
Associations between Physical Activity and Mental Health in Iranian Adolescents during the COVID-19 Pandemic: An Accelerometer-Based Study


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Physical Activity
2.2.2. Mental Health
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Physical Activity
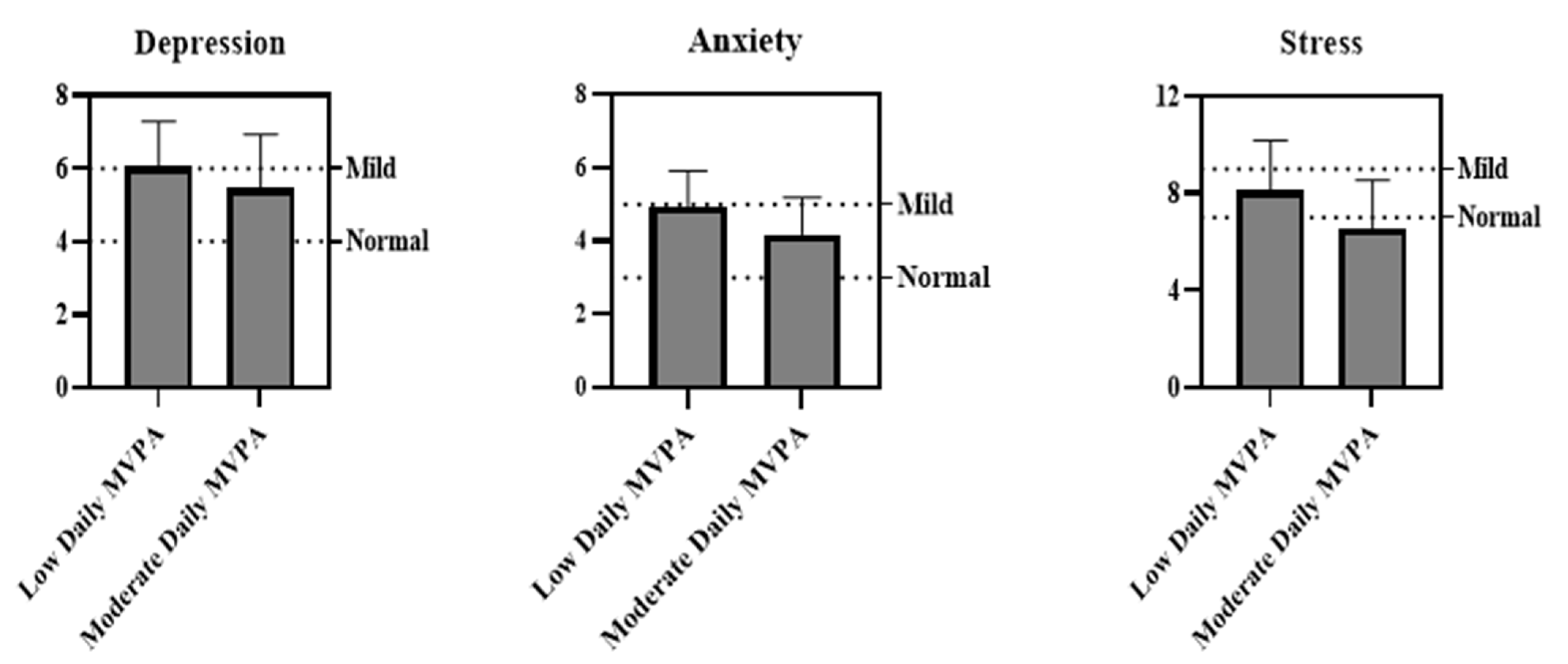
3.2. Physical Activity and Mental Health
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Caspersen, C.J.; E Powell, K.; Christenson, G.M. Physical Activity, Exercise, and Physical Fitness: Definitions and Distinctions for Health-Related Research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Thivel, D.; Tremblay, A.; Genin, P.M.; Panahi, S.; Riviere, D.; Duclos, M. Physical Activity, Inactivity, and Sedentary Behaviors: Definitions and Implications in Occupational Health. Front. Public Health 2018, 6, 288. [Google Scholar] [CrossRef] [PubMed]
- Marker, A.M.; Steele, R.G.; Noser, A.E. Physical Activity and Health-Related Quality of Life in Children and Adolescents: A Systematic Review and Meta-Analysis. Health Psychol. 2018, 37, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; LeBlanc, A.G. Systematic Review of the Health Benefits of Physical Activity and Fitness in School-Aged Children and Youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warburton, D.E.R.; Bredin, S.S.D. Health Benefits of Physical Activity: A Systematic Review of Current Systematic Reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Poitras, V.J.; Gray, C.; Borghese, M.M.; Carson, V.; Chaput, J.-P.; Janssen, I.; Katzmarzyk, P.; Pate, R.R.; Gorber, S.C.; Kho, M.; et al. Systematic Review of the Relationships Between Objectively Measured Physical Activity and Health Indicators in School-Aged Children and Youth. Appl. Physiol. Nutr. Metab. 2016, 41, S197–S239. [Google Scholar] [CrossRef]
- Huotari, P.; Nupponen, H.; Mikkelsson, L.; Laakso, L.; Kujala, U. Adolescent Physical Fitness and Activity as Predictors of Adulthood Activity. J. Sports Sci. 2011, 29, 1135–1141. [Google Scholar] [CrossRef]
- Telama, R.; Yang, X.; Viikari, J.; Välimäki, I.; Wanne, O.; Raitakari, O. Physical Activity from Childhood to Adulthood: A 21-Year Tracking Study. Am. J. Prev. Med. 2005, 28, 267–273. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour 2020. Geneva, Switzerland: World Health Organization. 2020. Available online: https://www.who.int/publications/i/item/9789240015128. (accessed on 2 June 2021).
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Bio Med. Atenei Parm. 2020, 91, 157–160. [Google Scholar] [CrossRef]
