

Association of Meconium-Stained Amniotic Fluid and Histological Chorioamnionitis with Fetal Inflammatory Response in Preterm Deliveries
 , , , , ,
, , , , ,
Abstract
1. Introduction
1.1. MSAF and Preterm Pregnancies
1.2. MSAF and Intrauterine Inflammation
1.3. Aim of Our Study
2. Methods
2.1. Histopathology
2.2. Perinatal Data
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Perinatal Characteristics
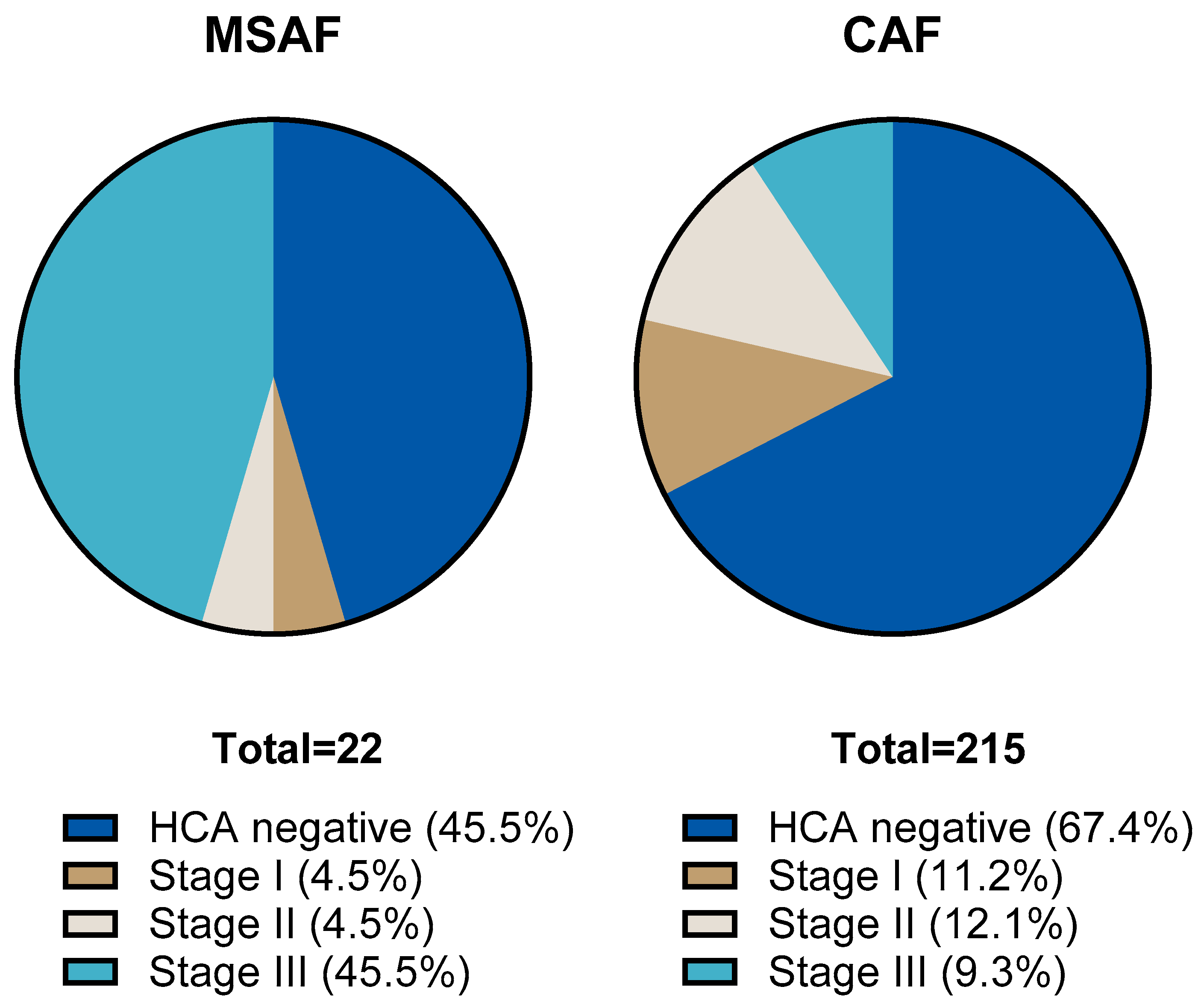
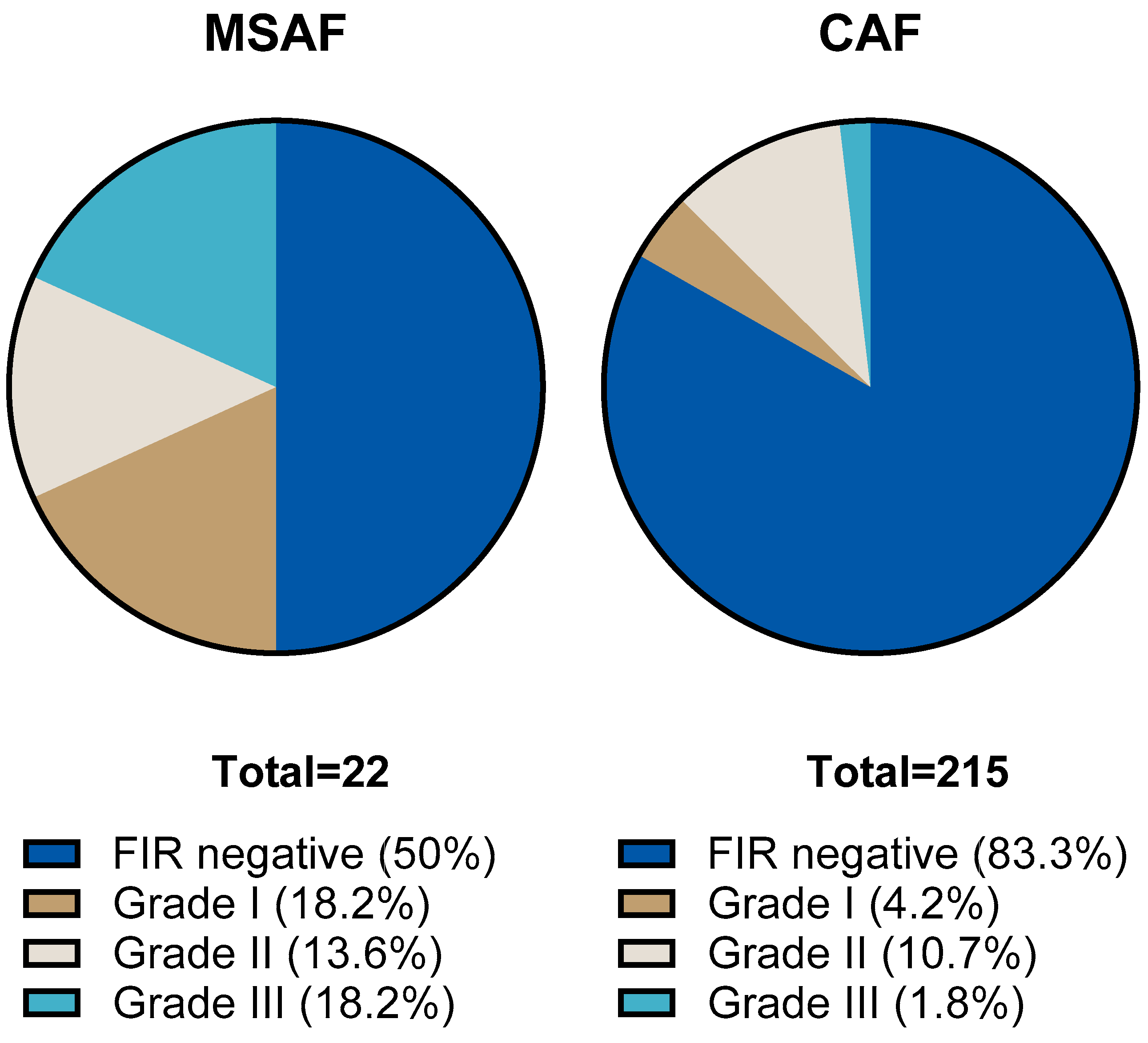
3.2. Histological Findings
3.3. Laboratory Parameters
3.4. Neonatal Outcomes
4. Discussion
4.1. MSAF and the Diagnosis of Chorioamnionitis
4.2. Histological Evaluation
4.3. Laboratory Findings
4.4. Neonatal Outcomes
4.5. Clinical Significance
4.6. Limitations of the Present Study, and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gluck, O.; Kovo, M.; Tairy, D.; Herman, H.G.; Bar, J.; Weiner, E. The effect of meconium thickness level on neonatal outcome. Early Hum. Dev. 2020, 142, 104953. [Google Scholar] [CrossRef] [PubMed]
- Whitfield, J.M.; Charsha, D.S.; Chiruvolu, A. Prevention of meconium aspiration syndrome: An update and the Baylor experience. Bayl. Univ. Med. Cent. Proc. 2009, 22, 128–131. [Google Scholar] [CrossRef]
