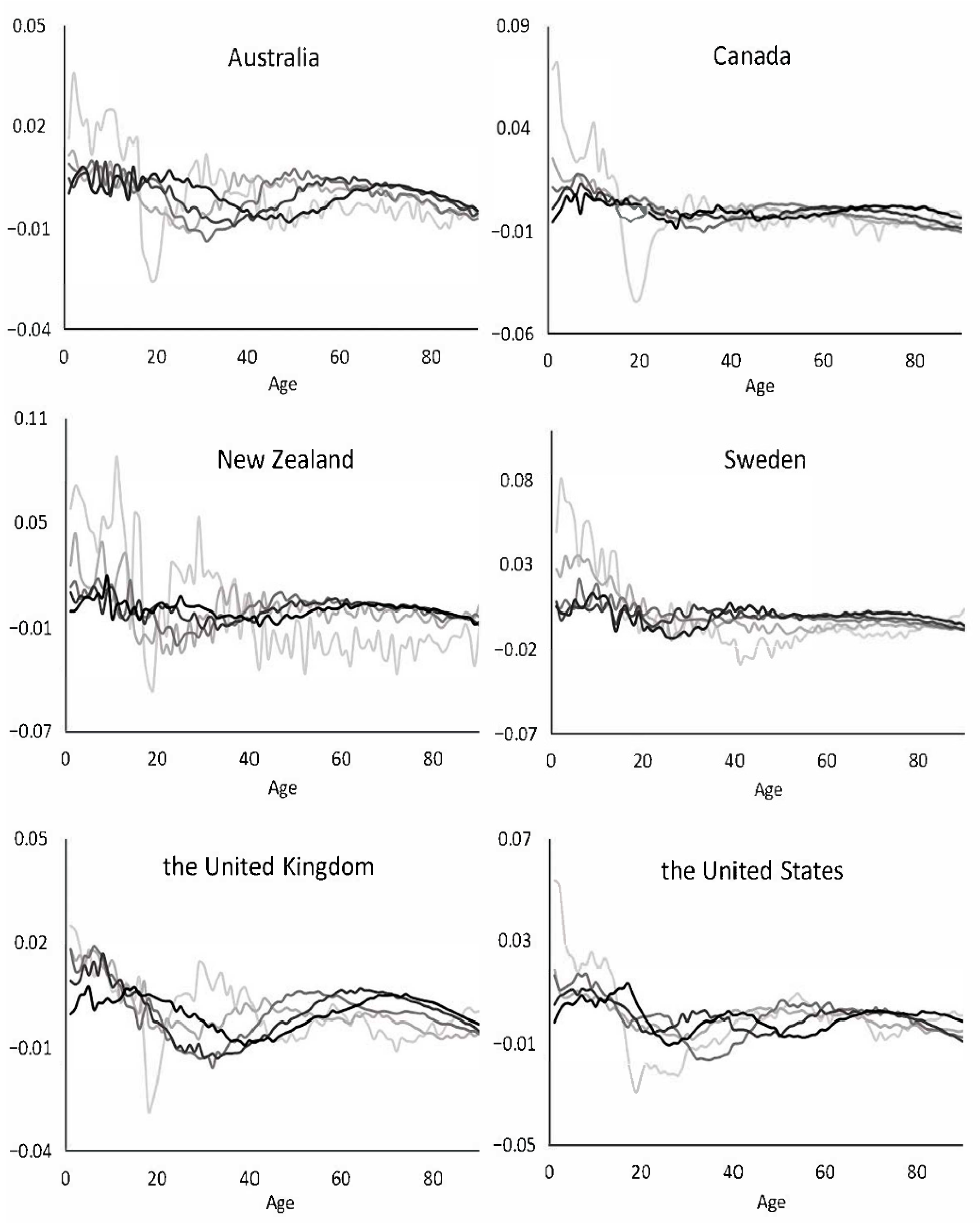
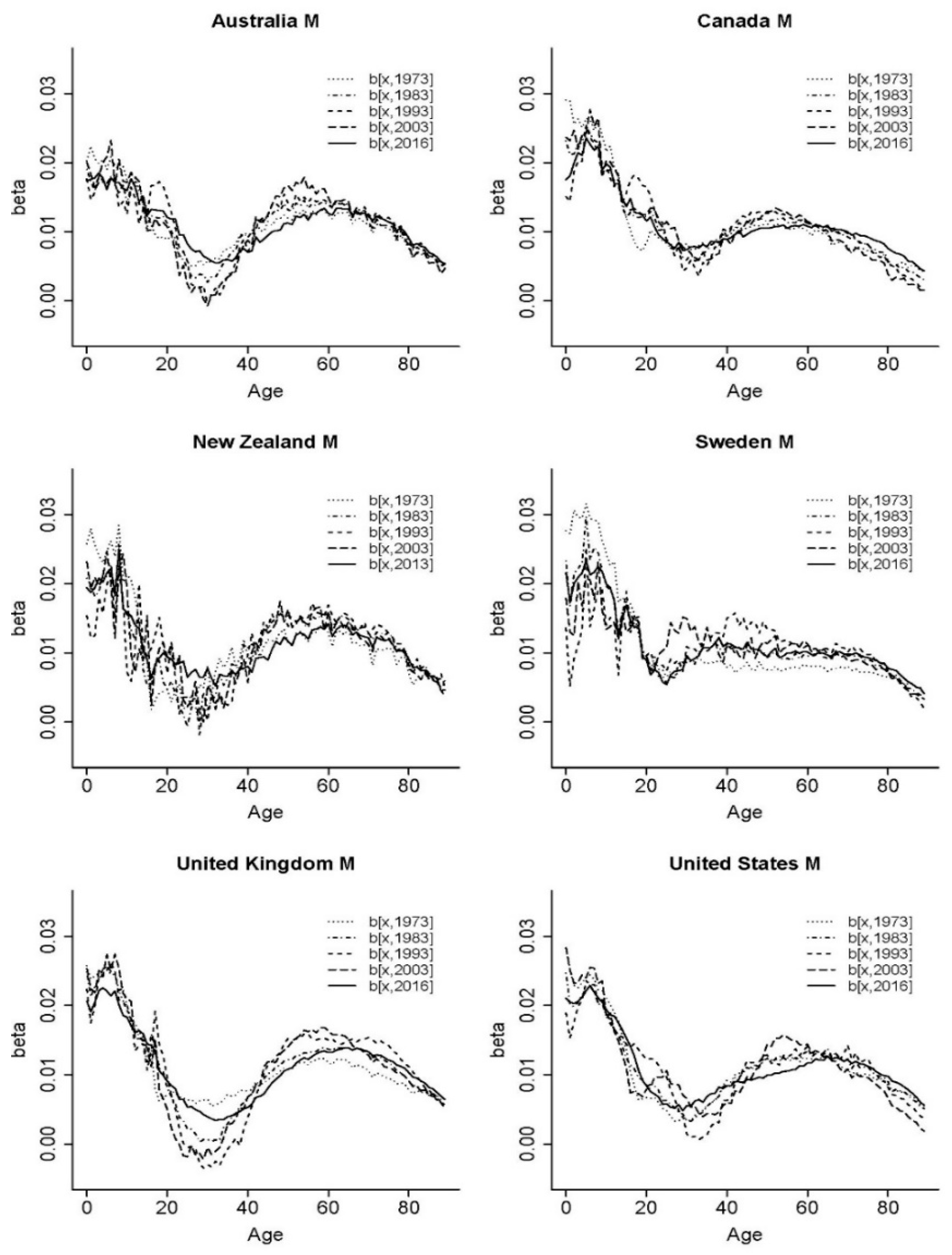
2001), we first examined the structure of the age effects under the Lee-Carter model. Setting the same length of fitting periods as in their paper, the first subsample included years 1950–1973. Then, both the starting and ending points of the subsample increased by one year sequentially until the latest data in the sample were employed. For example, the sample period between 1950 and 2016 can be arranged to form 44 subperiods.