- Bedford, J.; Enria, D.; Giesecke, J.; Heymann, D.L.; Ihekweazu, C.; Kobinger, G.; Lane, H.C.; Memish, Z.; Oh, M.-D.; Schuchat, A. COVID-19: Towards Controlling of a Pandemic. Lancet 2020, 395, 1015–1018. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Leblanc, A.G.; E Kho, M.; Saunders, T.J.; Larouche, R.; Colley, R.C.; Goldfield, G.; Gorber, S.C. Systematic Review of Sedentary Behaviour and Health Indicators in School-Aged Children and Youth. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallis, J.F.; Bull, F.; Guthold, R.; Heath, G.W.; Inoue, S.; Kelly, P.; Oyeyemi, A.L.; Perez, L.G.; Richards, J.; Hallal, P.C. Progress in Physical Activity over the Olympic Quadrennium. Lancet 2016, 388, 1325–1336. [Google Scholar] [CrossRef]
- Yomoda, K.; Kurita, S. Influence of Social Distancing During the COVID-19 Pandemic on Physical Activity in Children: A Scoping Review of the Literature. J. Exerc. Sci. Fit. 2021, 19, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Dunton, G.F.; Do, B.; Wang, S.D. Early Effects of the COVID-19 Pandemic on Physical Activity and Sedentary Behavior in Children Living in the U.S. BMC. Public. Heal. 2020, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, V.A.; Starc, G.; Brandes, M.; Kaj, M.; Blagus, R.; Leskošek, B.; Suesse, T.; Dinya, E.; Guinhouya, B.C.; Zito, V.; et al. Physical Activity, Screen Time and the COVID-19 School Closures in Europe—An Observational Study in 10 Countries. Eur. J. Sport Sci. 2021, 29, 1–10. [Google Scholar] [CrossRef]
- Ruíz-Roso, M.B.; de Carvalho Padilha, P.; Matilla-Escalante, D.C.; Brun, P.; Ulloa, N.; Acevedo-Correa, D.; Arantes Ferreira Peres, W.; Martorell, M.; Rangel Bousquet Carrilho, T.; de Oliveira Cardoso, L.; et al. Changes of Physical Activity and Ultraprocessed Food Consumption in Adolescents from Different Countries during COVID-19 Pandemic: An Observational Study. Nutrients 2020, 12, 2289. [Google Scholar] [CrossRef] [PubMed]
- Arvidsson, D.; Fridolfsson, J.; Börjesson, M. Measurement of Physical Activity in Clinical Practice Using Accelerometers. J. Intern. Med. 2019, 286, 137–153. [Google Scholar] [CrossRef] [Green Version]
- Mueller, C.; Winter, C.; Rosenbaum, D. Current Objective Techniques for Physical Activity Assessment in Comparison with Subjective Methods. Dtsch. Z. Sportmed. 2010, 61, 11–18. [Google Scholar]
- Slootmaker, S.M.; Schuit, A.J.; Chinapaw, M.J.; Seidell, J.C.; van Mechelen, W. Disagreement in Physical Activity Assessed by Accelerometer and Self-Report in Subgroups of Age, Gender, Education and Weight Status. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 17. [Google Scholar] [CrossRef] [Green Version]
- Marasso, D.; Lupo, C.; Collura, S.; Rainoldi, A.; Brustio, P. Subjective versus Objective Measure of Physical Activity: A Systematic Review and Meta-Analysis of the Convergent Validity of the Physical Activity Questionnaire for Children (PAQ-C). Int. J. Environ. Res. Public. Heal. 2021, 18, 3413. [Google Scholar] [CrossRef]
- Abawi, O.; Welling, M.S.; Eynde, E.V.D.; Van Rossum, E.F.C.; Halberstadt, J.; Akker, E.L.T.V.D.; Van Der Voorn, B. COVID -19 Related Anxiety in Children and Adolescents with Severe Obesity: A Mixed-Methods Study. Clin. Obes. 2020, 10, e12412. [Google Scholar] [CrossRef] [PubMed]
