
Feasibility of Mouth-to-Mouth Ventilation through FFP2 Respirator in BLS Training during COVID-19 Pandemic (MOVERESP Study): Simulation-Based Study

 , , ,
, , ,
Abstract
1. Introduction
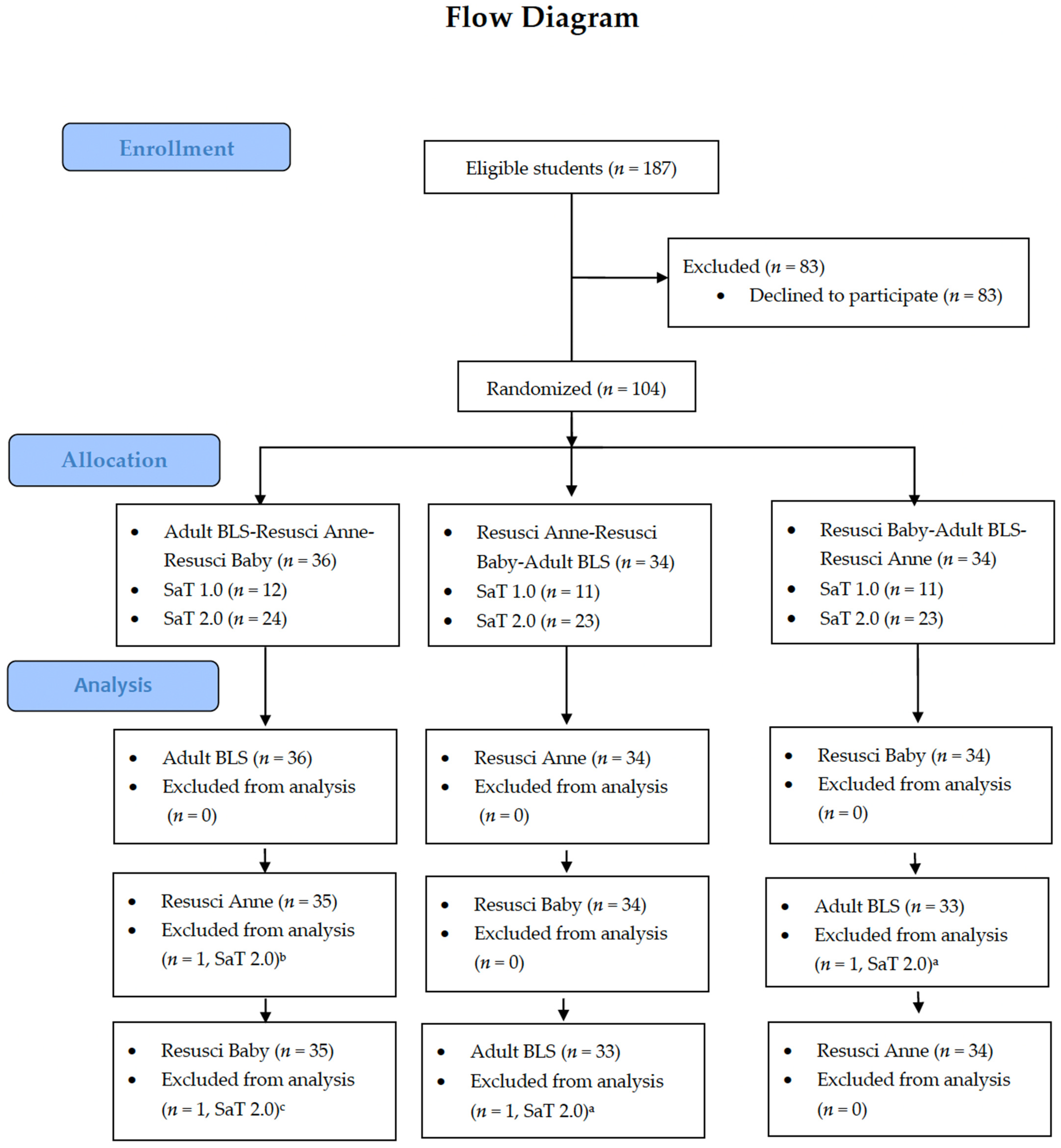
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, S.-Y.; Shin, D.; Kim, H.J.; Karm, M.-H. Changes of Knowledge and Practical Skills before and after Retraining for Basic Life Support: Focused on Students of Dental School. Int. J. Med. Sci. 2020, 17, 3082–3090. [Google Scholar] [CrossRef] [PubMed]
- Baldi, E.; Contri, E.; Bailoni, A.; Rendic, K.; Turcan, V.; Donchev, N.; Nadareishvili, I.; Petrica, A.-M.; Yerolemidou, I.; Petrenko, A.; et al. Final-Year Medical Students’ Knowledge of Cardiac Arrest and CPR: We Must Do More! Int. J. Cardiol. 2019, 296, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Pande, S.; Pande, S.; Parate, V.; Pande, S.; Sukhsohale, N. Evaluation of Retention of Knowledge and Skills Imparted to First-Year Medical Students through Basic Life Support Training. Adv. Physiol. Educ. 2014, 38, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Ralapanawa, D.M.P.U.K.; Jayawickreme, K.P.; Ekanayake, E.M.M.; Kumarasiri, P.V.R. A Study on the Knowledge and Attitudes on Advanced Life Support among Medical Students and Medical Officers in a Tertiary Care Hospital in Sri Lanka. BMC Res. Notes 2016, 9, 462. [Google Scholar] [CrossRef] [PubMed]
- WHO. Director-General’s Opening Remarks at the Media Briefing on COVID-19. 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 3 June 2021).
- Nolan, J.P.; Monsieurs, K.G.; Bossaert, L.; Böttiger, B.W.; Greif, R.; Lott, C.; Madar, J.; Olasveengen, T.M.; Roehr, C.C.; Semeraro, F.; et al. European Resuscitation Council COVID-19 Guidelines Executive Summary. Resuscitation 2020, 153, 45–55. [Google Scholar] [CrossRef]
- Riva, G.; Ringh, M.; Jonsson, M.; Svensson, L.; Herlitz, J.; Claesson, A.; Djärv, T.; Nordberg, P.; Forsberg, S.; Rubertsson, S.; et al. Survival in Out-of-Hospital Cardiac Arrest After Standard Cardiopulmonary Resuscita-Tion or Chest Compressions Only Before Arrival of Emergency Medical Services. Circulation 2019, 139, 2600–2609. [Google Scholar] [CrossRef]
- Hsu, C.H.; Neumar, R.W. To Breathe, or Not to Breathe, That Is the Question. Circulation 2019, 139, 2610–2612. [Google Scholar] [CrossRef]
