
Antimicrobial Stewardship Improvement in Pediatric Intensive Care Units in Spain—What Have We Learned?

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Definitions
2.2. Outcome
2.3. Variables
2.4. Statistical Analysis
3. Results
3.1. Patients and Clinical Characteristics
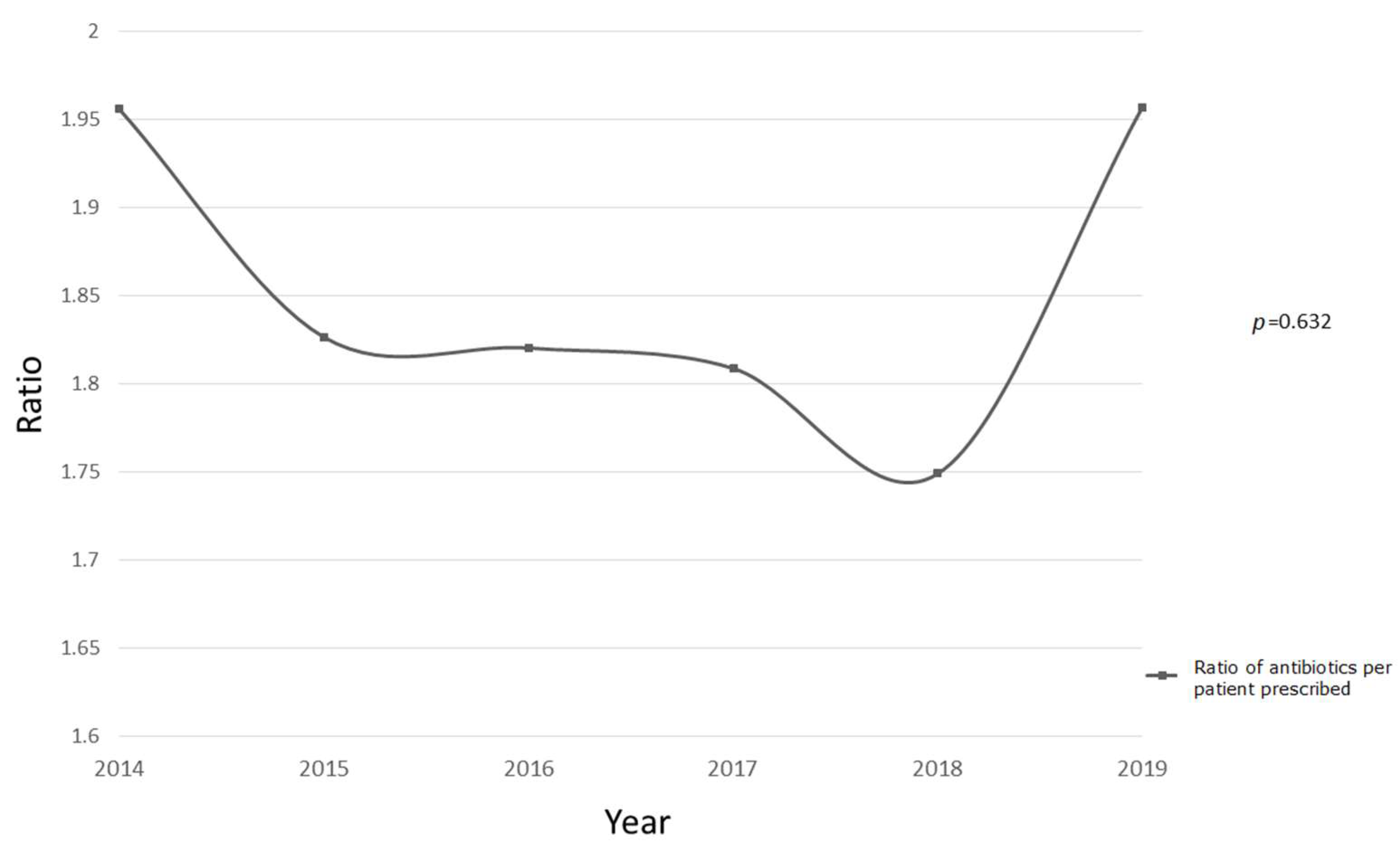
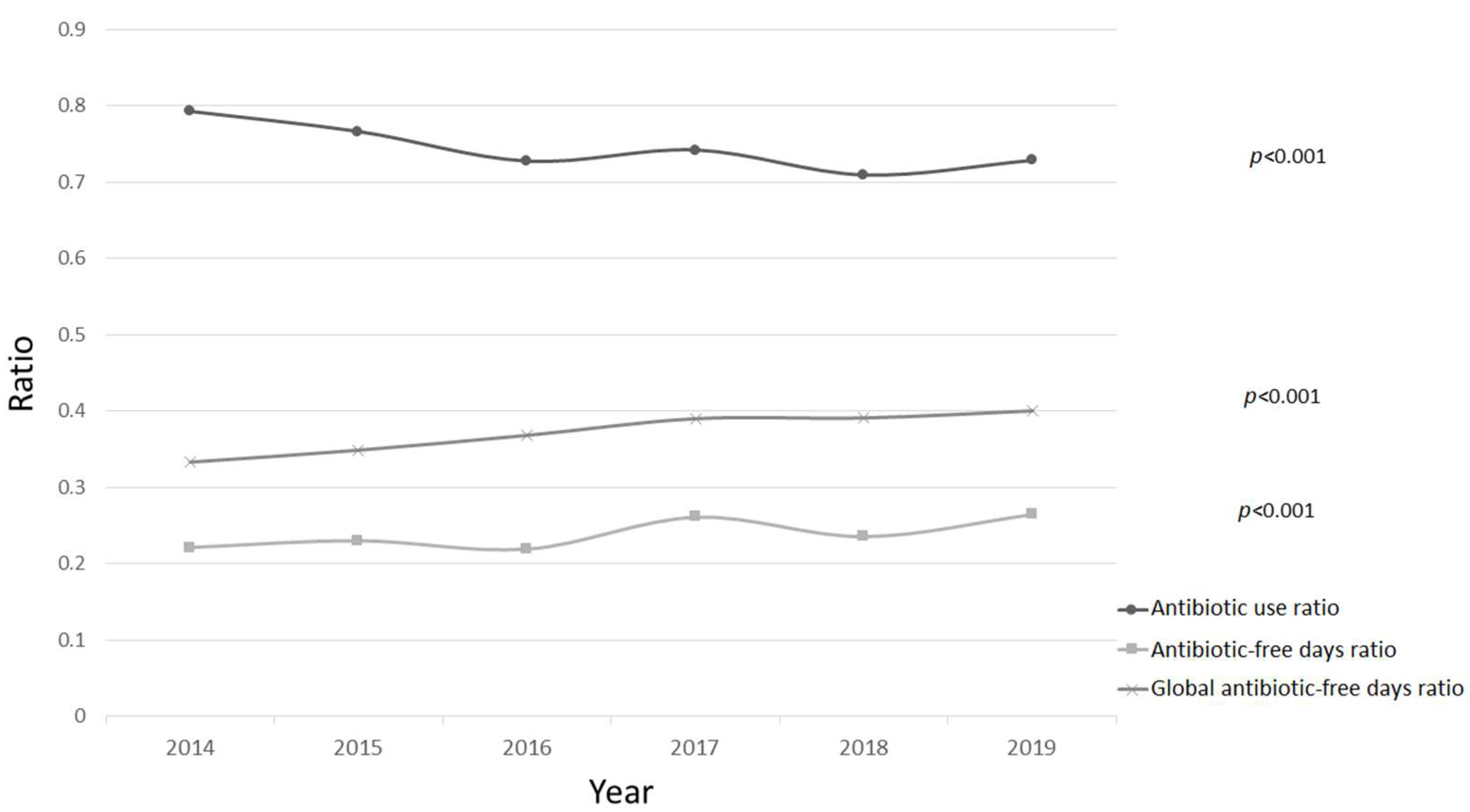
3.2. General Use of Antibiotics
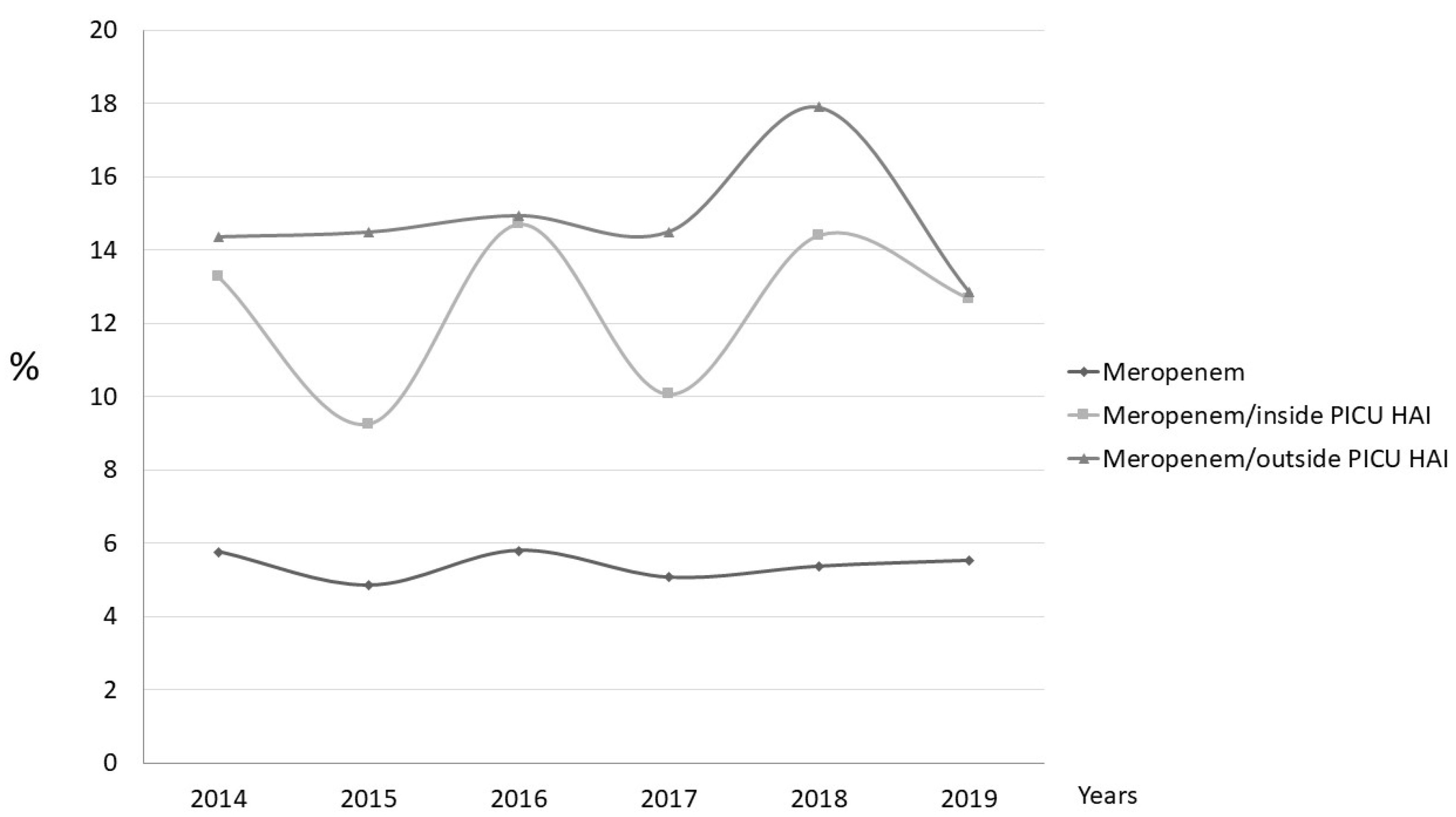
3.3. Types of Antibiotics Prescribed
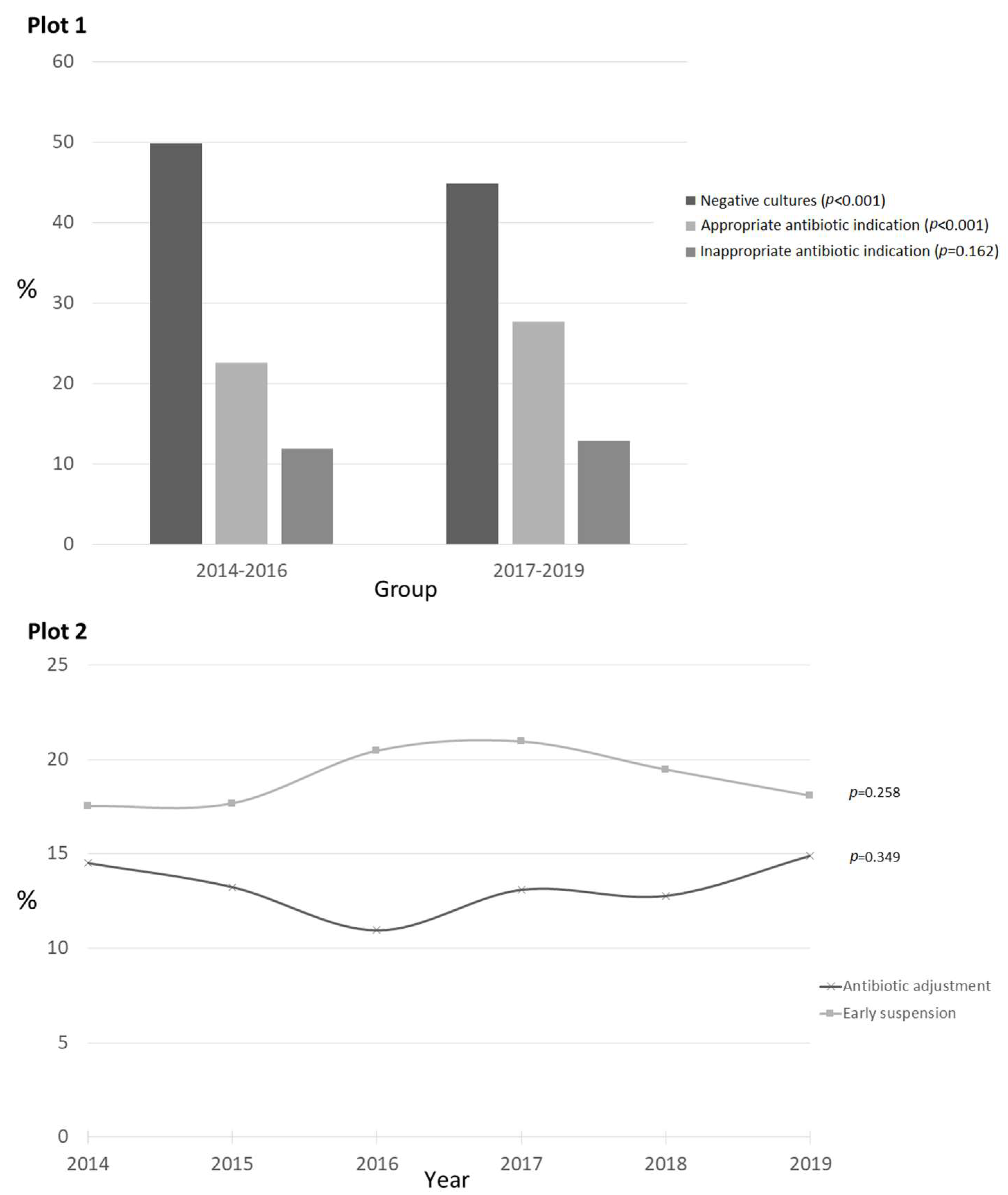
3.4. Empirical Use of Antibiotics in Suspected Infections
