
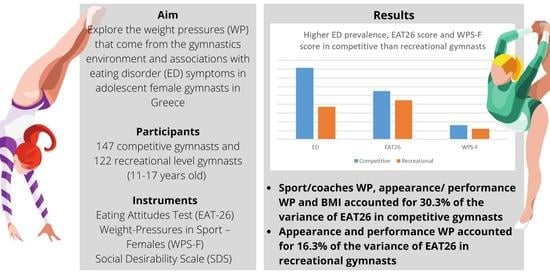
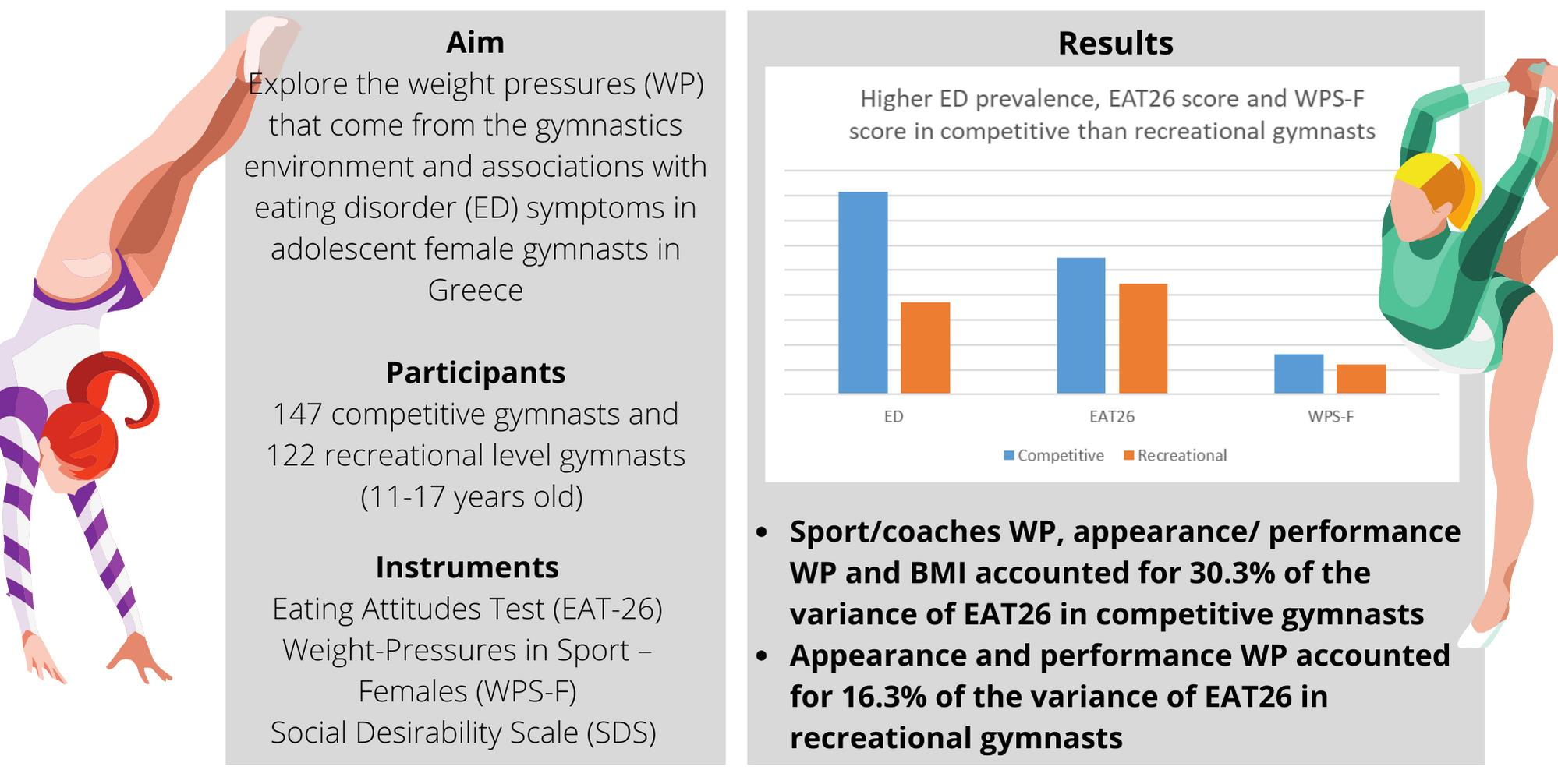
Weight Pressures and Eating Disorder Symptoms among Adolescent Female Gymnasts of Different Performance Levels in Greece




Abstract
1. Introduction
2. Materials and Methods
2.1. Participants’ Recruitment and Inclusion Criteria
2.2. Ethical Permission, Consent and Anonymity
2.3. Questionnaires and Tools applied
2.3.1. Eating Attitudes Test-26
2.3.2. Weight Pressures in Sport-Females
2.3.3. Social Desirability Scale
2.3.4. Other Information
2.3.5. Anthropometric Indices
2.4. Statistical Analyses
3. Results
3.1. Population Characteristics
3.2. Eating Disorder Symptoms and Weight Pressures
3.3. Regression Analyses
4. Discussion
4.1. Prevalence of Eating Disorder Symptoms
4.2. Weight Pressures between Competitive and Non-Competitive Gymnasts
4.3. Associations between Weight-Pressures and Eating Disorder Symptoms
4.4. Limitations
4.5. Strengths of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fédération Internationale de Gymnastique. FIG—Population. Available online: https://www.gymnastics.sport/site/pages/about-population.php (accessed on 29 December 2021).
- Fédération Internationale de Gymnastique. FIG—Disciplines. Available online: https://www.gymnastics.sport/site/discipline.php?disc=1 (accessed on 15 March 2021).
- Malina, R.M.; Baxter-Jones, A.D.G.; Armstrong, N.; Beunen, G.P.; Caine, D.; Daly, R.M.; Lewis, R.D.; Rogol, A.D.; Russell, K. Role of Intensive Training in the Growth and Maturation of Artistic Gymnasts. Sports Med. 2013, 43, 783–802. [Google Scholar] [CrossRef] [PubMed]
- Brooks, T.J. Women’s Collegiate Gymnastics: A Multifactorial Approach to Training and Conditioning. Strength Cond. J. 2003, 25, 23–37. [Google Scholar] [CrossRef]
- Bacciotti, S.; Baxter-Jones, A.; Gaya, A.; Maia, J. The Physique of Elite Female Artistic Gymnasts: A Systematic Review. J. Hum. Kinet. 2017, 58, 247–259. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, H.; Slater, G. Losing, Gaining and Making Weight for Athletes. In Sport and Exercise Nutrition; John Wiley & Sons, Ltd.: New York, NY, USA, 2011; pp. 210–232. ISBN 978-1-4443-4490-5. [Google Scholar]
- Sundgot-Borgen, J.; Garthe, I. Elite Athletes in Aesthetic and Olympic Weight-Class Sports and the Challenge of Body Weight and Body Composition. J. Sports Sci. 2011, 29 (Suppl. S1), S101–S114. [Google Scholar] [CrossRef]
- Claessens, A.L.; Lefevre, J.; Beunen, G.; Malina, R.M. The Contribution of Anthropometric Characteristics to Performance Scores in Elite Female Gymnasts. J. Sports Med. Phys. Fit. 1999, 39, 355–360. [Google Scholar]