- Olasveengen, T.M.; Semeraro, F.; Ristagno, G.; Castren, M.; Handley, A.; Kuzovlev, A.; Monsieurs, K.G.; Raffay, V.; Smyth, M.; Soar, J.; et al. European Resuscitation Council Guidelines 2021: Basic Life Support. Resuscitation 2021, 161, 98–114. [Google Scholar] [CrossRef]
- Van de Voorde, P.; Turner, N.M.; Djakow, J.; de Lucas, N.; Martinez-Mejias, A.; Biarent, D.; Bingham, R.; Brissaud, O.; Hoffmann, F.; Johannesdottir, G.B.; et al. European Resuscitation Council Guidelines 2021: Paediatric Life Support. Resuscitation 2021, 161, 327–387. [Google Scholar] [CrossRef]
- Baldi, E.; Contri, E.; Savastano, S.; Cortegiani, A. The Challenge of Laypeople Cardio-Pulmonary Resuscitation Training during and after COVID-19 Pandemic. Resuscitation 2020, 152, 3–4. [Google Scholar] [CrossRef]
- Lederer, W.; Isser, M. Barrier Resuscitation by Lay Rescuers during COVID-19 Pandemic. Med. Hypotheses 2021, 154, 110648. [Google Scholar] [CrossRef] [PubMed]
- Greif, R.; Lockey, A.; Breckwoldt, J.; Carmona, F.; Conaghan, P.; Kuzovlev, A.; Pflanzl-Knizacek, L.; Sari, F.; Shammet, S.; Scapigliati, A.; et al. European Resuscitation Council Guidelines 2021: Education for Resuscitation. Resuscitation 2021, 161, 388–407. [Google Scholar] [CrossRef] [PubMed]
- Chaplin, T.; McColl, T.; Petrosoniak, A.; Hall, A.K. “Building the Plane as You Fly”: Simulation during the COVID-19 Pandemic. Can. J. Emerg. Med. 2020, 22, 576–578. [Google Scholar] [CrossRef] [PubMed]
- Hanel, E.; Bilic, M.; Hassall, K.; Hastings, M.; Jazuli, F.; Ha, M.; Trotter, B.; Fraser, C.; Rutledge, G. Virtual Application of in Situ Simulation during a Pandemic. CJEM 2020. [Google Scholar] [CrossRef]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients. N. Engl. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef]
- Ueki, H.; Furusawa, Y.; Iwatsuki-Horimoto, K.; Imai, M.; Kabata, H.; Nishimura, H.; Kawaoka, Y. Effectiveness of Face Masks in Preventing Airborne Transmission of SARS-CoV-2. mSphere 2020, 5, e00637-20. [Google Scholar] [CrossRef]
- National Research Council (US) Chemical Sciences Roundtable. C. Carbon Management: Implications for R&D in the Chemical Sciences and Technology: A Workshop Report to the Chemical Sciences Roundtable. In Commodity Polymers from Renewable Resources: Polylactic Acid; National Academies Press: Washington, DC, USA, 2001. Available online: https://www.ncbi.nlm.nih.gov/books/NBK44131/ (accessed on 3 June 2021).
