
Cluster Randomized Trial: Sun Protection Intervention ‘Clever in Sun and Shade for Preschools’—Effectiveness and Dissemination

Abstract
:1. Introduction
2. Methods
2.1. Trial Design
2.2. Participants
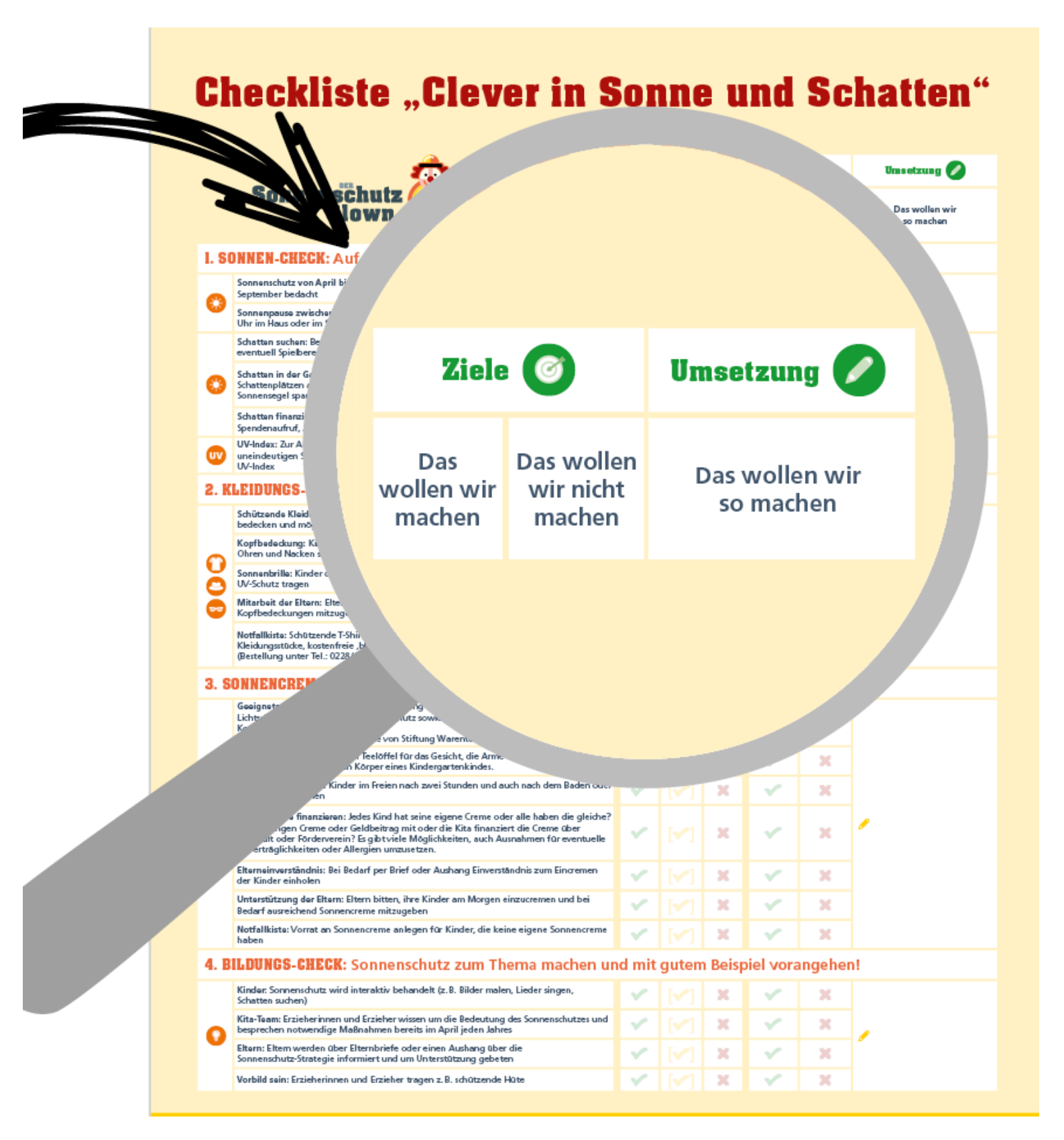
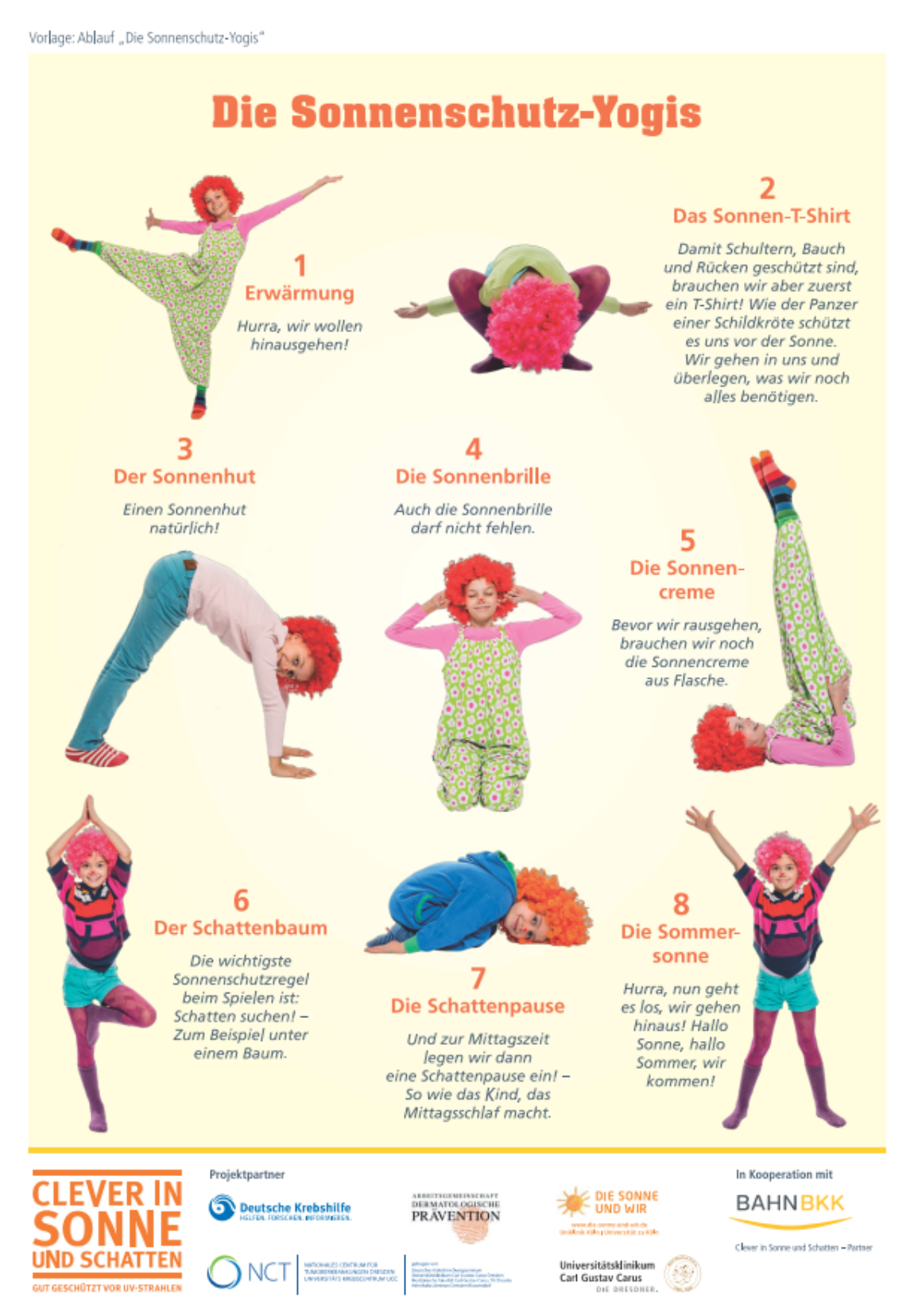
2.3. Interventions
2.4. Measures

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scale | Reliability 1 | Item | Reference |
|---|---|---|---|
| Sunscreen Use 2 | 0.63 | I put sunscreen on my students when we go outside. | [61] |
| I take sunscreen along when we go on field trips. | [61] | ||
| I use sunscreen with an UV-protection factor of 30+ for my students. | [61] | ||
| I reapply sunscreen on my students every 2 h when we are outside between 11 a.m. and 3 p.m. | [61] | ||
| I put sunscreen on myself when I go outside with my students. | (role model) | ||
| Sun-Avoidance 2 | 0.34 | My students wear hats or caps when they go outside. | [61] |
| My students wear tank tops or halter tops when they go outside. 5 | [61] | ||
| My students wear long shorts or skirts when they go outside. | [61] | ||
| I take sun shade sails or parasols outside and on field trips so that I can set up shaded areas. | [61] | ||
| When I go outside with my students, I keep to shaded areas myself and wear protective clothing. | (role model) | ||
| Psychosocial Outcomes | |||
| Sunscreen Use Self-Efficacy 3 | 0.62 | I am confident of being able | |
| … to properly apply sunscreen on my students. | [61] (task) | ||
| … to ensure that my students’ parents support me in the provision or use of sunscreen. | (task) | ||
| … to take sunscreen with me on any occasion when my students may be outside. | [61] (maintenance) | ||
| … to get more sunscreen for my students whenever necessary. | [61] (maintenance) | ||
| Sun-Avoidance Self-Efficacy 3 | 0.58 | I am confident of being able | |
| … to ensure that my students’ parents provide them with protective clothing. | (task) | ||
| … to decide if an area is sufficiently shaded to protect my students from the sun. | [61] (task) | ||
| … to check that my students are wearing protective clothes before they go outside. | [61] (maintenance) | ||
