
Orthorexia Nervosa in Adolescents and Young Adults: A Literature Review




Abstract
{kind=link}
1. Introduction
2. Materials and Methods
3. Results
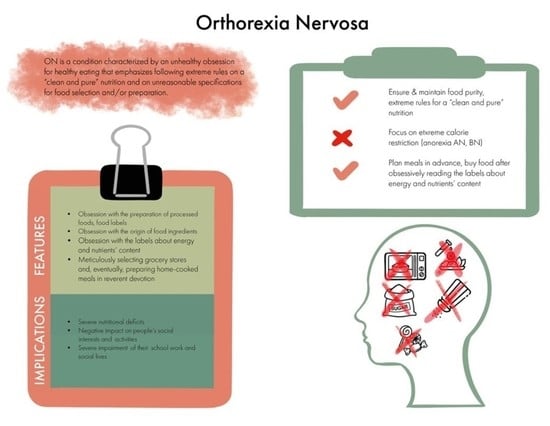
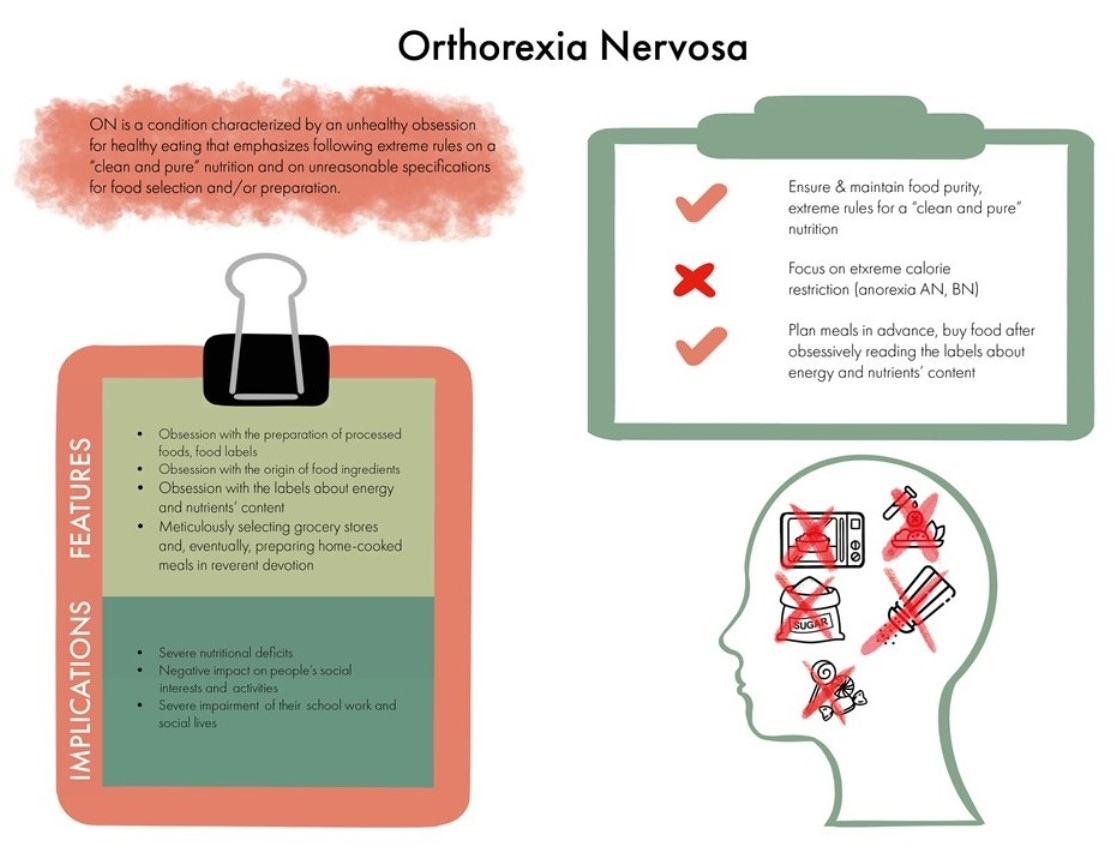
3.1. ON: Definition and Main Features
3.2. Origin of the Term “Orthorexia Nervosa”
3.3. ON and the Spectrum of EDs
3.4. Diagnosis of ON-Questionnaires
3.5. Epidemiology, Prevalence, and Sociodemographic Correlates of ON
3.6. Mental Health-Related and Nutritional Correlates of ON
3.7. ON and Social Media as an Important Risk Factor among Adolescents and Young Adults
3.8. Management of ON
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef]
- Barnes, M.A.; Caltabiano, M.L. The interrelationship between orthorexia nervosa, perfectionism, body image and attachment style. Eat. Weight Disord. 2017, 22, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Reel, J.; Voelker, D.; Greenleaf, C. Weight status and body image perceptions in adolescents: Current perspectives. Adolesc. Health Med. Ther. 2015, 6, 149–158. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Nutrition in Adolescence: Issues and Challenges for the Health Sector: Issues in Adolescent Health and Development; World Health Organization: Geneva, Switzerland, 2005.