- Scully, J.R. The COVID-19 Pandemic, Part 1: Can Antimicrobial Copper-Based Alloys Help Suppress Infectious Transmission of Viruses Originating from Human Contact with High-Touch Surfaces? Corrosion 2020, 76, 523–527. [Google Scholar] [CrossRef]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Hewawaduge, C.; Senevirathne, A.; Jawalagatti, V.; Kim, J.W.; Lee, J.H. Copper-Impregnated Three-Layer Mask Efficiently Inactivates SARS-CoV2. Environ. Res. 2021, 196, 110947. [Google Scholar] [CrossRef]
- Soar, J.; Böttiger, B.W.; Carli, P.; Couper, K.; Deakin, C.D.; Djärv, T.; Lott, C.; Olasveengen, T.; Paal, P.; Pellis, T.; et al. European Resuscitation Council Guidelines 2021: Adult Advanced Life Support. Resuscitation 2021, 161, 115–151. [Google Scholar] [CrossRef]
- Adelborg, K.; Dalgas, C.; Grove, E.L.; Jørgensen, C.; Al-Mashhadi, R.H.; Løfgren, B. Mouth-to-Mouth Ventilation Is Superior to Mouth-to-Pocket Mask and Bag-Valve-Mask Ventilation during Lifeguard CPR: A Randomized Study. Resuscitation 2011, 82, 618–622. [Google Scholar] [CrossRef] [PubMed]
- Beesems, S.G.; Wijmans, L.; Tijssen, J.G.P.; Koster, R.W. Duration of Ventilations during Cardiopulmonary Resuscitation by Lay Rescuers and First Responders: Relationship between Delivering Chest Compressions and Outcomes. Circulation 2013, 127, 1585–1590. [Google Scholar] [CrossRef] [PubMed]
- Carballo-Fazanes, A.; Barcala-Furelos, R.; Eiroa-Bermúdez, J.; Fernández-Méndez, M.; Abelairas-Gómez, C.; Martínez-Isasi, S.; Murciano, M.; Fernández-Méndez, F.; Rodríguez-Núñez, A. Physiological Demands of Quality Cardiopulmonary Resuscitation Performed at Simulated 3250 Meters High. Am. J. Emerg. Med. 2020, 38, 2580–2585. [Google Scholar] [CrossRef] [PubMed]
- Simmons, M.; Deao, D.; Moon, L.; Peters, K.; Cavanaugh, S. Bench Evaluation: Three Face-Shield CPR Barrier Devices. Respir. Care 1995, 40, 618–623. [Google Scholar]



{kind=link}
{kind=link}
| Valid Attempts for Rescue Breath | Visible Chest Rise n (%) 1 | Mean of Attempts Per Subject 2 (n = 104) | Comparison | p 3 |
|---|---|---|---|---|
| ADULT BLS (n = 981) | 951 (96.9%) | 96.9% | Resusci Anne vs. ADULT BLS | <0.001 |
| Resusci Anne (n = 906) | 822 (90.7%) | 90.8% | Resusci Anne vs. Resusci Baby | <0.001 |
| Resusci Baby (n = 1857) | 1777 (95.7%) | 95.8% | ADULT BLS vs. Resusci Baby | 0.106 |
| ADULT (Resusci Anne) | INFANT (Resusci Baby) | |||
