
Is a Parry Fracture—An Isolated Fracture of the Ulnar Shaft—Associated with the Probability of Abuse in Children between 2 and 16 Years Old?


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.1.1. Radiographs
2.1.2. Patients
2.2. Data Analysis
2.2.1. Radiographic Classification
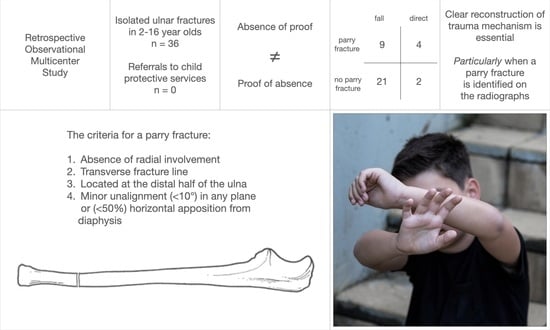
- the absence of radial involvement;
- a transverse fracture line (≤45°);
- a location below the midshaft (<0.5 adjusted distance to the lesion’s center); and
- either minor unalignment (≤10°) in any plane or horizontal apposition from the diaphysis (<50%).
2.2.2. Chart Assessment
2.3. Statistical Analysis
3. Results
3.1. Data Collection
3.2. Data Analysis
3.3. Statistical Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Judd, M.A. The parry problem. J. Arch. Sci. 2008, 35, 1658–1666. [Google Scholar] [CrossRef]
- Geldenhuys, E.M.; Burger, E.H.; Alblas, A.; Greyling, L.M.; Kotzé, S.H. The association between healed skeletal fractures indicative of interpersonal violence and alcoholic liver disease in a cadaver cohort from the Western Cape, South Africa. Alcohol 2016, 52, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Pierce, M.C.; Kaczor, K.; Lohr, D.; Richter, K.; Starling, S.P. A practical guide to differentiating abusive from accidental fractures: An injury plausibility approach. Clin. Pediatric Emerg. Med. 2012, 13, 166–177. [Google Scholar] [CrossRef]
- Jenny, C.; Hymel, K.P.; Ritzen, A.; Reinert, S.E.; Hay, T.C. Analysis of missed cases of abusive head trauma. J. Am. Med. Assoc. 1999, 281, 621–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenfeld, E.H.; Johnson, B.; Wesson, D.E.; Shah, S.R.; Vogel, A.M.; Naik-Mathuria, B. Understanding non-accidental trauma in the United States: A national trauma databank study. J. Pediatr. Surg. 2020, 55, 693–697. [Google Scholar] [CrossRef]
- Bilo, R.A.C.; Robben, S.G.F.; van Rijn, R.R. Forensic Aspects of Pediatric Fractures: Differentiating Accidental Trauma from Child Abuse, 1st ed.; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Kemp, A.M.; Dunstan, F.; Harrison, S.; Morris, S.; Mann, M.; Rolfe, K.; Datta, S.; Thomas, D.P.; Sibert, J.R.; Maguire, S. Patterns of skeletal fractures in child abuse: Systematic review. BMJ 2008, 337, a1518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandya, N.K.; Baldwin, K.; Wolfgruber, H.; Christian, C.W.; Drummond, D.S.; Hosalkar, H.S. Child abuse and orthopaedic injury patterns: Analysis at a level I pediatric trauma center. J. Pediatr. Orthop. 2009, 29, 618–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryznar, E.; Rosado, N.; Flaherty, E.G. Understanding forearm fractures in young children: Abuse or not abuse? Child Abus. Negl. 2015, 47, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Slongo, T.; Audigé, L. AO Pediatric Comprehensive Classification of Long-Bone Fractures (PCCF); AO Foundation: Davos, Switzerland, 2010. [Google Scholar]
- Cohen, J. Weighted Kappa: Nominal scale agreement with provision for scaled disagreement or partial credit. Psychol. Bull. 1968, 70, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar]
- Flaherty, E.G.; Perez-Rossello, J.M.; Levine, M.A.; Hennrikus, W.L. Evaluating children with fractures for child physical abuse. Pediatrics 2014, 133, e477–e489. [Google Scholar] [CrossRef] [Green Version]