- Prentice, A.M.; Ward, K.; Goldberg, G.R.; Jarjou, L.M.; Moore, S.E.; Fulford, A.J.; Prentice, A. Critical windows for nutritional interventions against stunting. Am. J. Clin. Nutr. 2013, 97, 911–918. [Google Scholar] [CrossRef] [PubMed]
- Christian, P.; Smith, E.R. Adolescent Undernutrition: Global Burden, Physiology, and Nutritional Risks. Ann. Nutr. Metab. 2018, 72, 316–328. [Google Scholar] [CrossRef]
- Bazzano, L.A. The High Cost of Not Consuming Fruits and Vegetables. J. Am. Diet. Assoc. 2006, 106, 1364–1368. [Google Scholar] [CrossRef]
- McComb, S.E.; Mills, J.S. Orthorexia nervosa: A review of psychosocial risk factors. Appetite 2019, 140, 50–75. [Google Scholar] [CrossRef]
- Dunn, T.M.; Bratman, S. On orthorexia nervosa: A review of the literature and proposed diagnostic criteria. Eat. Behav. 2016, 21, 11–17. [Google Scholar] [CrossRef]
- Brytek-Matera, A.; Rogoza, R.; Gramaglia, C.; Zeppegno, P. Predictors of orthorexic behaviours in patients with eating disorders: A preliminary study. BMC Psychiatry 2015, 15, 252. [Google Scholar] [CrossRef]
- Turner, P.G.; Lefevre, C.E. Instagram use is linked to increased symptoms of orthorexia nervosa. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2017, 22, 277–284. [Google Scholar] [CrossRef]
- Bratman, S. Health Food Junkies: Overcoming the Obession with Healthful Eating, 1st ed.; Broadway Books: New York, NY, USA, 2000. [Google Scholar]
- Donini, L.M.; Marsili, D.; Graziani, M.P.; Imbriale, M.; Cannella, C. Orthorexia nervosa: A preliminary study with a proposal for diagnosis and an attempt to measure the dimension of the phenomenon. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2004, 9, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Moroze, R.M.; Dunn, T.M.; Holland, J.C.; Yager, J.; Weintraub, P. Microthinking About Micronutrients: A Case of Transition from Obsessions About Healthy Eating to Near-Fatal “Orthorexia Nervosa” and Proposed Diagnostic Criteria. J. Psychosom. Res. 2015, 56, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Costa, C.B.; Khalil, K.; Gibbs, K. Orthorexia Nervosa: A Review of the Literature. Issues Ment. Health Nurs. 2017, 38, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Cena, H.; Barthels, F.; Cuzzolaro, M.; Bratman, S.; Brytek-Matera, A.; Dunn, T.; Varga, M.; Missbach, B.; Donini, L.M. Definition and diagnostic criteria for orthorexia nervosa: A narrative review of the literature. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2019, 24, 209–246. [Google Scholar] [CrossRef] [PubMed]
- Koven, N.S.; Senbonmatsu, R. A neuropsychological evaluation of orthorexia nervosa. Open J. Psychiatry 2013, 3, 214–222. [Google Scholar] [CrossRef]
- Park, S.W.; Kim, J.Y.; Go, G.J.; Jeon, E.S.; Pyo, H.J.; Kwon, Y.J. Orthorexia Nervosa with Hyponatremia, Subcutaneous Emphysema, Pneumomediastimum, Pneumothorax, and Pancytopenia. Electrolytes Blood Press. 2011, 9, 32–37. [Google Scholar] [CrossRef]
- Koven, N.; Abry, A. The clinical basis of orthorexia nervosa: Emerging perspectives. Neuropsychiatr. Dis. Treat. 2015, 11, 385–394. [Google Scholar] [CrossRef]
- Segura-Garcia, C.; Ramacciotti, C.; Rania, M.; Aloi, M.; Caroleo, M.; Bruni, A.; Gazzarrini, D.; Sinopoli, F.; de Fazio, P. The prevalence of orthorexia nervosa among eating disorder patients after treatment. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2015, 20, 161–166. [Google Scholar] [CrossRef]
