
Cardiac Evaluation of Exercise Testing in a Contemporary Population of Preschool Children: A New Approach Providing Reference Values

 , , ,
, , ,  and
and
Abstract

1. Introduction
2. Materials and Methods
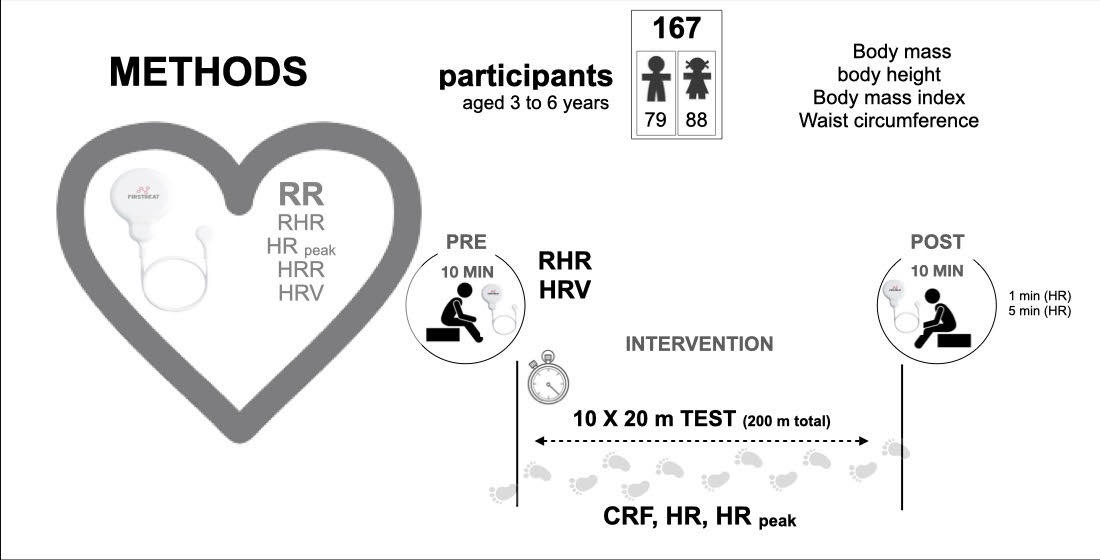
2.1. Participants
2.2. Materials and Testing
2.2.1. Anthropometric Variables
2.2.2. Cardiorespiratory Analysis
2.3. Procedure
2.4. Statistical Analyses
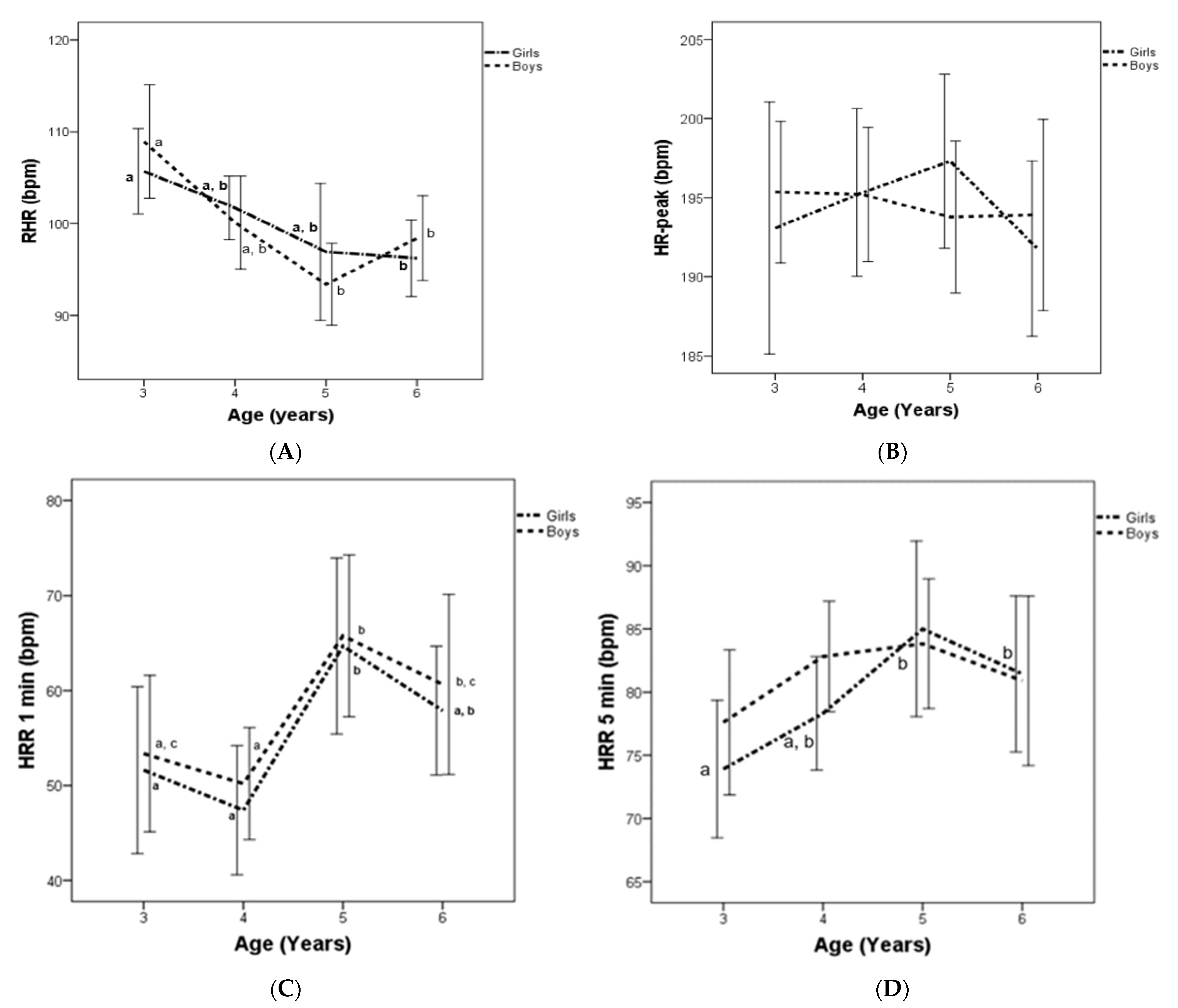
3. Results
4. Discussion
4.1. Cardiac Autonomic Function at Rest
4.2. Cardiac Autonomic Function during Maximal Exercise
4.3. Cardiac Autonomic Function at Recovery after Exercise
4.4. Heart Rate Variability
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Timmons, B.W.; Naylor, P.J.; Pfeiffer, K.A. Physical activity for preschool children—How much and how? Can. J. Public Health 2007, 98, S122–S134. [Google Scholar] [CrossRef] [PubMed]
- Veijalainen, A.; Haapala, E.A.; Väistö, J.; Leppänen, M.H.; Lintu, N.; Tompuri, T.; Seppälä, S.; Ekelund, U.; Tarvainen, M.P.; Westgate, K.; et al. Associations of physical activity, sedentary time, and cardiorespiratory fitness with heart rate variability in 6- to 9-year-old children: The PANIC study. Eur. J. Appl. Physiol. 2019, 119, 2487–2498. [Google Scholar] [CrossRef] [PubMed]
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor Gorber, S.; Kho, M.E.; et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S197–S239. [Google Scholar] [CrossRef] [PubMed]
- Bürgi, F.; Meyer, U.; Granacher, U.; Schindler, C.; Marques-Vidal, P.; Kriemler, S.; Puder, J.J. Relationship of physical activity with motor skills, aerobic fitness and body fat in preschool children: A cross-sectional and longitudinal study (Ballabeina). Int. J. Obes. 2011, 35, 937–944. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef]
- Bongers-Karmaoui, M.N.; Jaddoe, V.W.V.; Roest, A.A.W.; Gaillard, R. The Cardiovascular Stress Response as Early Life Marker of Cardiovascular Health: Applications in Population-Based Pediatric Studies—A Narrative Review. Pediatr. Cardiol. 2020, 41, 1739–1755. [Google Scholar] [CrossRef]
- Van Brussel, M.; Bongers, B.C.; Hulzebos, E.H.J.; Burghard, M.; Takken, T. A systematic approach to interpreting the cardiopulmonary exercise test in pediatrics. Pediatr. Exerc. Sci. 2019, 31, 194–203. [Google Scholar] [CrossRef]
- Schuster, I.; Karpoff, L.; Perez-Martin, A.; Oudot, C.; Startun, A.; Rubini, M.; Obert, P.; Vinet, A. Cardiac function during exercise in obese prepubertal boys: Effect of degree of obesity. Obesity 2009, 17, 1878–1883. [Google Scholar] [CrossRef]
- Harkel, A.D.J.T.; Takken, T.; Van Osch-Gevers, M.; Helbing, W.A. Normal values for cardiopulmonary exercise testing in children. Eur. J. Prev. Cardiol. 2011, 18, 48–54. [Google Scholar] [CrossRef]