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Armstrong, G.L.; Conn, L.A.; Pinner, R.W. Trends in Infectious Disease Mortality in the United States During the 20th Century. J. Am. Med. Assoc. 1999, 281, 61–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antão, E.M.; Wagner-Ahlfs, C. Antibiotic resistance: A challenge for society. Bundesgesundheitsblatt Gesundh. Gesundh. 2018, 61, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Baño, J.; Paño-Pardo, J.R.; Alvarez-Rocha, L.; Asensio, Á.; Calbo, E.; Cercenado, E.; Cisneros, J.M.; Cobo, J.; Delgado, O.; Garnacho-Montero, J.; et al. Programas de optimización de uso de antimicrobianos (PROA) en hospitales españoles: Documento de consenso GEIH-SEIMC, SEFH y SEMPSPH. Enferm. Infecc. Microbiol. Clin. 2012, 30, 22.e1–22.e23. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.; Ramirez, P.; Gordon, M.; Villarreal, E.; Frasquet, J.; Poveda-Andres, J.; Salavert-Lletí, M.; Catellanos, A. Antimicrobial stewardship programme in critical care medicine: A prospective interventional study. Med. Intensiv. 2018, 42, 266–273. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Core Elements of Hospital Antibiotic Stewardship Programs. US Dep. Health Hum. Serv. CDC 2019. Available online: https://www.cdc.gov/antibiotic-use/core-elements/hospital.html (accessed on 11 April 2020).