- Sherman, R.T.; Thompson, R.A.; Rose, J.S. Body Mass Index and Athletic Performance in Elite Female Gymnasts. J. Sport Behav. 1996, 19, 338–346. [Google Scholar]
- Malina, R.M. Physical Growth and Biological Maturation of Young Athletes. Exerc. Sport Sci. Rev. 1994, 22, 389–433. [Google Scholar] [CrossRef]
- Georgopoulos, N.; Markou, K.; Theodoropoulou, A.; Paraskevopoulou, P.; Varaki, L.; Kazantzi, Z.; Leglise, M.; Vagenakis, A.G. Growth and Pubertal Development in Elite Female Rhythmic Gymnasts. J. Clin. Endocrinol. Metab. 1999, 84, 4525–4530. [Google Scholar] [CrossRef]
- Taboada-Iglesias, Y.; Santana, M.V.; Gutiérrez-Sánchez, Á. Anthropometric Profile in Different Event Categories of Acrobatic Gymnastics. J. Hum. Kinet. 2017, 57, 169–179. [Google Scholar] [CrossRef]
- Sundgot-Borgen, J. Eating Disorders, Energy Intake, Training Volume, and Menstrual Function in High-Level Modern Rhythmic Gymnasts. Int. J. Sport Nutr. 1996, 6, 100–109. [Google Scholar] [CrossRef]
- Okano, G.; Holmes, R.A.; Mu, Z.; Yang, P.; Lin, Z.; Nakai, Y. Disordered Eating in Japanese and Chinese Female Runners, Rhythmic Gymnasts and Gymnasts. Int. J. Sports Med. 2005, 26, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.; Petrie, T.A. Prevalence of Disordered Eating and Pathogenic Weight Control Behaviors among NCAA Division I Female Collegiate Gymnasts and Swimmers. Res. Q Exerc. Sport 2012, 83, 120–124. [Google Scholar] [CrossRef] [PubMed]
- de Bruin, A.P.; Oudejans, R.R.D.; Bakker, F.C. Dieting and Body Image in Aesthetic Sports: A Comparison of Dutch Female Gymnasts and Non-Aesthetic Sport Participants. Psychol. Sport Exerc. 2007, 8, 507–520. [Google Scholar] [CrossRef]
- Krentz, E.M.; Warschburger, P. A Longitudinal Investigation of Sports-Related Risk Factors for Disordered Eating in Aesthetic Sports. Scand. J. Med. Sci. Sports 2013, 23, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Sundgot-Borgen, J.; Meyer, N.L.; Lohman, T.G.; Ackland, T.R.; Maughan, R.J.; Stewart, A.D.; Müller, W. How to Minimise the Health Risks to Athletes Who Compete in Weight-Sensitive Sports Review and Position Statement on Behalf of the Ad Hoc Research Working Group on Body Composition, Health and Performance, under the Auspices of the IOC Medical Commission. Br. J. Sports Med. 2013, 47, 1012–1022. [Google Scholar] [CrossRef]
- Cupisti, A.; D’Alessandro, C.; Castrogiovanni, S.; Barale, A.; Morelli, E. Nutrition Survey in Elite Rhythmic Gymnasts. J. Sports Med. Phys. Fit. 2000, 40, 350–355. [Google Scholar]