- da Silva, C.F.; Burgos, M.S.; da Silva, P.T.; Burgos, L.T.; Welser, L.; Sehn, A.P.; Horta, J.A.; de Mello, E.D.; Reuter, C.P. Relationship between Cardiometabolic Parameters and Elevated Resting and Effort Heart Rate in Schoolchildren. Arq. Bras. Cardiol. 2017, 109, 191–198. [Google Scholar] [CrossRef]
- Fernandes, R.A.; Freitas, I.F.; Codogno, J.S.; Christofaro, D.G.D.; Monteiro, H.L.; Roberto Lopes, D.M.H. Resting heart rate is associated with blood pressure in male children and adolescents. J. Pediatr. 2011, 158, 634–637. [Google Scholar] [CrossRef] [PubMed]
- Jat, K.R.; Lodha, R.; Kabra, S.K. Arrhythmias in children. Indian J. Pediatr. 2011, 78, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Clausen, H.; Theophilos, T.; Jackno, K.; Babl, F.E. Paediatric arrhythmias in the emergency department. Emerg. Med. J. 2012, 29, 732–737. [Google Scholar] [CrossRef]
- Egan, K.R.; Ralphe, J.C.; Weinhaus, L.; Maginot, K.R. Just Sinus Bradycardia or Something More Serious? Case Rep. Pediatr. 2013, 2013, 736164. [Google Scholar] [CrossRef] [PubMed]
- Massin, M.M. The role of exercise testing in pediatric cardiology Intérêt du test d’effort en cardiologie pédiatrique. Arch. Cardiovasc. Dis. 2014, 107, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Baba, R.; Iwagaki, S.; Tauchi, N.; Tsurusawa, M. Is the chronotropic index applicable to children and adolescents? Circ. J. 2005, 69, 471–474. [Google Scholar] [CrossRef][Green Version]
- Brubaker, P.H.; Kitzman, D.W. Chronotropic incompetence: Causes, consequences, and management. Circulation 2011, 123, 1010–1020. [Google Scholar] [CrossRef]
- Alvarado, A.M.; Ward, K.M.; Muntz, D.S.; Thompson, A.A.; Rodeghier, M.; Fernhall, B.; Liem, R.I. Heart rate recovery is impaired after maximal exercise testing in children with sickle cell anemia. J. Pediatr. 2015, 166, 389–393. [Google Scholar] [CrossRef]
- Singh, T.P.; Rhodes, J.; Gauvreau, K. Determinants of heart rate recovery following exercise in children. Med. Sci. Sports Exerc. 2008, 40, 601–605. [Google Scholar] [CrossRef]
- Bjelakovic, L.; Vukovic, V.; Jovic, M.; Bankovic, S.; Kostic, T.; Radovanovic, D.; Pantelic, S.; Zivkovic, M.; Stojanovic, S.; Bjelakovic, B. Heart rate recovery time in metabolically healthy and metabolically unhealthy obese children. Phys. Sportsmed. 2017, 45, 438–442. [Google Scholar] [CrossRef]
- Michels, N.; Clays, E.; De Buyzere, M.; Huybrechts, I.; Marild, S.; Vanaelst, B.; De Henauw, S.; Sioen, I. Determinants and reference values of short-term heart rate variability in children. Eur. J. Appl. Physiol. 2013, 113, 1477–1488. [Google Scholar] [CrossRef] [PubMed]
- Massin, M.; Von Bernuth, G. Clinical and haemodynamic correlates of heart rate variability in children with congenital heart disease. Eur. J. Pediatr. 1998, 157, 967–971. [Google Scholar] [CrossRef] [PubMed]