|---|---|---|---|---|
| Attempts (%) 1 (n = 906) | Mean of Attempts Per Student 2 (n = 104) | Attempts (%) 1 (n = 1 857) | Mean of Attempts Per Student 2 (n = 104) | |
| No volume | 84 (9.3%) | 9.2% | 80 (4.3%) | 4.2% |
| Low volume | 262 (28.9%) | 31.6% | 295 (15.9%) | 16.7% |
| Optimal volume | 299 (33.0%) | 32.5% | 817 (44.0%) | 42.1% |
| High volume | 261 (28.8%) | 26.7% | 665 (35.8%) | 36.9% |
| Question | 1 (Easy) | 2 | 3 | 4 | 5 (Impossible) |
|---|---|---|---|---|---|
| I felt mouth-to-mouth ventilation through a respirator was: | 35 (33.7%) | 51 (49%) | 15 (14.4%) | 3 (2.9%) | 0 |
| Mouth-to-mouth ventilation on the mannequin compared to ventilation without a respirator seemed to me: (3 = the same; if you cannot decide, do not mention any possibility) *: | 1 (1.0%) | 5 (5.0%) | 46 (45.5%) | 46 (45.5%) | 3 (3.0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosinová, M.; Štourač, P.; Prokopová, T.; Vafková, T.; Vafek, V.; Barvík, D.; Skříšovská, T.; Dvořáček, J.; Djakow, J.; Klučka, J.; et al. Feasibility of Mouth-to-Mouth Ventilation through FFP2 Respirator in BLS Training during COVID-19 Pandemic (MOVERESP Study): Simulation-Based Study. Children 2022, 9, 1751. https://doi.org/10.3390/children9111751
Kosinová M, Štourač P, Prokopová T, Vafková T, Vafek V, Barvík D, Skříšovská T, Dvořáček J, Djakow J, Klučka J, et al. Feasibility of Mouth-to-Mouth Ventilation through FFP2 Respirator in BLS Training during COVID-19 Pandemic (MOVERESP Study): Simulation-Based Study. Children. 2022; 9(11):1751. https://doi.org/10.3390/children9111751
Chicago/Turabian StyleKosinová, Martina, Petr Štourač, Tereza Prokopová, Tereza Vafková, Václav Vafek, Daniel Barvík, Tamara Skříšovská, Jan Dvořáček, Jana Djakow, Jozef Klučka, and et al. 2022. "Feasibility of Mouth-to-Mouth Ventilation through FFP2 Respirator in BLS Training during COVID-19 Pandemic (MOVERESP Study): Simulation-Based Study" Children 9, no. 11: 1751. https://doi.org/10.3390/children9111751
APA StyleKosinová, M., Štourač, P., Prokopová, T., Vafková, T., Vafek, V., Barvík, D., Skříšovská, T., Dvořáček, J., Djakow, J., Klučka, J., Jarkovský, J., & Plevka, P. (2022). Feasibility of Mouth-to-Mouth Ventilation through FFP2 Respirator in BLS Training during COVID-19 Pandemic (MOVERESP Study): Simulation-Based Study. Children, 9(11), 1751. https://doi.org/10.3390/children9111751