| … to provide spare clothes in case the students‘ parents have forgotten suitable clothes. | (maintenance) | ||
| Health-Related Outcome Expectancies 3 | 0.74 | Avoiding overexposure to the sun protects from premature skin-aging. | [65] |
| Avoiding overexposure to the sun decreases the risk for skin cancer. | [65] | ||
| Appearance-Related Outcome Expectancies 3 | 0.58 | Tanning makes me look better. 5 | [37] |
| Tanned skin is healthy skin. 5 | [37] | ||
| Impediments to Sunscreen Use 3 | 0.78 | Putting on sunscreen on my students takes too much time. | [61] |
| Putting on sunscreen on my students is always messy. | [61] | ||
| Impediments to Sun-Avoidance 3 | 0.40 | We do not have enough shade from trees, sun-shade sails, or parasols. | |
| Preventing students from taking off protective clothing outdoors is difficult. | |||
| Necessity of Sun protection 3 | 0.68 | I think it is important to protect oneself from the sun in the following situations … at the beach. … at noon. … on sunny evenings. … on cloudy summer days. … during outdoor sports activities. | [31] |
| Sun protection Policy 4 | 0.76 | Is it recorded in writing in the facility concept or other documents, that parents are requested … to bring hats or protective clothing? … to provide sunscreen or if the preschool supplies sunscreen? … to provide a written permission for the use of sunscreen? | [14] |
2.5. Sample Size
2.6. Randomization
2.7. Statistical Methods
3. Results
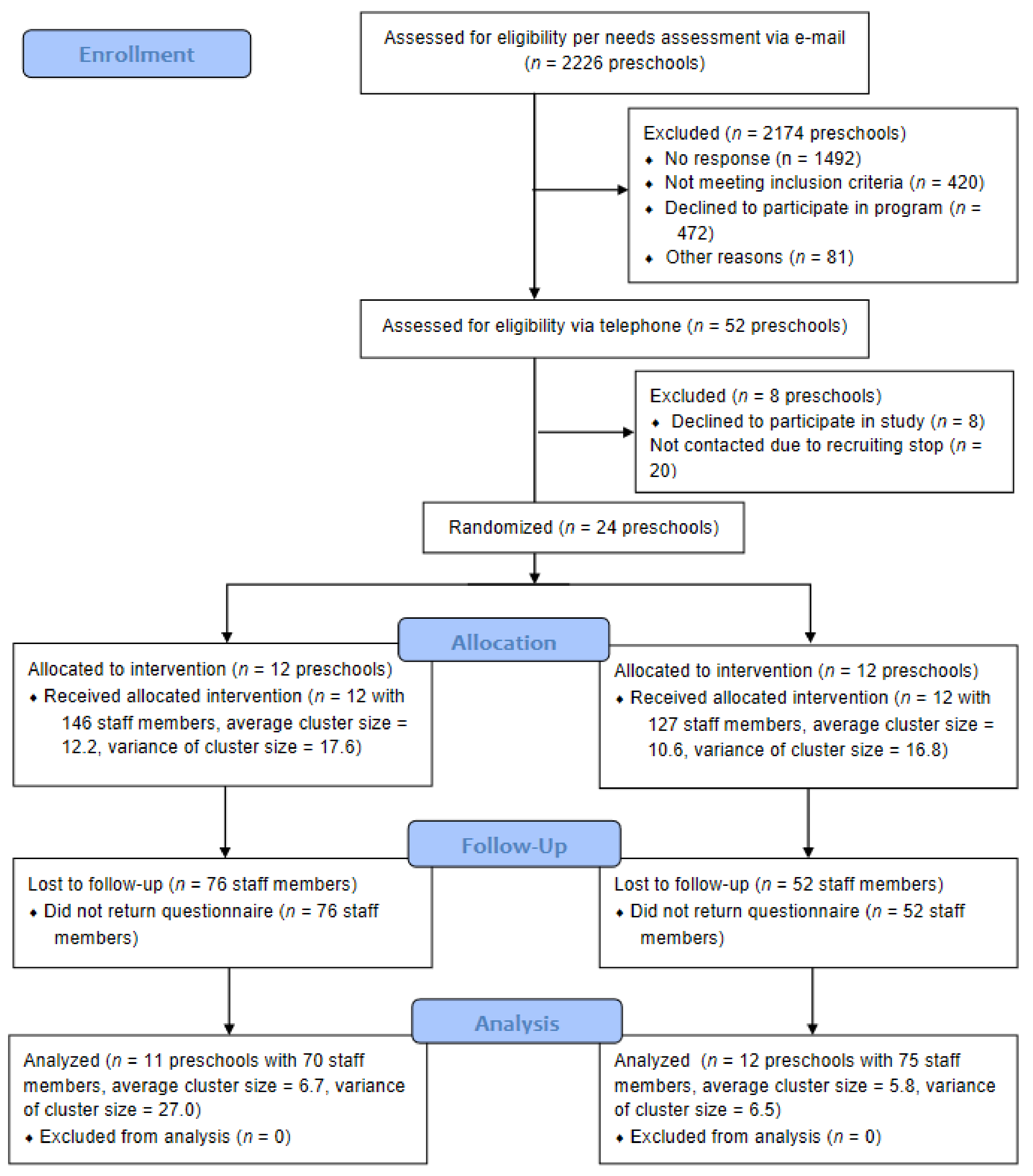
3.1. Participant Flow
3.2. Recruitment
3.3. Baseline Data
3.4. Outcomes
3.4.1. Program Exposure
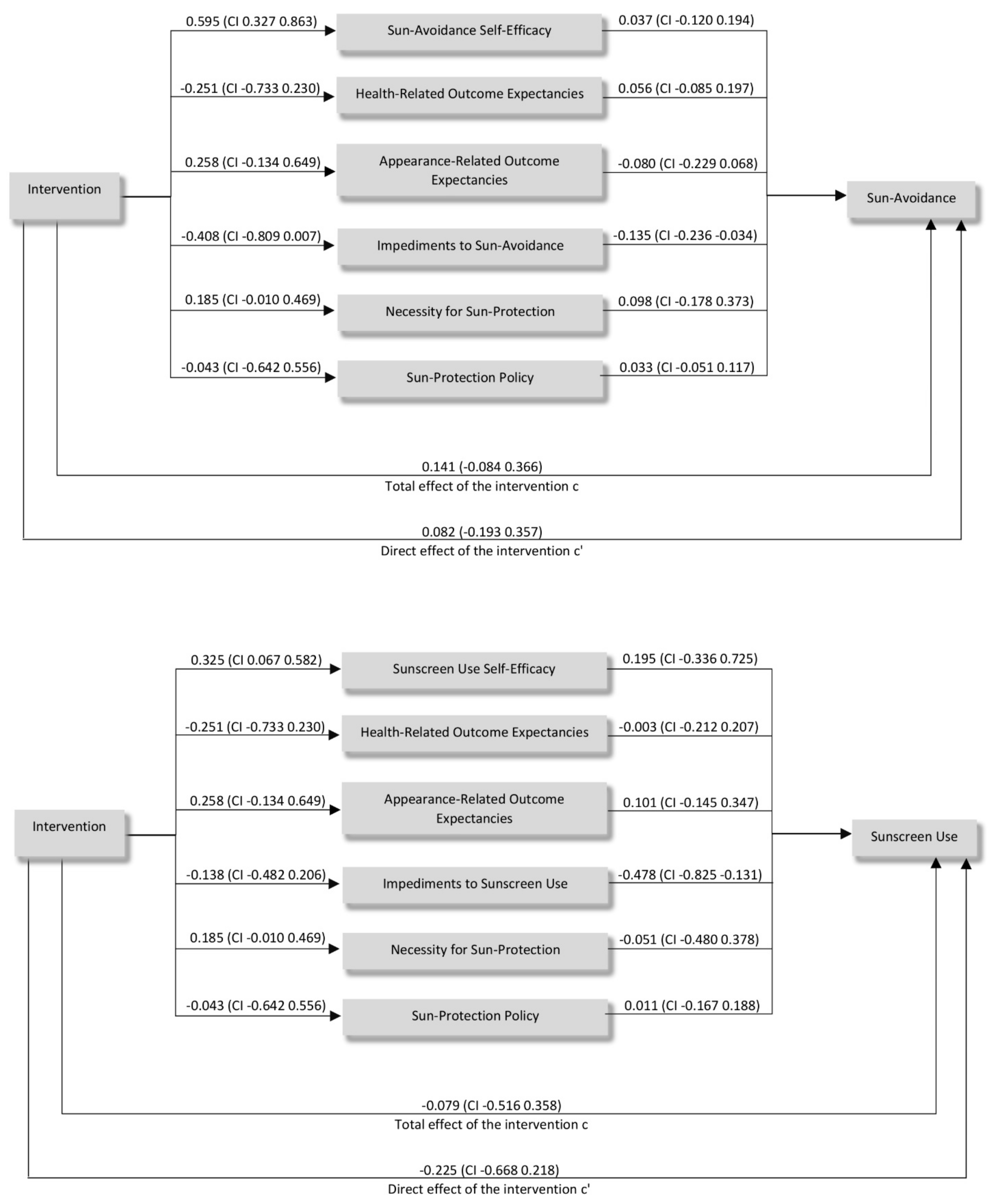
3.4.2. Intervention Effects
3.4.3. Dissemination and Implementation of CLEVER
4. Discussion
4.1. Effectiveness
4.2. Dissemination
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Apalla, Z.; Nashan, D.; Weller, R.B.; Castellsagué, X. Skin Cancer: Epidemiology, Disease Burden, Pathophysiology, Diagnosis, and Therapeutic Approaches. Dermatol. Ther. 2017, 7, 5–19. [Google Scholar] [CrossRef] [Green Version]
