Familial Factors Associating with Youth Physical Activity Using a National Sample

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Data Processing
2.4. Statistical Analysis
3. Results
3.1. Child-Level Demographics
3.2. Physical Activity and Family-Level Descriptive Statistics
3.3. Weighted Logistic Regression Results
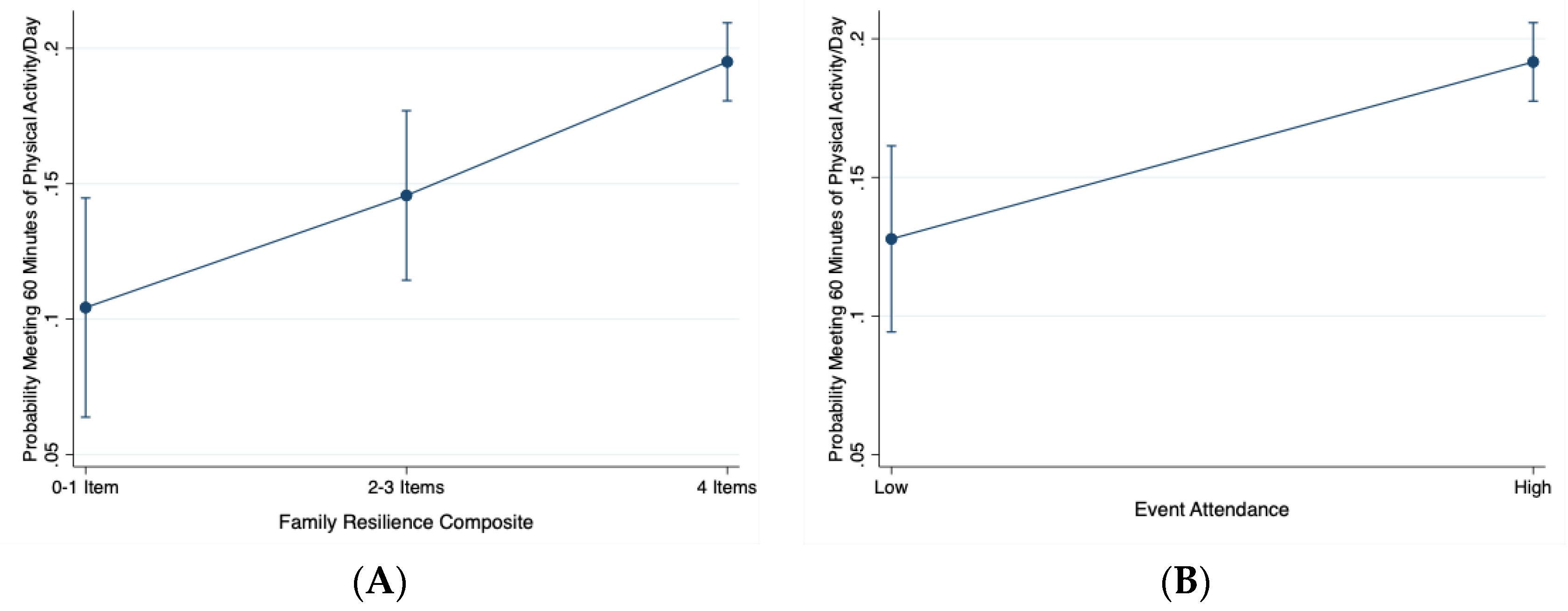
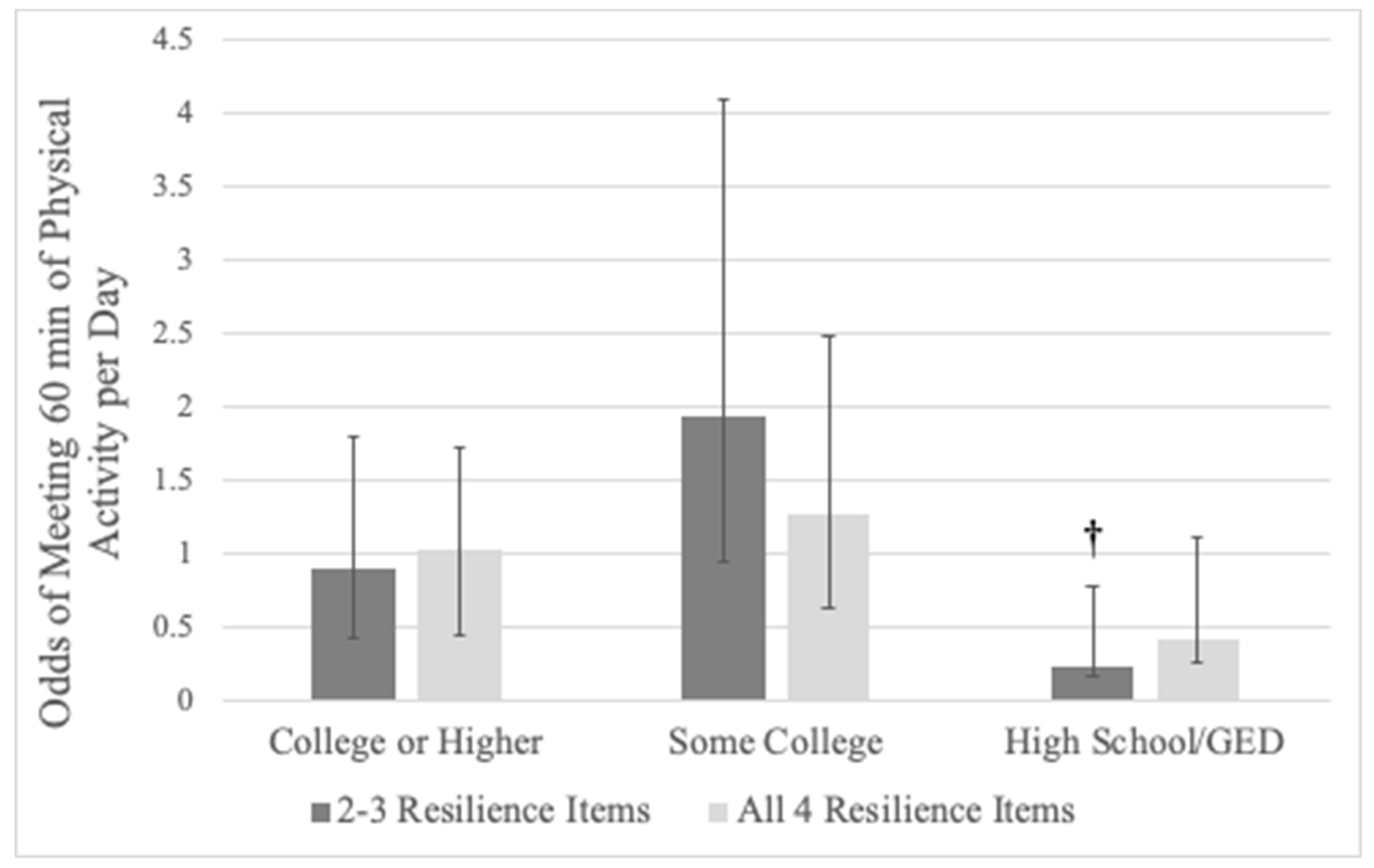
3.4. Family-Level and Child-Level Joint Associations
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ekelund, U.; Luan, J.; Sherar, L.B.; Eslinger, D.W.; Griew, P.; Cooper, A.; International Children’s Accelerometry Database (ICAD) Collaborators. Moderate to vigorous physical activity and sedentary time and cardio-metabolic risk factors in children and adolescents. JAMA 2012, 307, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be smart, exercise your heart: Exercise effects on brain and cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef]
- Biddle, S.J.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–995. [Google Scholar] [CrossRef]
- National Physical Activity Plan Alliance. The 2018 United States Report Card on Physical Activity for Children and Youth; National Physical Activity Plan Alliance: Washington, DC, USA, 2018. [Google Scholar]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1.6 million participants. Lancet Child. Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Pate, R.R.; Dowda, M.; Dishman, R.K.; Colabianchi, N.; Saunders, R.P.; McIver, K.L. Change in children’s physical activity: Predictors in the transition from elementary to middle school. Am. J. Prev. Med. 2019, 56, e65–e73. [Google Scholar] [CrossRef]
- Rebold, M.J.; Lepp, A.; Kobak, M.S.; McDaniel, J.; Barkley, J.E. The effect of parental involvement on children’s physical activity. J. Pediatr. 2016, 170, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Zecevic, C.A.; Tremblay, L.; Lovsin, T.; Michel, L. Parental influence on young children’s physical activity. Int. J. Pediatr. 2010, 2010, 468526. [Google Scholar] [CrossRef] [PubMed]
- Gapin, J.I.; Etnier, J.L. Parental perceptions of the effects of exercise on behavior in children and adolescents with ADHD. J. Sport Health Sci. 2014, 3, 320–325. [Google Scholar] [CrossRef]