Figure 1 shows the estimated age sensitivity parameters of the Lee-Carter model calibrated using the sequential subsamples. The colour intensity of the curve increases with the date of the corresponding subsample, with the darkest representing the parameters obtained from the latest subperiod. For presentation purposes, we only displayed the values with a 10-year gap.
It was interesting to see that the age responses were wave-like, and the shape propagated and deformed over time. These observations inspired us to fit a Fourier series with time-varying parameters comprised of single or multiple sine and cosine waves. The Fourier analysis was initially introduced by the mathematician Baron Jean Baptiste Joseph Fourier in his study about temperature distributions. It helped to decompose complicated periodic functions into a sum of sinusoidal components and identify critical features of interest. It can interpret characteristics of a time series process (e.g., peaks, troughs, cycles) in terms of values in the frequency domain (e.g., frequencies, amplitudes, phases). Researchers have applied the Fourier analysis to a wide range of fields such as optics (
Lombardet et al. 2005;
Mei and Svanberg 2015), agriculture (
Canisius et al. 2007), electricity (
Amaral et al. 2008), magnetics (
Gysen et al. 2010) and insurance (
Powers and Powers 2015). For more technical details of Fourier series and its applications, one may refer to Chapters 1 and 2 of
Bracewell (
1978).
An alternative to the Fourier approach is fitting a smooth curve using cubic splines comprising piecewise third-order polynomials joined at a set of knots. Splines are capable of producing a good fit when the number of knots is sufficiently large. However, the coefficients of splines are not readily interpretable, causing difficulties in choosing an appropriate method to predict their future trends. In this paper, we applied both the Fourier function and cubic splines to capture the development of age patterns of mortality and compare their performances with those under the baseline Lee-Carter model.
Overall, we propose a potential method to model the time-varying age patterns of mortality development. Our main objective was to investigate the performance of the proposed models and to test the impact of incorporating the age effects of structural changes. The remainder of the paper is organized as follows.
Section 2 introduces the specifications of the Lee-Carter and proposed models constructed using the Fourier series and cubic splines.
Section 3 and
Section 4 compare the prediction performance of the mortality models and conduct backtesting using mortality data of the six above-mentioned countries.
Section 5 presents a case study to illustrate how the proposed model can readily integrate the age and period effects of structural changes based on data from the United Kingdom.
Section 6 concludes.
2. Methodology
The original Lee-Carter model expresses the logarithm of central death rates
as a linear/bilinear combination of age and time effects,
where
represents the average mortality level at each age,
is a time-varying mortality index,
is the age-specific factor
2 indicating the sensitivity of
to the changes in
, and
follows a Gaussian distribution with a mean of zero. As mentioned earlier, there has been clear evidence against the assumption of a time-invariant age response in the original Lee-Carter model, which can be addressed by allowing the age sensitivity factor to vary over time.
The term
is denoted as the age response at age
x in year
. Projecting
directly brings almost a hundred time series processes for a wide age range. To reduce the dimensionality, a parametric function can be fitted to the time-varying age response. Specifically, we considered two methods—the Fourier-like series and cubic splines with time-varying parameters and refer to them as the Fourier and cubic Lee-Carter models in the rest of the paper. Unlike other approaches of dimensionality reduction such as the principal component analysis that contains artificial variables (
Vyas and Kumaranayake 2006), the Fourier series has the advantage that its parameters are interpretable. This property becomes useful in incorporating assumptions of future age patterns into mortality projections.
For a given sample relating to year
t, the age response
can be expressed as a series ordered by age
x. We then add the time dimension to the coefficients and apply a Fourier series
3 as follows,
where
represents the intercept of the Fourier series relating to year
t,
is a predefined total number of harmonic waves, the amplitude parameter
measures the distance from the peak (or trough) to the central value, the phase parameter
represents the number of “sinusoidal periods” (measured in the age dimension) that has been shifted from a predefined point, the frequency parameter
gives the number of cycles per unit of age, and
is the Gaussian error term with null mean. One could use time-varying frequencies to obtain a better fit, but allowing frequency values to change over time leads to different dimensions of Fourier parameters at different points of time, which makes the extrapolation infeasible. Given the frequency values, one can estimate
,
, and
via linear regression sequentially.
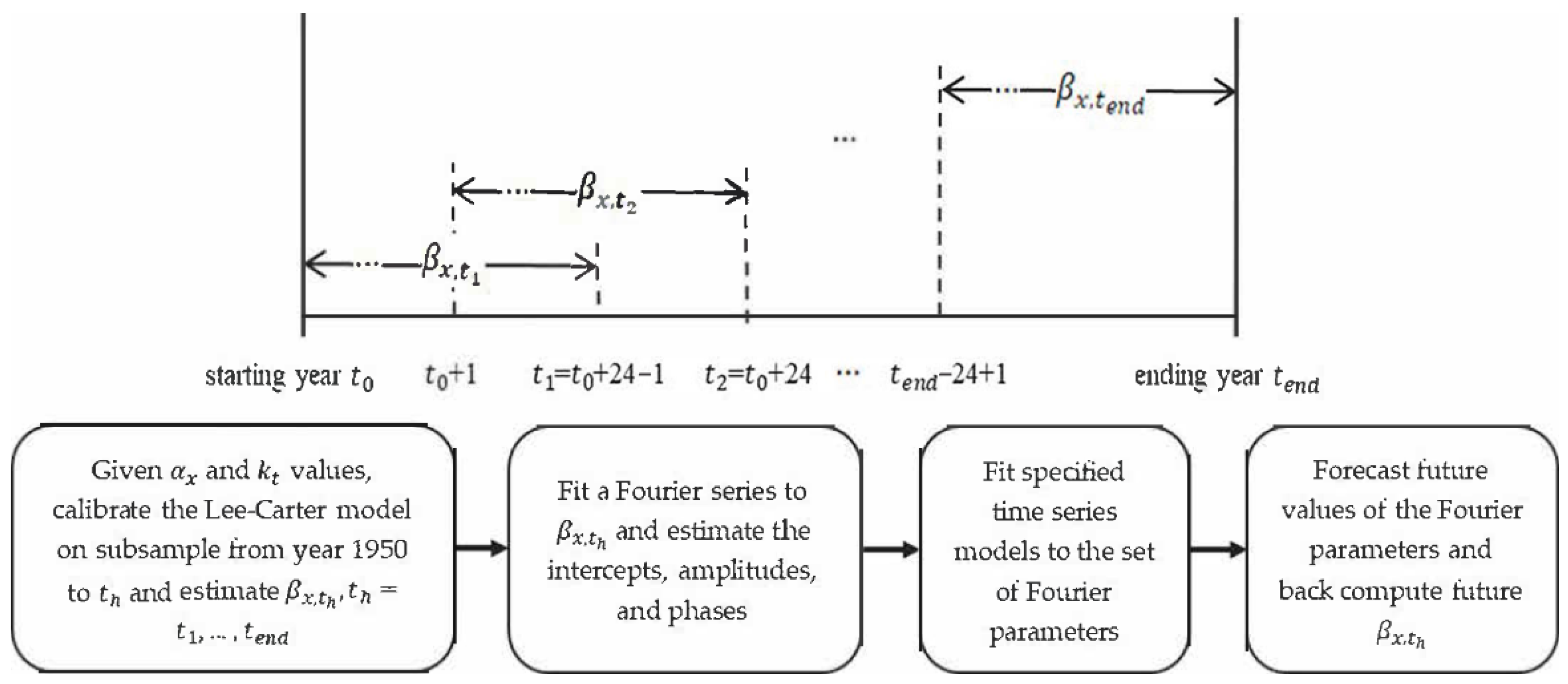
Figure 2 presents a flow diagram of the modelling process of
.