- Varga, M.; Dukay-Szabó, S.; Túry, F.; Eric, F.V.F. Evidence and gaps in the literature on orthorexia nervosa. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2013, 18, 103–111. [Google Scholar] [CrossRef]
- Mathieu, J. What is orthorexia? J. Am. Diet. Assoc. 2005, 105, 1510–1512. [Google Scholar] [CrossRef]
- Zickgraf, H.F.; Barrada, J.R. Orthorexia nervosa vs. healthy orthorexia: Relationships with disordered eating, eating behavior, and healthy lifestyle choices. Eat. Weight Disord. 2021. [Google Scholar] [CrossRef] [PubMed]
- Strahler, J.; Stark, R. Perspective: Classifying Orthorexia Nervosa as a New Mental Illness—Much Discussion, Little Evidence. Adv. Nutr. Int. Rev. J. 2020, 11, 784–789. [Google Scholar] [CrossRef] [PubMed]
- Dell’Osso, L.; Abelli, M.; Carpita, B.; Pini, S.; Castellini, G.; Carmassi, C.; Ricca, V. Historical evolution of the concept of anorexia nervosa and relationships with orthorexia nervosa, autism, and obsessive-compulsive spectrum. Neuropsychiatr. Dis. Treat. 2016, 12, 1651–1660. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5 (R.)); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Rodgers, R.F.; Melioli, T. The Relationship between Body Image Concerns, Eating Disorders and Internet Use, Part I: A Review of Empirical Support. Adolesc. Res. Rev. 2016, 1, 95–119. [Google Scholar] [CrossRef]
- Zagaria, A.; Vacca, M.; Cerolini, S.; Ballesio, A.; Lombardo, C. Associations between orthorexia, disordered eating, and obsessive—Compulsive symptoms: A systematic review and meta-analysis. Int. J. Eat. Disord. 2021. [Google Scholar] [CrossRef]
- Håman, L.; Barker-Ruchti, N.; Patriksson, G.; Lindgren, E.-C. Orthorexia nervosa: An integrative literature review of a lifestyle syndrome. Int. J. Qual. Stud. Health Well-Being 2015, 10, 26799. [Google Scholar] [CrossRef]
- Crawford, R. Healthism and the Medicalization of Everyday Life. Int. J. Health Serv. 1980, 10, 365–388. [Google Scholar] [CrossRef]
- Ramacciotti, C.E.; Perrone, P.; Coli, E.; Burgalassi, A.; Conversano, C.; Massimetti, G.; Dell’Osso, L. Orthorexia nervosa in the general population: A preliminary screening using a self-administered questionnaire (ORTO-15). Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2011, 16, e127–e130. [Google Scholar] [CrossRef]
- Donini, L.M.; Marsili, D.; Graziani, M.P.; Imbriale, M.; Cannella, C. Orthorexia nervosa: Validation of a diagnosis questionnaire. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2005, 10, e28–e32. [Google Scholar] [CrossRef]
- Chard, C.A.; Hilzendegen, C.; Barthels, F.; Stroebele-Benschop, N. Psychometric evaluation of the English version of the Düsseldorf Orthorexie Scale (DOS) and the prevalence of orthorexia nervosa among a U.S. student sample. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2019, 24, 275–281. [Google Scholar] [CrossRef]
- Vaccari, G.; Cutino, A.; Luisi, F.; Giambalvo, N.; Daneshmand, S.N.; Pinelli, M.; Maina, G.; Galeazzi, G.M.; Kaleci, S.; Albert, U.; et al. Is orthorexia nervosa a feature of obsessive—Compulsive disorder? A multicentric, controlled study. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2021, 26, 2531–2544. [Google Scholar] [CrossRef] [PubMed]