- Solomon-Moore, E.; Toumpakari, Z.; Sebire, S.J.; Thompson, J.L.; Lawlor, D.A.; Jago, R. Roles of mothers and fathers in supporting child physical activity: A cross-sectional mixed-methods study. BMJ Open 2018, 8, e019732. [Google Scholar] [CrossRef]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Ann. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef]
- Burns, R.D.; Bai, Y.; Fu, Y.; Pfledderer, C.D.; Brusseau, T.A. Parent engagement and support, physical activity and academic performance (PESPAAP): A proposed theoretical model. Int. J. Env. Res. Public Health 2019, 16, 4698. [Google Scholar] [CrossRef] [PubMed]
- Brown, H.E.; Atkin, A.J.; Panter, J.; Wong, G.; Chinapaw, M.J.M.; van Sluijs, E.M.F. Family-based interventions to increase physical activity in children: A systematic review, meta-analysis, and realist synthesis. Obes. Rev. 2016, 17, 345–360. [Google Scholar] [CrossRef]
- Burns, R.D. Enjoyment, self-efficacy, and physical activity within parent-adolescent dyads: Application of the Actor-Partner Interdependence Model. Prev. Med. 2019, 126, 105756. [Google Scholar] [CrossRef] [PubMed]
- Davison, K.K.; Cutting, T.M.; Birch, L.L. Parents’ activity-related parenting practices predict girls’ physical activity. Med. Sci. Sports Exerc. 2003, 35, 1589–1595. [Google Scholar] [PubMed]
- Mutz, M.; Albrecht, P. Parents’ social status and children’s daily physical activity: The role of familial socialization and support. J. Child Fam. Stud. 2017, 26, 3026–3035. [Google Scholar] [CrossRef]
- Maher, J.P.; Ra, C.; O’Connor, S.G.; Belcher, B.R.; Leventhal, A.; Margolin, G.; Dunton, G.F. Associations between maternal mental health and well-being and physical activity and sedentary behavior in children. J. Dev. Behav. Pediatr. 2017, 38, 385–394. [Google Scholar] [CrossRef]
- Liu, J.; Probst, J.C.; Harun, N.; Bennett, K.J.; Torres, M.E. Acculturation, physical activity, and obesity among Hispanic adolescents. Ethn. Health 2009, 14, 509–525. [Google Scholar] [CrossRef]
- Muthuri, S.K.; Onywera, V.O.; Tremblay, M.S.; Broyles, S.T.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; et al. Relationships between parental education and overweight with childhood overweight and physical activity in 9-11 year old children: Results from a 12 country study. PLoS ONE 2016, 11, e0147746. [Google Scholar] [CrossRef]
- Min, J.; Xue, H.; Wang, Y. Association between household poverty dynamics and childhood overweight risk and health behaviours in the United States: A 8-year nationally representative longitudinal study of 16 800 children. Pediatr. Obes. 2018, 13, 590–597. [Google Scholar] [CrossRef]