- Michopoulou, E.; Avloniti, A.; Kambas, A.; Leontsini, D.; Michalopoulou, M.; Tournis, S.; Fatouros, I.G. Elite Premenarcheal Rhythmic Gymnasts Demonstrate Energy and Dietary Intake Deficiencies during Periods of Intense Training. Pediatr. Exerc. Sci. 2011, 23, 560–572. [Google Scholar] [CrossRef]
- Silva, M.-R.G.; Paiva, T. Low Energy Availability and Low Body Fat of Female Gymnasts before an International Competition. Eur. J. Sport Sci. 2014, 15, 591–599. [Google Scholar] [CrossRef]
- Silva, M.-R.G.; Silva, H.-H.; Paiva, T. Sleep Duration, Body Composition, Dietary Profile and Eating Behaviours among Children and Adolescents: A Comparison between Portuguese Acrobatic Gymnasts. Eur. J. Pediatrics 2018, 177, 815–825. [Google Scholar] [CrossRef]
- Villa, M.; Villa-Vicente, J.G.; Seco-Calvo, J.; Mielgo-Ayuso, J.; Collado, P.S. Body Composition, Dietary Intake and the Risk of Low Energy Availability in Elite-Level Competitive Rhythmic Gymnasts. Nutrients 2021, 13, 2083. [Google Scholar] [CrossRef]
- Miteva, S.; Yanev, I.; Kolimechkov, S.; Petrov, L.; Mladenov, L.; Georgieva, V.; Somlev, P. Nutrition and Body Composition of Elite Rhythmic Gymnasts from Bulgaria. Int. J. Sports Sci. Coach. 2019, 15, 108–116. [Google Scholar] [CrossRef]
- Dallas, G.; Dallas, C.; Simatos, J. Nutritional Status and Dietary Assessment of Elite Female Artistic and Rythmic Gymnasts—A Case Study. Sci. Gymnast. J. 2016, 8, 16. [Google Scholar]
- Soric, M.; Misigoj-Durakovic, M.; Pedisic, Z. Dietary Intake and Body Composition of Prepubescent Female Aesthetic Athletes. Int. J. Sport Nutr. Exerc. Metab. 2008, 18, 343–354. [Google Scholar] [CrossRef]
- D’Alessandro, C.; Morelli, E.; Evangelisti, I.; Galetta, F.; Franzoni, F.; Lazzeri, D.; Piazza, M.; Cupisti, A. Profiling the Diet and Body Composition of Subelite Adolescent Rhythmic Gymnasts. Pediatr. Exerc. Sci. 2007, 19, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Martinsen, M.T.; Sundgot-Borgen, J. Higher Prevalence of Eating Disorders among Adolescent Elite Athletes than Controls. Med. Sci. Sports Exerc. 2013, 45, 1188–1197. [Google Scholar] [CrossRef] [PubMed]
- Nordin, S.M.; Harris, G.; Cumming, J. Disturbed Eating in Young, Competitive Gymnasts: Differences between Three Gymnastics Disciplines. Eur. J. Sport Sci. 2003, 3, 1–14. [Google Scholar] [CrossRef]
- Tan, J.O.A.; Calitri, R.; Bloodworth, A.; McNamee, M.J. Understanding Eating Disorders in Elite Gymnastics: Ethical and Conceptual Challenges. Clin. Sports Med. 2016, 35, 275–292. [Google Scholar] [CrossRef]
