
Dental Caries, Oral Health Behavior, and Living Conditions in 6–8-Year-Old Romanian School Children

 ,
,  ,
,  , ,
, ,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
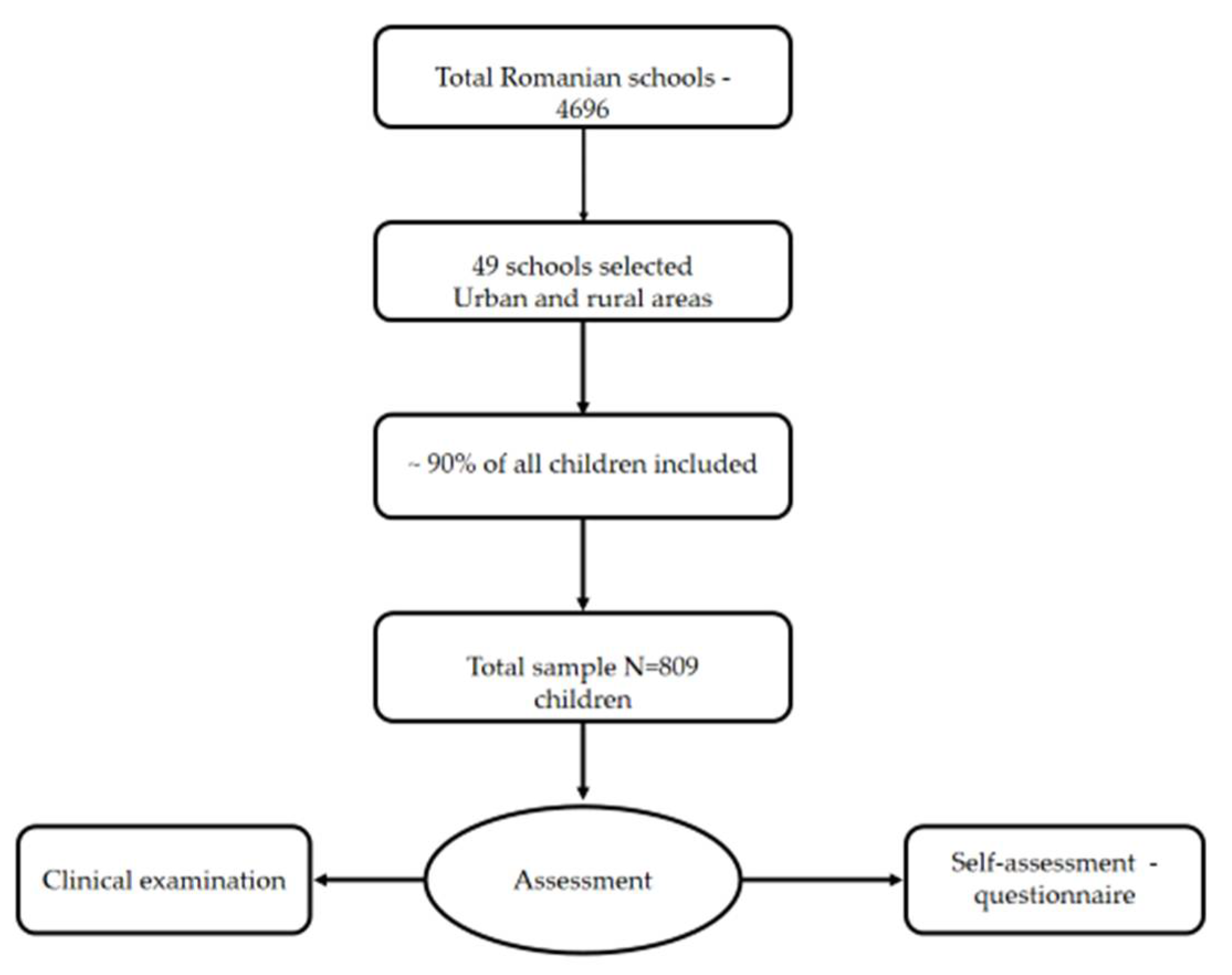
2.1. Study Design and Sample Selection
2.2. Clinical Examination
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2017 Oral Disorders Collaborators; Bernabe, E.; Marcenes, W.; Hernandez, C.R.; Bailey, J.; Abreu, L.G.; Alipour, V.; Amini, S.; Arabloo, J.; Arefi, Z.; et al. Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J. Dent. Res. 2020, 99, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Zhou, N.; Zhu, H.; Chen, Y.; Jiang, W.; Lin, X.; Tu, Y.; Chen, D.; Chen, H. Dental Caries and Associated Factors in 3 to 5-Year-Old Children in Zhejiang Province, China: An Epidemiological Survey. BMC Oral Health 2019, 19, 9. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The Global Burden of Oral Diseases and Risks to Oral Health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar] [CrossRef]
- Kwan, S.Y.L.; Petersen, P.E.; Pine, C.M.; Borutta, A. Health-Promoting Schools: An Opportunity for Oral Health Promotion. Bull. World Health Organ. 2005, 83, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Macey, R.; Walsh, T.; Riley, P.; Glenny, A.-M.; Worthington, H.V.; O’Malley, L.; Clarkson, J.E.; Ricketts, D. Visual or Visual-Tactile Examination to Detect and Inform the Diagnosis of Enamel Caries. Cochrane Database Syst. Rev. 2021, 2021, CD014546. [Google Scholar] [CrossRef]
- Banu, A.; Șerban, C.; Pricop, M.; Urechescu, H.; Vlaicu, B. Dental Health between Self-Perception, Clinical Evaluation and Body Image Dissatisfaction—A Cross-Sectional Study in Mixed Dentition Pre-Pubertal Children. BMC Oral Health 2018, 18, 74. [Google Scholar] [CrossRef]
- Smyth, E.; Caamano, F.; Fernández-Riveiro, P. Oral Health Knowledge, Attitudes and Practice in 12-Year-Old Schoolchildren. Med. Oral Patol. Oral Cir. Bucal 2007, 12, E614–E620. [Google Scholar]
- Petersen, P.E.; Kwan, S. Evaluation of Community-Based Oral Health Promotion and Oral Disease Prevention--WHO Recommendations for Improved Evidence in Public Health Practice. Community Dent. Health 2004, 21, 319–329. [Google Scholar]
- Zhu, L.; Petersen, P.E.; Wang, H.-Y.; Bian, J.-Y.; Zhang, B.-X. Oral Health Knowledge, Attitudes and Behaviour of Adults in China. Int. Dent. J. 2005, 55, 231–241. [Google Scholar] [CrossRef]