- Langoy, A.; Smith, O.R.F.; Wold, B.; Samdal, O.; Hang, E.M. Associations between family structure and young people’s physical activity and screen time behaviors. BMC Public Health 2019, 19, 433. [Google Scholar] [CrossRef]
- Walsh, F. Family resilience: A developmental systems framework. Eur. J. Dev. Psychol. 2016, 13, 313–324. [Google Scholar] [CrossRef]
- Bethell, C.D.; Gombojav, N.; Whitaker, R.C. Family resilience and connection promote flourishing among US children, even amid adversity. Health Aff. 2019, 38, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, M.I.; Birnie-Lefcovitch, S.; Ungar, M.T. Pathways between social support, family well-being, quality of parenting, and child resilience: What we know. J. Child. Fam. Stud. 2005, 14, 269–281. [Google Scholar] [CrossRef]
- Jeffries, P.; Ungar, M.; Aubertin, P.; Kriellaars, D. Physical literacy and resilience in children and youth. Front. Public Health 2019, 7, 346. [Google Scholar] [CrossRef] [PubMed]
- Ho, F.K.; Louie, L.H.; Chow, C.B.; Wong, W.H.; Ip, P. Physical activity improves mental health through resilience in Hong Kong Chinese adolescents. BMC Pediatr. 2015, 15, 48. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Young, M.D.; Barnes, A.T.; Eather, N.; Pollock, E.R.; Lubans, D.R. Engaging father to increase activity in girls: The “Dads and Daughters Exercising and Empowered (DADEE) Randomized Controlled Trial. Ann. Behav. Med. 2019, 53, 39–52. [Google Scholar] [CrossRef]
- Beets, M.W.; Cardinal, B.J.; Alderman, B.L. Parental social support and the physical activity-related behaviors of youth: A review. Health Educ. Behav. 2010, 37, 621–644. [Google Scholar] [CrossRef]
- Child and Adolescent Health Measurement Initiative (CAHMI) (2019). 2017–2018 National Survey of Children’s Health (2 Years Combined Data Set): Child and Family Health Measures, National Performance and Outcome Measures, and Subgroups, STATA Codebook, Version 1.0, Data Resource Center for Child and Adolescent Health supported by Cooperative Agreement U59MC27866 from the U.S. Department of Health and Human Services, Health Resources and Services Administration (HRSA), Maternal and Child Health Bureau (MCHB). Available online: https://www.childhealthdata.org (accessed on 2 January 2020).