- Emin, O.; Esra, G.; Aysegül, D.; Ufuk, E.; Ayhan, S.; Rusen, D.M. Autonomic nervous system dysfunction and their relationship with disease severity in children with atopic asthma. Respir. Physiol. Neurobiol. 2012, 183, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Lory, C.; Kadlaskar, G.; McNally Keehn, R.; Francis, A.L.; Keehn, B. Brief Report: Reduced Heart Rate Variability in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2020, 50, 4183–4190. [Google Scholar] [CrossRef]
- Verrotti, A.; Chiarelli, F.; Morgese, G. Autonomic dysfunction in newly diagnosed insulin-dependent diabetes mellitus children. Pediatr. Neurol. 1996, 14, 49–52. [Google Scholar] [CrossRef]
- Rukmani, M.R.; Seshadri, S.P.; Thennarasu, K.; Raju, T.R.; Sathyaprabha, T.N. Heart rate variability in children with attention-deficit/hyperactivity disorder: A pilot study. Ann. Neurosci. 2016, 23, 81–88. [Google Scholar] [CrossRef]
- Li, A.M.; Yin, J.; Yu, C.C.W.; Tsang, T.; So, H.K.; Wong, E.; Chan, D.; Hon, E.K.L.; Sung, R. The six-minute walk test in healthy children: Reliability and validity. Eur. Respir. J. 2005, 25, 1057–1060. [Google Scholar] [CrossRef]
- Akdur, H.; Sözen, A.B.; Yiǧit, Z.; Öztunç, F.; Kudat, H.; Güven, Ö. The evaluation of cardiovascular response to exercise in healthy Turkish children. Turk. J. Pediatr. 2009, 51, 472–477. [Google Scholar]
- Speer, K.E.; Semple, S.; Naumovski, N.; McKune, A.J. Measuring Heart Rate Variability Using Commercially Available Devices in Healthy Children: A Validity and Reliability Study. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 390–404. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Latorre, P.A.; Mora, D.; Fernández, M.; Salas, J.; Moriana, F. GFTest-retest reliability of a field-based physical fitness assessment for children aged 3–6 years. Nutr. Hosp. 2015, 32, 1683. [Google Scholar]
- Latorre-Román, P.Á.; García-Pinillos, F.; Salas Sánchez, J.; Jiménez, M.M.; Serrano Huete, V.; Martínez Redondo, M.; Vela, J.A.; Párraga-Montilla, J.A. A New Approach for Evaluation of Cardiovascular Fitness and Cardiac Responses to Maximal Exercise Test in Master Runners: A Cross-Sectional Study. J. Clin. Med. 2022, 11, 1648. [Google Scholar] [CrossRef]
- Bobkowski, W.; Stefaniak, M.E.; Krauze, T.; Gendera, K.; Wykretowicz, A.; Piskorski, J.; Guzik, P. Measures of Heart Rate Variability in 24-h ECGs Depend on Age but Not Gender of Healthy Children. Front. Physiol. 2017, 8, 311. [Google Scholar] [CrossRef]
- Cachadiña, E.S.; De la Cruz Torres, B.; Sixto, A.S.; Martín, P.F.; Berral de la Rosa, F.J.; Orellana, J.N. Heart rate variability is lower in patients with intermittent claudication: A preliminary study. Arch. Med. Del Deport. 2018, 35, 218–221. [Google Scholar]
- European Society of Cardiology. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef]