- Theodorakou, K.; Donti, O. Prevalence of Eating Disorders and Psychological Parameters in Elite Female Gymnasts: Their Relation to Body Image and Body Mass Index. Athlitiki Psychol. 2013, 24, 11–23. [Google Scholar]
- Donti, O.; Donti, A.; Gaspari, V.; Pleksida, P.; Psychountaki, M. Are They Too Perfect to Eat Healthy? Association between Eating Disorder Symptoms and Perfectionism in Adolescent Rhythmic Gymnasts. Eat. Behav. 2021, 41, 101514. [Google Scholar] [CrossRef]
- Sweeney, E.; Howell, D.R.; Seehusen, C.N.; Tilley, D.; Casey, E. Health Outcomes among Former Female Collegiate Gymnasts: The Influence of Sport Specialization, Concussion, and Disordered Eating. Phys. Sports Med. 2020, 49, 1–7. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 978-0-89042-555-8. [Google Scholar]
- Reardon, C.L.; Hainline, B.; Aron, C.M.; Baron, D.; Baum, A.L.; Bindra, A.; Budgett, R.; Campriani, N.; Castaldelli-Maia, J.M.; Currie, A.; et al. Mental Health in Elite Athletes: International Olympic Committee Consensus Statement. Br. J. Sports Med. 2019, 53, 667–699. [Google Scholar] [CrossRef] [PubMed]
- Bonci, C.M.; Bonci, L.J.; Granger, L.R.; Johnson, C.L.; Malina, R.M.; Milne, L.W.; Ryan, R.R.; Vanderbunt, E.M. National Athletic Trainers’ Association Position Statement: Preventing, Detecting, and Managing Disordered Eating in Athletes. J. Athl. Train 2008, 43, 80–108. [Google Scholar] [CrossRef] [PubMed]
- Golden, N.H.; Schneider, M.; Wood, C. Preventing Obesity and Eating Disorders in Adolescents. Pediatrics 2016, 138, e20161649. [Google Scholar] [CrossRef] [PubMed]
- Rosen, D.S. The Committee on Adolescence Identification and Management of Eating Disorders in Children and Adolescents. Pediatrics 2010, 126, 1240–1253. [Google Scholar] [CrossRef]
- Desbrow, B.; McCormack, J.; Burke, L.M.; Cox, G.R.; Fallon, K.; Hislop, M.; Logan, R.; Marino, N.; Sawyer, S.M.; Shaw, G.; et al. Sports Dietitians Australia Position Statement: Sports Nutrition for the Adolescent Athlete. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 570–584. [Google Scholar] [CrossRef]
- Bingham, M.E.; Borkan, M.; Quatromoni, P. Sports Nutrition Advice for Adolescent Athletes: A Time to Focus on Food. Am. J. Lifestyle Med. 2015, 9, 398–402. [Google Scholar] [CrossRef]
- Kontele, I.; Vassilakou, T. Nutritional Risks among Adolescent Athletes with Disordered Eating. Children 2021, 8, 715. [Google Scholar] [CrossRef]
- Nattiv, A.; Loucks, A.B.; Manore, M.M.; Sanborn, C.F.; Sundgot-Borgen, J.; Warren, M.P.; American College of Sports Medicine American College of Sports Medicine Position Stand. The Female Athlete Triad. Med. Sci. Sports Exerc. 2007, 39, 1867–1882. [Google Scholar] [CrossRef]