- Tiszai-Szucs, T.; Mac Sweeney, C.; Keaveny, J.; Bozza, F.A.; Hagan, Z.O.; Martin-Loeches, I. Feasibility of Antimicrobial Stewardship (AMS) in Critical Care Settings: A Multidisciplinary Approach Strategy. Med Sci. 2018, 6, 40. [Google Scholar] [CrossRef] [Green Version]
- Velasco-Arnaiz, E.; Simó-Nebot, S.; Ríos-Barnés, M.; López Ramos, M.G.L.; Monsonís, M.; Urrea-Ayala, M.; Jordan, I.; Mas-Comas, A.; Casadevall-Llandrich, R.; Ormazábal-Kirchner, D.; et al. Benefits of a Pediatric Antimicrobial Stewardship Program in Antimicrobial Use and Quality of Prescriptions in a Referral Children’s Hospital. J. Pediatr. 2020, 225, 222–230.e1. [Google Scholar] [CrossRef]
- Newland, J.G.; Hersh, A.L. Purpose and Design of Antimicrobial Stewardship Programs in Pediatrics. Pediatr. Infect. Dis. J. 2010, 29, 862–863. [Google Scholar] [CrossRef] [Green Version]
- Navas, A.L. Informe Anual PRAN. Junio 2019—Junio 2020. 2020, p. 38. Available online: https://resistenciaantibioticos.es/es/system/files/field/files/informe_anual_pran_2019_2020_0.pdf?file=1&type=node&id=577&force=0 (accessed on 8 August 2020).
- Hospital in Europe Link for Infection Control through Surveillance. Surveillance of Nosocomial Infections in Intensive Care Units Protocol 6.1. Eur. Cent. Dis. Control. 2004, 1, 1–51. Available online: https://www.sicsag.scot.nhs.uk/hai/helics_protocol.pdf (accessed on 17 October 2019).
- SEMICYUC. MANUAL DE “ESTUDIO NACIONAL DE VIGILANCIA DE INFECCIÓN NOSOCOMIAL EN UCI” (ENVIN- HELICS) Abril de 2016 Grupo de Trabajo de Enfermedades Infecciosas y Sepsis de SEMICYUC. 2016. Available online: https://hws.vhebron.net/envin-helics/Help/Manual_2020.pdf (accessed on 20 November 2019).
- Jordan Garcia, I.; Esteban Torné, E.; Bustinza Arriortua, A.; de Carlos Vicente, J.C.; García Soler, P.; Concha Torre, J.A.; Flores González, J.C.; Madurga Revilla, P.; Palomar Martínez, M.; VINCIP Study Group. Trends in nosocomial infections and multidrug-resistant microorganisms in Spanish pediatric intensive care units. Enferm. Infecc. Microbiol. Clin. 2016, 34, 286–292. [Google Scholar] [CrossRef]
- Briassoulis, P.; Briassoulis, G.; Christakou, E.; Machaira, M.; Kassimis, A.; Barbaressou, C.; Nikolaou, F.; Sdougka, M.; Gikas, A.; Ilia, S. Active Surveillance of Healthcare-associated Infections in Pediatric Intensive Care Units: Multicenter ECDC HAI-net ICU protocol (v2.2) implementation, antimicrobial resistance and challenges: Multicenter ECDC HAI-net ICU protocol (v2.2) implementation, antimicrobial resistance and challenges. Pediatr. Infect. Dis. J. 2021, 40, 231–237. [Google Scholar] [CrossRef]
- Elnasser, Z.; Obeidat, H.; Amarin, Z. Device-related infections in a pediatric intensive care unit: The Jordan University of Sci-ence and Technology experience. Medicine (Baltimore). Medicine 2021, 100, e27651. [Google Scholar] [CrossRef] [PubMed]
- Gould, C.V.; Umscheid, C.A.; Agarwal, R.K.; Kuntz, G.; Pegues, D.A.; the Healthcare Infection Control Practices Advisory Committee (HICPAC). Guideline for Prevention of Catheter-associated Urinary Tract Infections 2009. Guidel. Prev. Catheter Urin. Tract. Infect. 2019, 1–61. Available online: https://www.cdc.gov/infectioncontrol/pdf/guidelines/cauti-guidelines-H.pdf (accessed on 7 July 2019).