- Child and Adolescent Health Measurement Initiative. 2018 National Survey of Children’s Health, Sampling and Survey Administration. Data Resource Center for Child and Adolescent Health, Supported by Cooperative Agreement 1-U59-MC06980-01 from the U.S. Department of Health and Human Services, Health Resources and Services Administration (HRSA), Maternal and Child Health Bureau (MCHB). Available online: https//www.childhealthdata.org (accessed on 2 January 2020).
- The United States Census Bureau. Associate Director of Demographic Programs, National Survey of Children’s Health. 2018 National Survey of Children’s Health Frequently Asked Questions. September 2019. Available online: https://www2.census.gov/programs-surveys/nsch/technical-documentation/methodology/2018-NSCH-FAQs.pdf (accessed on 2 January 2020).
- Coyle, J. Resilient families help make resilient children. J. Fam. Strengths 2011, 11, 5. [Google Scholar]
- Jaeschke, L.; Steinbrecher, A.; Luzak, A.; Puggina, A.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Chantal, S.; et al. Socio-cultural determinants of physical activity across the life course: A ‘Determinants of Diet and Physical Activity’ (DEDIPAC) umbrella systematic literature review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 173. [Google Scholar] [CrossRef]
- McMinn, A.M.; Griffin, S.J.; Jones, A.P.; van Sluijs, E.M.F. Family and home influences on children’s after-school and weekend physical activity. Eur. J. Public Health 2013, 23, 805–810. [Google Scholar] [CrossRef]
- Pyper, E.; Harrington, D.; Manson, H. The impact of different types of parental support behaviours on child physical activity, healthy eating, and screen time: A cross-sectional study. BMC Public Health 2016, 16, 568. [Google Scholar] [CrossRef] [PubMed]
- Dowda, M.; Dishman, R.K.; Pfeiffer, K.A.; Pate, R.R. Family support for physical activity in girls from 8th to 12th grade in South Carolina. Prev. Med. 2007, 44, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Dishman, R.K.; Motl, R.W.; Saunders, R.; Felton, G.; Ward, D.S.; Dowda, M.; Pate, R.R. Enjoyment mediates effects of a school-based physical-activity intervention. Med. Sci. Sports Exerc. 2005, 37, 478–487. [Google Scholar] [CrossRef] [PubMed]
- Eather, N.; Morgan, P.J.; Lubans, D.R. Social support from teacher mediates physical activity behavior change in children participating in the Fit-4-Fun intervention. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 68. [Google Scholar] [CrossRef]
- Bentley, G.F.; Goodred, J.K.; Jago, R.; Sebire, S.J.; Lucas, P.J.; Fox, K.R.; Stewart-Brown, S.; Turner, K.M. Parents’ views on child physical activity and their implications for physical activity parenting interventions: A qualitative study. BMC Pediatr. 2012, 12, 180. [Google Scholar] [CrossRef]
- Laird, Y.; Fawkner, S.; Kelly, P.; McNamee, L.; Niven, A. The role of social support on physical activity behavior in adolescent girls: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 79. [Google Scholar] [CrossRef]
- Davison, K.K.; Schmalz, D.L. Youth at risk of physical inactivity may benefit more from activity-related support than youth not at risk. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 5. [Google Scholar] [CrossRef][Green Version]