- Sundgot-Borgen, J.; Torstveit, M.K. Prevalence of Eating Disorders in Elite Athletes Is Higher than in the General Population. Clin. J. Sport Med. 2004, 14, 25–32. [Google Scholar] [CrossRef]
- Mancine, R.P.; Gusfa, D.W.; Moshrefi, A.; Kennedy, S.F. Prevalence of Disordered Eating in Athletes Categorized by Emphasis on Leanness and Activity Type—A Systematic Review. J. Eat. Disord. 2020, 8, 47. [Google Scholar] [CrossRef]
- Kong, P.; Harris, L.M. The Sporting Body: Body Image and Eating Disorder Symptomatology Among Female Athletes from Leanness Focused and Nonleanness Focused Sports. J. Psychol. 2015, 149, 141–160. [Google Scholar] [CrossRef] [PubMed]
- Francisco, R.; Narciso, I.; Alarcão, M. Individual and Relational Risk Factors for the Development of Eating Disorders in Adolescent Aesthetic Athletes and General Adolescents. Eat. Weight Disord. 2013, 18, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Voelker, D.K.; Gould, D.; Reel, J.J. Prevalence and Correlates of Disordered Eating in Female Figure Skaters. Psychol. Sport Exerc. 2014, 15, 696–704. [Google Scholar] [CrossRef]
- Ravi, S.; Ihalainen, J.K.; Taipale-Mikkonen, R.S.; Kujala, U.M.; Waller, B.; Mierlahti, L.; Lehto, J.; Valtonen, M. Self-Reported Restrictive Eating, Eating Disorders, Menstrual Dysfunction, and Injuries in Athletes Competing at Different Levels and Sports. Nutrients 2021, 13, 3275. [Google Scholar] [CrossRef]
- Teixidor-Batlle, C.; Ventura, C.; Andrés, A. Eating Disorder Symptoms in Elite Spanish Athletes: Prevalence and Sport-Specific Weight Pressures. Front. Psychol. 2021, 11, 559832. [Google Scholar] [CrossRef]
- Bratland-Sanda, S.; Sundgot-Borgen, J.K. Eating Disorders in Athletes: Overview of Prevalence, Risk Factors and Recommendations for Prevention and Treatment. Eur. J. Sport Sci. 2013, 13, 499–508. [Google Scholar] [CrossRef]
- Anderson, C.M.; Petrie, T.A.; Neumann, C.S. Effects of Sport Pressures on Female Collegiate Athletes: A Preliminary Longitudinal Investigation. Sport Exerc. Perform. Psychol. 2012, 1, 120–134. [Google Scholar] [CrossRef]
- de Bruin, A.P.K.; Oudejans, R.R.D.; Bakker, F.C.; Woertman, L. Contextual Body Image and Athletes’ Disordered Eating: The Contribution of Athletic Body Image to Disordered Eating in High Performance Women Athletes. Eur. Eat. Disord. Rev. 2011, 19, 201–215. [Google Scholar] [CrossRef]
- Petrie, T.A.; Greenleaf, C. Eating Disorders in Sport. Available online: https://www.oxfordhandbooks.com/view/10.1093/oxfordhb/9780199731763.001.0001/oxfordhb-9780199731763-e-34 (accessed on 16 September 2021).