- Qiu, R.M.; Tao, Y.; Zhou, Y.; Zhi, Q.H.; Lin, H.C. The Relationship between Children’s Oral Health-Related Behaviors and Their Caregiver’s Social Support. BMC Oral Health 2016, 16, 86. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Divaris, K. The Ethical Imperative of Addressing Oral Health Disparities: A Unifying Framework. J. Dent. Res. 2014, 93, 224–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amin, T.; Al-Abad, B. Oral Hygiene Practices, Dental Knowledge, Dietary Habits and Their Relation to Caries among Male Primary School Children in Al Hassa, Saudi Arabia. Int. J. Dent. Hyg. 2008, 6, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Woodward, M.; Walker, A.R. Sugar Consumption and Dental Caries: Evidence from 90 Countries. Br. Dent. J. 1994, 176, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Alhabdan, Y.A.; Albeshr, A.G.; Yenugadhati, N.; Jradi, H. Prevalence of Dental Caries and Associated Factors among Primary School Children: A Population-Based Cross-Sectional Study in Riyadh, Saudi Arabia. Environ. Health Prev. Med. 2018, 23, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szöke, J.; Petersen, P.E. Evidence for Dental Caries Decline among Children in an East European Country (Hungary): Decline in Dental Caries in Hungarian Children. Community Dent. Oral Epidemiol. 2000, 28, 155–160. [Google Scholar] [CrossRef]
- Lin, Y.-T.; Chou, C.-C.; Lin, Y.-T.J. Caries Experience between Primary Teeth at 3–5 Years of Age and Future Caries in the Permanent First Molars. J. Dent. Sci. 2021, 16, 899–904. [Google Scholar] [CrossRef]
- Bhumireddy, J.; Nirmala, S.S.G.; Mallineni, S.; Nuvvula, S. Diagnostic Performance of the Visual Caries Classification of International Caries Detection and Assessment System II versus Conventional Radiography for the Detection of Occlusal Carious Lesions in Primary Molars. SRM J. Res. Dent. Sci. 2019, 10, 117. [Google Scholar] [CrossRef]
- dos Santos, N.M.; Leal, S.C.; Gouvea, D.B.; Sarti, C.S.; Toniolo, J.; Neves, M.; Rodrigues, J.A. Sealing of Cavitated Occlusal Carious Lesions in the Dentine of Deciduous Molars: A Two-Year Randomised Controlled Clinical Trial. Clin. Oral Investig. 2022, 26, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E.; Baez, R.J.; World Health Organization. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013; ISBN 978-92-4-154864-9. [Google Scholar]
- Raudenbush, S.W.; Bryk, A.S.; Cheong, Y.F.; Congdon, R.T.; DuToit, M. HLM7: Hierarchical Linear and Nonlinear Modeling; SSI, Scientific Software International: Skokie, IL, USA, 2011; ISBN 978-0-89498-057-2. [Google Scholar]
- Signori, C.; CaCIA Collaborative Group; Queiroz, A.B.L.; Avila, A.B.; Souza, B.O.; Signori, C.; Dias, C.R.; Becker, C.T.; Chaves, E.T.; Malhão, E.C.; et al. Comparison of Two Clinical Approaches Based on Visual Criteria for Secondary Caries Assessments and Treatment Decisions in Permanent Posterior Teeth. BMC Oral Health 2022, 22, 77. [Google Scholar] [CrossRef]
- Radić, M.; Benjak, T.; Dečković Vukres, V.; Rotim, Ž.; Filipović Zore, I. Presentation of DMF Index in Croatia and Europe. Acta Stomatol. Croat. 2015, 49, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Oulis, C.J.; Tsinidou, K.; Vadiakas, G.; Mamai-Homata, E.; Polychronopoulou, A.; Athanasouli, T. Caries Prevalence of 5, 12 and 15-Year-Old Greek Children: A National Pathfinder Survey. Community Dent. Health 2012, 29, 29–32. [Google Scholar] [PubMed]