- Anil, C.; Aritici, G.; Ari, H.; Tutuncu, N.B. Prevalence of orthorexia in diabetic patients. Endocr. Abstr. 2015, 37. [Google Scholar] [CrossRef]
- Oberle, C.D.; Samaghabadi, R.O.; Hughes, E.M. Orthorexia nervosa: Assessment and correlates with gender, BMI, and personality. Appetite 2017, 108, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Forman, S.F.; McKenzie, N.; Hehn, R.; Monge, M.C.; Kapphahn, C.J.; Mammel, K.A.; Callahan, S.T.; Sigel, E.J.; Bravender, T.; Romano, M.; et al. Predictors of Outcome at 1 Year in Adolescents with DSM-5 Restrictive Eating Disorders: Report of the National Eating Disorders Quality Improvement Collaborative. J. Adolesc. Health 2014, 55, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Keller, M.F.; Konradsen, H. Ortoreksi blandt unge fitness-medlemmer. Klin. Sygepleje 2013, 27, 63–71. [Google Scholar] [CrossRef]
- Fidan, T.; Ertekin, V.; Işikay, S.; Kırpınar, I. Prevalence of orthorexia among medical students in Erzurum, Turkey. Compr. Psychiatry 2010, 51, 49–54. [Google Scholar] [CrossRef]
- Strahler, J. Sex differences in orthorexic eating behaviors: A systematic review and meta-analytical integration. Nutrition 2019, 67, 110534. [Google Scholar] [CrossRef]
- Hyrnik, J.; Janas-Kozik, M.; Stochel, M.; Jelonek, I.; Siwiec, A.; Rybakowski, J.K. The assessment of orthorexia nervosa among 1899 Polish adolescents using the ORTO-15 questionnaire. Int. J. Psychiatry Clin. Pract. 2016, 20, 199–203. [Google Scholar] [CrossRef]
- Tremelling, K.; Sandon, L.; Vega, G.L.; McAdams, C.J. Orthorexia Nervosa and Eating Disorder Symptoms in Registered Dietitian Nutritionists in the United States. J. Acad. Nutr. Diet. 2017, 117, 1612–1617. [Google Scholar] [CrossRef]
- Chaniotis, D.; Soultatou, P.; Letsios, A.; Chaniotis, F.I. Assessing Nutritional Habits and Self-Perception Factors to Develop a Standard Questionnaire for Diagnosing “Orthorexic” Behavior: ORTO 7E. J. Sci. Technol. 2011, 6, 53–67. [Google Scholar]
- Reynolds, R. Is the prevalence of orthorexia nervosa in an Australian university population 6.5%? Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2018, 23, 453–458. [Google Scholar] [CrossRef]
- Strahler, J.; Haddad, C.; Salameh, P.; Sacre, H.; Obeid, S.; Hallit, S. Cross-cultural differences in orthorexic eating behaviors: Associations with personality traits. Nutrition 2020, 77, 110811. [Google Scholar] [CrossRef] [PubMed]
- Gramaglia, C.; Gambaro, E.; Delicato, C.; Marchetti, M.; Sarchiapone, M.; Ferrante, D.; Roncero, M.; Perpiñá, C.; Brytek-Matera, A.; Wojtyna, E.; et al. Orthorexia nervosa, eating patterns and personality traits: A cross-cultural comparison of Italian, Polish and Spanish university students. BMC Psychiatry 2019, 19, 235. [Google Scholar] [CrossRef] [PubMed]
- Kass, A.E.; Kolko, R.P.; Wilfley, D.E. Psychological treatments for eating disorders. Curr. Opin. Psychiatry 2013, 26, 549–555. [Google Scholar] [CrossRef]
- Cerniglia, L.; Cimino, S.; Tafà, M.; Marzilli, E.; Ballarotto, G.; Bracaglia, F. Family profiles in eating disorders: Family functioning and psychopathology. Psychol. Res. Behav. Manag. 2017, 10, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Darling, K.E.; Ranzenhofer, L.M.; Hadley, W.; Villalta, D.; Kasper, V.; Jelalian, E. Negative childhood experiences and disordered eating in adolescents in a weight management program: The role of depressive symptoms. Eat. Behav. 2020, 38, 101402. [Google Scholar] [CrossRef] [PubMed]