As illustrated, the entire sample period can be split into different subperiods. These subperiods were structured as overlapping to some extent
4 in order to obtain more data points and smoother changes over time for the Fourier parameters. However, these overlapping subsamples would give different
and
values. To make the estimates of the age sensitivity factor more comparable across the subperiods, we first fitted the Lee-Carter model to the whole sample period and treated the computed
and
as given. The Lee-Carter model was then calibrated to each (overlapping) subperiod in turn using a Poisson updating scheme
5 (
Brouhns et al. 2002;
Li 2013) and a unique set of
values was obtained, where
referred to the last year of a subsample. For instance, the first
corresponded to the age response over the period from the starting year of the sample to 24 years later; the last one
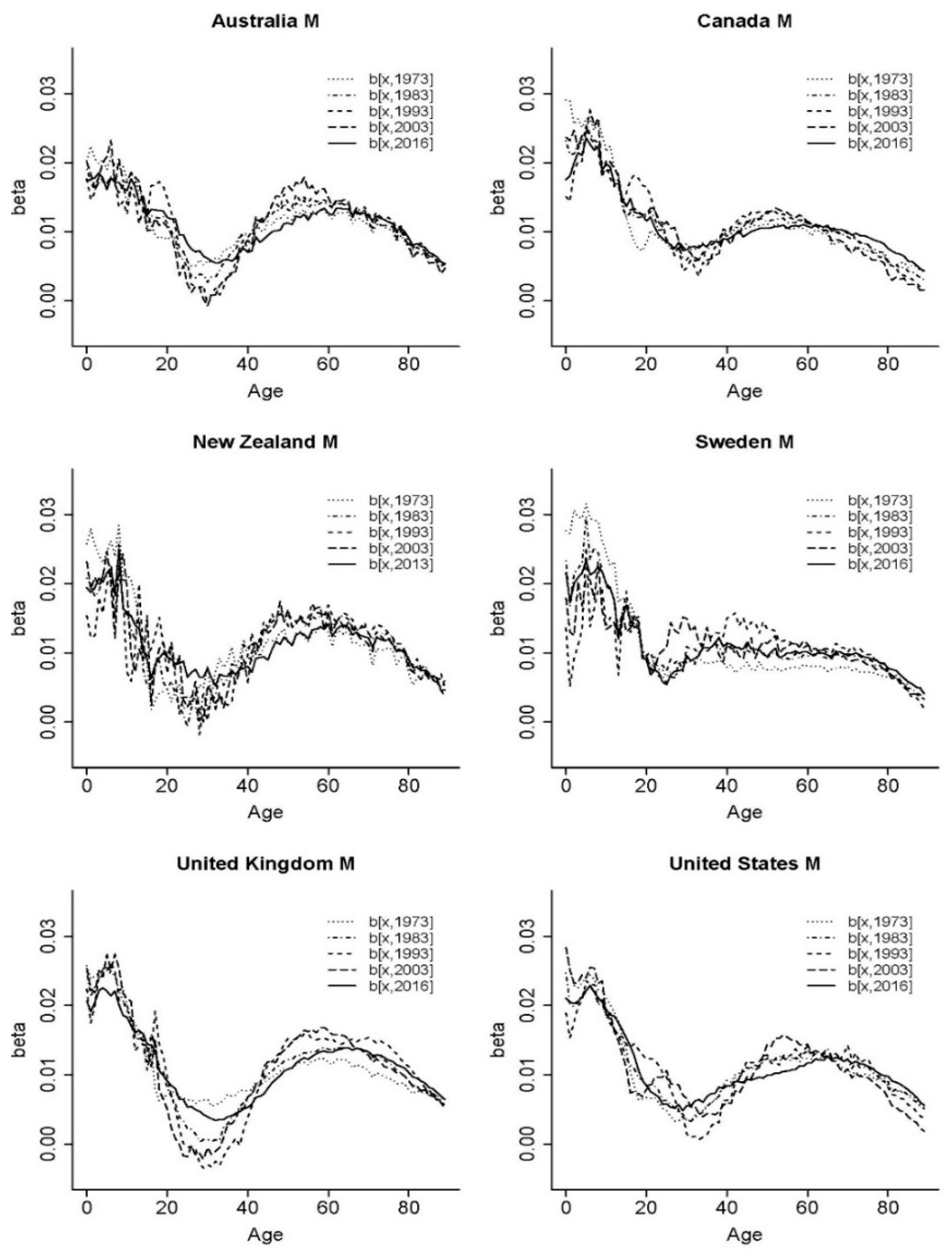
corresponded to the years between the ending year of the sample and 24 years earlier. The age sensitivity parameters calibrated on different subperiods of the sample from 1950 to the latest year are plotted in
Figure 3.
