
Adverse Childhood Experiences Are Associated with Reduced Psychological Resilience in Youth: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
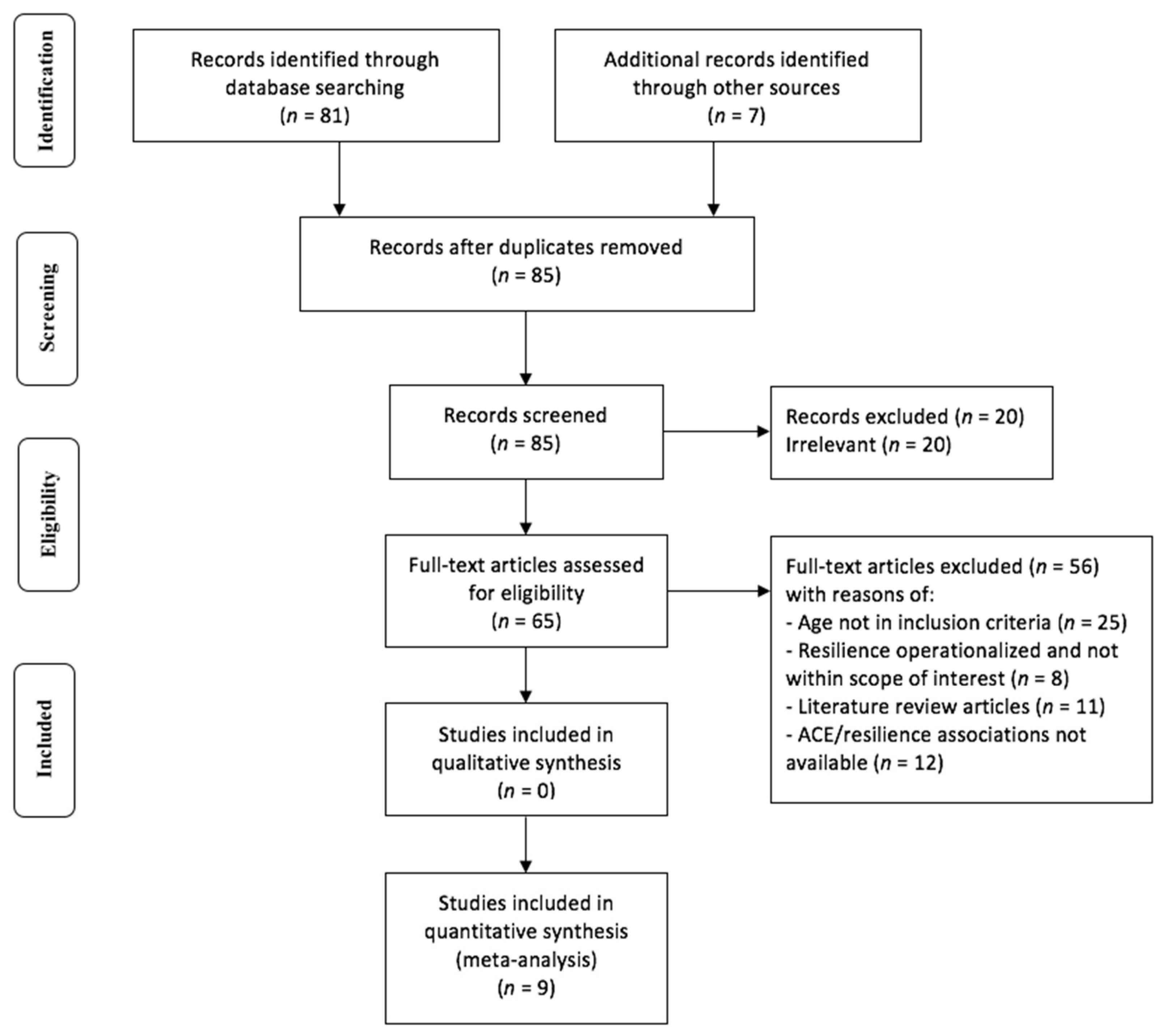
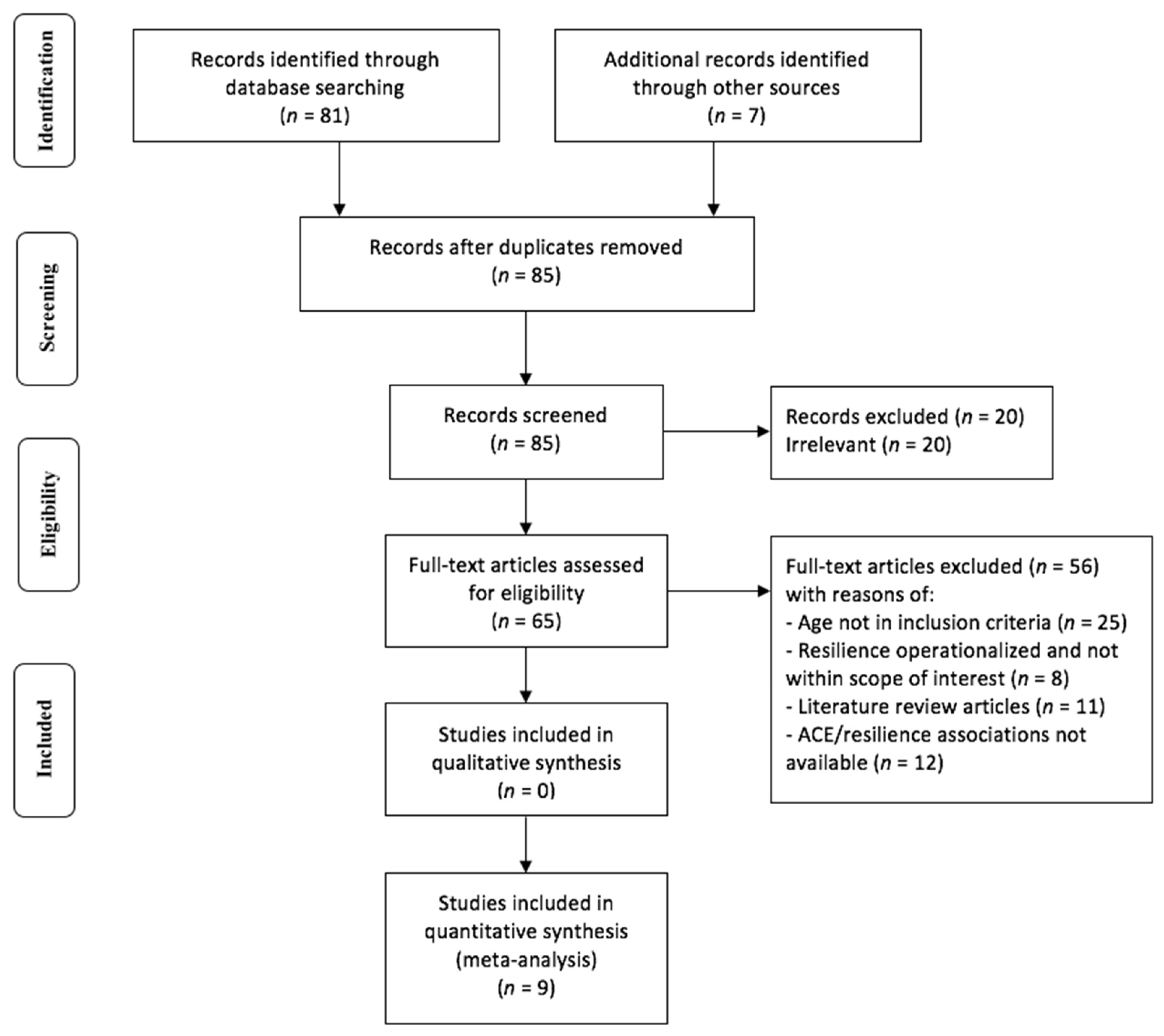
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Analysis