- Altman, S.E.; Shankman, S.A. What is the association between obsessive—Compulsive disorder and eating disorders? Clin. Psychol. Rev. 2009, 29, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Brytek-Matera, A.; Pardini, S.; Modrzejewska, J.; Modrzejewska, A.; Szymańska, P.; Czepczor-Bernat, K.; Novara, C. Orthorexia Nervosa and its association with obsessive—Compulsive disorder symptoms: Initial cross-cultural comparison between Polish and Italian university students. Eat. Weight Disord. 2021. [Google Scholar] [CrossRef]
- Barnett, M.J.; Dripps, W.R.; Blomquist, K.K. Organivore or organorexic? Examining the relationship between alternative food network engagement, disordered eating, and special diets. Appetite 2016, 105, 713–720. [Google Scholar] [CrossRef]
- Brytek-Matera, A.; Donini, L.M.; Krupa, M.; Poggiogalle, E.; Hay, P. Orthorexia nervosa and self-attitudinal aspects of body image in female and male university students. J. Eat. Disord. 2015, 3, 1–8. [Google Scholar] [CrossRef]
- Barthels, F.; Meyer, F.; Pietrowsky, R. Orthorexic and restrained eating behaviour in vegans, vegetarians, and individuals on a diet. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2018, 23, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Luck-Sikorski, C.; Jung, F.; Schlosser, K.; Riedel-Heller, S.G. Is orthorexic behavior common in the general public? A large representative study in Germany. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2019, 24, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Dunn, T.M.; Gibbs, J.; Whitney, N.; Starosta, A. Prevalence of orthorexia nervosa is less than 1%: Data from a US sample. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2017, 22, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Çiçekoğlu, P.; Tunçay, G.Y. A Comparison of Eating Attitudes between Vegans/Vegetarians and Nonvegans/Nonvegetarians in Terms of Orthorexia Nervosa. Arch. Psychiatr. Nurs. 2018, 32, 200–205. [Google Scholar] [CrossRef]
- Voglino, G.; Parente, E.; Bert, F.; Moro, G.L.; Corradi, A.; Lapiccirella, M.; Gualano, M.R.; Siliquini, R. Orthorexia Nervosa, a challenging evaluation: Analysis of a sample of customers from organic food stores. Psychol. Health Med. 2021, 26, 478–486. [Google Scholar] [CrossRef]
- Segura-García, C.; Papaianni, M.C.; Caglioti, F.; Procopio, L.; Nisticò, C.G.; Bombardiere, L.; Ammendolia, A.; Rizza, P.; De Fazio, P.; Capranica, L. Orthorexia nervosa: A frequent eating disordered behavior in athletes. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2012, 17, e226–e233. [Google Scholar]
- Clifford, T.; Blyth, C. A pilot study comparing the prevalence of orthorexia nervosa in regular students and those in University sports teams. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2019, 24, 473–480. [Google Scholar] [CrossRef]
- Oberle, C.D.; Watkins, R.S.; Burkot, A.J. Orthorexic eating behaviors related to exercise addiction and internal motivations in a sample of university students. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2018, 23, 67–74. [Google Scholar] [CrossRef]