Here, we followed the choice of
Carter and Prskawetz (
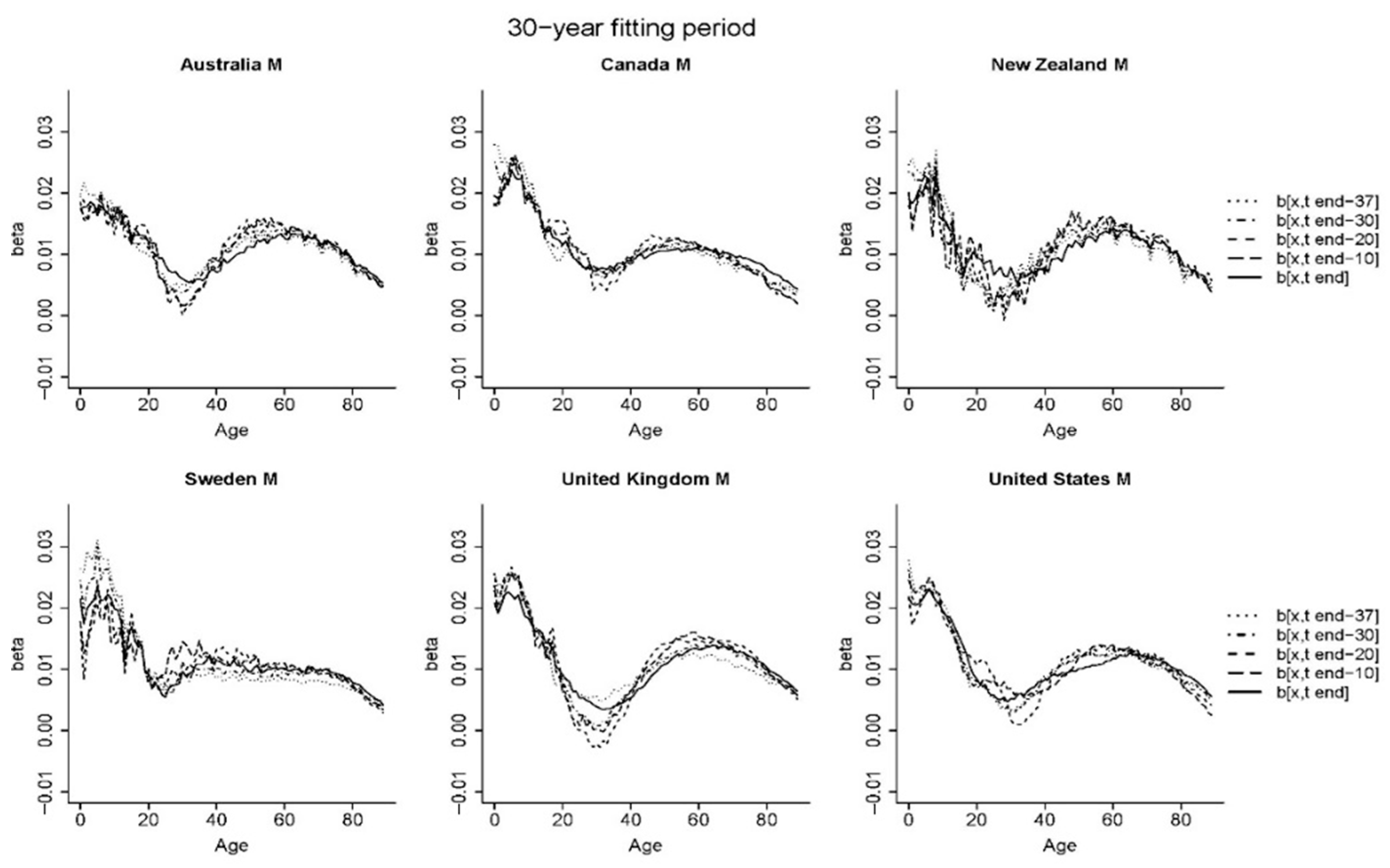
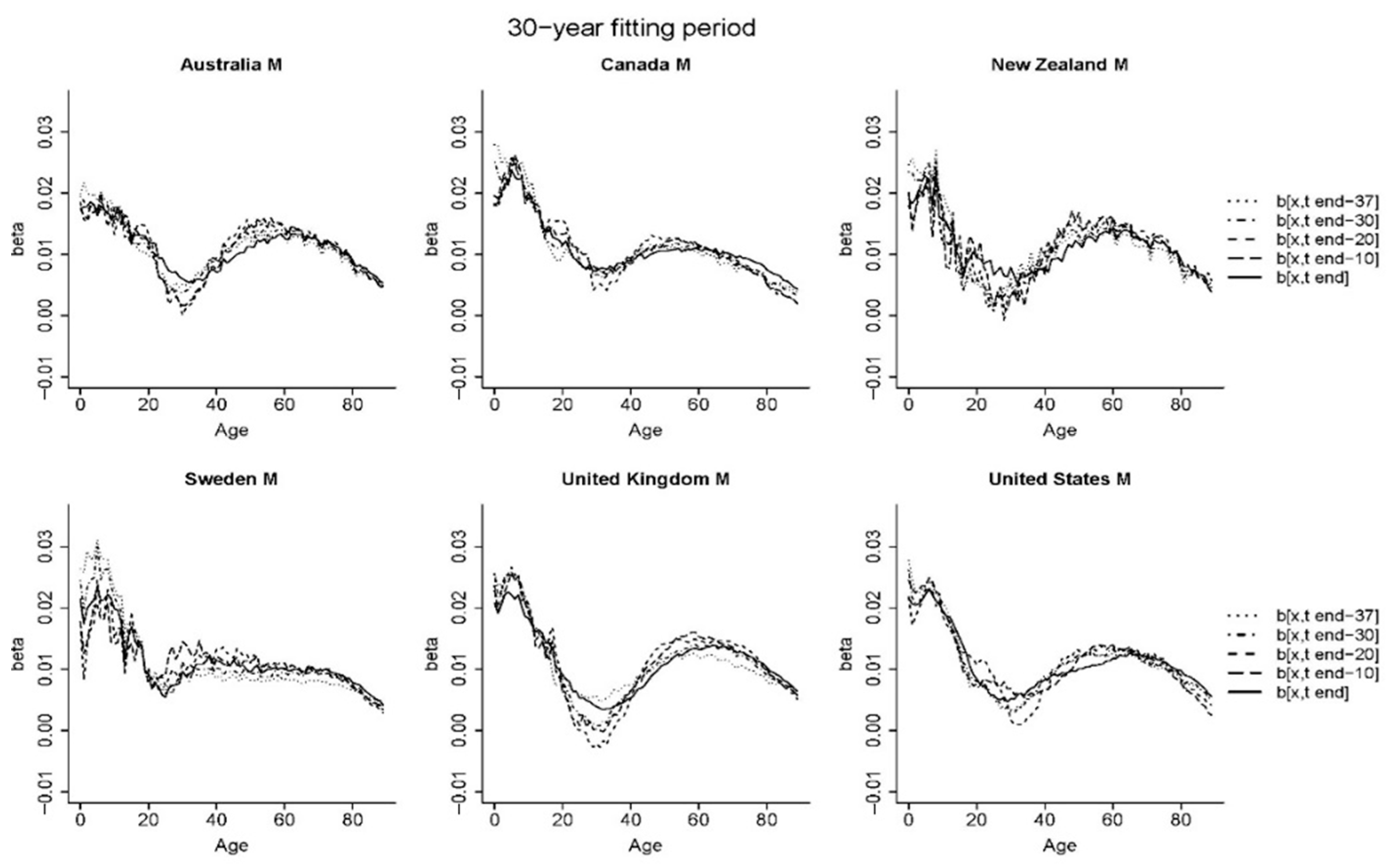
2001) and used an arbitrary fixed value of 24 years for each subsample, although other lengths of subperiods may be chosen. We tested four different lengths of the subperiods and presented the estimated age response parameters in
Figure A1 in
Appendix A. When longer subperiods were employed, the changes in the shape of age response were relatively less evident. Overall, the lengths of 20, 24, and 30 years produced a similar extent of “volatility” in the age response parameters calibrated on sequential subsamples
6. On the other hand, the 10-year window appeared to be too short and the resulting parameter estimates were volatile.
In general, the curves of most of the countries showed two peak values occurring at the youngest ages and around ages 50–65. One exception was Sweden whose age-specific response curve was relatively flat over middle ages. The magnitude of the first peak tended to be greater than the other, implying a high sensitivity of new-borns to mortality changes. Compared with the curves presented in
Figure 1, the age sensitivity factors in
Figure 3 showed less evident development patterns over time (e.g., peaks shifting towards higher ages). The
plotted in
Figure 3 were estimated by treating the same set of
and
values as given. Therefore, the shapes of
from different subperiods were more comparable with one another than those estimated using different sets of
and
.