- Reel, J.J.; Petrie, T.A.; SooHoo, S.; Anderson, C.M. Weight Pressures in Sport: Examining the Factor Structure and Incremental Validity of the Weight Pressures in Sport—Females. Eat. Behav. 2013, 14, 137–144. [Google Scholar] [CrossRef]
- Kerr, G.; Berman, E.; Souza, M.J.D. Disordered Eating in Women’s Gymnastics: Perspectives of Athletes, Coaches, Parents, and Judges. J. Appl. Sport Psychol. 2006, 18, 28–43. [Google Scholar] [CrossRef]
- Francisco, R.; Alarcão, M.; Narciso, I. Aesthetic Sports as High-Risk Contexts for Eating Disorders—Young Elite Dancers and Gymnasts Perspectives. Span. J. Psychol. 2012, 15, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Greenleaf, C. Weight Pressures and Social Physique Anxiety among Collegiate Synchronized Skaters. J. Sport Behav. 2004, 27, 260–276. [Google Scholar]
- Reel, J.J.; SooHoo, S.; Petrie, T.A.; Greenleaf, C.; Carter, J.E. Slimming down for Sport: Developing a Weight Pressures in Sport Measure for Female Athletes. J. Clin. Sport Psychol. 2010, 4, 99–111. [Google Scholar] [CrossRef]
- Reel, J.J.; Jamieson, K.; Soohoo, S.; Gill, D. Femininity to the Extreme: Body Image Concerns among College Female Dancers. Women Sport Phys. Act. J. 2005, 14, 39–51. [Google Scholar] [CrossRef]
- SooHoo, S.; Reel, J.J.; Pearce, P.F. Socially Constructed Body Image of Female Adolescent Cheerleaders. Women Sport Phys. Act. J. 2011, 20, 22–34. [Google Scholar] [CrossRef]
- Torres-McGehee, T.M.; Monsma, E.V.; Dompier, T.P.; Washburn, S.A. Eating Disorder Risk and the Role of Clothing in Collegiate Cheerleaders’ Body Images. J. Athl. Train 2012, 47, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Gill, D.; Reel, J. Slim Enough to Swim? Weight Pressures for Competitive Swimmers and Coaching Implications. Sport J. 2001, 4, 1–4. [Google Scholar]
- Reel, J.J.; Gill, D.L. Psychosocial Factors Related to Eating Disorders among High School and College Female Cheerleaders. Sport Psychol. 1996, 10, 195–206. [Google Scholar] [CrossRef][Green Version]
- Yannakoulia, M.; Sitara, M.; Matalas, A.-L. Reported Eating Behavior and Attitudes Improvement after a Nutrition Intervention Program in a Group of Young Female Dancers. Int. J. Sport Nutr. Exerc. Metab. 2002, 12, 24–32. [Google Scholar] [CrossRef]
- Michou, M.; Costarelli, V. Disordered Eating Attitudes in Relation to Anxiety Levels, Self-Esteem and Body Image in Female Basketball Players. J. Exerc. Sci. Fit. 2011, 9, 109–115. [Google Scholar] [CrossRef]
- Chaikali, P.; Vassilakou, Τ. Comparison of Eating Habits and Physical Characteristics of Adolescent Dancers and Peers of the General Population. In Proceedings of the 9th Panhellenic Conference on Public Health and Health Services, Athens, Greece, 9 March 2012; p. 72. [Google Scholar]
- Gonidakis, F.; Liakopoulou, E.; Psychountaki, M.; Varsou, E.; Soldatos, K. Differences in Eating Disorder Symptomatology between Athletes and Non-Athletes. Arch. Hell. Med. 2008, 25, 341–347. [Google Scholar]
- Costarelli, V.; Stamou, D. Emotional Intelligence, Body Image and Disordered Eating Attitudes in Combat Sport Athletes. J. Exerc. Sci. Fit. 2009, 7, 104–111. [Google Scholar] [CrossRef]
- Garner, D.M.; Garfinkel, P.E. The Eating Attitudes Test: An Index of the Symptoms of Anorexia Nervosa. Psychol. Med. 1979, 9, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Douka, A.; Grammatopoulou, E.; Skordilis, E.; Koutsouki, D. Factor Analysis and Cut-off Score of the 26-Item Eating Attitudes Test in a Greek Sample. J. Biol. Exerc. 2009, 5, 51–68. [Google Scholar] [CrossRef]