- O’Grady, N.P.; Alexander, M.; Burns, L.A.; Dellinger, E.P.; Garland, J.; Heard, S.O.; Lipsett, P.A.; Masur, H.; Mermel, L.A.; Pearson, M.L.; et al. Guideline Intravascular Catheter-Related Infection, 2011. Cent. Dis. Control Prev. 2017, 1–80. Available online: https://www.cdc.gov/infectioncontrol/pdf/guidelines/bsi-guidelines-H.pdf (accessed on 18 January 2018).
- Grant, M.J.; Hardin-Reynolds, T. Preventable Health Care–Associated Infections in Pediatric Critical Care. J. Pediatr. Intensiv. Care 2015, 4, 079–086. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Surveillance of Healthcare-Associated Infections and Prevention Indicators in European Intensive Care Units—HAI-Net ICU Protocol Version 2.2; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2017; pp. 1–55. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/HAI-Net-ICU-protocol-v2.2_0.pdf (accessed on 18 February 2018).
- Gerber, J.S.; Newland, J.G.; Hall, M.; Thurm, C.; Prasad, P.A.; Feudtner, C.; Zaoutis, T.E. Variability in Antibiotic Use at Children’s Hospitals Throughout the United States HHS Public Access. Pediatrics 2010, 126, 1067–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Versporten, A.; Bielicki, J.; Drapier, N.; Sharland, M.; Goossens, H.; Calle, G.M.; Garrahan, J.P.; Clark, J.; Cooper, C.; Blyth, C.C.; et al. The Worldwide Antibiotic Resistance and Prescribing in European Children (ARPEC) point prevalence survey: Developing hospital-quality indicators of antibiotic prescribing for children. J. Antimicrob. Chemother. 2016, 71, 1106–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Araujo da Silva, A.R.; Albernaz de Almeida Dias, D.C.; Marques, A.F.; Biscaia di Biase, C.; Murni, I.K.; Dramowski, A.; Sharland, M.; Huebner, J.; Zingg, W. Role of antimicrobial stewardship programmes in children: A systematic review. J. Hosp. Infect. 2018, 99, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Ansari, F.; Erntell, M.; Goossens, H.; Davey, P. The European Surveillance of Antimicrobial Consumption (ESAC) Point-Prevalence Survey of Antibacterial Use in 20 European Hospitals in 2006. Clin. Infect. Dis. 2009, 49, 1496–1504. [Google Scholar] [CrossRef]
- Amadeo, B.; Zarb, P.; Muller, A.; Drapier, N.; Vankerckhoven, V.; Rogues, A.-M.; Davey, P.; Goossens, H.; on behalf of the ESAC III Hospital Care Subproject Group. European Surveillance of Antibiotic Consumption (ESAC) point prevalence survey 2008: Paediatric antimicrobial prescribing in 32 hospitals of 21 European countries. J. Antimicrob. Chemother. 2010, 65, 2247–2252. [Google Scholar] [CrossRef] [Green Version]
- Di Pentima, M.C.; Chan, S.; Hossain, J. Benefits of a pediatric antimicrobial stewardship program at a children’s hospital. Pediatrics 2011, 128, 1062–1070. [Google Scholar] [CrossRef]
- Renk, H.; Sarmisak, E.; Spott, C.; Kumpf, M.; Hofbeck, M.; Hölzl, F. Antibiotic stewardship in the PICU: Impact of ward rounds led by paediatric infectious diseases specialists on antibiotic consumption. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Guo, Y.; Gao, W.; Yang, H.; Ma, C.; Sui, S. De-escalation of empiric antibiotics in patients with severe sepsis or septic shock: A meta-analysis. Heart Lung J. Acute Crit. Care 2016, 45, 454–459. [Google Scholar] [CrossRef]
- Battula, V.; Krupanandan, R.K.; Nambi, P.S.; Ramachandran, B. Safety and Feasibility of Antibiotic De-escalation in Critically Ill Children With Sepsis—A Prospective Analytical Study From a Pediatric ICU. Front. Pediatr. 2021, 9, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Al-Omari, A.; Al Mutair, A.; Alhumaid, S.; Salih, S.; Alanazi, A.; Albarsan, H.; AbouRayan, M.; Al Subaie, M. The impact of antimicrobial stewardship program implementation at four tertiary private hospitals: Results of a five-years pre-post analysis. Antimicrob. Resist. Infect. Control 2020, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- García-Rodríguez, J.F.; Bardán-García, B.; Peña-Rodríguez, M.F.; Álvarez-Díaz, H.; Mariño-Callejo, A. Meropenem antimicrobial stewardship program: Clinical, economic, and antibiotic resistance impact. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.J.; Gerber, J.S.; Hersh, A.L. Inpatient Antimicrobial Stewardship in Pediatrics: A Systematic Review. J. Pediatr. Infect. Dis. Soc. 2015, 4, e127–e135. [Google Scholar] [CrossRef] [Green Version]