When modelling the human age response, it was desirable to keep the main features in the original values such as the peaks mentioned above. Also, the spikes at the youngest ages might have affected the estimates of Fourier parameters which then would not capture the characteristics at older ages
7 adequately. To differentiate between the noticeable patterns at younger and older ages, the estimated age sensitivity factors displayed in
Figure 3 may be described as one quarter of a complete wave at the younger ages followed by a half wave with a smaller amplitude over the remaining age range. Therefore, we decomposed the age response into two waves and estimated two sets of Fourier parameters instead of modelling it as a whole. For each of the two regions, we employed only one harmonic wave (
) to depict the shape of age sensitivity factors to avoid over-parameterisation
8. The adjusted Fourier series with a split can be expressed as follows,
where
is the common intercept shared by the two piecewise functions,
is the splitting age at which a wave for the older population starts,
,
and
are the frequency, amplitude and phase parameters of the
wave,
and
are the coefficients of the
regression,
. The two peak values were observed at age
and
, respectively. The frequency values that controlled the lengths of harmonic waves are determined to maintain the observed features of human age sensitivity. As mentioned above, the first wave displayed about one quarter of a complete cycle, suggesting that the length of the wave was approximately
. Similarly, the second wave corresponded to a half cycle, so the length of the second wave could be estimated by
, where
was the maximum age in the sample data. Accordingly, the two frequency values
and
were employed. Thereinto,
was chosen as age 0 arbitrarily for all the countries, although the locations of
and
were not deduced directly from the graph. They were estimated using the ages at which the minimum and maximum (excluding the first peak)
were achieved, averaged over all subperiods. Note that
did not affect the choice of frequencies and could have been captured by the second phase parameter. For the six countries considered, the splitting age
occurred at around age 30, and the second peak
generally fell within ages 50–60. Specifically, we set
as the age-specific sensitivity value at the linking age which approximated the average level of the first and second waves.
After specifying the frequency values, the amplitude and phase parameters could be estimated via the linear regression method, specifically, for the ith wave, . Rearranging the expressions, we could calculate the and as: and .
However, the identification problem existed in estimating the phase parameter due to the periodicity of trigonometric functions. For instance, could be either 0 or , as and always resulted in equivalent tangent values. Therefore, we imposed restrictions on the range of the two phase parameters according to the general shape of age sensitivity factors. Since one would have expected a peak followed by a decreasing pattern at young ages, the range of was set to (). Similarly, the range of was restricted to (−), so that a bell-shaped curve could be observed for ages after the knot . Next, we explained the rationale of these two constraints.
Several features can be preserved when fitting a Fourier series to the age sensitivity factor based on the historical shape. On the one hand, the curve went downward before the splitting age, although such a pattern is not necessarily monotonic from age 0. On the other hand, the age response at ages older than the knot
generally showed a bell shape for the six countries considered. Based on these observations,
Figure 4 illustrated possible shapes of
over the domain
and
for
, respectively. Since the two frequency parameters were determined such that the first (second) wave corresponded to a quarter (half) of a complete wave, we focused on the curves for
(
) on the left (right) graph. As shown in the left column of
Figure 4, when the first phase parameter
took values between
(red curve) and
(green curve), the first quarter of the waves were mainly downward, matching with the historical characteristics of
at younger ages. For possible shapes of
at older ages (right column), the first half of the waves
demonstrated a bell shape when
ranged from
to
.
Overall, for each t we fitted the Fourier series with two waves to and estimated the Fourier parameters , and , . Accordingly, the dimension was reduced from 90 (ages) to 5 (one intercept, two amplitude, and two phase parameters). The intercepts, amplitudes and phases were time-varying, the future values of which were predicted via time series models. Forecasts of the age response could then be computed from the predictions of its Fourier parameters.
The above specification of the Fourier Lee-Carter model is similar to the cubic spline technique which has been widely applied in smoothing mortality rates (e.g.,
Currie et al. 2004;
Armstrong 2006;
De Jong and Tickle 2006;
Debón et al. 2006). A function
defined on
with
interior knots
is a cubic spline if it is a cubic polynomial in each of the intervals and
is continuous up to the second derivative. Thereinto, one sub-category that solves the potential problem of erratic fitting at boundary values is referred to as natural cubic splines. It imposes additional constraints on the second and third derivatives at the two limits
and
such that
is linear in the two boundary intervals
and
. We borrowed this concept and considered a so-called cubic Lee-Carter model whose age sensitivity factor
was modelled as natural cubic splines. The idea was to interpolate a curve using segments of cubic polynomials connected by knots that were placed at turning points. As analyzed above, there were two peaks at ages
and
and one trough at age
. The three internal knots were selected for our cubic Lee-Carter model and located at (0,
,
). The chosen knots would result in a decreasing trend from age 0 to the trough age
, followed by a bell-shaped curve peaked at
. The piecewise polynomial could be estimated using linear regression and the R package “
splines”. Again, we modeled the cubic-spline parameters as time series processes to predict future age sensitivity. In matrix notation, the age sensitivity factor under the cubic Lee-Carter model could be written as follows,
where the
vector
referred to the age response at all ages at time
, vector
comprised the constants and error terms for each regression of
.
was the (
) basis matrix defining the vector space of the spline function, which could be obtained by the command “
ns” in R. Then the
vector
containing the time-varying cubic-spline coefficients was estimated via linear regression.
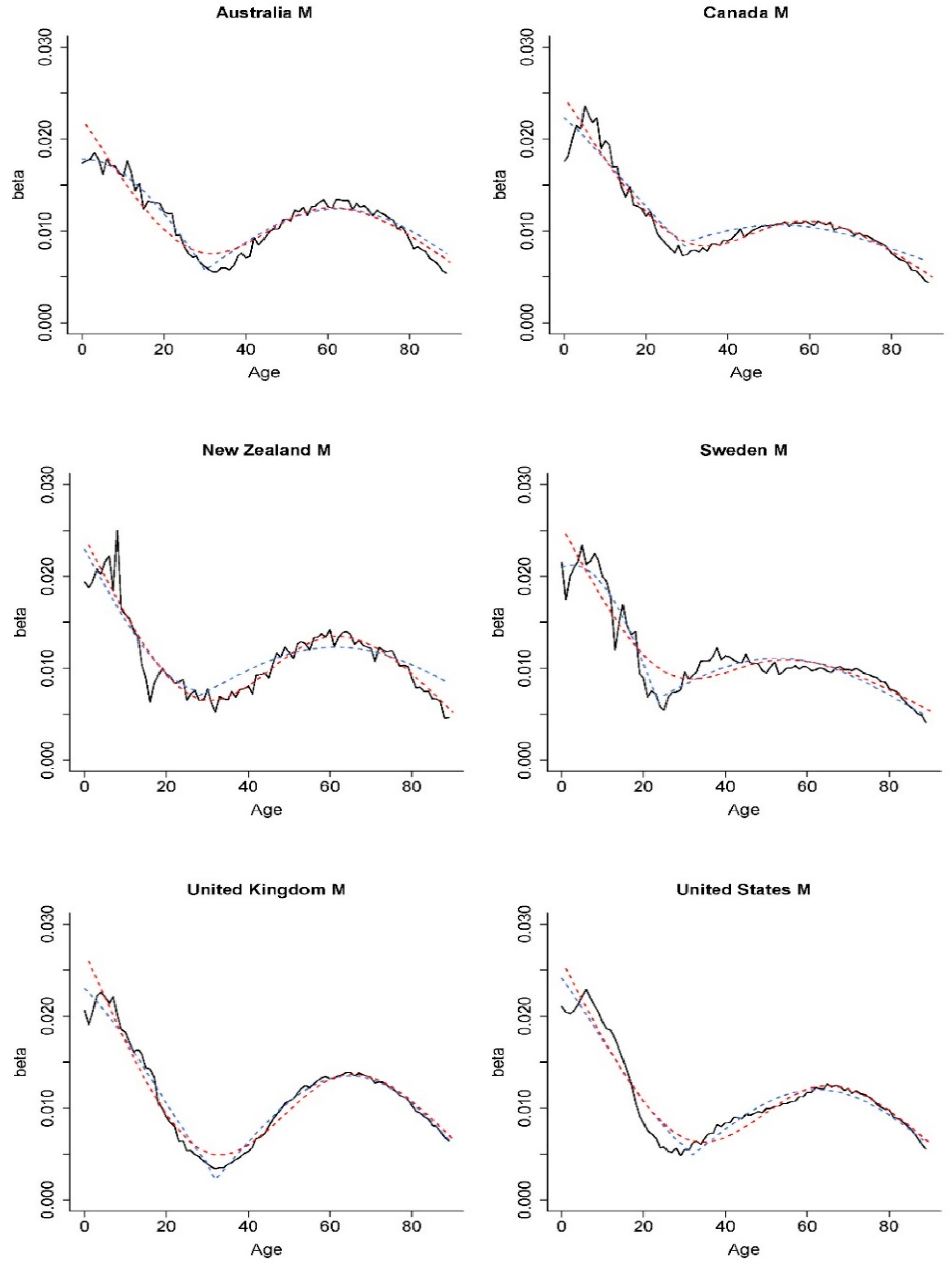
Figure 5 displays the estimated and fitted values of the age sensitivity parameter using the Fourier and cubic-spline approaches based on the mortality data of the latest 24-year subperiod. Both methods can capture the general shape of the age response. Unlike the Fourier approach, however, no meaningful interpretation was available for the coefficients of the cubic splines.