- Kontele, I.; Vassilakou, T.; Psychountaki, M.; Donti, O. Psychometric Characteristics of the Greek Version of Weight Pressures in Sport-Females (WPS-F) Questionnaire. In Proceedings of the 6th Congress of Sport Science, Athens, Greece, 26–28 March 2021; p. 140. [Google Scholar]
- Reynolds, W.M. Development of Reliable and Valid Short Forms of the Marlowe-Crowne Social Desirability Scale. J. Clin. Psychol. 1982, 38, 119–125. [Google Scholar] [CrossRef]
- Psychountaki, M.; Ekkekakis, P.; Zervas, I. Short-form of Social Desirability Scale: Adaptation of the Marlowe-Crowne Scale; Unpublished Research; Department of Physical Education & Sport Science, National & Kapodistrian University of Athens: Athens, Greece, 1993. [Google Scholar]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Jankauskiene, R.; Baceviciene, M. Body Image and Disturbed Eating Attitudes and Behaviors in Sport-Involved Adolescents: The Role of Gender and Sport Characteristics. Nutrients 2019, 11, 3061. [Google Scholar] [CrossRef]
- Toro, J.; Galilea, B.; Martinez-Mallén, E.; Salamero, M.; Capdevila, L.; Mari, J.; Mayolas, J.; Toro, E. Eating Disorders in Spanish Female Athletes. Int. J. Sports Med. 2005, 26, 693–700. [Google Scholar] [CrossRef]
- Muscat, A.; Long, B. Critical Comments About Body Shape and Weight: Disordered Eating of Female Athletes and Sport Participants. J. Appl. Sport Psychol. 2008, 20, 1–24. [Google Scholar] [CrossRef]
- Ranby, K.W.; Aiken, L.S.; MacKinnon, D.P.; Elliot, D.L.; Moe, E.L.; McGinnis, W.; Goldberg, L. A Mediation Analysis of the ATHENA Intervention for Female Athletes: Prevention of Athletic-Enhancing Substance Use and Unhealthy Weight Loss Behaviors. J. Pediatr. Psychol. 2009, 34, 1069–1083. [Google Scholar] [CrossRef]
- Anderson, C.M.; Petrie, T.A.; Neumann, C.S. Psychosocial Correlates of Bulimic Symptoms among NCAA Division-I Female Collegiate Gymnasts and Swimmers/Divers. J. Sport Exerc. Psychol. 2011, 33, 483–505. [Google Scholar] [CrossRef] [PubMed]
- Heradstveit, O.; Hysing, M.; Nilsen, S.A.; Bøe, T. Symptoms of Disordered Eating and Participation in Individual- and Team Sports: A Population-Based Study of Adolescents. Eat. Behav. 2020, 39, 101434. [Google Scholar] [CrossRef] [PubMed]
- Costa, N.F.D.; Schtscherbyna, A.; Soares, E.A.; Ribeiro, B.G. Disordered Eating among Adolescent Female Swimmers: Dietary, Biochemical, and Body Composition Factors. Nutrition 2013, 29, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Pustivšek, S.; Hadžić, V.; Dervišević, E.; Carruthers, J. Risk for Eating Disorders and Body Composition among Adolescent Female and Male Athletes and Non-Athlete Controls. Int. J. Adolesc. Med. Health 2020, 32, 20170190. [Google Scholar] [CrossRef]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American College of Sports Medicine Joint Position Statement. Nutrition and Athletic Performance. Med. Sci. Sports Exerc. 2016, 48, 543–568. [Google Scholar] [CrossRef] [PubMed]
- Berg, E.K. Performance Nutrition for the Adolescent Athlete: A Realistic Approach. Clin. J. Sport Med. 2019, 29, 345–352. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Competitive (n = 147) | Non-Competitive (n = 122) | X2 | p | ||
|---|---|---|---|---|---|
| Training Experience (years) | >8 years | 47 (32.2%) | 25 (20.7%) | 12.319 | 0.002 |