- Duncan, S.C.; Duncan, T.E.; Strycker, L.A. Sources and type of social support in youth physical activity. Health Psychol. 2005, 24, 3–10. [Google Scholar] [CrossRef]
- Heitzler, C.D.; Martin, S.L.; Duke, J.; Huhman, M. Correlates of physical activity in a national sample of children aged 9–13 years. Prev. Med. 2006, 42, 254–260. [Google Scholar] [CrossRef]
- Prochaska, J.J.; Rodgers, M.W.; Sallis, J.F. Association of parent and peer support with adolescent physical activity. Res. Q Exerc. Sport 2002, 73, 206–210. [Google Scholar] [CrossRef]
- Anselma, M.; Chinapaw, M.J.M.; Altenburg, T.M. Determinants of child health behaviors in a disadvantaged area from a community perspective: A participatory needs assessment. Int. J. Env. Res. Public Health 2018, 15, 644. [Google Scholar] [CrossRef] [PubMed]
- Kantomaa, M.T.; Tammelin, T.H.; Nayha, S.; Taanila, A.N. Adolescents physical activity in relation to family income and parental education. Prev. Med. 2007, 44, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Duncan, S.C.; Strycker, L.A.; Chaumeton, N.R. Personal, family, and peer correlates of general and sport physical activity among African American, Latino, and White Girls. J. Health Dispar. Res. Pr. 2015, 8, 12–28. [Google Scholar]
- Romero, A.J. Low-income neighborhood barriers and resources for adolescents’ physical activity. J. Adolesc. Health 2005, 36, 253–259. [Google Scholar] [CrossRef]
- Gordon-Larsen, P.; Nelson, M.C.; Page, P.; Popkin, B.M. Inequality in the built environment underlies key health disparities in physical activity and obesity. Pediatrics 2006, 177, 417–424. [Google Scholar] [CrossRef]
- Stanley, R.M.; Ridley, K.; Dollman, J. Correlates of children’s time-specific physical activity: A review of the literature. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 50. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Level | Count | Unweighted % | Weighted % |
|---|---|---|---|---|
| Child Physical Activity | Not 60 min/day | 29,213 | 79.0% | 77.4% |
| 60 min/day | 7767 | 21.0% | 22.6% | |
| Family Resilience | 0–1 item | 2474 | 6.7% | 7.4% |
| 2–3 items | 4305 | 11.7% | 12.1% | |
| 4 items | 30,130 | 81.6% | 80.5% | |
| Event Attendance | Rarely/Sometimes | 3762 | 10.2% | 14.6% |
| Usually/Always | 33,141 | 89.8% | 85.4% | |
| Mother’s Health | Poor/Fair/Good | 9498 | 28.7% | 30.9% |
| Very Good/Excellent | 23,584 | 71.3% | 69.1% | |
| Father’s Health | Poor/Fair/Good | 8017 | 28.0% | 28.8% |
| Very Good/Excellent | 20,615 | 72.0% | 71.2% | |
| Generational Status | Born in US | 28,729 | 77.7% | 65.5% |
| Born Outside of US | 8244 | 22.3% | 34.5% | |
| Adult Education | College Degree or Higher | 22,195 | 59.4% | 47.3% |
| Some College | 9063 | 24.3% | 22.3% | |
| High School/GED | 5127 | 13.7% | 19.8% | |
| Less than high school | 1007 | 2.7% | 10.6% | |
| Family Income | 0–99% FPL | 4566 | 12.2% | 20.2% |
| 100–199% FPL | 5884 | 15.7% | 21.7% | |
| 200–399% FPL | 11,248 | 30.8% | 27.1% | |
| 400% FPL or greater | 15,694 | 42.0% | 31.0% | |
| Family Structure | Two Married Parents | 25,744 | 70.3% | 64.7% |
| Two Un-Married Parents | 2239 | 6.1% | 8.0% | |
| Single Parent | 7108 | 19.3% | 21.3% |
| Predictor | Level | Crude OR (95% CI) | Model 1 aOR (95% CI) | Model 2 aOR (95% CI) |
|---|---|---|---|---|
| Family Resilience | 0–1 Items | referent | referent | referent |