The primary purpose of introducing a time-varying age sensitivity parameter is to discover whether the age effects of structural changes in mortality can be modelled and predicted over time. We now examine and compare performances of the original Lee-Carter model, Fourier Lee-Carter model and cubic Lee-Carter model in the following sections.
5. Integrating the Age and Period Effects of Structural Changes
In this section, we examined the impact of incorporating the age and period effects of structural changes, either separately or simultaneously. Under the original Lee-Carter model, structural changes are often analyzed in the literature through the period effects. One needs to determine the dates of structural changes (breakpoints in the mortality index), then apply extended models such as the regime-switching model, broken-trend stationary model (time series process with piecewise-linear deterministic trends) and difference stationary model with breakpoints.
Coelho and Nunes (
2011) argued that the regime-switching model might not be appropriate because mortality reductions caused by medical advancement and healthcare improvements are unlikely to be reversed. They fitted the Lee-Carter model to each gender of eighteen populations with the mortality index modelled by a trend or difference stationary time series process and concluded that a difference stationary model was more suitable in the event of structural shifts. The main purpose of this section is to illustrate that the Lee-Carter model with time-varying age patterns can integrate both the age and period effects of structural changes. The impact of incorporating the period effects of structural changes is explored using the difference stationary model with one breakpoint in this paper
11. For demonstration purposes, we present our analysis based on male mortality data from the United Kingdom with the same fitting (1950–2001) and testing (2002–2016) periods as above.
Without considering potential breakpoints, the mortality index
can be modelled by a random walk with drift (RWD) as follows:
where
is the drift term, and
is the Gaussian error term with zero mean. The drift term is estimated by
which only depends on the starting and ending values of
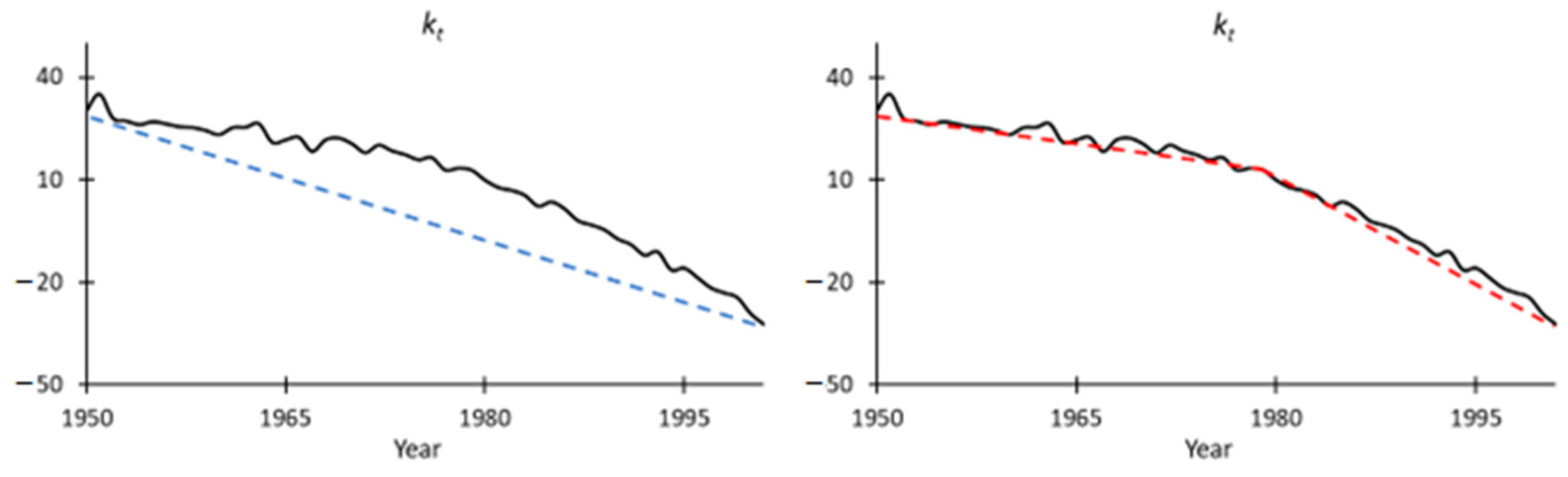
over the fitting period. However, as shown by the dashed lines in
Figure 8, the slope of the estimated mortality index actually became steeper since the middle of the fitting period. The estimate of the drift term over the whole period would then be too small to capture the future declining trend and underestimate future mortality improvements. In this case, a piecewise RWD might provide a better fit than a straight line (
van Berkum et al. 2013). The formula is expressed as follows:
where
,
is the date of the detected structural shift. Given the location of the breakpoint, we fit two RWD processes to the calibrated
values before and after the break date. Then the latter set of parameter estimates were employed to project future mortality scenarios. We used the
R package ‘
strucchange’ to identify the potential structural change for male mortality in the United Kingdom between 1950 and 2001. The structural change is detected in 1979, which is in accordance with the graphical observation. For more details of this modelling strategy, one may refer to
Section 3 of van
Berkum et al. (
2013) who investigated the period effects under various mortality models. The estimated value of
based on the whole fitting period is −1.35, and the
calculated using the latest period is −2.25.