- Castagnino, M.; Paglino, A.; Berardi, C.; Riccioni, S.; Esposito, S. Recording risk factors of physical abuse in children younger than 36 months with bone fractures: A 12-years retrospective study in an Italian general hospital emergency room. Front. Pediatr. 2020, 8, 183. [Google Scholar] [CrossRef]
- Mortensson, W.; Thönel, S. Left-side dominance of upper extremity fracture in children. Acta Orthop. Scand. 1991, 62, 154–155. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Determinant | n (%) | mean ± SD (Range) |
|---|---|---|
| Age (years) | 8.9 ± 3.8 (2.3–15.4) | |
| Sex (male) | 23 (64%) | |
| Side (right) | 15 (42%) | |
| Previous fracture (yes) | 3 (8%) | |
| Delay (yes) | 8 (22%) | 9.3 ± 3.9 (1–14) * |
| Fall from | n | Fall during | n |
| bicycle | 1 | cartwheeling | 1 |
| bouncy castle | 2 | dancing | 1 |
| chair | 1 | field hockey | 1 |
| climbing frame | 3 | gymnastics | 2 |
| couch | 1 | handball | 1 |
| gymnastic vault | 2 | playing with old rubber tire | 1 |
| hoverboard | 1 | playing in the mud | 1 |
| pony | 1 | soccer | 1 |
| sandbox | 1 | ||
| sidewalk | 1 | Direct Trauma | n |
| slide | 2 | kicked by other kid | 2 |
| small pole | 1 | kicked by pony | 1 |
| standing | 1 | other kid fell on arm | 1 |
| swing | 1 | other kid stepped on arm | 2 |
| Classification | Contributing Assessments (%) | ||
|---|---|---|---|
| AO Pediatric | n | yes | no |
| Bowing (1.1) | |||
| Greenstick (2.1) | 9 | 69 | 31 |
| Complete transverse 1 (4.1) | 10 | 75 | 25 |
| Complete transverse 2 (4.2) | |||
| Complete oblique or spiral 1 (5.1) | 15 | 68 | 32 |
| Complete oblique or spiral 2 (5.2) | 2 | 75 | 25 |
| Paleopathology | |||
| Parry fracture | 14 | 77 | 23 |
| No parry fracture | 22 | 89 | 11 |
| Exp(B) [95% C.I.] | p-Value | |
|---|---|---|
| Age | 1.289 [0.980–1.695] | 0.069 |
| Sex | 1.158 [0.182–7.384] | 0.877 |
| Side | 0.229 [0.240–2.198] | 0.201 |
| Previous fracture | 2.800 [0.212–37.03] | 0.434 |
| Delay | 1.029 [0.846–1.251] | 0.778 |
| AO Pediatric | 1.055 [0.554–2.011] | 0.870 |
| Paleopathology | 4.667 [0.720–30.23] | 0.106 |
| Fall (n = 30) | Direct (n = 6) | p-Value | |
|---|---|---|---|
| Age | 8.41 ± 3.78 | 11.71 ± 3.10 | 0.053 |
| Sex | 0.63 ± 0.49 | 0.67 ± 0.52 | 0.881 |
| Side | 0.47 ± 0.51 | 0.17 ± 0.41 | 0.183 |
| Previous fracture | 0.07 ± 0.25 | 0.17 ± 0.41 | 0.433 |
| Delay | 1.97 ± 4.06 | 2.50 ± 5.65 | 0.784 |
| AO Pediatric | 3.73 ± 1.34 | 3.83 ± 1.72 | 0.874 |
| Paleopathology | 0.30 ± 0.47 | 0.67 ± 0.52 | 0.093 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hermans, K.; Fransz, D.; Walbeehm-Hol, L.; Hustinx, P.; Staal, H. Is a Parry Fracture—An Isolated Fracture of the Ulnar Shaft—Associated with the Probability of Abuse in Children between 2 and 16 Years Old? Children 2021, 8, 650. https://doi.org/10.3390/children8080650
Hermans K, Fransz D, Walbeehm-Hol L, Hustinx P, Staal H. Is a Parry Fracture—An Isolated Fracture of the Ulnar Shaft—Associated with the Probability of Abuse in Children between 2 and 16 Years Old? Children. 2021; 8(8):650. https://doi.org/10.3390/children8080650
Chicago/Turabian StyleHermans, Kyra, Duncan Fransz, Lisette Walbeehm-Hol, Paul Hustinx, and Heleen Staal. 2021. "Is a Parry Fracture—An Isolated Fracture of the Ulnar Shaft—Associated with the Probability of Abuse in Children between 2 and 16 Years Old?" Children 8, no. 8: 650. https://doi.org/10.3390/children8080650