- Greinert, R.; de Vries, E.; Erdmann, F.; Espina, C.; Auvinen, A.; Kesminiene, A.; Schüz, J. European Code against Cancer 4th Edition: Ultraviolet radiation and cancer. Cancer Epidemiol. 2015, 39 (Suppl. 1), S75–S83. [Google Scholar] [CrossRef] [Green Version]
- El Ghissassi, F.; Baan, R.; Straif, K.; Grosse, Y.; Secretan, B.; Bouvard, V.; Benbrahim-Tallaa, L.; Guha, N.; Freeman, C.; Galichet, L.; et al. A review of human carcinogens—part D: Radiation. Lancet Oncol. 2009, 10, 751–752. [Google Scholar] [CrossRef]
- Schmitt, J.; Haufe, E.; Trautmann, F.; Schulze, H.-J.; Elsner, P.; Drexler, H.; Bauer, A.; Letzel, S.; John, S.M.; Fartasch, M.; et al. Occupational UV-Exposure is a Major Risk Factor for Basal Cell Carcinoma: Results of the Population-Based Case-Control Study FB-181. J. Occup. Environ. Med. 2018, 60, 36–43. [Google Scholar] [CrossRef]
- Autier, P.; Doré, J.-F.; for Epimel and Eortc Melanoma Cooperative Group. Influence of sun exposures during childhood and during adulthood on melanoma risk. Int. J. Cancer 1998, 77, 533–537. [Google Scholar] [CrossRef]
- Volkmer, B.; Greinert, R. UV and children’s skin. Prog. Biophys. Mol. Biol. 2011, 107, 386–388. [Google Scholar] [CrossRef] [PubMed]
- Green, A.C.; Wallingford, S.C.; McBride, P. Childhood exposure to ultraviolet radiation and harmful skin effects: Epidemiological evidence. Prog. Biophys. Mol. Biol. 2011, 107, 349–355. [Google Scholar] [CrossRef] [Green Version]
- Oliveria, S.A.; Saraiya, M.; Geller, A.C.; Heneghan, M.K.; Jorgensen, C. Sun exposure and risk of melanoma. Arch. Dis. Child. 2006, 91, 131–138. [Google Scholar] [CrossRef] [Green Version]
- Gandini, S.; Sera, F.; Cattaruzza, M.S.; Pasquini, P.; Picconi, O.; Boyle, P.; Melchi, C.F. Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure. Eur. J. Cancer 2005, 41, 45–60. [Google Scholar] [CrossRef] [PubMed]
- Greinert, R.; Volkmer, B.; Wende, A.; Voss, S.; Breitbart, E.W. Prävention von Hautkrebs: Notwendigkeit, Durchführung und Erfolg. Hautarzt 2003, 54, 1152–1163. [Google Scholar] [CrossRef] [PubMed]
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF). S3-Leitlinie Prävention von Hautkrebs AWMF Registernummer: 032/052OL. Available online: https://www.leitlinienprogramm-onkologie.de/leitlinien/hautkrebs-praevention/ (accessed on 11 June 2021).