- De Miranda, D.M.; Athanasio, B.d.S.; Oliveira, A.C.S.; Simoes-e-Silva, A.C. How Is COVID-19 Pandemic Impacting Mental Health of Children and Adolescents? Int. J. Disaster. Risk. Reduct. 2020, 51, 101845. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Devine, J.; Schlack, R.; Otto, C. Impact of the COVID-19 Pandemic on Quality of Life and Mental Health in Children and Adolescents in Germany. Eur. Child. Adolesc. Psychiatry. 2021, 1–11. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, H.; Ma, X.; Di, Q. Mental Health Problems during the COVID-19 Pandemics and the Mitigation Effects of Exercise: A Longitudinal Study of College Students in China. Int. J. Environ. Res. Public. Heal. 2020, 17, 3722. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.; Fedewa, A.L. A Meta-analysis of the Relationship Between Children’s Physical Activity and Mental Health. J. Pediatr. Psychol. 2011, 36, 385–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Moor, M.; Beem, A.; Stubbe, J.; Boomsma, D.; de Geus, E. Regular Exercise, Anxiety, Depression and Personality: A Population-Based Study. Prev. Med. 2006, 42, 273–279. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Ayllon, M.; Cadenas-Sánchez, C.; Estévez-López, F.; Muñoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-Garcia, P.; Henriksson, H.; Mena-Molina, A.; Martínez-Vizcaíno, V.; et al. Role of Physical Activity and Sedentary Behavior in the Mental Health of Preschoolers, Children and Adolescents: A Systematic Review and Meta-Analysis. Sports. Med. 2019, 49, 1383–1410. [Google Scholar] [CrossRef] [PubMed]
- Ussher, M.H.; Owen, C.G.; Cook, D.G.; Whincup, P.H. The Relationship Between Physical Activity, Sedentary Behaviour and Psychological Well-being among Adolescents. Soc. Psychiatry. Psychiatr. Epidemiology. 2007, 42, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.; Richards, J.; Hillman, C.; Faulkner, G.; Beauchamp, M.; Nilsson, M.; Kelly, P.; Smith, J.; Raine, L.; Biddle, S. Physical Activity for Cognitive and Mental Health in Youth: A Systematic Review of Mechanisms. Pediatrics 2016, 138, e20161642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, K.R. The Influence of Physical Activity on Mental Well-being. Public. Heal. Nutr. 1999, 2, 411–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijndaele, K.; Westgate, K.; Stephens, S.K.; Blair, S.N.; Bull, F.C.; Chastin, S.F.; Dunstan, D.W.; Ekelund, U.; Esliger, D.W.; Freedson, P.S.; et al. Utilization and Harmonization of Adult Accelerometry Data: Review and Expert Consensus. Med. Sci. Sports. Exerc. 2015, 47, 2129–2139. [Google Scholar] [CrossRef] [Green Version]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales, 2nd ed.; Psychology Foundation of Australia: Sydney, Australia, 1995. [Google Scholar]