- von Scheidt, F.; Meier, S.; Krämer, J.; Apitz, A.; Siaplaouras, J.; Bride, P.; Kaestner, M.; Apitz, C. Heart Rate Response During Treadmill Exercise Test in Children and Adolescents with Congenital Heart Disease. Front. Pediatr. 2019, 7, 65. [Google Scholar] [CrossRef]
- Easley, E.A.; Black, W.S.; Bailey, A.L.; Lennie, T.A.; Sims, W.J.; Clasey, J.L. Recovery Responses to Maximal Exercise in Healthy-Weight Children and Children with Obesity. Res. Q. Exerc. Sport 2018, 89, 38–46. [Google Scholar] [CrossRef]
- Paridon, S.M.; Alpert, B.S.; Boas, S.R.; Cabrera, M.E.; Caldarera, L.L.; Daniels, S.R.; Kimball, T.R.; Knilans, T.K.; Nixon, P.A.; Rhodes, J.; et al. Clinical Stress Testing in the Pediatric Age Group. Circulation 2006, 113, 1905–1920. [Google Scholar] [CrossRef]
- Latorre-Román, P.A.; Floody, P.D.; Martínez-Redondo, M.; Salas-Sánchez, J.; Consuegra-González, P.J.; Aragón-Vela, J.; Robles-Fuentes, A.; Sarabia-Cachadiña, E.; Párraga-Montilla, J.A. Comprehensive cardiac evaluation to maximal exercise in a contemporary population of prepubertal children. Pediatr. Res. 2021, 30, 1–10. [Google Scholar] [CrossRef]
- Buchheit, M.; Millet, G.P.; Parisy, A.; Pourchez, S.; Laursen, P.B.; Ahmaidi, S. Supramaximal Training and Postexercise Parasympathetic Reactivation in Adolescents. Med. Sci. Sports Exerc. 2008, 40, 362–371. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.R.; Castro-Piñero, J.; Artero, E.G.; Ortega, F.B.; Sjöström, M.; Suni, J.; Castillo, M.J. Predictive validity of health-related fitness in youth: A systematic review. Br. J. Sports Med. 2009, 43, 909–923. [Google Scholar] [CrossRef] [PubMed]
- Latorre-Román, P.; Fernández-Sánchez, M.; Moriana-Coronas, F.J.; García-Pinillos, F. Design and validation of a cardiorespiratory capacity test for preschool children. S. Afr. J. Res. Sport Phys. Educ. Recreat. 2016, 38, 129–137. [Google Scholar]
- Mimura, K.I.; Maeda, K. Heart rate response to treadmill exercise in children of ages 4-6 years. Ann. Physiol. Anthropol. 1989, 8, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Ostchega, Y.; Porter, K.S.; Hughes, J.; Dillon, C.F.; Nwankwo, T. Resting pulse rate reference data for children, adolescents, and adults: United States, 1999–2008. Natl. Health Stat. Rep. 2011, 24, 1–16. [Google Scholar]
- Mahon, A.D.; Anderson, C.S.; Hipp, M.J.; Hunt, K.A. Heart Rate Recovery from Submaximal Exercise in Boys and Girls. Med. Sci. Sports Exerc. 2003, 35, 2093–2097. [Google Scholar] [CrossRef]
- Sarganas, G.; Schaffrath Rosario, A.; Neuhauser, H.K. Resting Heart Rate Percentiles and Associated Factors in Children and Adolescents. J. Pediatr. 2017, 187, 174–181. [Google Scholar] [CrossRef]
- Rabbia, F.; Grosso, T.; Cat Genova, G.; Conterno, A.; De Vito, B.; Mulatero, P.; Chiandussi, L.; Veglio, F. Assessing resting heart rate in adolescents: Determinants and correlates. J. Hum. Hypertens. 2002, 16, 327–332. [Google Scholar] [CrossRef]