- Green, A.C.; Williams, G.M.; Logan, V.; Strutton, G.M. Reduced melanoma after regular sunscreen use: Randomized trial follow-up. J. Clin. Oncol. 2011, 29, 257–263. [Google Scholar] [CrossRef] [Green Version]
- Buller, D.B.; Borland, R. Skin cancer prevention for children: A critical review. Health Educ. Behav. 1999, 26, 317–343. [Google Scholar] [CrossRef] [PubMed]
- Crane, L.A.; Schneider, L.S.; Yohn, J.J.; Morelli, J.G.; Plomer, K.D. Block the Sun, Not the Fun: Evaluation of a Skin Cancer Prevention Program for Child Care Centers. Am. J. Prev. Med. 1999, 17, 31–37. [Google Scholar] [CrossRef]
- Buller, D.B.; Taylor, A.M.; Buller, M.K.; Powers, P.J.; Maloy, J.A.; Beach, B.H. Evaluation of the Sunny Days, Healthy Ways sun safety curriculum for children in kindergarten through fifth grade. Pediatr. Dermatol. 2006, 23, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Loescher, L.J.; Buller, M.K.; Buller, D.B.; Emerson, J.; Taylor, A.M. Public education projects in skin cancer. The evolution of skin cancer prevention education for children at a comprehensive cancer center. Cancer 1995, 75, 651–656. [Google Scholar] [CrossRef]
- Baranowski, T.; Bar-Or, O.; Blair, S.; Corbin, C.; Dowda, M.; Freedson, P.; Pate, R.; Plowman, S.; Sallis, J.; Saunders, R.; et al. Guidelines for School and Community Programs to Promote Lifelong Physical Activity Among Young People. Morb. Mortal. Wkly. Rep. 1997, 50, 1–36. [Google Scholar]
- Stöver, L.A.; Hinrichs, B.; Petzold, U.; Kuhlmei, H.; Baumgart, J.; Parpart, C.; Rademacher, O.; Stockfleth, E. Getting in early: Primary skin cancer prevention at 55 German kindergartens. Br. J. Dermatol. 2012, 167 (Suppl. 2), 63–69. [Google Scholar] [CrossRef]
- Gritz, E.R.; Tripp, M.K.; James, A.S.; Carvajal, S.C.; Harrist, R.B.; Mueller, N.H.; Chamberlain, R.M.; Parcel, G.S. An intervention for parents to promote preschool children’s sun protection: Effects of Sun Protection is Fun! Prev. Med. 2005, 41, 357–366. [Google Scholar] [CrossRef]
- Gritz, E.R.; Tripp, M.K.; James, A.S.; Harrist, R.B.; Mueller, N.H.; Chamberlain, R.M.; Parcel, G.S. Effects of a preschool staff intervention on children’s sun protection: Outcomes of sun protection is fun! Health Educ. Behav. 2007, 34, 562–577. [Google Scholar] [CrossRef]
- Swetter, S.M.; Geller, A.C.; Leachman, S.A.; Kirkwood, J.M.; Katalinic, A.; Gershenwald, J.E. Melanoma Prevention and Screening. In Cutaneous Melanoma; Balch, C.M., Atkins, M.B., Garbe, C., Gershenwald, J.E., Halpern, A.C., Kirkwood, J.M., McArthur, G.A., Thompson, J.F., Sober, A.J., Eds.; Springer International Publishing: Basel, Switzerland, 2020; pp. 525–570. ISBN 978-3-030-05068-9. [Google Scholar]
- Seidel, N.; Stoelzel, F.; Garzarolli, M.; Herrmann, S.; Breitbart, E.W.; Berth, H.; Baumann, M.; Ehninger, G. Sun protection training based on a theater play for preschoolers: An effective method for imparting knowledge on sun protection? J. Cancer Educ. 2013, 28, 435–438. [Google Scholar] [CrossRef]
- Turrisi, R.; Hillhouse, J.; Heavin, S.; Robinson, J.; Adams, M.; Berry, J. Examination of the short-term efficacy of a parent-based intervention to prevent skin cancer. J. Behav. Med. 2004, 27, 393–412. [Google Scholar] [CrossRef] [PubMed]
- Abeck, D.; Feucht, J.; Schäfer, T.; Behrendt, H.; Krämer, U.; Ring, J. Parental sun protection management in preschool children. Photodermatol. Photoimmunol. Photomed. 2000, 16, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Seiffge-Krenke, I. Gesundheit als aktiver Gestaltungsprozess im menschlichen Lebenslauf. Entwicklungspsychologie 2008, 6, 822–836. [Google Scholar]
- Klostermann, S.; Bolte, G. Determinants of inadequate parental sun protection behaviour in their children--results of a cross-sectional study in Germany. Int. J. Hyg. Environ. Health 2014, 217, 363–369. [Google Scholar] [CrossRef]
- Duignan, M.; Signal, L.; Thomson, G. Good intentions, but inadequate practices-sun protection in early childhood centres, a qualitative study from New Zealand. N. Z. Med. J. 2014, 127, 40–50. [Google Scholar]
- Giles-Corti, B.; English, D.R.; Costa, C.; Milne, E.; Cross, D.; Johnston, R. Creating SunSmart schools. Health Educ. Res. 2004, 19, 98–109. [Google Scholar] [CrossRef]
- Börner, F.; Greinert, R.; Schütz, H.; Wiedemann, P. UV-Risikowahrnehmung in der Bevölkerung: Ergebnisse einer repräsentativen Umfrage in Deutschland. Gesundheitswesen 2010, 72, e89–e97. [Google Scholar] [CrossRef]
- Eichhorn, C.; Seibold, C.; Loss, J.; Steinmann, A.; Nagel, E. Kenntnisstand zum Thema UV-Strahlung und Sonnenschutz: Befragung von bayerischen Jugendlichen und jungen Erwachsenen. Hautarzt 2008, 59, 821–827. [Google Scholar] [CrossRef]
- Gefeller, O.; Uter, W.; Pfahlberg, A.B. Good, but Not Perfect: Parental Knowledge about Risk Factors for Skin Cancer and the Necessity of Sun Protection in Southern Germany. Pediatr. Dermatol. 2015, 32, e159–e160. [Google Scholar] [CrossRef]
- Keeney, S.; McKenna, H.; Fleming, P.; McIlfatrick, S. Attitudes, knowledge and behaviours with regard to skin cancer: A literature review. Eur. J. Oncol. Nurs. 2009, 13, 29–35. [Google Scholar] [CrossRef]
- Herrmann, S. Bedarfsanalyse zur Hautkrebsprävention in sächsischen Kindertageseinrichtungen. Ph.D. Thesis, Technical University Dresden, Dresden, Germany, 2017. [Google Scholar]
- Dobbinson, S.; Wakefield, M.; Hill, D.; Girgis, A.; Aitken, J.F.; Beckmann, K.; Reeder, A.I.; Herd, N.; Spittal, M.J.; Fairthorne, A.; et al. Children’s sun exposure and sun protection: Prevalence in Australia and related parental factors. J. Am. Acad. Dermatol. 2012, 66, 938–947. [Google Scholar] [CrossRef] [PubMed]