- Shaw, T.; Campbell, M.; Runions, K.; Zubrick, S. Properties of the DASS-21 in an Australian Community Adolescent Population. J. Clin. Psychol. 2016, 73, 879–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asghari, A.; Saed, F.; Dibajnia, P. Psychometric Properties of the Depression Anxiety Stress Scales-21 (DASS-21) in a Non-Clinical Iranian Sample. Int. J. Psychol. 2008, 2, 82–102. [Google Scholar]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of Two Objective Measures of Physical Activity for Children. J. Sports. Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Choi, L.; Liu, Z.; Matthews, C.E.; Buchowski, M.S. Validation of Accelerometer Wear and Non-Wear Time Classification Algorithm. Med. Sci. Sports. Exerc. 2011, 43, 357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morres, I.; Galanis, E.; Hatzigeorgiadis, A.; Androutsos, O.; Theodorakis, Y. Physical Activity, Sedentariness, Eating Behaviour and Well-Being during a COVID-19 Lockdown Period in Greek Adolescents. Nutrients 2021, 13, 1449. [Google Scholar] [CrossRef] [PubMed]
- Tulchin-Francis, K.; Stevens, W.; Gu, X.; Zhang, T.; Roberts, H.; Keller, J.; Dempsey, D.; Borchard, J.; Jeans, K.; VanPelt, J. The Impact of the Coronavirus Disease 2019 Pandemic on Physical Activity in U.S. Children. J. Sport. Heal. Sci. 2021, 10, 323–332. [Google Scholar] [CrossRef]
- Moore, S.; Faulkner, G.; Rhodes, R.E.; Brussoni, M.; Chulak-Bozzer, T.; Ferguson, L.J.; Mitra, R.; O’Reilly, N.; Spence, J.C.; Vanderloo, L.M.; et al. Impact of the COVID-19 Virus Outbreak on Movement and Play Behaviours of Canadian Children and Youth: A National Survey. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Vilhjalmsson, R.; Kristjánsdóttir, G. Gender Differences in Physical Activity in Older Children and Adolescents: The Central Role of Organized Sport. Soc. Sci. Med. 2002, 56, 363–374. [Google Scholar] [CrossRef]
- Ishii, K.; Shibata, A.; Adachi, M.; Nonoue, K.; Oka, K. Gender and Grade Differences in Objectively Measured Physical Activity and Sedentary Behavior Patterns among Japanese Children and Adolescents: A Cross-Cectional Study. BMC. Public. Heal. 2015, 15, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Trost, S.G.; Pate, R.R.; Sallis, J.F.; Freedson, P.S.; Taylor, W.C.; Dowda, M.; Sirard, J. Age and Gender Differences in Objectively Measured Physical Activity in Youth. Med. Sci. Sports. Exerc. 2002, 34, 350–355. [Google Scholar] [CrossRef]
- Saller, F.V.I.; Khaled, S.M. Potential Psychosocial Influences on Gender Differences in Physical Activity among Qatari Adolescents: A First Insight Through Descriptive Observation. Int. J. Adolesc. Youth. 2018, 24, 234–251. [Google Scholar] [CrossRef] [Green Version]