- Simhaee, D.; Corriveau, N.; Gurm, R.; Geiger, Z.; Kline-Rogers, E.; Goldberg, C.; Eagle, K.A.; Jackson, E.A. Recovery heart rate: An indicator of cardiovascular risk among middle school children. Pediatr. Cardiol. 2013, 34, 1431–1437. [Google Scholar] [CrossRef]
- Kwok, S.Y.; So, H.K.; Choi, K.C.; Lo, A.F.C.; Li, A.M.; Sung, R.Y.T.; Nelson, E.A.S. Resting heart rate in children and adolescents: Association with blood pressure, exercise and obesity. Arch. Dis. Child. 2013, 98, 287–291. [Google Scholar] [CrossRef]
- Hart, J. Normal resting pulse rate ranges. J. Nurs. Educ. Pract. 2015, 5, 95–98. [Google Scholar] [CrossRef]
- Gelbart, M.; Ziv-Baran, T.; Williams, C.A.; Yarom, Y.; Dubnov-Raz, G. Prediction of maximal heart rate in children and adolescents. Clin. J. Sport Med. 2017, 27, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef]
- Proudfoot, N.A.; King-Dowling, S.; Cairney, J.; Bray, S.R.; MacDonald, M.J.; Timmons, B.W. Physical activity and trajectories of cardiovascular health indicators during early childhood. Pediatrics 2019, 144, e20182242. [Google Scholar] [CrossRef] [PubMed]
- Jae, S.Y.; Kurl, S.; Laukkanen, J.A.; Zaccardi, F.; Choi, Y.-H.; Fernhall, B.; Carnethon, M.; Franklin, B.A. Exercise Heart Rate Reserve and Recovery as Predictors of Incident Type 2 Diabetes. Am. J. Med. 2016, 129, 536.e7–536.e12. [Google Scholar] [CrossRef]
- Verschuren, O.; Maltais, D.B.; Takken, T. The 220-age equation does not predict maximum heart rate in children and adolescents. Dev. Med. Child Neurol. 2011, 53, 861–864. [Google Scholar] [CrossRef] [PubMed]
- Cadenas-Sánchez, C.; Alcántara-Moral, F.; Sánchez-Delgado, G.; Mora-González, J.; Martínez-Téllez, B.; Herrador-Colmenero, M.; Jiménez-Pavón, D.; Femia, P.; Ruiz, J.R.; Ortega, F.B. Assessment of cardiorespiratory fitness in preschool children: Adaptation of the 20 metres shuttle run test. Nutr. Hosp. 2014, 30, 1333–1343. [Google Scholar] [CrossRef]
- Nikolaidis, P.; Kintziou, E.; Georgoudis, G.; Afonso, J.; Vancini, R.; Knechtle, B. The Effect of Body Mass Index on Acute Cardiometabolic Responses to Graded Exercise Testing in Children: A Narrative Review. Sports 2018, 6, 103. [Google Scholar] [CrossRef]
- Danieli, A.; Lusa, L.; Potočnik, N.; Meglič, B.; Grad, A.; Bajrović, F.F. Resting heart rate variability and heart rate recovery after submaximal exercise. Clin. Auton. Res. 2014, 24, 53–61. [Google Scholar] [CrossRef]
- Fernando, R.J.; Ravichandran, K.; Vaz, M. Aerobic fitness, heart rate recovery and heart rate recovery time in indian school children. Indian J. Physiol. Pharmacol. 2015, 59, 407–413. [Google Scholar]