- Adams, S.M.; Ngo, L.; Morphew, T.; Babbitt, C.J. Does an Antimicrobial Time-Out Impact the Duration of Therapy of Antimicrobials in the PICU? Pediatr. Crit. Care Med. 2019, 20, 560–567. [Google Scholar] [CrossRef]
- Aizawa, Y.; Suwa, J.; Higuchi, H.; Fukuoka, K.; Furuichi, M.; Kaneko, T.; Morikawa, Y.; Okazaki, K.; Shimizu, N.; Horikoshi, Y. Antimicrobial Stewardship Program in a Pediatric Intensive Care Unit. J. Pediatr. Infect. Dis. Soc. 2018, 7, e156–e159. [Google Scholar] [CrossRef]
- Cook, P.P.; Catrou, P.G.; Christie, J.D.; Young, P.D.; Polk, R.E. Reduction in broad-spectrum antimicrobial use associated with no improvement in hospital antibiogram. J. Antimicrob. Chemother. 2004, 53, 853–859. [Google Scholar] [CrossRef] [Green Version]
- Talpaert, M.J.; Rao, G.G.; Cooper, B.S.; Wade, P. Impact of guidelines and enhanced antibiotic stewardship on reducing broad-spectrum antibiotic usage and its effect on incidence of Clostridium difficile infection. J. Antimicrob. Chemother. 2011, 66, 2168–2174. [Google Scholar] [CrossRef] [Green Version]
- Aldeyab, M.A.; Kearney, M.P.; Scott, M.G.; Aldiab, M.A.; Alahmadi, Y.M.; Elhajji, F.W.D.; Magee, F.A.; McElnay, J.C. An evaluation of the impact of antibiotic stewardship on reducing the use of high-risk antibiotics and its effect on the incidence of Clostridium difficile infection in hospital settings. J. Antimicrob. Chemother. 2012, 67, 2988–2996. [Google Scholar] [CrossRef] [Green Version]
- Fishman, N. Antimicrobial Stewardship. Am. J. Med. 2006, 119 (Suppl. S1), 53–61. [Google Scholar] [CrossRef]
- Dellit, T.H. Summary of the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America Guidelines for Developing an Institutional Program to Enhance Antimicrobial Stewardship. Infect. Dis. Clin. Pract. 2007, 15, 263–264. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Infection | Definition |
|---|---|
| Central line-associated bloodstream infection (CLABSI) | Primary blood stream infection (no other apparent source of infection) and positive blood cultures, all involving the same microorganism, fulfilling one of the following situations: Quantitative central venous catheter (CVC) culture ≥103 CFU/mL; Quantitative blood culture ratio CVC blood sample/peripheral blood sample >5; Differential delay in positivity of blood cultures: CVC blood sample culture positive two hours or more before peripheral blood culture; Positive culture with the same microorganism found in pus at insertion site. |
| Ventilator-associated pneumonia (VAP) | A. Clinical diagnosis: Presence of a new and persistent pulmonary infiltrate on one chest X-ray or CT scan in a previously healthy patient; OR Two or more images suggestive of pneumonia in patients with underlying heart or lung disease; AND at least one of the following: Fever ≥ 38 °C with no other discernable cause; Leukopenia (<4000 WBC/mm3) or leukocytosis (≥12,000 WBC/mm3); AND at least one of the following (or at least two, if clinical pneumonia only): Increased respiratory secretions, change in previous characteristics of sputum, or sputum with purulent appearance; New onset of cough, dyspnea, and/or tachypnea; Abnormal lung sounds, such as crackles, bronchial breath, wheezing; Increased oxygen requirements or ventilatory demand; AND, depending on the diagnostic method used: B. Bacteriological diagnosis: (PN1). Positive quantitative culture from a minimally contaminated specimen: Bronchoalveolar lavage (BAL) with a threshold of ≥1 × 104 colony-forming units (CFU)/mL or ≥5% of BAL-obtained cells containing intracellular bacteria upon direct microscope exam; Protected specimen brush or protected distal aspirate, with a threshold of ≥1 × 103 CFU/mL; (PN2). Positive quantitative culture from a possibly contaminated specimen: Quantitative culture from an endotracheal aspirate with a threshold of ≥1 × 106 CFU/mL; (PN3). Alternative microbiological methods: Positive blood culture not related to another source of infection; Positive growth in pleural fluid culture; Pleural or pulmonary abscess, with positive needle aspiration; Histological evidence of pneumonia; Positive detection of viral antigen or antibodies in respiratory secretions; Seroconversion; or Detection of viral antigen in urine; (PN4). Positive sputum culture or non-quantitative specimen culture; (PN5). No positive microbiology. |