- Meise, R.; Uter, W.; Gefeller, O.; Pfahlberg, A. Hautkrebsprävention an bayerischen Kindergärten-Ausgewählte Ergebnisse der ErlKing Sun-Studie zum Thema Sonnenschutz. Das Gesundh. 2015, 77, A1. [Google Scholar] [CrossRef]
- Vorbeck, L. Kindlicher Sonnenschutz in Oberfranken: Eine Empirische Erhebung in 79 Kindergärten. Ph.D. Thesis, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany, 2020. [Google Scholar]
- Gefeller, O.; Li, J.; Uter, W.; Pfahlberg, A.B. The impact of parental knowledge and tanning attitudes on sun protection practice for young children in Germany. Int. J. Environ. Res. Public Health 2014, 11, 4768–4781. [Google Scholar] [CrossRef] [Green Version]
- Kok, G.; Gottlieb, N.H.; Peters, G.-J.Y.; Mullen, P.D.; Parcel, G.S.; Ruiter, R.A.C.; Fernández, M.E.; Markham, C.; Bartholomew, L.K. A taxonomy of behaviour change methods: An Intervention Mapping approach. Health Psychol. Rev. 2016, 10, 297–312. [Google Scholar] [CrossRef]
- Weissberg, R.P.; Kumpfer, K.L.; Seligman, M.E.P. Prevention that works for children and youth. An introduction. Am. Psychol. 2003, 58, 425–432. [Google Scholar] [CrossRef]
- Quéreux, G.; Nguyen, J.-M.; Volteau, C.; Dréno, B. Prospective trial on a school-based skin cancer prevention project. Eur. J. Cancer Prev. 2009, 18, 133–144. [Google Scholar] [CrossRef]
- Buller, D.B.; Borland, R.; Woodall, W.G.; Hall, J.R.; Hines, J.M.; Burris-Woodall, P.; Cutter, G.R.; Miller, C.; Balmford, J.; Starling, R.; et al. Randomized trials on consider this, a tailored, internet-delivered smoking prevention program for adolescents. Health Educ. Behav. 2008, 35, 260–281. [Google Scholar] [CrossRef]
- Gies, P.; van Deventer, E.; Green, A.C.; Sinclair, C.; Tinker, R. Review of the Global Solar UV Index 2015 Workshop Report. Health Phys. 2018, 114, 84–90. [Google Scholar] [CrossRef] [Green Version]
- Purim, K.S.M.; Titski, A.C.K.; Leite, N. Photoprotection and the Environment. In Dermatology in Public Health Environments; Bonamigo, R.R., Dornelles, S.I.T., Eds.; Springer International Publishing: Basel, Switzerland, 2018; pp. 1077–1087. ISBN 978-3-319-33917-7. [Google Scholar]
- Schofield, M.J.; Edwards, K.; Pearce, R. Effectiveness of two strategies for dissemination of sun-protection policy in New South Wales primary and secondary schools. Aust. N. Z. J. Public Health 1997, 21, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Heckman, C.J.; Liang, K.; Riley, M. Awareness, understanding, use, and impact of the UV index: A systematic review of over two decades of international research. Prev. Med. 2019, 123, 71–83. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, A.J.; Olson, A.L.; Sox, C.H.; Tosteson, T.D.; Grant-Petersson, J. Persistent increase in children’s sun protection in a randomized controlled community trial. Prev. Med. 2000, 31, 569–574. [Google Scholar] [CrossRef]
- Hart, K.M.; Demarco, R.F. Primary prevention of skin cancer in children and adolescents: A review of the literature. J. Pediatr. Oncol. Nurs. 2008, 25, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Catford, J. Ottawa 1986: The fulcrum of global health development. Promot. Educ. 2007, 14 (Suppl. 2), 6–7. [Google Scholar] [CrossRef] [PubMed]
- Geene, R.; Reese, M. Handbuch Präventionsgesetz: Neuregelungen der Gesundheitsförderung; Mabuse-Verlag: Frankfurt am Main, Germany, 2017. [Google Scholar]
- Tripp, M.K.; Vernon, S.W.; Gritz, E.R.; Diamond, P.M.; Mullen, P.D. Children’s skin cancer prevention: A systematic review of parents’ psychosocial measures. Am. J. Prev. Med. 2013, 44, 265–273. [Google Scholar] [CrossRef]
- Rabin, B.A.; Glasgow, R.E.; Kerner, J.F.; Klump, M.P.; Brownson, R.C. Dissemination and implementation research on community-based cancer prevention: A systematic review. Am. J. Prev. Med. 2010, 38, 443–456. [Google Scholar] [CrossRef] [PubMed]
- Wandersman, A.; Duffy, J.; Flaspohler, P.; Noonan, R.; Lubell, K.; Stillman, L.; Blachman, M.; Dunville, R.; Saul, J. Bridging the gap between prevention research and practice: The interactive systems framework for dissemination and implementation. Am. J. Community Psychol. 2008, 41, 171–181. [Google Scholar] [CrossRef]
- Flaspohler, P.; Lesesne, C.A.; Puddy, R.W.; Smith, E.; Wandersman, A. Advances in bridging research and practice: Introduction to the second special issue on the interactive system framework for dissemination and implementation. Am. J. Community Psychol. 2012, 50, 271–281. [Google Scholar] [CrossRef]
- Campbell, M.K.; Piaggio, G.; Elbourne, D.R.; Altman, D.G. Consort 2010 statement: Extension to cluster randomised trials. BMJ 2012, 345, e5661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michie, S.; Carey, R.N.; Johnston, M.; Rothman, A.J.; de Bruin, M.; Kelly, M.P.; Connell, L.E. From Theory-Inspired to Theory-Based Interventions: A Protocol for Developing and Testing a Methodology for Linking Behaviour Change Techniques to Theoretical Mechanisms of Action. Ann. Behav. Med. 2018, 52, 501–512. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Joronen, K.; Rankin, S.H.; Astedt-Kurki, P. School-based drama interventions in health promotion for children and adolescents: Systematic review. J. Adv. Nurs. 2008, 63, 116–131. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social Learning Theory; General Limiting Press: Morristown, NJ, USA, 1971. [Google Scholar]
- Bandura, A. Health promotion from the perspective of social cognitive theory. Psychol. Health 1998, 13, 623–649. [Google Scholar] [CrossRef]
- Stiftung Deutsche Krebshilfe. Sommer, Sonne, Schattenspiele: Gut behütet vor UV-Strahlung. Available online: https://www.krebshilfe.de/fileadmin/Downloads/PDFs/Praeventionsratgeber/407_0076.pdf (accessed on 14 June 2021).