In addition to the inclusion of a breakpoint, we applied the Fourier and cubic Lee-Carter models to incorporate time-varying age patterns. Then we followed the same strategies described in
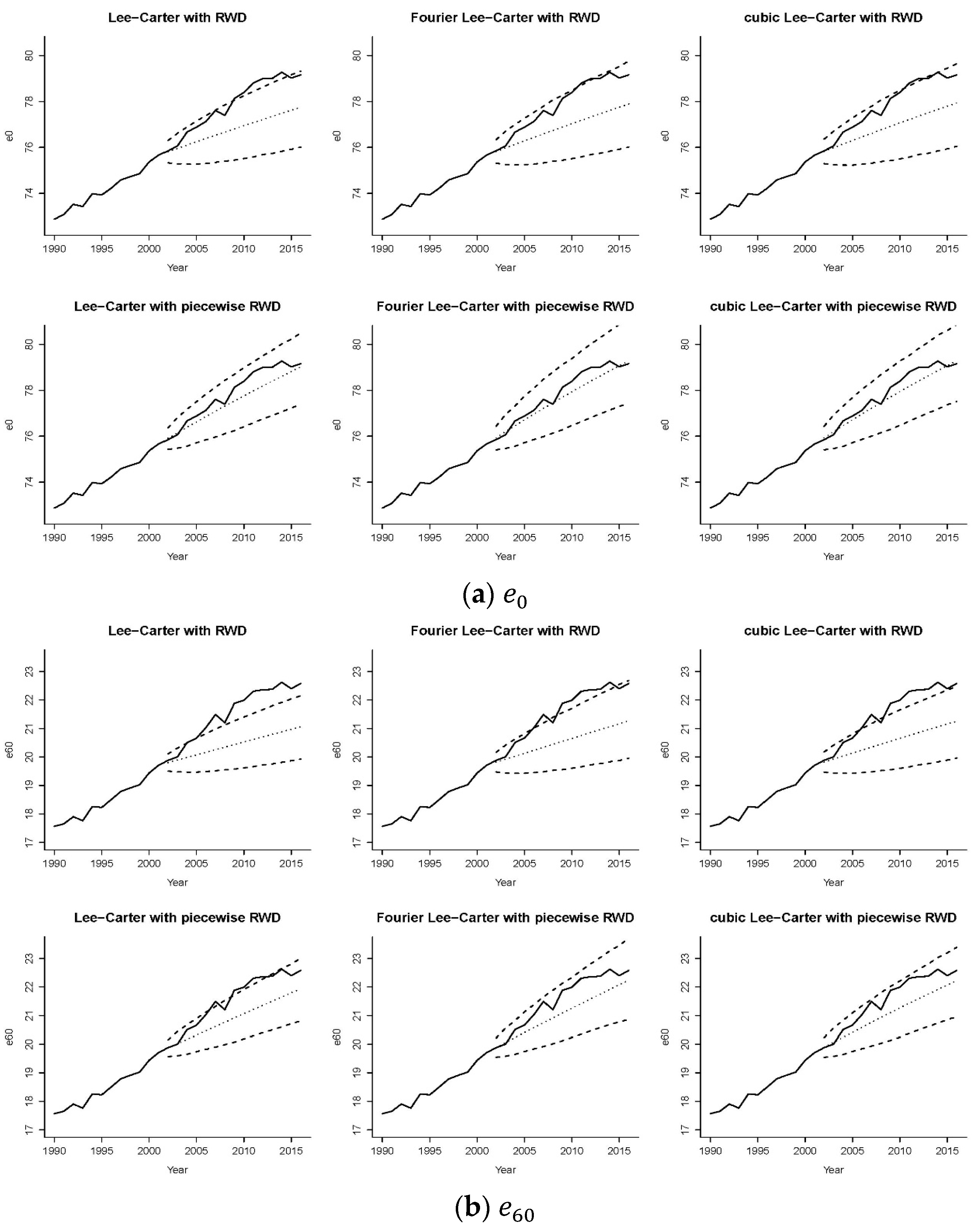
Section 4.2 to simulate future mortality scenarios over the testing period 2002–2016. We compared six sets of mortality forecasts simulated from (1) the Lee-Carter model with RWD, (2) the Fourier Lee-Carter model with RWD, (3) the cubic Lee-Carter model with RWD, (4) the Lee-Carter model with piecewise RWD, (5) the Fourier Lee-Carter model with piecewise RWD and (6) the cubic Lee-Carter model with piecewise RWD. The observed and projected life expectancies at birth and age 60 with 95% prediction intervals are displayed in
Figure 9.
There are some interesting observations to make on these diagrams. Comparing the graphs in each row, allowing for time-varying age effects with a Fourier pattern (middle column) tended to give the widest prediction intervals because the model had increasing uncertainty over time on both the mortality index and phase parameters. The projected life expectancy values under the original Lee-Carter model with RWD (the top left graph) showed an apparent deviation from historical data. The gap can be narrowed slightly by introducing a time-varying age effect. Comparing the graphs in each column, we saw that employing piecewise random walk processes could redirect the RWD projection to the ‘right’ trend, with the bottommost panels showing more accurate predictions of life expectancies at both ages 0 and 60 regarding the projected values and prediction intervals when the period effects of structural changes were incorporated. Considering the age effects (the top middle and top right figures) or time effects (the bottom left figure) of structural changes alone yielded better performance than the original Lee-Carter model (the top left figure) did. Furthermore, the integration of the two sources of structural changes (the bottom middle and bottom right figures) produced the best performance among these six models. The above observations held for life expectancies at both ages, although the age effects of structural changes appear to be more influential for older ages. Although employing a piecewise RWD was enough to properly predict
of British males (the bottom left graph of
Figure 9a), it failed to do so for
. As illustrated by the bottom panel of
Figure 9b, the prediction intervals could capture the realized trend of
only when both the age and period effects of structural changes were taken into account.
The proportions of observed life expectancies at ages 0 and 60 falling outside the prediction intervals under models (4)–(6) for the six countries are displayed in
Table 4. Comparing with the figures in
Table 3, incorporating the period effects of structural changes reduced the outliers of life expectancies at both ages by up to 75% and up to 67% under the Lee-Carter model with and without time-varying age patterns, respectively. One exception was the Canadian male life expectancy at age 60 under the original Lee-Carter model and the cubic Lee-Carter model whose forecasting errors reduced by 0%. The current results were mostly acceptable under the Fourier Lee-Carter model, especially for life expectancy at birth. With the integration of the two sources of structural changes, significant outliers of
were still observed in two out of the six cases. Among the two proposed approaches, the Fourier assumption generated better prediction intervals for
, with an improvement over the baseline model of 60% and 67% for Canada and the United States, respectively. This outperformance of the Fourier Lee-Carter model with piecewise RWD was possibly attributable to the unbounded variability assumed for the second phase parameter that was related to the age response at higher ages. Although one may adopt similar time series processes for the cubic-spline parameters, there is no practical interpretation of the cubic-spline coefficients and the choice of time series was hard to justify.