| Catheter-associated urinary tract infections (CAUTI) | Defined in a patient who has at least one of the following symptoms, with no other recognized cause: Fever >38 °C, increased urgency and/or frequency, dysuria, or suprapubic tenderness; Pyuria in urine specimen, with ≥10 WBC/mL or ≥3 WBC/high-power field of unspun urine; AND Positive urine culture with a threshold of ≥1 × 105 CFU/mL with no more than two species of microorganisms in a patient that is not receiving antibiotic treatment; OR A threshold of <1 × 105 CFU/mL of one single microorganism in patients receiving antibiotic treatment. |
| Variables | Global | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2014–2016 | 2017–2019 | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|
| Hospitals (n) | 33 | 27 | 27 | 25 | 24 | 29 | 26 | 79 | 79 | - |
| Total admissions (n) | 11,260 | 1724 | 1748 | 1877 | 1983 | 2176 | 1752 | 5349 | 5911 | - |
| Stays (days) | 69,512 | 11,743 | 11,635 | 10,972 | 11,556 | 12,880 | 10,726 | 34,350 | 35,162 | - |
| LOS in days, median (IQR) | 3 (6–2) | 4 (3–7) | 4 (3–6) | 3 (2–6) | 3 (2–6) | 3 (2–5) | 3 (2–6) | 4 (2–7) | 3 (2–6) | <0.001 |
| Age in months, median (IQR) | 43 (10–115) | 42.3 (9.6–104.9) | 40 (8–111) | 47.7 (11–118) | 42 (9–115) | 42 (10–121) | 46 (11–120.3) | 43 (10–111) | 43 (10–119) | 0.096 |
| Gender (male), n (%) | 6368 (56.6%) | 971 (56.3%) | 1019 (58.3%) | 1057 (56.3%) | 1121 (56.5%) | 1242 (57.1%) | 958 (54.7%) | 3047 (57%) | 3321 (56.2%) | 0.404 |
| PRISM score, median (IQR) | 2 (0–5) | 3 (0–7) | 3 (0–7) | 2 (0–5) | 2 (0–5) | 2 (0–6) | 2 (0–5) | 3 (0–6) | 2 (0–5) | <0.001 |
| Comorbidity, n (%) | 2317 (20.6%) | 396 (23%) | 380 (21.7%) | 377 (20.1%) | 419 (22.1%) | 388 (17.8%) | 357 (20.4%) | 1153 (21.6%) | 1164 (19.7%) | 0.015 |
| New AMS programs, n (%) | 26 (84%) | 9 (29%) | 4 (12.9%) | 4 (12.9%) | 1 (3.2%) | 6 (19.4%) | 2 (6.4%) | 17 (54.8%) | 9 (29%) | - |
| HAI/1000 patient-days (‰) | 6.3 | 7.3 | 5.9 | 6.7 | 5.1 | 5.4 | 7.5 | 6.6 | 6 | - |
| Deaths, n (%) | 213 (1.9%) | 44 (2.6%) | 35 (2%) | 45 (1.8%) | 35 (2%) | 30 (1.4%) | 24 (1.4%) | 124 (2.3%) | 89 (1.5%) | 0.002 |
| Type of Antibiotic Indication, n (%) | 2014–2016 n = 7597 | 2017–2019 n = 7851 | p-Value |
|---|---|---|---|
| Suspicion of community-acquired infection | 2328 (30.6%) | 2362 (30.1%) | 0.451 |
| Suspicion of outside-PICU-acquired HAIs | 1075 (14.2%) | 1047 (13.3% | <0.001 |
| Suspicion of inside-PICU-acquired HAIs | 1059 (13.9%) | 1142 (14.5%) | 0.281 |
| Surgical prophylaxis | 2447 (32.2%) | 2577 (32.8%) | 0.416 |
| Non-surgical prophylaxis | 613 (8.1%) | 686 (8.7%) | 0.134 |
| Unknown reason for prescription | 75 (0.99%) | 37 (0.47%) | <0.001 |
| Ratios | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2014–2016 | 2017–2019 | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| No. of antibiotics per patient prescribed antibiotics | |||||||||
| All indications | 1.96 | 1.83 | 1.82 | 1.81 | 1.75 | 1.96 | 1.87 | 1.84 | 0.632 |
| Community-acquired infections | 1.95 | 1.81 | 1.90 | 1.82 | 1.83 | 1.87 | 1.89 | 1.84 | 0.425 |
| Outside-PICU-acquired HAIs | 2.35 | 2.52 | 2.59 | 2.55 | 2.28 | 2.32 | 2.49 | 2.38 | 0.111 |
| Inside-PICU-acquired HAIs | 2.51 | 2.84 | 2.59 | 2.49 | 2.54 | 3.64 | 2.65 | 2.89 | <0.001 |
| Antibiotic use ratio | |||||||||
| All indications | 0.79 | 0.77 | 0.73 | 0.74 | 0.71 | 0.73 | 0.76 | 0.73 | <0.001 |
| Community-acquired infections | 0.24 | 0.24 | 0.22 | 0.20 | 0.21 | 0.24 | 0.23 | 0.22 | 0.137 |