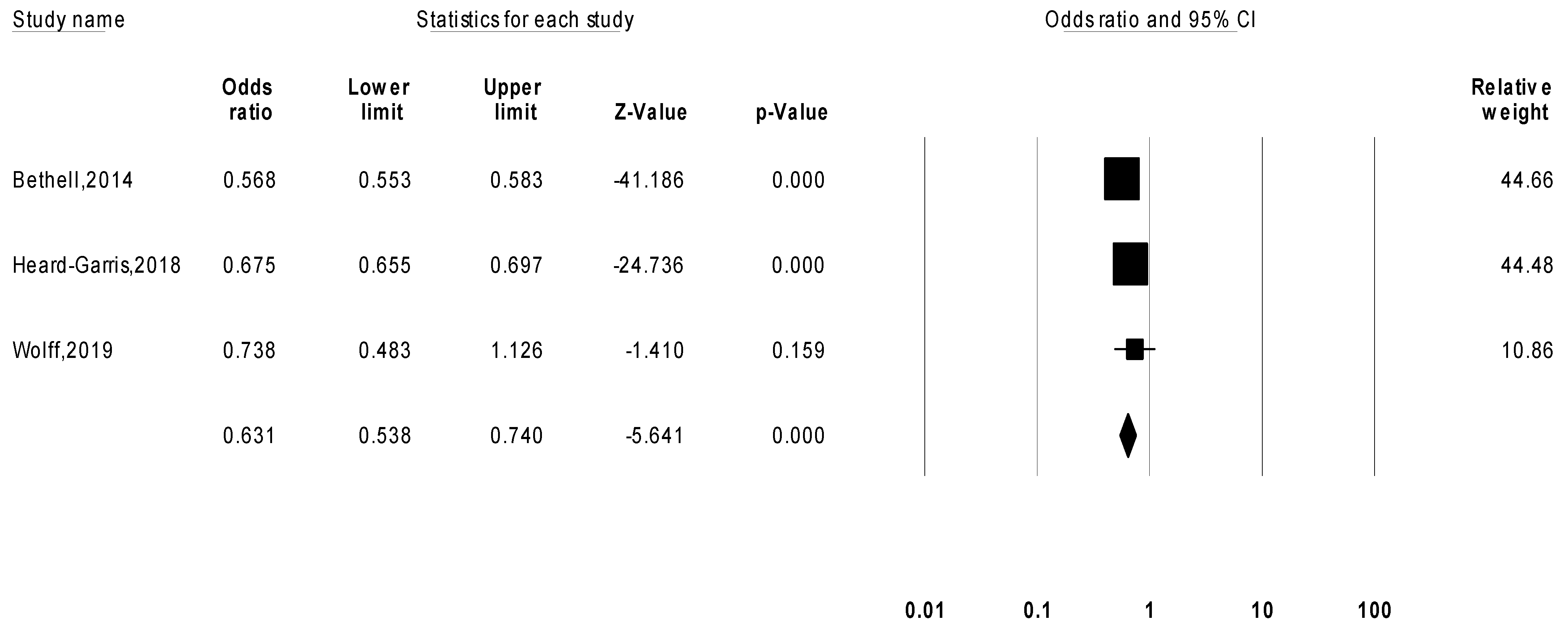
3. Results
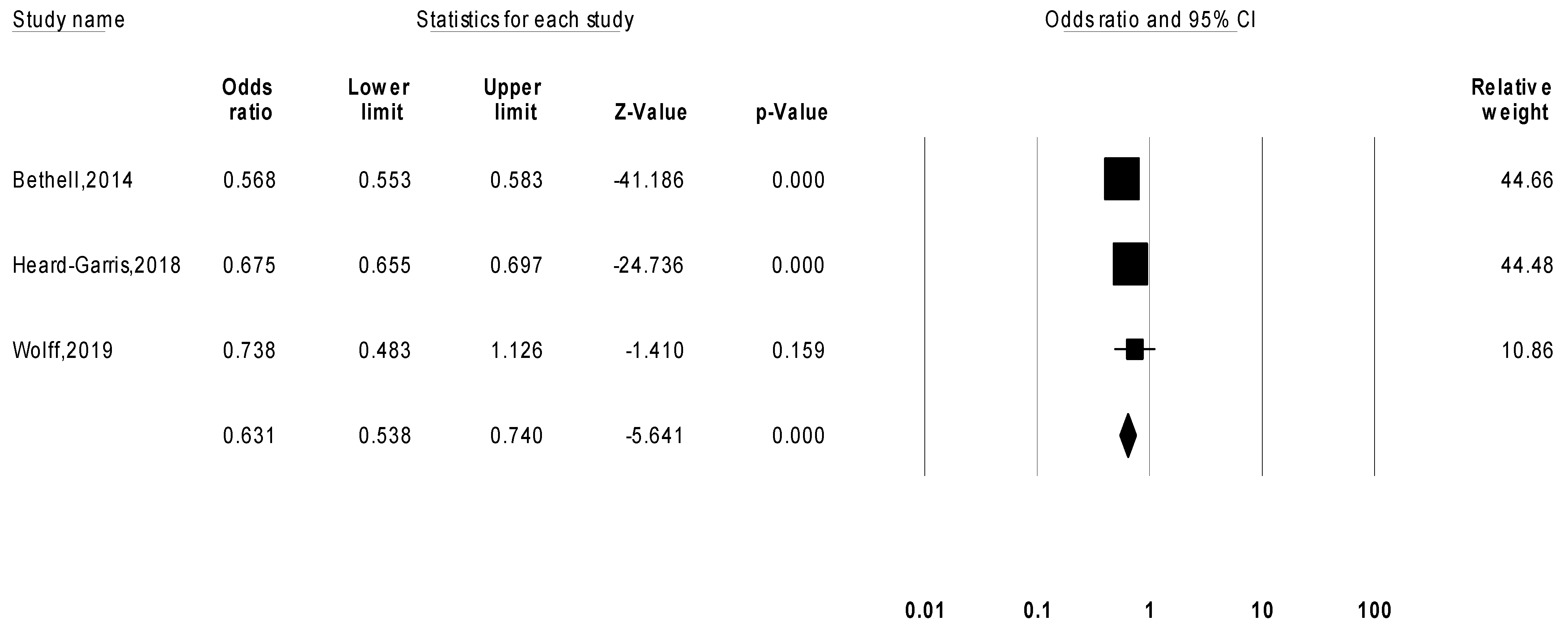
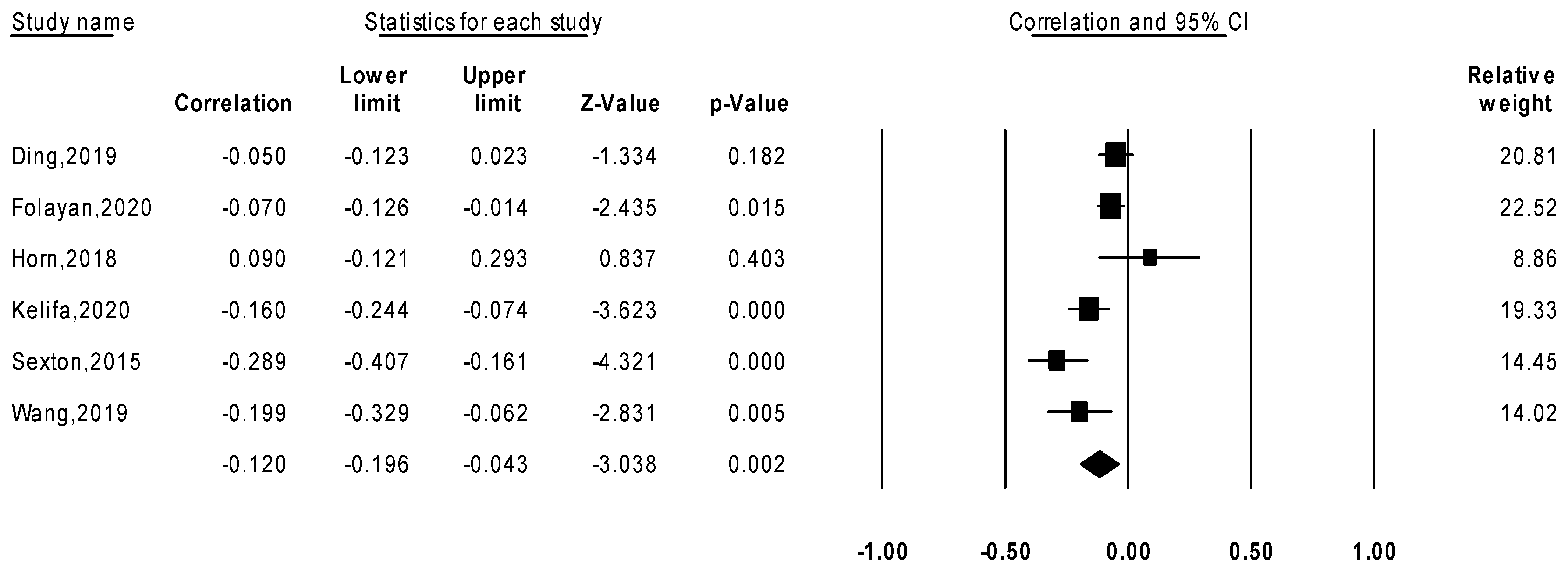
Meta-Analysis Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Committee on Improving the Health Safety and Well-Being of Young Adults; Institute of Medicine; National Research Council. Investing in the Health and Well-Being of Young Adults; National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Kostić, M.; Lazarević, L.; Maravić, V.M.; Vončina, M.M.; Kirćanski, J.R.; Stojković, A.; Videnović, M. Adverse Childhood Experiences (ACE) Study: UNICEF in Serbia. 2019. Available online: https://www.unicef.org/serbia/media/10726/file/Adverse%20Childhood%20Experiences%20(ACE)%20Study.pdf (accessed on 20 October 2021).