- Plaza-Florido, A.; Migueles, J.H.; Mora-Gonzalez, J.; Molina-Garcia, P.; Rodriguez-Ayllon, M.; Cadenas-Sanchez, C.; Esteban-Cornejo, I.; Navarrete, S.; Lozano, R.M.; Michels, N.; et al. The role of heart rate on the associations between body composition and heart rate variability in children with overweight/Obesity: The active brains project. Front. Physiol. 2019, 10, 895. [Google Scholar] [CrossRef]
- Jarrin, D.C.; McGrath, J.J.; Poirier, P.; Séguin, L.; Tremblay, R.E.; Montplaisir, J.Y.; Paradis, G.; Séguin, J.R. Short-term heart rate variability in a population-based sample of 10-year-old children. Pediatr. Cardiol. 2015, 36, 41–48. [Google Scholar] [CrossRef]
- Gasior, J.S.; Sacha, J.; Jeleń, P.J.; Pawlowski, M.; Werner, B.; Dabrowski, M.J. Interaction between heart rate variability and heart rate in pediatric population. Front. Physiol. 2015, 18, 385. [Google Scholar] [CrossRef]
- Gasior, J.S.; Sacha, J.; Pawlowski, M.; Zielinski, J.; Jelen, P.J.; Tomik, A.; Ksiazczyk, T.M.; Werner, B.; Dabrowski, M.J. Normative values for heart rate variability parameters in school-aged children: Simple approach considering differences in average heart rate. Front. Physiol. 2018, 24, 1495. [Google Scholar] [CrossRef]
- Cysarz, D.; Linhard, M.; Edelhäuser, F.; Längler, A.; van Leeuwen, P.; Henze, G.; Seifert, G. Unexpected course of nonlinear cardiac interbeat interval dynamics during childhood and adolescence. PLoS ONE 2011, 6, e19400. [Google Scholar] [CrossRef]
- Eyre, E.L.J.; Duncan, M.J.; Birch, S.L.; Fisher, J.P. The influence of age and weight status on cardiac autonomic control in healthy children: A review. Auton. Neurosci. Basic Clin. 2014, 186, 8–21. [Google Scholar] [CrossRef]
- Voss, A.; Schroeder, R.; Heitmann, A.; Peters, A.; Perz, S. Short-Term Heart Rate Variability—Influence of Gender and Age in Healthy Subjects. PLoS ONE 2015, 10, e0118308. [Google Scholar] [CrossRef]
- Raffin, J.; Barthélémy, J.-C.; Dupré, C.; Pichot, V.; Berger, M.; Féasson, L.; Busso, T.; Da Costa, A.; Colvez, A.; Montuy-Coquard, C.; et al. Exercise Frequency Determines Heart Rate Variability Gains in Older People: A Meta-Analysis and Meta-Regression. Sport Med. 2019, 49, 719–729. [Google Scholar] [CrossRef]
- Guilkey, J.P.; Dykstra, B.; Erichsen, J.; Mahon, A.D. Heart rate response and variability following maximal exercise in overweight children. Pediatr. Exerc. Sci. 2017, 29, 341–349. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Girls Mean (SD) | Boys Mean (SD) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Years | All n = 79 | 3 n = 16 | 4 n = 25 | 5 n = 13 | 6 n = 25 | p-Value | All n = 88 | 3 n = 14 | 4 n = 25 | 5 n = 18 | 6 n = 31 | p-Value |
| Body mass (kg) | 20.51 (4.90) | 15.61 (2.17) | 19.88 (3.55) | 21.69 (4.64) | 23.69 (4.90) | <0.001 | 20.30 (4.55) | 16.16 (4.84) | 19.95 (2.72) | 18.31 (3.27) | 23.55 (4.21) | <0.001 |