| 2–3 items | 1.29†(0.90–1.84) | 1.30 (0.89–1.91) | 1.55 (0.92–2.65) | |
| 4 items | 1.70†(1.23–2.35) | 1.80†(1.28–2.53) | 2.17†(1.35–3.49) | |
| Event Attendance | Rarely/Sometimes | referent | referent | referent |
| Usually/Always | 1.31†(1.14–1.70) | 1.72†(1.29–2.29) | 1.65†(1.18–2.31) | |
| Mother’s Health | Poor/Fair/Good | referent | referent | referent |
| Very Good/Excellent | 1.16†(1.01–1.32) | 1.17 (0.99–1.40) | 1.15 (0.92–1.45) | |
| Father’s Health | Poor/Fair/Good | referent | referent | referent |
| Very Good/Excellent | 1.22†(1.06–1.41) | 1.13 (0.96–1.33) | 1.01 (0.81–1.25) | |
| Generational Status | Born in US | referent | referent | referent |
| Born Outside US | 0.90 (0.82–1.00) | 0.72†(0.60–0.86) | 0.81 (0.62–1.05) | |
| Adult Education | College Degree | referent | referent | referent |
| Some College | 0.93 (0.85–1.02) | 1.11 (0.93–1.32) | 1.24 (0.99–1.49) | |
| High School/GED | 0.79†(0.70–0.90) | 1.11 (0.89–1.39) | 0.95 (0.78–1.16) | |
| Less than high school | 0.57†(0.45–0.72) | 1.06 (0.71–1.61) | 0.87 (0.58–1.32) | |
| Family Income | 0–99% FPL | referent | referent | referent |
| 100–199% FPL | 1.10 (0.86–1.43) | 1.15†(1.00–1.33) | 1.17 (0.98–1.41) | |
| 200–399% FPL | 1.22†(1.05–1.42) | 1.57†(1.29–1.91) | 1.60†(1.24–2.04) | |
| 400% FPL Greater | 1.22†(1.07–1.38) | 1.71†(1.31–2.25) | 1.84†(1.34–2.52) | |
| Family Structure | Two Married Parents | referent | referent | referent |
| Two Un-Married Parents | 1.21 (0.96–1.53) | 1.27 (0.8–1.64) | 1.50 (0.97–2.16) | |
| Single Parent | 1.05 (0.92–1.21) | 0.63 (0.13–2.90) | 0.67 (0.09–4.62) | |
| Grandparent Household | 1.38 (1.06–1.80) | 0.46 (0.17–1.21) | 0.35 (0.08–1.70) | |
| Child Age | 6–11 years old | referent | referent | referent |
| 12–17 years old | 0.55†(0.49–0.62) | 0.63†(0.52–0.78) | ||
| Child Sex | Male | referent | referent | referent |
| Female | 0.68†(0.62–0.76) | 0.56†(0.46–0.65) | ||
| Child BMI Class | Not Overweight/Obese | referent | referent | referent |
| Overweight/Obese | 0.82†(0.75–0.89) | 0.49†(0.39–0.61) | ||
| Child Race/Ethnicity | White/Non-Hispanic | referent | referent | referent |
| Hispanic | 0.85 (0.72–1.01) | 0.90 (0.65–1.23) | ||
| Black, Non-Hispanic | 0.92 (0.78–1.08) | 0.86 (0.62–1.19) | ||
| Other/Multi-racial | 0.81†(0.70–0.94) | 0.90 (0.68–1.20) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burns, R.D.; Colotti, T.E.; Pfledderer, C.D.; Fu, Y.; Bai, Y.; Byun, W. Familial Factors Associating with Youth Physical Activity Using a National Sample. Children 2020, 7, 79. https://doi.org/10.3390/children7070079
Burns RD, Colotti TE, Pfledderer CD, Fu Y, Bai Y, Byun W. Familial Factors Associating with Youth Physical Activity Using a National Sample. Children. 2020; 7(7):79. https://doi.org/10.3390/children7070079
Chicago/Turabian StyleBurns, Ryan D., Taylor E. Colotti, Christopher D. Pfledderer, You Fu, Yang Bai, and Wonwoo Byun. 2020. "Familial Factors Associating with Youth Physical Activity Using a National Sample" Children 7, no. 7: 79. https://doi.org/10.3390/children7070079
APA StyleBurns, R. D., Colotti, T. E., Pfledderer, C. D., Fu, Y., Bai, Y., & Byun, W. (2020). Familial Factors Associating with Youth Physical Activity Using a National Sample. Children, 7(7), 79. https://doi.org/10.3390/children7070079