- James, A.S.; Tripp, M.K.; Parcel, G.S.; Sweeney, A.; Gritz, E.R. Psychosocial correlates of sun-protective practices of preschool staff toward their students. Health Educ. Res. 2002, 17, 305–314. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundations of thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986; ISBN 013815614X. [Google Scholar]
- Schwarzer, R. Modeling Health Behavior Change: How to Predict and Modify the Adoption and Maintenance of Health Behaviors. Appl. Psychol. 2008, 57, 1–29. [Google Scholar] [CrossRef]
- Schüz, N.; Eid, M. Beyond the usual suspects: Target group- and behavior-specific factors add to a theory-based sun protection intervention for teenagers. J. Behav. Med. 2013, 36, 508–519. [Google Scholar] [CrossRef]
- Schwarzer, R.; Renner, B. Health-specific self-efficacy scales. Freie Univ. Berl. 2009, 14, 2009. [Google Scholar]
- Rogers, E.M. Diffusion of Innovations; The Free Press: New York, NY, USA, 1995. [Google Scholar]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the public health impact of health promotion interventions: The RE-AIM framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Academic Press: New York, NY, USA, 1988. [Google Scholar]
- Reilly, J.J.; Kelly, L.; Montgomery, C.; Williamson, A.; Fisher, A.; McColl, J.H.; Lo Conte, R.; Paton, J.Y.; Grant, S. Physical activity to prevent obesity in young children: Cluster randomised controlled trial. BMJ 2006, 333, 1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedges, L.V.; Hedberg, E.C. Intraclass Correlation Values for Planning Group-Randomized Trials in Education. Educ. Eval. Policy Anal. 2007, 29, 60–87. [Google Scholar] [CrossRef] [Green Version]
- Peñalvo, J.L.; Sotos-Prieto, M.; Santos-Beneit, G.; Pocock, S.; Redondo, J.; Fuster, V. The Program SI! intervention for enhancing a healthy lifestyle in preschoolers: First results from a cluster randomized trial. BMC Public Health 2013, 13, 1208. [Google Scholar] [CrossRef] [Green Version]
- Van Breukelen, G.J.P.; Candel, M.J.J.M. Calculating sample sizes for cluster randomized trials: We can keep it simple and efficient! J. Clin. Epidemiol. 2012, 65, 1212–1218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutterford, C.; Copas, A.; Eldridge, S. Methods for sample size determination in cluster randomized trials. Int. J. Epidemiol. 2015, 44, 1051–1067. [Google Scholar] [CrossRef] [Green Version]
- Field, A. Discovering Statistics Using SPSS (and Sex and Drugs and ROCK’N’ROLL); Sage: London, UK, 2009. [Google Scholar]
- Wu, S.; Crespi, C.M.; Wong, W.K. Comparison of methods for estimating the intraclass correlation coefficient for binary responses in cancer prevention cluster randomized trials. Contemp. Clin. Trials 2012, 33, 869–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedges, L.V. Effect Sizes in Cluster-Randomized Designs. J. Educ. Behav. Stat. 2007, 32, 341–370. [Google Scholar] [CrossRef] [Green Version]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- IBM SPSS Statistics for Windows; IBM Corp: Armonk, NY, USA, 2020.
- Owen, N.; Glanz, K.; Sallis, J.F.; Kelder, S.H. Evidence-based approaches to dissemination and diffusion of physical activity interventions. Am. J. Prev. Med. 2006, 31, S35–S44. [Google Scholar] [CrossRef] [PubMed]
- Sümen, A.; Öncel, S. Development of sun protection behaviors in preschoolers: A systematic review. Turkderm 2018, 52, 56–63. [Google Scholar] [CrossRef]
- Thoonen, K.; van Osch, L.; de Vries, H.; Jongen, S.; Schneider, F. Are Environmental Interventions Targeting Skin Cancer Prevention among Children and Adolescents Effective? A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunkin, H.; Pollock, K.; Scupham, R. The National SunSmart Schools Program: Impact on sun protection policies and practices in Australian primary schools. Health Promot. J. Austr. 2020, 31, 251–257. [Google Scholar] [CrossRef]
- Tripp, M.; Talati, P.P.; Winters, E.; Yallen, A.S.; Galvan, C.; Euresti, M.; Garrison, S.; Gritz, E.; Peterson, S. Sunbeatables™ program implementation research in preschools. In Proceedings of the 8th Annual Conference on the Science of Dissemination and Implementation, Washington, DC, USA, 14–15 December 2015. [Google Scholar]
- Fiessler, C.; Pfahlberg, A.B.; Uter, W.; Gefeller, O. Shedding Light on the Shade: How Nurseries Protect Their Children from Ultraviolet Radiation. Int. J. Environ. Res. Public Health 2018, 15, 1793. [Google Scholar] [CrossRef] [Green Version]
- Hunkin, H.; Morris, J.N. A decade of sun protection in Australian early-childhood services: Analysis of cross-sectional and repeated-measures data. Health Educ. Res. 2020, 35, 99–109. [Google Scholar] [CrossRef]
- Harrison, S.L.; Saunders, V.; Nowak, M. Baseline survey of sun-protection knowledge, practices and policy in early childhood settings in Queensland, Australia. Health Educ. Res. 2007, 22, 261–271. [Google Scholar] [CrossRef] [Green Version]
- Tripp, M.; Talati, P.P.; Galvan, C.; Garrison, S.; Parrish, M.; Sibai, D.; Giordano, J.; Euresti, M.; Yallen, A.S.; Gritz, E.; et al. Sunbeatables™: Conceptualization of Implementation and Sustainability for a Preschool Sun Protection Program. In Proceedings of the 9th Annual Conference on the Science of Dissemination and Implementation, Washington, DC, USA, 14–15 December 2016. [Google Scholar]
- Li, J.; Uter, W.; Pfahlberg, A.; Gefeller, O. A comparison of patterns of sun protection during beach holidays and everyday outdoor activities in a population sample of young German children. Br. J. Dermatol. 2012, 166, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Herbert, R.D.; McAuley, J.H. Mediation Analysis. JAMA 2019, 321, 697–698. [Google Scholar] [CrossRef] [PubMed]
- Gefeller, O.; Uter, W.; Pfahlberg, A.B. Protection from Ultraviolet Radiation during Childhood: The Parental Perspective in Bavaria. Int. J. Environ. Res. Public Health 2016, 13, 1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bock-Famulla, K.; Münchow, A.; Frings, J.; Kempf, F.; Schütz, J. Länderreport Frühkindliche Bildungssysteme 2019; Bertelsmann Stiftung: Gütersloh, Germany, 2020. [Google Scholar]
- LoConte, N.K.; Gershenwald, J.E.; Thomson, C.A.; Crane, T.E.; Harmon, G.E.; Rechis, R. Lifestyle Modifications and Policy Implications for Primary and Secondary Cancer Prevention: Diet, Exercise, Sun Safety, and Alcohol Reduction. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 88–100. [Google Scholar] [CrossRef]