- Sacks, V.; Murphey, D. The Prevalence of Adverse Childhood Experiences, Nationally, by State, and by Race/Ethnicity; Child Trends, 2018; Available online: https://www.childtrends.org/wp-content/uploads/2018/02/ACESBriefUpdatedFinal_ChildTrends_February2018.pdf (accessed on 20 October 2021).
- Bethell, C.; Newacheck, P.; Hawes, E.; Halfon, N. Adverse childhood experiences: Assessing the impact on health and school engagement and the mitigating role of resilience. Health Aff. 2014, 33, 2106–2115. [Google Scholar] [CrossRef] [PubMed]
- Ding, C.; Wang, T.; Chen, X.; Li, J.; Wang, W.; Huang, D.; Yan, H.; Li, S. Association of adverse childhood experience and attention deficit hyperactivity disorder with depressive symptoms among men who have sex with men in China: Moderated mediation effect of resilience. BMC Public Health 2019, 19, 1706. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-C.; Guerola, M.M.; Lin, Y.-C.; Hsieh, Y.-P.; Strong, C.; Tsai, M.-C.; Lin, C.-Y. Effects of childhood adversity and resilience on Taiwanese youth health behaviors. Pediatrics Neonatol. 2019, 60, 368–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrucceli, K.; Davis, J.; Berman, T. Adverse childhood experiences and associated health outcomes: A systematic review and meta-analysis. Child Abus. Negl. 2019, 97, 104–127. [Google Scholar] [CrossRef]
- Richter, A.; Kramer, B.; Diekhof, E.; Gruber, O. Resilience to adversity is associated with increased activity and connectivity in the VTA and hippocampus. NeuroImage Clin. 2019, 23, 101920. [Google Scholar] [CrossRef] [PubMed]
- Schilling, E.; Aseltine, R.; Gore, S. Adverse childhood experiences and mental health in young adults: A longitudinal survey. BMC Public Health 2007, 7, 30. [Google Scholar] [CrossRef] [Green Version]
- Hochberg, Z.; Konner, M. Emerging adulthood a pre-adult life-history stage. Front. Endocrinol. 2020, 10, 918. [Google Scholar] [CrossRef]
- Arnett, J.J. Emerging adulthood. Am. Psychol. Assoc. 2000, 55, 469–480. [Google Scholar] [CrossRef]
- United Nations Office on Drugs and Crime. World Drug Report. Available online: https://www.unodc.org/doc/wdr2018/WDR_2018_Press_ReleaseENG.PDF (accessed on 20 October 2020).