- Strahler, J.; Wachten, H.; Mueller-Alcazar, A. Obsessive healthy eating and orthorexic eating tendencies in sport and exercise contexts: A systematic review and meta-analysis. J. Behav. Addict. 2021, 10, 456–470. [Google Scholar] [CrossRef]
- Bartel, S.; Sherry, S.; Farthing, G.; Stewart, S. Classification of Orthorexia Nervosa: Further evidence for placement within the eating disorders spectrum. Eat. Behav. 2020, 38, 101406. [Google Scholar] [CrossRef]
- Karli, A.M. Dietary Habits of Young Persons with Orthorexic Behavior. Master’s Thesis, National School of Public Health, Athens, Greece, 2014. (In Greek). [Google Scholar]
- Grammatikopoulou, M.G.; Gkiouras, K.; Markaki, A.; Theodoridis, X.; Tsakiri, V.; Mavridis, P.; Dardavessis, T.; Chourdakis, M. Food addiction, orthorexia, and food-related stress among dietetics students. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2018, 23, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.; Melo, R.; Pereira, B.D. Orthorexia nervosa and comorbid depression successfully treated with mirtazapine: A case report. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2020, 25, 163–167. [Google Scholar] [CrossRef]
- Rania, M.; de Filippis, R.; Caroleo, M.; Carbone, E.; Aloi, M.; Bratman, S.; Segura-Garcia, C. Pathways to orthorexia nervosa: A case series discussion. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2021, 26, 1675–1683. [Google Scholar] [CrossRef] [PubMed]
- Reeves, G.M.; Mazaheri, S.; Snitker, S.; Langenberg, P.; Giegling, I.; Hartmann, A.M.; Konte, B.; Friedl, M.; Okusaga, O.; Groer, M.W.; et al. A Positive Association between T. gondii Seropositivity and Obesity. Front. Public Health 2013, 1, 73. [Google Scholar] [CrossRef] [PubMed]
- Huke, V.; Turk, J.; Saeidi, S.; Kent, A.; Morgan, J.F. Autism Spectrum Disorders in Eating Disorder Populations: A Systematic Review. Eur. Eat. Disord. Rev. 2013, 21, 345–351. [Google Scholar] [CrossRef]
- Kalra, S.; Kapoor, N.; Jacob, J. Orthorexia nervosa. J. Pak. Med. Assoc. 2020, 70, 1282–1284. [Google Scholar]
- Misra, M.; Klibanski, A. Anorexia Nervosa and Its Associated Endocrinopathy in Young People. Horm. Res. Paediatr. 2016, 85, 147–157. [Google Scholar] [CrossRef]
- Cashman, K.D. Vitamin D in childhood and adolescence. Postgrad. Med. J. 2007, 83, 230–235. [Google Scholar] [CrossRef]
- Barthels, F.; Meyer, F.; Huber, T.; Pietrowsky, R. Orthorexic eating behaviour as a coping strategy in patients with anorexia nervosa. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2017, 22, 269–276. [Google Scholar] [CrossRef]
- Grammatikopoulou, M.G.; Gkiouras, K.; Polychronidou, G.; Kaparounaki, C.; Gkouskou, K.K.; Magkos, F.; Donini, L.M.; Eliopoulos, A.G.; Goulis, D.G. Obsessed with Healthy Eating: A Systematic Review of Observational Studies Assessing Orthorexia Nervosa in Patients with Diabetes Mellitus. Nutrients 2021, 13, 3823. [Google Scholar] [CrossRef]
- Hausmann, J.S.; Touloumtzis, C.; White, M.T.; Colbert, J.A.; Gooding, H.C. Adolescent and Young Adult Use of Social Media for Health and Its Implications. J. Adolesc. Health 2017, 60, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Huang, C. Internet use and psychological well-being: A meta-analysis. Cyberpsychol. Behav. Soc. Netw. 2010, 13, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Radovic, A.; Gmelin, T.; Stein, B.D.; Miller, E. Depressed adolescents’ positive and negative use of social media. J. Adolesc. 2017, 55, 5–15. [Google Scholar] [CrossRef]