| Height (cm) | 110.14 (14.60) | 102.50 (9.21) | 107.72 (5.20) | 114.92 (6.71) | 115.16 (22.36) | <0.001 | 109.28 (20.27) | 100.86 (5.20) | 110.56 (6.32) | 114.65 (4.95) | 109.10 (32.72) | <0.001 |
| BMI (kg/m2) | 16.40 (2.88) | 14.97 (2.11) | 17.18 (3.18) | 16.50 (3.51) | 16.49 (2.44) | 0.108 | 15.81(2.76) | 15.89 (4.16) | 16.31 (1.72) | 14.04 (2.91) | 16.34 (2.26) | 0.118 |
| WC (cm) | 56.94 (9.75) | 54.27 (11.18) | 60.84 (6.54) | 55.0 (11.72) | 55.16 (9.93) | 0.047 | 52.29 (13.19) * | 50.0 (12.87) | 52.78 (13.81) | 50.78 (13.24) | 54.70 (13.19) | 0.263 |
| RHR (bpm)≠ | 100.00 (10.22) | 105.69 (8.76) | 101.72 (8.32) | 96.92 (12.31) | 96.24 (10.11) | 0.014 | 99.55 (12.27) | 108.93 (10.68) | 100.12 (12.23) | 93.39 (8.95) | 98.42 (12.53) | 0.003 |
| 10 × 20 m (s)≠ | 79.09 (18.35) | 91.38 (11.21) | 87.96 (14.26) | 68.69 (16.00) | 67.76 (17.58) | <0.001 | 74.84 (15.82) | 96.07 (13.69) | 77.00 (10.77) ** | 70.67 (11.30) | 65.93 (13.14) | <0.001 |
| CI≠ | 0.81 (0.11) | 0.79 (0.12) | 0.82 (0.11) | 0.84 (0.07) | 0.81 (0.12) | 0.578 | 0.82 (0.11) | 0.80 (0.08) | 0.82 (0.07) | 0.83 (0.08) | 0.82 (0.15) | 0.864 |
| HRr (bpm)≠ | 94.06 (14.80) | 87.37 (13.27) | 93.60 (12.02) | 100.3 (14.08) | 95.52 (17.45) | 0.114 | 94.93 (15.95) | 86.43 (13.83) | 95.08 (11.82) | 100.39 (11.73) | 95.48 (20.33) | 0.104 |
| HRPeak (bpm) | 194.07 (12.80) | 193.0 (14.92) | 185.32 (12.84) | 197.31 (9.10) | 191.77 (13.42) | 0.663 | 194.48 (12.25) | 195.36 (7.75) | 195.20 (10.29) | 193.78 (9.65) | 193.91 (16.44) | 0.914 |
| HRR1min(bpm) | 54.42 (17.15) | 51.63 (16.49) | 47.40 (16.51) | 64.69 (15.32) | 57.89 (16.46) | 0.024 | 57.57 (20.25) | 53.36 (14.27) | 50.20 (14.28) | 65.78 (17.12) | 60.65 (25.85) | 0.012 |
| HRR5min(bpm) | 79.51 (12.60) | 73.91 (10.22) | 78.32 (10.89) | 85.00 (11.47) | 81.45 (14.66) | 0.026 | 81.53 (13.64) | 77.61 (9.92) | 82.82 (10.59) | 83.83(10.31) | 80.91 (18.30) | 0.396 |
| RMSSD (ms) | 28.58 (10.61) | 24.06 (9.54) | 28.16 (9.5) | 34.77 (13.26) | 29.00 (6.03) | 0.083 | 29.10 (13.15) | 21.07 (8.28) | 28.08 (10.84) | 36.06 (15.16) | 31.60 (16.62) | 0.025 |
| SDNN (ms) | 54.28 (19.33) | 44.69 (13.50) | 53.24 (16.86) | 68.69 (25.29) | 53.00 (10.92) | 0.036 | 56.82 (23.06) | 41.93 (10.45) | 57.40 (24.54) | 66.00 (24.39) | 62.60 (20.40) | 0.012 |
| HF (ms2) | 1289.92 (935.1) | 856.1 (566.4) | 1256.6 (866.77) | 1944 (1206) | 1167.2 (718.07) | 0.025 | 1270.10 (915.9) | 852 (611) | 1201 (972.48) | 1614.92 (867.1) | 1546.8 (1198.3) | 0.079 |
| LF (ms2) | 1894 (1536.77) | 1196.2 (942) | 1770.5 (1844.9) | 2496 (1630) | 2151.2 (1334.8) | 0.011 | 1896.5 (1416.8) | 1023.34 (630.9) | 1576.1 (1211.4) | 2348.7 (1288.5) | 2286.7 (1677.2) | 0.003 |
| LF/HF | 176.83 (74.10) | 167.6 (57.3) | 166.8 (72.90) | 154.6 (43.85) | 204.30 (91.12) | 0.295 | 199.42 (95.47) | 184.8 (118) | 189.44 (67.76) | 190.47 (84.51) | 218.94 (108.91) | 0.334 |
| RHR | HRpeak | HRR1min | HRR5min | |||||