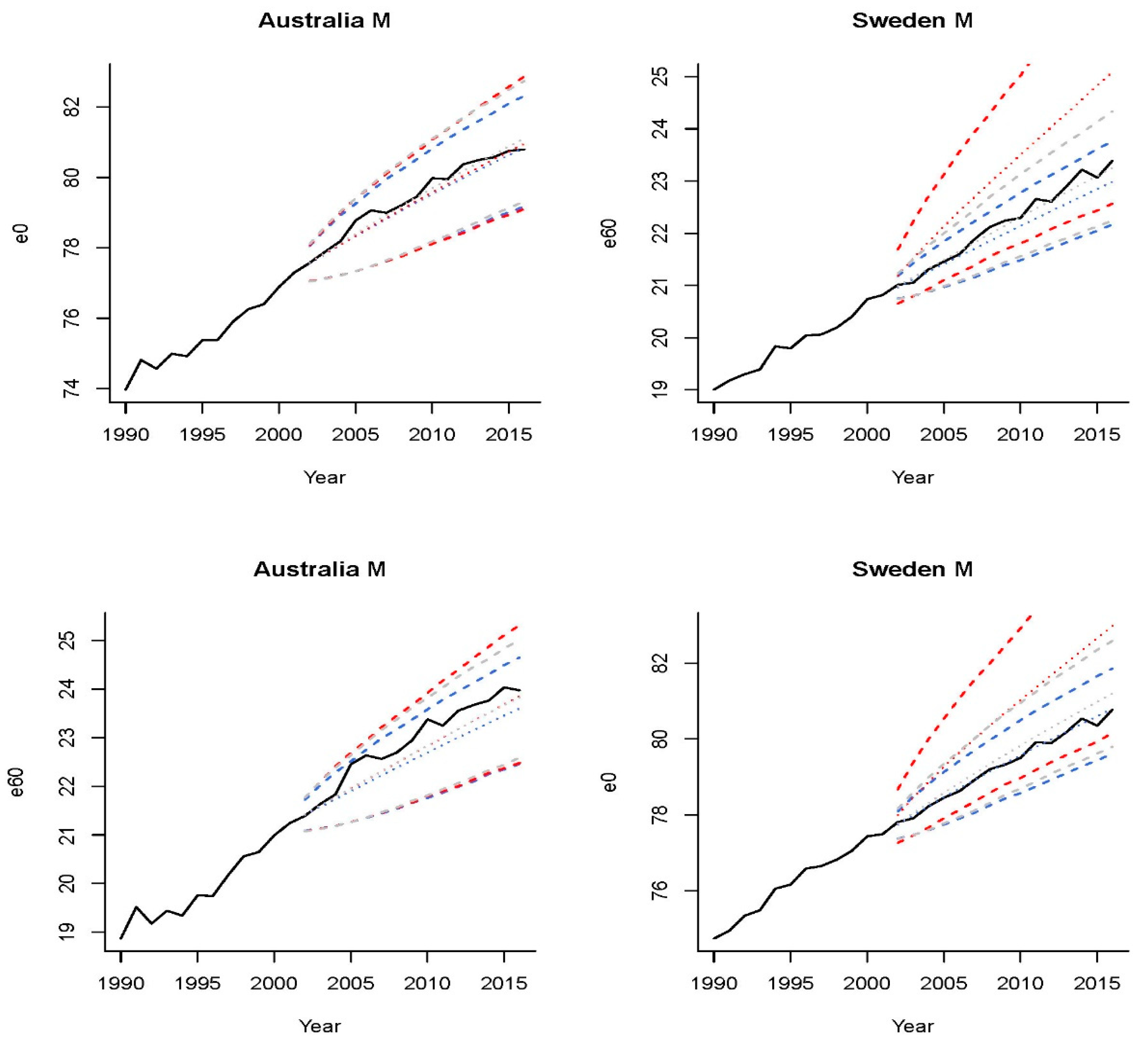
Recalling that
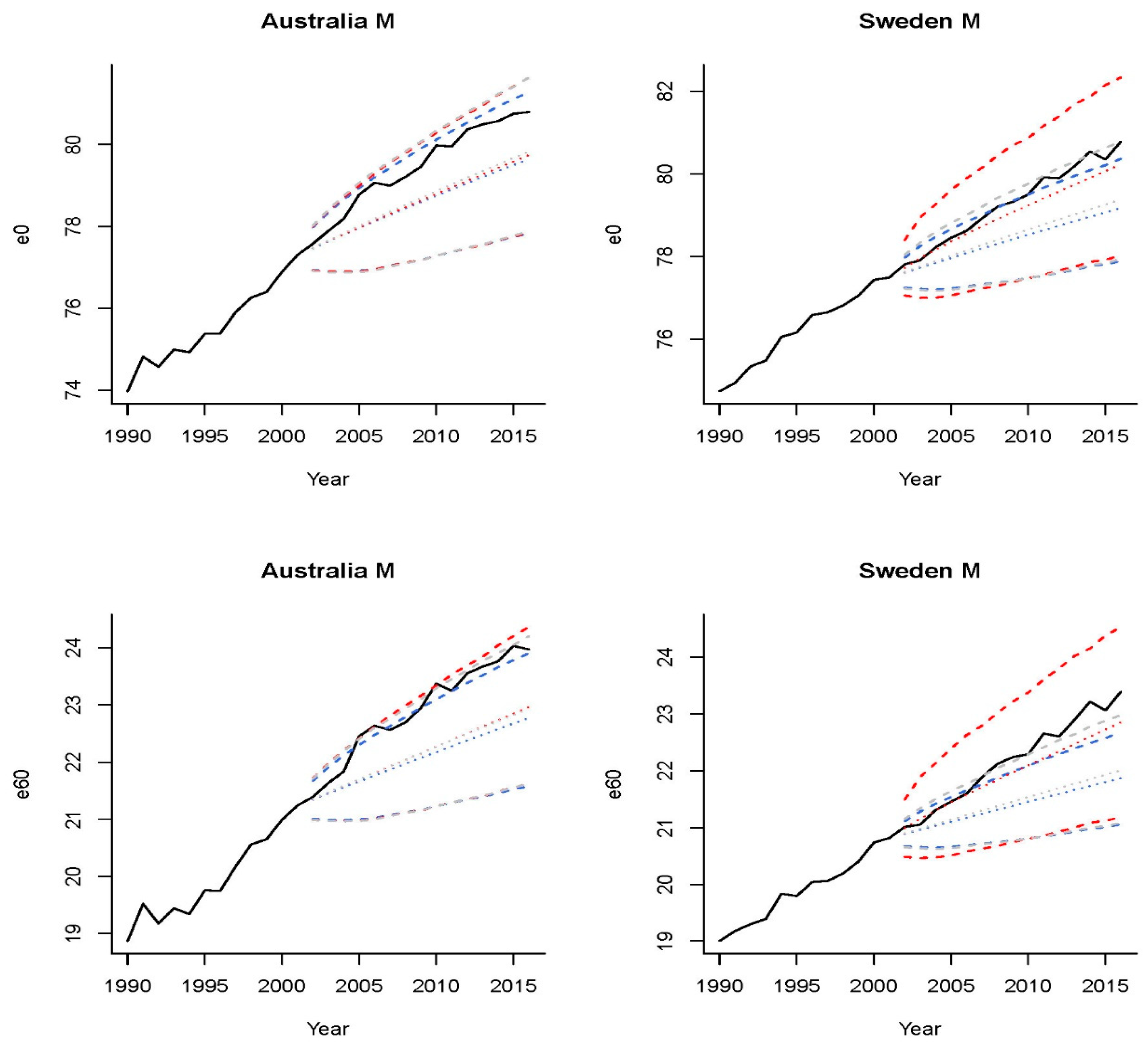
Figure 7 depicts two representative examples, Australia and Sweden, the three sets of projections for the former presented an evident deviation from the observed trend, although the Fourier method seemed to capture the trend of the latter. We plot in
Figure 10 the predicted life expectancies at age 0 and 60 of these two countries under the three mortality models with piecewise RWD. Interestingly, none of the historical
and
values of Swedish males fell outside the prediction intervals under the Fourier Lee-Carter model, both before and after introducing a piecewise RWD. As illustrated in the right column of
Figure 10, arbitrarily introducing the time effects of structural changes to the Fourier Lee-Carter model (red dotted lines) might make life expectancy projections deviate from the observed trend. The results for Swedish male mortality data suggested that incorporating the Fourier time-varying age patterns alone or using the piecewise RWD alone was sufficient for generating the prediction intervals.
In summary, this section demonstrates that structural changes could not only be reflected in the overall mortality reduction trends, but could also be in the sensitivity to those changes at different ages. Two mortality models were proposed to capture the time-varying patterns of the age effects by fitting a Fourier-like (cubic-spline) process to the age sensitivity parameters in the original Lee-Carter model. For the six datasets tested, allowing for either the time-varying age sensitivity or the mortality index with breakpoints tends to improve backtesting results, and the integration of these two approaches was superior for five out of the six countries in this case.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}