| Outside-PICU-acquired HAIs | 0.09 | 0.08 | 0.08 | 0.08 | 0.06 | 0.09 | 0.08 | 0.08 | 1.000 |
| Inside-PICU-acquired HAIs | 0.09 | 0.07 | 0.06 | 0.07 | 0.07 | 0.07 | 0.07 | 0.07 | 1.000 |
| Antibiotic-free days ratio | |||||||||
| All indications | 0.22 | 0.23 | 0.22 | 0.26 | 0.24 | 0.26 | 0.22 | 0.25 | <0.001 |
| Community-acquired infections | 0.15 | 0.21 | 0.28 | 0.24 | 0.28 | 0.29 | 0.21 | 0.27 | <0.001 |
| Outside-PICU-acquired HAIs | 0.33 | 0.28 | 0.25 | 0.26 | 0.29 | 0.36 | 0.29 | 0.30 | 0.173 |
| Inside-PICU-acquired HAIs | 0.47 | 0.46 | 0.45 | 0.53 | 0.47 | 0.49 | 0.46 | 0.50 | <0.001 |
| Global antibiotic-free days ratio | |||||||||
| All indications | 0.33 | 0.35 | 0.37 | 0.39 | 0.39 | 0.40 | 0.35 | 0.39 | <0.001 |
| Community-acquired infections | 0.70 | 0.78 | 0.80 | 0.83 | 0.78 | 0.79 | 0.76 | 0.80 | <0.001 |
| Outside-PICU-acquired HAIs | 0.88 | 0.89 | 0.90 | 0.89 | 0.93 | 0.89 | 0.89 | 0.90 | 0.043 |
| Inside-PICU-acquired HAIs | 0.84 | 0.85 | 0.86 | 0.87 | 0.86 | 0.49 | 0.85 | 0.74 | <0.001 |
| Total n, % | 2014–2016 n, % | 2017–2019 n, % | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Surgical prophylaxis | 5024 | 2447 | 2577 | ||||
| Cefazolin | 2457 | 48.9 | 1119 | 45.7 | 1338 | 51.9 | <0.001 |
| Amoxicillin–clavulanate | 788 | 15.7 | 381 | 15.6 | 407 | 15.8 | 0.828 |
| Community-acquired infections | 4690 | 2328 | 2362 | ||||
| Cefotaxime | 1097 | 23.4 | 548 | 23.5 | 549 | 23.2 | 0.810 |
| Amoxicillin–clavulanate | 510 | 10.9 | 251 | 10.8 | 259 | 11.0 | 0.840 |
| Vancomycin | 368 | 7.8 | 187 | 8.0 | 181 | 7.7 | 0.638 |
| Outside-PICU-acquired HAIs | 2122 | 1075 | 1047 | ||||
| Meropenem | 313 | 14.8 | 157 | 14.6 | 156 | 14.9 | 0.739 |
| Vancomycin | 230 | 10.8 | 86 | 8.0 | 144 | 13.8 | <0.001 |
| Piperacillin–tazobactam | 167 | 7.9 | 109 | 10.1 | 58 | 5.5 | <0.001 |
| Amikacin | 139 | 6.6 | 68 | 6.3 | 71 | 6.8 | 0.928 |
| Teicoplanin | 90 | 4.2 | 29 | 2.7 | 61 | 5.8 | <0.001 |
| Inside-PICU-acquired HAIs | |||||||
| Vancomycin | 346 | 15.7 | 164 | 15.5 | 182 | 15.9 | 0.772 |
| Piperacillin–tazobactam | 340 | 15.4 | 162 | 15.3 | 178 | 15.6 | 0.851 |
| Meropenem | 273 | 12.4 | 131 | 12.4 | 142 | 12.4 | 0.964 |
| Teicoplanin | 166 | 7.5 | 64 | 6.0 | 102 | 8.9 | 0.010 |
| Amikacin | 135 | 6.1 | 71 | 6.7 | 64 | 5.6 | 0.282 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fresán-Ruiz, E.; Izurieta-Pacheco, A.C.; Girona-Alarcón, M.; de Carlos-Vicente, J.C.; Bustinza-Arriortua, A.; Slocker-Barrio, M.; Belda-Hofheinz, S.; Nieto-Moro, M.; Uriona-Tuma, S.M.; Pinós-Tella, L.; et al. Antimicrobial Stewardship Improvement in Pediatric Intensive Care Units in Spain—What Have We Learned? Children 2022, 9, 902. https://doi.org/10.3390/children9060902
Fresán-Ruiz E, Izurieta-Pacheco AC, Girona-Alarcón M, de Carlos-Vicente JC, Bustinza-Arriortua A, Slocker-Barrio M, Belda-Hofheinz S, Nieto-Moro M, Uriona-Tuma SM, Pinós-Tella L, et al. Antimicrobial Stewardship Improvement in Pediatric Intensive Care Units in Spain—What Have We Learned? Children. 2022; 9(6):902. https://doi.org/10.3390/children9060902
Chicago/Turabian StyleFresán-Ruiz, Elena, Ana Carolina Izurieta-Pacheco, Mònica Girona-Alarcón, Juan Carlos de Carlos-Vicente, Amaya Bustinza-Arriortua, María Slocker-Barrio, Sylvia Belda-Hofheinz, Montserrat Nieto-Moro, Sonia María Uriona-Tuma, Laia Pinós-Tella, and et al. 2022. "Antimicrobial Stewardship Improvement in Pediatric Intensive Care Units in Spain—What Have We Learned?" Children 9, no. 6: 902. https://doi.org/10.3390/children9060902
APA StyleFresán-Ruiz, E., Izurieta-Pacheco, A. C., Girona-Alarcón, M., de Carlos-Vicente, J. C., Bustinza-Arriortua, A., Slocker-Barrio, M., Belda-Hofheinz, S., Nieto-Moro, M., Uriona-Tuma, S. M., Pinós-Tella, L., Morteruel-Arizcuren, E., Schuffelmann, C., Peña-López, Y., Bobillo-Pérez, S., Jordan, I., & on behalf of the Pediatric-ENVIN-HELICS Study Group. (2022). Antimicrobial Stewardship Improvement in Pediatric Intensive Care Units in Spain—What Have We Learned? Children, 9(6), 902. https://doi.org/10.3390/children9060902