| 6–8 years | 60 (41.1%) | 39 (32.2%) | |||
| <6 years | 39 (26.7%) | 57 (47.1%) | |||
| Training frequency (sessions/week) | ≥5 sessions/week | 120 (81.6%) | 14 (11.6%) | 133.105 | <0.001 |
| 3–4 sessions/week | 23 (15.6%) | 69 (57.0%) | |||
| 1–2 sessions/week | 4 (2.7%) | 38 (31.4%) | |||
| Training session duration (hours/session) | >4 h | 36 (24.5%) | 0 (0.0%) | 118.908 | <0.001 |
| 3–4 h | 81 (55.1%) | 16 (13.3%) | |||
| 1–2 h | 30 (20.4%) | 104 (86.7%) | |||
| Competitions/Events Frequency (events/year) | >3/year | 51 (35.2%) | 26 (21.8%) | 35.326 | <0.001 |
| 2–3/year | 82 (56.6%) | 47 (39.5%) | |||
| 1/year | 12 (8.3%) | 46 (38.7%) | |||
| Competitive (n = 147) | Non-Competitive (n = 122) | t (df = 267) | p | Cohen’s d | |
|---|---|---|---|---|---|
| Age (years) | 13.89 ± 1.75 | 13.91 ± 1.76 | 0.064 | 0.949 | 0.01 |
| Height (cm) | 156.32 ± 8.72 | 158.78 ± 7.83 | 2.409 | 0.017 | 0.29 |
| Body weight (kg) | 45.93 ± 8.87 | 49.37 ± 8.48 | 3.223 | 0.001 | 0.39 |
| BMI (kg/m2) | 18.63 ± 2.32 | 19.49 ± 2.54 | 2.890 | 0.004 | 0.35 |
| Competitive (n = 147) | Non-Competitive (n = 122) | t | p | Cohen’s d | |
|---|---|---|---|---|---|
| EAT-26 | 10.99 ± 8.08 | 8.91 ± 6.95 | 2.230 | 0.027 | 0.27 |
| Dieting | 6.36 ± 6.03 | 5.06 ± 5.72 | 1.804 | 0.072 | 0.22 |
| Bulimia and Food Preoccupation | 0.74 ± 1.40 | 0.56 ± 1.19 | 1.089 | 0.277 | 0.14 |
| Oral Control | 3.79 ± 3.39 | 3.24 ± 2.77 | 1.457 | 0.146 | 0.18 |
| WPS-F | 3.23 ± 1.04 | 2.43 ± 0.95 | 6.562 | 0.000 | 0.80 |
| Pressures from Coaches and Sports about Weight | 3.50 ± 1.16 | 2.46 ± 1.17 | 7.285 | 0.000 | 0.89 |
| Pressures regarding Appearance and Performance | 2.91 ± 1.23 | 2.39 ± 1.13 | 3.568 | 0.000 | 0.44 |
| 95% CI | |||||||
|---|---|---|---|---|---|---|---|
| Variables | B | SE | Βeta | t | p | Lower | Upper |
| Pressures from Coaches and Sports about Weight | 1.510 | 0.563 | 0.217 | 2.681 | 0.008 | 0.397 | 2.624 |
| Pressures regarding Appearance and Performance | 2.954 | 0.589 | 0.449 | 5.012 | 0.000 | 1.789 | 4.119 |
| BMI | −1.554 | 0.273 | −0.447 | −5.692 | 0.000 | −2.094 | −1.014 |
| Adjusted R2 = 0.303, p < 0.001 | |||||||
| 95% CI | |||||||
|---|---|---|---|---|---|---|---|
| Variables | B | SE | Βeta | t | p | Lower | Upper |
| Pressures regarding Appearance and Performance | 2.523 | 0.510 | 0.412 | 4.948 | 0.000 | 1.514 | 3.533 |
| Adjusted R2 = 0.163, p < 0.001 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kontele, I.; Vassilakou, T.; Donti, O. Weight Pressures and Eating Disorder Symptoms among Adolescent Female Gymnasts of Different Performance Levels in Greece. Children 2022, 9, 254. https://doi.org/10.3390/children9020254
Kontele I, Vassilakou T, Donti O. Weight Pressures and Eating Disorder Symptoms among Adolescent Female Gymnasts of Different Performance Levels in Greece. Children. 2022; 9(2):254. https://doi.org/10.3390/children9020254
Chicago/Turabian StyleKontele, Ioanna, Tonia Vassilakou, and Olyvia Donti. 2022. "Weight Pressures and Eating Disorder Symptoms among Adolescent Female Gymnasts of Different Performance Levels in Greece" Children 9, no. 2: 254. https://doi.org/10.3390/children9020254
APA StyleKontele, I., Vassilakou, T., & Donti, O. (2022). Weight Pressures and Eating Disorder Symptoms among Adolescent Female Gymnasts of Different Performance Levels in Greece. Children, 9(2), 254. https://doi.org/10.3390/children9020254