- Nicholson, A.K.; Hill, J.; Walker, H.; Heward, S.; Dobbinson, S. Teacher perceptions of sun protection practices in the secondary school setting: Barriers, enablers and recommendations for future. Health Promot. J. Austr. 2020, 31, 258–267. [Google Scholar] [CrossRef]
- Bell, M.L.; Kenward, M.G.; Fairclough, D.L.; Horton, N.J. Differential dropout and bias in randomised controlled trials: When it matters and when it may not. BMJ 2013, 346, e8668. [Google Scholar] [CrossRef] [Green Version]
- Hall, H.; Jorgensen, C.M.; McDavid, K.; Kraft, J.M.; Breslow, R. Protection from sun exposure in US white children ages 6 months to 11 years. Public Health Rep. 2001, 116, 353–361. [Google Scholar] [CrossRef]
- Mayer, J.A.; Sallis, J.F.; Eckhardt, L.; Creech, L.; Johnston, M.R.; Elder, J.P.; Lui, K.J. Assessing children’s ultraviolet radiation exposure: The use of parental recall via telephone interviews. Am. J. Public Health 1997, 87, 1046–1049. [Google Scholar] [CrossRef] [PubMed]








| Type of Measure | Recommendation |
|---|---|
| Knowledge-related | Educational measures on UV radiation and protective measures in kindergarten/preschools and schools can improve knowledge about sun protection. |
| UV-risk communication should address aspects relevant to everyday life, the subjective perception of gain by UV exposure and the ideal of beauty of tanned skin. An important starting point for communication should be social ideals and behavioral routines with regard to tanned skin and sunbathing. | |
| The range of media information on skin cancer prevention should be expanded qualitatively and quantitatively, since the media are the most important source of information for adults. | |
| Digital media literacy as part of the population’s health literacy should be promoted in order to be able to find, understand, and assess the quality of information on skin cancer and skin cancer prevention in a more targeted manner. | |
| Parents with children in kindergarten/preschool as well as educators, teachers, and daycare center/preschool managers should be informed about UV radiation as a risk factor for skin cancer and about the inadequate protective function of clouds against UV radiation. | |
| Behavioral | Interventions aimed at influencing behavior over the long term should consist of several components, be intensive, and designed to be repeated. |
| Behavioral change interventions should be based on behavioral theories and should take available evidence into account. | |
| Measures to convey primary prevention of skin cancer should be multimedia-based as well as interactive and integrate several communication channels. | |
| Information can be provided through parents, teachers, educators, peers, and other multipliers. | |
| Skin cancer prevention interventions that also address external appearance are a promising strategy for changing sun protection behavior. | |
| Measures for primary prevention of skin cancer should be designed with a focus on the target group and take the target group’s needs into account. | |
| In order to reach people where they shape their everyday lives, measures for primary prevention of skin cancer should be setting-related. | |
| Sun protection interventions for children and adolescents should be conducted in preschools and schools. | |
| The UV Index should be more intensively communicated and used in sun protection recommendations and programs. | |
| Environmental | A sufficient amount of shaded areas should be provided in kindergartens, preschools, and schools. |
| Technical and organizational measures to avoid excessive UV exposure, especially during the midday hours (e.g., provision of shaded areas, consideration of sun protection when scheduling sporting events for example) should be an essential part of primary prevention. | |
| Evaluation: Primary skin cancer prevention interventions should be evaluated formatively and summatively. The evaluation parameters used should be derived from a theoretically proven model. |
| Scope | Content | Methods for Change |
|---|---|---|
| Promoting staff’s knowledge, attitudes and behavior | Information about effects of the sun and sun protection recommendations: Background and recommendations on the prevention of skin cancer in children | Tailoring: information designed to meet staff’s stated needs of sun protection measures Facilitation: pointing at barriers to adequate sun protection and advice on overcoming these barriers Persuasive communication: Appeal to staff’s vocational goal of caring for children’s health and well-being Framing: emphasizing risks of inappropriate sun protection Consciousness raising: providing scientific background information about consequences of UV exposure Active learning: presentation of information is combined with opportunities for staff members to discuss experiences and habits |
| Group discussion on consequences of excessive UV exposure and tanning attitudes | Discussion: Staff members are encouraged to discuss their attitudes and behavior in an open debate Self-reevaluation: encouraging reflection on knowledge and attitudes | |
| Joint planning of suitable sun- protection measures on behavioral and environmental level | Participation: joint discussion assures high level of engagement of staff members, which helps to promote changes in attitudes and behavior (individual level) Goal setting/implementation intentions: discussing and fixing goals and concrete behaviors for sun protection | |
| Environmental changes in preschool | Development of an individual sun protection strategy | Participatory problem solving: staff team identifies current sun protection measures and develops a strategy for future measures Structural redesign: staff team reflects on organizational and technical elements that impede sun protection and finds ways to change them Public commitment: sun protection strategy is displayed in preschool, visible for staff and parents |
| Providing material for educational measures | Presentation and distribution of the CLEVER project week material | Facilitation: easy-to-use materials reduce barriers to sensitize children for sun protection |
| Intervention (n = 146) | Control (n = 127) | |
|---|---|---|
| Demographic characteristics | ||
| Age, mean (SD) | 42.5 (12.43) | 43.7 (12.52) |
| Gender, N females (%) | 140 (96.6) | 123 (96.9) |