- Lenhart, C.M.; Hanlon, A.; Kang, Y.; Daly, B.P.; Brown, M.D.; Patterson, F. Gender Disparity in Structured Physical Activity and Overall Activity Level in Adolescence: Evaluation of Youth Risk Behavior Surveillance Data. ISRN. Public. Health. 2012, 2012. [Google Scholar] [CrossRef] [Green Version]
- Chalabaev, A.; Sarrazin, P.; Fontayne, P.; Boiché, J.; Clément-Guillotin, C. The Influence of Sex Stereotypes and Gender Roles on Participation and Performance in Sport and Exercise: Review and Future Directions. Psychol. Sport. Exerc. 2013, 14, 136–144. [Google Scholar] [CrossRef] [Green Version]
- Leaper, C.; Friedman, C.K. The Socialization of Gender. In Handbook of Socialization: Theory and Research; Grusec, J.E., Hastings, P.D., Eds.; The Guilford Press: New York, USA, 2007; pp. 561–587. [Google Scholar]
- Butt, J.; Weinberg, R.S.; Breckon, J.D.; Claytor, R.P. Adolescent Physical Activity Participation and Motivational Determinants Across Gender, Age, and Race. J. Phys. Act. Heal. 2011, 8, 1074–1083. [Google Scholar] [CrossRef] [PubMed]
- Dragun, R.; Veček, N.N.; Marendić, M.; Pribisalić, A.; Đivić, G.; Cena, H.; Polašek, O.; Kolčić, I. Have Lifestyle Habits and Psychological Well-Being Changed among Adolescents and Medical Students Due to COVID-19 Lockdown in Croatia? Nutrients 2021, 13, 97. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Sun, Y.; Zhang, X.; Sun, F.; Wang, B.; Zhu, W. Is Physical Activity Associated with Mental Health among Chinese Adolescents during Isolation in COVID-19 Pandemic? J. Epidemiol. Glob. Health. 2020, 11, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Chi, X.; Liang, K.; Chen, S.-T.; Huang, L.; Guo, T.; Jiao, C.; Yu, Q.; Veronese, N.; Soares, F.C.; et al. Moving More and Sitting Less as Healthy Lifestyle Behaviors are Protective Factors for Insomnia, Depression, and Anxiety Among Adolescents During the COVID-19 Pandemic. Psychol. Res. Behav. Manag. 2020, 13, 1223–1233. [Google Scholar] [CrossRef] [PubMed]
- Wunsch, K.; Nigg, C.; Niessner, C.; Schmid, S.C.E.; Oriwol, D.; Hanssen-Doose, A.; Burchartz, A.; Eichsteller, A.; Kolb, S.; Worth, A.; et al. The Impact of COVID-19 on the Interrelation of Physical Activity, Screen Time and Health-Related Quality of Life in Children and Adolescents in Germany: Results of the Motorik-Modul Study. Children 2021, 8, 98. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | Overall | Boys (n = 60) | Girls (n = 76) | Results of t-Tests | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| Age | 16.28 | 0.97 | 16.35 | 0.98 | 16.23 | 0.96 | t = 0.672 p = 0.503 |
| Height (cm) | 164.97 | 10.29 | 165.23 | 10.68 | 164.77 | 10.03 | t = 0.256 p = 0.798 |
| Weight (kg) | 63.25 | 10.03 | 64.36 | 10.47 | 62.36 | 9.64 | t = 1.155 p = 0.250 |
| BMI (kg/m2) | 23.28 | 3.49 | 23.63 | 3.71 | 23.00 | 3.31 | t = 1.044 p = 0.298 |
| Accelerometer Data | |||||||
| % Sedentary Behavior | 71.98 | 3.13 | 71.80 | 1.53 | 72.38 | 3.95 | t = 0.794 p = 0.428 |