- Lambert, M.J.; Vanobbergen, J.S.N.; Martens, L.C.; De Visschere, L.M.J. Socioeconomic Inequalities in Caries Experience, Care Level and Dental Attendance in Primary School Children in Belgium: A Cross-Sectional Survey. BMJ Open 2017, 7, e015042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwendicke, F.; Dörfer, C.E.; Schlattmann, P.; Page, L.F.; Thomson, W.M.; Paris, S. Socioeconomic Inequality and Caries: A Systematic Review and Meta-Analysis. J. Dent. Res. 2015, 94, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Poulton, R.; Caspi, A.; Milne, B.J.; Thomson, W.M.; Taylor, A.; Sears, M.R.; Moffitt, T.E. Association between Children’s Experience of Socioeconomic Disadvantage and Adult Health: A Life-Course Study. Lancet 2002, 360, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Listl, S.; Watt, R.G.; Tsakos, G. Early Life Conditions, Adverse Life Events, and Chewing Ability at Middle and Later Adulthood. Am. J. Public Health 2014, 104, e55–e61. [Google Scholar] [CrossRef]
- de Castilho, A.R.F.; Mialhe, F.L.; Barbosa, T.D.S.; Puppin-Rontani, R.M. Influence of Family Environment on Children’s Oral Health: A Systematic Review. J. Pediatr. (Rio J.) 2013, 89, 116–123. [Google Scholar] [CrossRef] [Green Version]
- Campus, G.; Cocco, F.; Strohmenger, L.; Cagetti, M.G. Caries Severity and Socioeconomic Inequalities in a Nationwide Setting: Data from the Italian National Pathfinder in 12-Years Children. Sci. Rep. 2020, 10, 15622. [Google Scholar] [CrossRef]
- Lewsey, J.D.; Thomson, W.M. The Utility of the Zero-Inflated Poisson and Zero-Inflated Negative Binomial Models: A Case Study of Cross-Sectional and Longitudinal DMF Data Examining the Effect of Socio-Economic Status. Community Dent. Oral Epidemiol. 2004, 32, 183–189. [Google Scholar] [CrossRef]
- Levin, K.A.; Davies, C.A.; Douglas, G.V.A.; Pitts, N.B. Urban-Rural Differences in Dental Caries of 5-Year Old Children in Scotland. Soc. Sci. Med. 2010, 71, 2020–2027. [Google Scholar] [CrossRef]
- Goldhagen, J.; Etzel, R.; Melinkovich, P. Council on Community Pediatrics and Committee on Native American Child Health Health Equity and Children’s Rights. Pediatrics 2010, 125, 838–849. [Google Scholar] [CrossRef] [Green Version]
- Levin, K.A.; Currie, C. Adolescent Toothbrushing and the Home Environment: Sociodemographic Factors, Family Relationships and Mealtime Routines and Disorganisation. Community Dent. Oral Epidemiol. 2010, 38, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.E.; Binkley, C.J.; Neace, W.P.; Gale, B.S. Barriers to Care-Seeking for Children’s Oral Health Among Low-Income Caregivers. Am. J. Public Health 2005, 95, 1345–1351. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | N (%) | Variables | N (%) |