|---|---|---|---|---|---|---|---|---|
| Beta | p-Valor | Beta | p-Valor | Beta | p-Valor | Beta | p-Valor | |
| Age (Years) | −0.301 | <0.001 | −0.049 | 0.528 | 0.219 | 0.004 | 0.134 | 0.084 |
| Sex | −0.020 | 0.796 | 0.016 | 0.833 | 0.084 | 0.283 | 0.077 | 0.326 |
| BMI (Kg/m2) | −0.050 | 0.508 | 0.010 | 0.904 | 0.083 | 0.280 | 0.143 | 0.067 |
| WC (cm) | −0.110 | 0.172 | −0.051 | 0.551 | −0.124 | 0.134 | 0.036 | 0.670 |
| 10 × 20 m (s) | 0.081 | 0.382 | −0.155 | 0.107 | 0.023 | 0.808 | −0.032 | 0.523 |
| RHR (bpm) | 0.171 | 0.036 | −0.251 | 0.001 | −0.371 | <0.001 | ||
| HRpeak (bpm) | 0.223 | 0.003 | 0.601 | <0.001 | ||||
| HRr (bpm) | −0.561 | <0.001 | 0.721 | <0.001 | 0.361 | <0.001 | 0.762 | <0.001 |
| CI | −0.021 | 0.782 | 0.966 | <0.001 | 0.268 | <0.001 | 0.672 | <0.001 |
| HRR1min(bpm) | 0.272 | <0.001 | ||||||
| HRR5min(bpm) | ||||||||
| RMSSD (ms), rest | −0.799 | <0.001 | −0.191 | 0.036 | 0.233 | 0.010 | 0.334 | <0.001 |
| SDNN (ms), rest | −0.771 | <0.001 | −0.100 | 0.274 | 0.150 | 0.098 | 0.347 | <0.001 |
| HF (ms2), rest | −0.686 | <0.001 | −0.211 | 0.020 | 0.236 | 0.009 | 0.274 | 0.002 |
| LF (ms2), rest | −0.604 | <0.001 | −0.077 | 0.324 | 0.260 | 0.001 | 0.263 | 0.001 |
| LF/HF rest | 0.243 | 0.001 | −0.012 | 0.880 | −0.055 | 0.483 | −0.044 | 0.572 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Latorre-Román, P.Á.; Martínez-Redondo, M.; Salas-Sánchez, J.; Consuegra-González, P.J.; Sarabia-Cachadiña, E.; Aragón-Vela, J.; Párraga-Montilla, J.A. Cardiac Evaluation of Exercise Testing in a Contemporary Population of Preschool Children: A New Approach Providing Reference Values. Children 2022, 9, 654. https://doi.org/10.3390/children9050654
Latorre-Román PÁ, Martínez-Redondo M, Salas-Sánchez J, Consuegra-González PJ, Sarabia-Cachadiña E, Aragón-Vela J, Párraga-Montilla JA. Cardiac Evaluation of Exercise Testing in a Contemporary Population of Preschool Children: A New Approach Providing Reference Values. Children. 2022; 9(5):654. https://doi.org/10.3390/children9050654
Chicago/Turabian StyleLatorre-Román, Pedro Ángel, Martínez Martínez-Redondo, Jesus Salas-Sánchez, Pedro José Consuegra-González, Elena Sarabia-Cachadiña, Jerónimo Aragón-Vela, and Juan A. Párraga-Montilla. 2022. "Cardiac Evaluation of Exercise Testing in a Contemporary Population of Preschool Children: A New Approach Providing Reference Values" Children 9, no. 5: 654. https://doi.org/10.3390/children9050654
APA StyleLatorre-Román, P. Á., Martínez-Redondo, M., Salas-Sánchez, J., Consuegra-González, P. J., Sarabia-Cachadiña, E., Aragón-Vela, J., & Párraga-Montilla, J. A. (2022). Cardiac Evaluation of Exercise Testing in a Contemporary Population of Preschool Children: A New Approach Providing Reference Values. Children, 9(5), 654. https://doi.org/10.3390/children9050654