- Shaw, H.; Ramirez, L.; Trost, A.; Randall, P.; Stice, E. Body Image and Eating Disturbances across Ethnic Groups: More Similarities Than Differences. Psychol. Addict. Behav. 2004, 18, 12–18. [Google Scholar] [CrossRef]
- Levine, M.P.; Murnen, S.K. “Everybody Knows That Mass Media are/are not [pick one] a Cause of Eating Disorders”: A Critical Review of Evidence for a Causal Link between Media, Negative Body Image, and Disordered Eating in Females. J. Soc. Clin. Psychol. 2009, 28, 9–42. [Google Scholar] [CrossRef]
- Campaioli, G.; Sale, E.; Simonelli, A.; Pomini, V. The Dual Value of the Web: Risks and Benefits of the Use of the Internet in Disorders with A Self-Destructive Component in Adolescents and Young Adults. Int. J. Fam. Ther. 2017, 39, 301–313. [Google Scholar] [CrossRef]
- Saul, J.S.; Rodgers, R.F. Adolescent Eating Disorder Risk and the Online World. Child Adolesc. Psychiatr. Clin. N. Am. 2018, 27, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Saul, J.; Rodgers, R.F.; Saul, M. Adolescent Eating Disorder Risk and the Social Online World: An Update. Child Adolesc. Psychiatr. Clin. 2022, 31, 167–177. [Google Scholar] [CrossRef]
- McCartney, M. Margaret McCartney: Clean eating and the cult of healthism. BMJ 2016, 354, i4095. [Google Scholar] [CrossRef]
- Syurina, E.V.; Bood, Z.M.; Ryman, F.V.M.; Muftugil-Yalcin, S. Cultural Phenomena Believed to Be Associated with Orthorexia Nervosa—Opinion Study in Dutch Health Professionals. Front. Psychol. 2018, 9, 1419. [Google Scholar] [CrossRef]
- Lupton, D.; Feldman, Z. Digital Food Cultures; Routledge: Aingdon, UK; New York, NY, USA, 2020. [Google Scholar]
- Kalra, S.; Kumar, A. Quinary prevention: Defined and conceptualized. J. Pak. Med. Assoc. 2019, 69, 1765–11766. [Google Scholar] [PubMed]
- Zickgraf, H.F. Treatment of Pathologic Healthy Eating (Orthorexia Nervosa). In Advanced Casebook of Obsessive—Compulsive and Related Disorders: Conceptualizations and Treatment; Elsevier Academic Press: San Diego, CA, USA, 2020; pp. 21–40. [Google Scholar]
- Alemany, M. Alemany Metabolic Syndrome: A Multifaceted Disease of Affluence. J. Endocrinol. Metab. 2012, 2, 155–165. [Google Scholar] [CrossRef][Green Version]
- Aarnio, K.; Lindeman, M. Magical food and health beliefs: A portrait of believers and functions of the beliefs. Appetite 2004, 43, 65–74. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gkiouleka, M.; Stavraki, C.; Sergentanis, T.N.; Vassilakou, T. Orthorexia Nervosa in Adolescents and Young Adults: A Literature Review. Children 2022, 9, 365. https://doi.org/10.3390/children9030365
Gkiouleka M, Stavraki C, Sergentanis TN, Vassilakou T. Orthorexia Nervosa in Adolescents and Young Adults: A Literature Review. Children. 2022; 9(3):365. https://doi.org/10.3390/children9030365
Chicago/Turabian StyleGkiouleka, Maria, Christina Stavraki, Theodoros N. Sergentanis, and Tonia Vassilakou. 2022. "Orthorexia Nervosa in Adolescents and Young Adults: A Literature Review" Children 9, no. 3: 365. https://doi.org/10.3390/children9030365
APA StyleGkiouleka, M., Stavraki, C., Sergentanis, T. N., & Vassilakou, T. (2022). Orthorexia Nervosa in Adolescents and Young Adults: A Literature Review. Children, 9(3), 365. https://doi.org/10.3390/children9030365