|---|---|---|---|
| Gender | Father’s education | ||
| Male | 382 (47.22%) | No school | 19 (2.35%) |
| Female | 427 (52.78%) | Primary school (4th grade) | 30 (3.71%) |
| Age | Gymnasium (8th grade) | 109 (13.47%) | |
| 6 y.o. | 438 (54.14%) | Secondary school (10th grade) | 155 (19.16%) |
| 7 y.o. | 342 (42.27%) | High school (12th grade) | 226 (27.94%) |
| 8 y.o. | 22 (2.72%) | Post-secondary school | 24 (2.97%) |
| Did not declare | 7 (0.87%) | University studies | 203 (25.09%) |
| Residence | Do not know/Did not answer | 28 (3.46%) | |
| Rural area | 345 (42.65%) | Do not have a father figure | 15 (1.85%) |
| Urban area | 464 (57.35%) | Mother’s education | |
| City type | No school | 24 (2.97%) | |
| Small town | 520 (64.28%) | Primary school (4th grade) | 25 (3.09%) |
| Middle-sized city | 56 (6.92%) | Gymnasium (8th grade) | 107 (13.23%) |
| Big city | 233 (28.80%) | Secondary school (10th grade) | 124 (15.33%) |
| High school (12th grade) | 204 (25.22%) | ||
| Post-secondary school | 49 (6.06%) | ||
| University studies | 256 (31.64%) | ||
| Do not know/Did not answer | 18 (12.22%) | ||
| Do not have a mother figure | 2 (0.25%) |
| Occurrence vs. 0. Non-Ocurrence of Carious Lesions (Multilevel Logistic Regression Bernouli Estimations) | ||||
|---|---|---|---|---|
| mt | d3t | rt | DMFT | |
| Individual-Level Variables | ||||
| Gender (−1 boy, 1—girl) | −0.01 (0.20) | −0.01 (0.16) | −0.03 (0.17) | −0.10 (0.20) |
| Father’s level of education | −0.10 (0.06) | −0.31 ** (0.05) | 0.08 (0.06) | −0.33 ** (0.06) |
| Mother’s level of education | −0.07 (0.07) | −0.29 ** (0.06) | 0.22 ** (0.06) | −0.25 ** (0.07) |
| How often cleans teeth (0—“never”) | 0.62 (0.09) | −0.23 ** (0.08) | 0.14 (0.09) | −0.15 (0.10) |
| Fruit consumption (0—“never”) | −0.10 (0.11) | 0.16 (0.09) | 0.14 (0.10) | 0.13 (0.12) |
| Pastry (0—“never”) | 0.24 * (0.12) | 0.05 (0.09) | −0.22 (0.10) | 0.14 (0.12) |
| Fizzy drinks (0—“never”) | 0.10 (0.09) | 0.18 * (0.07) | −0.15 (0.08) | 0.07 (0.09) |
| Honey (0—“never”) | 0.12 (0.09) | 0.02 (0.07) | −0.06 (0.08) | 0.01 (0.09) |
| Chewing gum (0—“never”) | −0.01 (0.09) | 0.22 * (0.08) | −0.14 (0.09) | 0.17 (0.10) |
| Candies (0—“never”) | 0.15 (0.09) | 0.26 * (0.08) | −0.09 (0.08) | 0.19 * (0.09) |
| Milk (0—“never”) | −0.03 (0.08) | 0.16 * (0.07) | −0.09 (0.07) | 0.12 (0.08) |
| Tea (0—“never”) | −0.01 (0.09) | 0.21 * (0.08) | 0.08 (0.09) | 0.18 (0.10) |
| Cocoa (0—“never”) | −0.02 (0.10) | 0.11 (0.08) | −0.01 (0.09) | 0.−10 (0.10) |
| School-level variables | ||||
| Type of residence (−1 Rural, 2 Urban) | 0.22 (0.35) | −0.57 (0.22) | 10.0 * (0.35) | −0.54 ** (0.25) |