| Education, N (%) | ||
| Less than 10th grade | 1 (0.7) | 0 (0.0) |
| 10th grade | 85 (61.6) | 76 (60.8) |
| Higher than 10th grade | 52 (30.2) | 49 (39.2) |
| Baseline outcome scores | ||
| Behavioral outcomes, mean (SD) | ||
| Sunscreen use | 2.40 (0.81) | 2.21 (0.81) |
| Sun avoidance | 2.80 (0.51) | 2.82 (0.43) |
| Psychosocial outcomes, mean (SD) | ||
| Sunscreen use self-efficacy | 3.11 (0.62) | 3.06 (0.73) |
| Sun avoidance self-efficacy | 3.03 (0.61) | 3.11 (0.61) |
| Health-related outcome expectancies | 3.40 (1.00) | 3.26 (1.08) |
| Appearance-related outcome expectancies | 2.50 (0.90) | 2.53 (1.03) |
| Impediments to sunscreen use | 0.73 (0.94) | 0.97 (1.23) |
| Impediments to sun avoidance | 1.65 (0.92) | 1.41 (1.01) |
| Necessity of sun protection | 3.08 (1.07) | 3.07 (0.62) |
| Sun protection policy, mean (SD) | 1.50 (1.18) | 1.73 (1.23) |
| Scale | Within Group Difference Intervention Group | Within Group Difference Control Group | Between Group Difference in Changes | |||||
|---|---|---|---|---|---|---|---|---|
| Score Range | Baseline–1 Month Mean (95% CI) 1 | Baseline–1 Year Mean (95% CI)1 | Baseline–1 Month Mean (95% CI)1 | Baseline–1 Year Mean (95% CI) 1 | Mean (95% CI) 1 | Test for Significance | Effect Size Hedges’ dB (95% CI) | |
| Behavioral Outcomes | ||||||||
| Sunscreen Use | 0–4 | 0.47 (0.25, 0.69) | 0.46 (0.24, 0.68) | −0.01 (−0.40, 0.37) | F(1, 12.6) = 0.01, p = 0.95 | −0.01 (−0.43, 0.40) | ||
| Sun-Avoidance | 0–4 | 0.17 (0.05, 0.29) | −0.02 (−0.15, 0.10) | 0.19 (0.02, 0.37) | F(1, 140) = 4.93, p ˂ 0.05 | 0.70 (0.04, 0.71) | ||
| Psychosocial Outcomes | ||||||||
| Sunscreen Use Self-Efficacy | 0–4 | 0.40 (0.26, 0.54) | 0.08 (−0.07, 0.23) | 0.30 (0.02, 0.57) | F(1, 18.2) = 5.12, p ˂ 0.05 | 0.71 (0.03, 0.88) | ||
| Sun-Avoidance Self-Efficacy | 0–4 | 0.29 (0.15, 0.43) | −0.20 (−0.35, −0.05) | 0.49 (0.26, 0.72) | F(1, 9.8) = 22.38, p ˂ 0.001 | 1.09 (0.39, 1.07) | ||
| Health-Related Outcome Expectancies | 0–4 | 0.24 (−0.03, 0.52) | 0.39 (0.10, 0.68) | 0.21 (−0.22, 0.65) | F(1, 15.7) = 0.40, p = 0.54 | 0.24 (−0.23, 0.69) | ||
| Appearance-Related Outcome Expectancies | 0–4 | 0.01 (−0.21, 0.22) | 0.00 (−0.22, 0.22) | 0.00 (−0.35, 0.36) | F(1, 16.3) = 0.00, p = 0.99 | 0.00 (−0.29, 0.30) | ||
| Impediments to Sunscreen Use | 0–4 | −0.17 (−0.37, 0.03) | −0.15 (−0.36, 0.06) | −0.15 (−0.43, 0.13) | F(1,18.2) = 0.00, p = 0.97 | −0.20 (−0.50, 0.15) | ||
| Impediments to Sun Avoidance | 0–4 | −0.32 (−0.52, −0.12) | 0.11 (−0.09, 0.32) | −0.43 (−0.72, −0.15) | F(1,141) = 9.27, p < 0.01 | −0.56 (−0.82, −0.17) | ||
| Necessity for Sun protection | 0–4 | 0.36 (−0.07, 0.33) | - | 0.23 (0.08, 0.37) | - | 0.14 (−0.09, 0.36) | F(1,18.6) = 1.62, p = 0.22 | 0.35 (−0.14, 0.57) |
| Sun protection Policy | 0–3 | 0.72 (0.38, 1.06) | 0.59 (0.26, 0.91) | 0.13 (−0.34, 0.60) | F(1,118) = 0.31, p = 0.58 | 0.08 (−0.26, 0.46) | ||
| Scales and Items | Scale Mean (SD) | Item Median (Range) |
|---|---|---|
| Behavioral outcomes | ||
| Sunscreen Use | 2.31 (0.82) | |
| Put sunscreen on students when outside | 3 (4) | |
| Take sunscreen along on field trips | 2 (4) | |
| Use sunscreen for students UPF 30+ | 4 (4) | |
| Reapply sunscreen every 2 h | 2 (4) | |
| Put sunscreen on myself when outside with students | 4 (4) | |
| Sun-Avoidance | 2.81 (0.47) | |
| Students wear hats/caps when outside | 2 (3) | |
| Students wear tank tops/halter tops when outside1 | 2 (4) | |
| Students wear long shorts/skirts when outside | 2 (4) | |
| Set up shaded areas outside and on field trips | 4 (4) | |
| Keep to shaded areas themselves and use protective clothing, when outside with students | 3 (4) | |
| Psychosocial outcomes | ||
| Sunscreen Use Self-Efficacy | 3.09 (0.67) | |
| Properly apply sunscreen | 4 (4) | |
| Ensure parents support provision/use of sunscreen | 3 (4) | |
| Take sunscreen on any occasion | 3 (4) | |
| Get more sunscreen when necessary | 3 (4) | |
| Sun-Avoidance Self-Efficacy | 3.07 (0.61) | |
| Ensure parents provide protective clothing | 3 (4) | |
| Decide if area is sufficiently shaded | 4 (4) | |
| Check students wearing protective clothing | 2 (4) | |
| Provide spare clothes | 4 (3) | |
| Health-Related Outcome Expectancies | 3.34 (1.04) | |
| Decreased risk for premature skin-aging | 4 (4) | |
| Decreased risk for skin cancer | 4 (4) | |
| Appearance-Related Outcome Expectancies | 2.51 (0.96) | |
| Tanning makes me look better 1 | 2 (4) | |
| Tanned skin is healthy skin 1 | 3 (4) | |
| Impediments to Sunscreen Use | 1.14 (0.84) | |
| It takes too much time | 0 (4) | |
| It is always messy | 0 (4) | |
| Impediments to Sun-Avoidance | 1.29 (0.88) | |
| We do not have enough shade | 0 (4) | |
| Preventing taking of protective clothing is difficult | 2 (4) | |
| Necessity of Sun protection | 3.08 (0.67) | |
| At the beach | 4 (4) | |
| At noon | 4 (4) | |
| On sunny evenings | 2 (4) | |
| On cloudy summer days | 2 (4) | |
| During outdoor sports activities | 4 (4) | |
| Sun Protection Policy | 1.60 (1.20) | |
| Parents are requested to bring hats or protective clothing | 1 (1) | |
| Parents are requested to provide sunscreen or preschool supplies sunscreen | 1 (1) | |
| Parents are requested to provide permission for the use of sunscreen | 0 (1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seidel, N.; Fieber, V.; Breitbart, E.W.; Bornhäuser, M.; Stölzel, F. Cluster Randomized Trial: Sun Protection Intervention ‘Clever in Sun and Shade for Preschools’—Effectiveness and Dissemination. Children 2021, 8, 651. https://doi.org/10.3390/children8080651
Seidel N, Fieber V, Breitbart EW, Bornhäuser M, Stölzel F. Cluster Randomized Trial: Sun Protection Intervention ‘Clever in Sun and Shade for Preschools’—Effectiveness and Dissemination. Children. 2021; 8(8):651. https://doi.org/10.3390/children8080651
Chicago/Turabian StyleSeidel, Nadja, Vera Fieber, Eckhard Wilhem Breitbart, Martin Bornhäuser, and Friederike Stölzel. 2021. "Cluster Randomized Trial: Sun Protection Intervention ‘Clever in Sun and Shade for Preschools’—Effectiveness and Dissemination" Children 8, no. 8: 651. https://doi.org/10.3390/children8080651
APA StyleSeidel, N., Fieber, V., Breitbart, E. W., Bornhäuser, M., & Stölzel, F. (2021). Cluster Randomized Trial: Sun Protection Intervention ‘Clever in Sun and Shade for Preschools’—Effectiveness and Dissemination. Children, 8(8), 651. https://doi.org/10.3390/children8080651