| s% Light PA | 23.19 | 2.24 | 22.83 | 0.88 | 23.30 | 2.89 | t = −0.713 p = 0.220 |
| % Moderate PA | 3.34 | 0.90 | 3.59 | 0.92 | 3.05 | 0.64 | t = −3.568 *** p = 0.000 |
| % Vigorous PA | 1.49 | 1.06 | 1.78 | 0.88 | 1.27 | 1.14 | t = 4.005 *** p = 0.000 |
| % MVPA | 4.83 | 1.57 | 5.37 | 1.66 | 4.32 | 1.45 | t = −4.651 *** p = 0.000 |
| Total MVPA (min) | 135.68 | 44.58 | 144.87 | 43.38 | 124.05 | 36.40 | t = −2.771 ** p = 0.006 |
| Daily MVPA (min) | 18.47 | 6.46 | 19.66 | 7.10 | 16.96 | 5.22 | t = −2.461 * p = 0.015 |
| Daily Energy Expenditure (Kcal) | 306.63 | 76.26 | 2368.32 | 608.97 | 2131.92 | 514.23 | t = −2.405 * p = 0.018 |
| Depression | Anxiety | Stress | |
|---|---|---|---|
| MVPA | β = −0.290 t = −3.505 R2 = 0.084 F1,134 = 12.288 * | β = −0.404 t = −5.106 R2 = 0.163 F1,134 = 26.069 ** | β = −0.298 t = −3.619 R2 = 0.089 F1,134 = 13.096 ** |
| Age | β = −0.142 t = −1.660 R2 = 0.020 F1,134 = 2.755 | β = −0.123 t = −1.450 R2 = 0.018 F1,134 = 2.325 | β = −0.113 t = −1.317 R2 = 0.013 F1,134 = 1.735 |
| Gender | β = −0.033 t = −0.380 R2 = 0.001 F1,134 = 0.144 | β = 0.084 t = 0.979 R2 = 0.007 F1,134 = 0.959 | β = 0.117 t = 1.368 R2 = 0.014 F1,134 = 1.871 |
| BMI | β = −0.071 t = −0.819 R2 = 0.005 F1,134 = 0.670 | β = −0.090 t = −1.041 R2 = 0.008 F1,134 = 1.084 | β = −0.146 t = −1.712 R2 = 0.021 F1,134 = 2.932 |
| Mental Health | Overall | Boys (n = 60) | Girls (n = 76) | Results of t-Tests | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| Depression | 5.86 | 1.33 | 5.91 | 1.36 | 5.82 | 1.31 | t = 0.380 p = 0.705 |
| Anxiety | 4.69 | 1.04 | 4.60 | 1.02 | 4.77 | 1.05 | t = −0.979 p = 0.329 |
| Stress | 7.61 | 2.16 | 7.33 | 2.28 | 7.84 | 2.04 | t = −1.368 p = 0.174 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghorbani, S.; Afshari, M.; Eckelt, M.; Dana, A.; Bund, A. Associations between Physical Activity and Mental Health in Iranian Adolescents during the COVID-19 Pandemic: An Accelerometer-Based Study. Children 2021, 8, 1022. https://doi.org/10.3390/children8111022
Ghorbani S, Afshari M, Eckelt M, Dana A, Bund A. Associations between Physical Activity and Mental Health in Iranian Adolescents during the COVID-19 Pandemic: An Accelerometer-Based Study. Children. 2021; 8(11):1022. https://doi.org/10.3390/children8111022
Chicago/Turabian StyleGhorbani, Saeed, Mostafa Afshari, Melanie Eckelt, Amir Dana, and Andreas Bund. 2021. "Associations between Physical Activity and Mental Health in Iranian Adolescents during the COVID-19 Pandemic: An Accelerometer-Based Study" Children 8, no. 11: 1022. https://doi.org/10.3390/children8111022
APA StyleGhorbani, S., Afshari, M., Eckelt, M., Dana, A., & Bund, A. (2021). Associations between Physical Activity and Mental Health in Iranian Adolescents during the COVID-19 Pandemic: An Accelerometer-Based Study. Children, 8(11), 1022. https://doi.org/10.3390/children8111022