| Development index (County, centered on the mean) | −0.01 (0.01) | −0.01 (0.00) | 0.02 (0.01) | −0.00 (0.01) |
| Poisson Analysis—Regressions of Non-Zero Count | |||
|---|---|---|---|
| d3t | rt | DMFT | |
| Individual-level variables | |||
| Gender (−1 boy, 1—girl) | −0.16 ** (0.02) | 0.14 (0.07) | −0.06 * (0.03) |
| Father’s level of education | −0.06 ** (0.00) | 0.08 ** (0.02) | −0.04 ** (0.01) |
| Mother’s level of education | −0.05 ** (0.01) | 0.14 ** (0.03) | −0.03 ** (0.01) |
| How often cleans teeth (0—“never”) | −0.03 * (0.01) | 0.14 ** (0.04) | −0.02 (0.01) |
| Fruit consumption (0—“never”) | 0.03 ** (0.01) | 0.03 (0.05) | 0.04 * (0.01) |
| Pastry (0—“never”) | 0.02 * (0.01) | −0.05 (0.048) | 0.02 (0.019) |
| Fizzy drinks (0—“never”) | 0.033 ** (0.01) | −0.20 ** (0.04) | 0.03 ** (0.01) |
| Honey (0—“never”) | 0.02 * (0.01) | 0.09 * (0.04) | 0.03 * (0.01) |
| Chewing gum (0—“never”) | −0.03 ** (0.01) | −0.16 ** (0.04) | 0.00 (0.00) |
| Candies (0—“never”) | −0.01 (0.01) | −0.07 (0.04) | 0.03 (0.01) |
| Milk (0—“never”) | 0.03 ** (0.01) | −0.06 (0.03) | 0.05 ** (0.01) |
| Tea (0—“never”) | 0.04 ** (0.01) | −0.00 (0.04) | 0.05 ** (0.01) |
| Cocoa (0—“never”) | 0.05 ** (0.01) | −0.09 * (0.04) | 0.04 * (0.01) |
| School-level variables | |||
| Typeof residence (−1 Rural, 2 Urban) | −0.18 (0.11) | −0.04 (0.12) | −00.04 (0.07) |
| Development index (County, centered on the mean) | −0.00 (0.00) | 0.00 (0.00) | −0.00 (0.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dumitrescu, R.; Sava-Rosianu, R.; Jumanca, D.; Balean, O.; Damian, L.-R.; Campus, G.G.; Maricutoiu, L.; Alexa, V.T.; Sfeatcu, R.; Daguci, C.; et al. Dental Caries, Oral Health Behavior, and Living Conditions in 6–8-Year-Old Romanian School Children. Children 2022, 9, 903. https://doi.org/10.3390/children9060903
Dumitrescu R, Sava-Rosianu R, Jumanca D, Balean O, Damian L-R, Campus GG, Maricutoiu L, Alexa VT, Sfeatcu R, Daguci C, et al. Dental Caries, Oral Health Behavior, and Living Conditions in 6–8-Year-Old Romanian School Children. Children. 2022; 9(6):903. https://doi.org/10.3390/children9060903
Chicago/Turabian StyleDumitrescu, Ramona, Ruxandra Sava-Rosianu, Daniela Jumanca, Octavia Balean, Lia-Raluca Damian, Guglielmo Giuseppe Campus, Laurentiu Maricutoiu, Vlad Tiberiu Alexa, Ruxandra Sfeatcu, Constantin Daguci, and et al. 2022. "Dental Caries, Oral Health Behavior, and Living Conditions in 6–8-Year-Old Romanian School Children" Children 9, no. 6: 903. https://doi.org/10.3390/children9060903
APA StyleDumitrescu, R., Sava-Rosianu, R., Jumanca, D., Balean, O., Damian, L.-R., Campus, G. G., Maricutoiu, L., Alexa, V. T., Sfeatcu, R., Daguci, C., Postolache, M., & Galuscan, A. (2022). Dental Caries, Oral Health Behavior, and Living Conditions in 6–8-Year-Old Romanian School Children. Children, 9(6), 903. https://doi.org/10.3390/children9060903