- Park, E.; Lee, J.; Han, J. The association between adverse childhood experiences and young adult outcomes: A scoping study. Child. Youth Serv. Rev. 2021, 123, 105916. [Google Scholar] [CrossRef]
- Windle, M.; Haardörfer, R.; Getachew, B.; Shah, J.; Payne, J.; Pillai, D.; Berg, C.J. A multivariate analysis of adverse childhood experiences and health behaviors and outcomes among college students. J. Am. Coll. Health 2018, 66, 246–251. [Google Scholar] [CrossRef]
- Kremen, A.; Block, J. IQ and ego-resiliency: Conceptual and empirical conncetions and separateness. J. Personal. Soc. Psychol. 1996, 70, 349–361. [Google Scholar]
- Hu, T.; Zhang, D.; Wang, J. A meta-analysis of the trait resilience and mental health. Personal. Individ. Differ. 2014, 76, 18–27. [Google Scholar] [CrossRef]
- Kuldas, S.; Foody, M. Neither resiliency-trait nor resilience-state: Transactional Resiliency/e. Youth Soc. 2021. [Google Scholar] [CrossRef]
- Maul, S.; Giegling, I.; Fabbri, C. Genetics of resilience: Implications from genome-wide association studies and candidate genes of the stress response system in posttraumatic stress disorder and depression. Am. J. Med. Genet. 2020, 183, 77–94. [Google Scholar] [CrossRef] [PubMed]
- Young-Wolff, K.C.; Alabaster, A.; McCaw, B.; Stoller, N.; Watson, C.; Sterling, S.; Ridout, K.K.; Flanagan, T. Adverse childhood experiences and mental and behavioral health conditions during pregnancy: The role of resilience. J. Womens Health 2019, 28, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Heard-Garris, N.; Davis, M.M.; Szilagyi, M.; Kan, K. Childhood adversity and parent perceptions of child resilience. BMC Pediatry 2018, 18, 204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleming, J.; Ledogar, R. Resilience, an evolving concept: A review of literature relevant to aboriginal research. Can. Inst. Health Res. 2008, 6, 7–23. [Google Scholar]
- Ong, A.D.; Bergeman, C.; Boker, S. Resilience comes of age: Defining features in later adulthood. J. Personal. 2009, 77, 1777–1804. [Google Scholar] [CrossRef] [Green Version]
- Folayan, M.O.; Oginni, O.; Arowolo, O.; Tantawi, M.E. Internal consistency and correlation of the adverse childhood experiences, bully victimization, self-esteem, resilience, and social support scales in Nigerian children. BMC Res. Notes 2020, 13, 331. [Google Scholar] [CrossRef]
- Kelifa, M.O.; Yang, Y.; Carly, H.; Bo, W.; Wang, P. How adverse childhood experiences relate to subjective wellbeing in college students: The role of resilience and depression. J. Happiness Stud. 2021, 22, 2103–2123. [Google Scholar] [CrossRef]
- Sexton, M.B.; Hamilton, L.; McGinnis, E.; Rosenblum, K.; Musik, M. The roles of resilience and childhood trauma history: Main and moderating effects on postpartum maternal mental health and functioning. J. Affect. Disord. 2015, 174, 562–568. [Google Scholar] [CrossRef] [Green Version]
- Horn, S.; Roos, L.; Beauchamp, K.; Flannery, J.; Fisher, P. Polyvictimization and externalizing symptoms in foster care children: The moderating role of executive function. J. Trauma Dissociation 2018, 19, 307–324. [Google Scholar] [CrossRef]
- Feder, A.; Nestler, E.; Charney, D. Psychobiology and molecular genetics of resilience. Nat. Rev. Neurosci. 2009, 10, 446–457. [Google Scholar] [CrossRef] [Green Version]
- Niitsu, K.; Rice, M.; Houfek, J.; Stoltenberg, S.; Kupzyk, K.; Barron, C. A systematic review of genetic influence on psychological resilience. Biol. Res. Nurs. 2019, 21, 61–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, E.J.; Miller, M.; Sullivan, D.R.; Amstadter, A.B.; Mitchell, K.S.; Goldberg, J.; Magruder, K.M. A classical twin study of PTSD symptoms and resilience: Evidence for a single spectrum of vulnerability to traumatic stress. Depress. Anxiety 2018, 35, 132–139. [Google Scholar] [CrossRef] [Green Version]
- Kunzler, A.; Chmitorz, A.; Bagusat, C.; Kaluza, A.J.; Hoffmann, I.; Schäfer, M.; Quiring, O.; Rigotti, T.; Kalisch, R.; Tüscher, O.; et al. Construct validitiy and population-based norms of the German brief resilience scale (BRS). Eur. J. Health Psychol. 2018, 25, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Herrenkohl, T. Person–environment interactions and the shaping of resilience. Trauma Violence Abus. 2013, 14, 191–194. [Google Scholar] [CrossRef] [Green Version]
- Hofgaard, L.S.; Nes, R.B.; Roysamb, E. Introducing two types of psychological resilience with partly unique genetic and environmental sources. Sci. Rep. 2021, 11, 8624. [Google Scholar] [CrossRef] [PubMed]
- Masten, A.S. Resilience from a developmental systems perspective. World Psychiatry 2019, 18, 101–102. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Li, Y.; Tollefsbol, T. Gene-environment interactions and epigenetic basis of human diseases. Curr. Issues Mol. Biol. 2008, 10, 25–36. [Google Scholar]
- Zheng, M.; Jin, H.; Shi, N.; Duan, C.; Wang, D.; Yu, X.; Li, X. The relationship between health literacy and quality of life: A systematic review and meta-analysis. Health Qual. Life Outcomes 2018, 16, 201. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Study | Population | Sample Size | Age | Name of ACE Measure | ACEs Measured | Resilience Scale | Association with Resilience | Covariates Examined |
|---|---|---|---|---|---|---|---|---|
| Heard-Garris et al. (2018) | National Survey of Children’s Health; United States population | 62,200 | 0–17 | NSCH-ACEs 1 | 9 | Parent-perceived resilience scale | Negative | Eating meals together * |
| Religious attendance * | ||||||||
| Sharing ideas with children * | ||||||||
| Neighborhood amenities and mentorship * | ||||||||
| Wolff et al. (2019) | Pregnant women (~14–23 weeks of gestation); United States population | 355 | 22–38 | BRFSMQ 2 | 8 | CD-RISC 10 7 | Negative | None |
| Bethell et al. (2014) | National Survey of Children’s Health; United States population | 95,677 | 0–17 | NSCH-ACEs | 9 | “Staying calm and in control when faced with a challenge” | Negative | Protective home environment |
| Healthy parents | ||||||||
| Supportive community | ||||||||
| Ding et al. (2019) | Gay/bisexual men; Chinese population | 714 | 19–35 | Kaiser-CDC study | 10 | CD-RISC10 | Negative | None |
| Folayan et al. (2020) | Nigerian population | 1209 | 11–16 | ACE questionnaire 3 | 10 | CD-RISC10 | Negative | Social support |
| Kelifa et al. (2020) | Eritrean college students | 507 | 18–25 | ACE-IQ 4 | 13 | CD-RISC10 | Negative | None |
| Sexton et al. (2015) | 4-months post-partum mothers | 214 | 23–33 | CTQ 5 | 28 | CD-RISC10 | Negative | None |
| Horn et al. (2018) | 88 foster-care and community children | 88 | 3–4 | MCS 6 | 5 | NEPSY 8 | Positive | None |
| Wang et al. (2019) | Taiwanese youth population | 200 | 15–22 | ACE-IQ | 14 | Inventory of Adolescent Resilience (Chinese version) | Negative | Household financial status |
| Parental education | ||||||||
| Family support * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morgan, C.A.; Chang, Y.-H.; Choy, O.; Tsai, M.-C.; Hsieh, S. Adverse Childhood Experiences Are Associated with Reduced Psychological Resilience in Youth: A Systematic Review and Meta-Analysis. Children 2022, 9, 27. https://doi.org/10.3390/children9010027
Morgan CA, Chang Y-H, Choy O, Tsai M-C, Hsieh S. Adverse Childhood Experiences Are Associated with Reduced Psychological Resilience in Youth: A Systematic Review and Meta-Analysis. Children. 2022; 9(1):27. https://doi.org/10.3390/children9010027
Chicago/Turabian StyleMorgan, Cyleen A., Yun-Hsuan Chang, Olivia Choy, Meng-Che Tsai, and Shulan Hsieh. 2022. "Adverse Childhood Experiences Are Associated with Reduced Psychological Resilience in Youth: A Systematic Review and Meta-Analysis" Children 9, no. 1: 27. https://doi.org/10.3390/children9010027
APA StyleMorgan, C. A., Chang, Y.-H., Choy, O., Tsai, M.-C., & Hsieh, S. (2022). Adverse Childhood Experiences Are Associated with Reduced Psychological Resilience in Youth: A Systematic Review and Meta-Analysis. Children, 9(1), 27. https://doi.org/10.3390/children9010027