- Ahanya, S.N.; Lakshmanan, J.; Morgan, B.L.; Ross, M.G. Meconium passage in utero: Mechanisms, consequences, and management. Obs. Gynecol. Surv. 2005, 60, 45–56, quiz 73–44. [Google Scholar] [CrossRef]
- Cohen, G.; Shilony, A.; Amrami, R.B.; Biron-Shental, T.; Kovo, M.; Schreiber, H. The combined impact of meconium stained amniotic fluid and small for gestational age on delivery outcomes. Arch. Gynecol. Obs. 2025. [Google Scholar] [CrossRef]
- Scott, H.; Walker, M.; Gruslin, A. Significance of meconium-stained amniotic fluid in the preterm population. J. Perinatol. Off. J. Calif. Perinat. Assoc. 2001, 21, 174–177. [Google Scholar] [CrossRef]
- Monfredini, C.; Cavallin, F.; Villani, P.E.; Paterlini, G.; Allais, B.; Trevisanuto, D. Meconium Aspiration Syndrome: A Narrative Review. Children 2021, 8, 230. [Google Scholar] [CrossRef]
- Dani, C.; Ciarcia, M.; Barone, V.; Di Tommaso, M.; Mecacci, F.; Pasquini, L.; Pratesi, S. Neonatal Outcomes of Term Infants Born with Meconium-Stained Amniotic Fluid. Children 2023, 10, 780. [Google Scholar] [CrossRef]
- Balchin, I.; Whittaker, J.C.; Lamont, R.F.; Steer, P.J. Maternal and fetal characteristics associated with meconium-stained amniotic fluid. Obstet. Gynecol. 2011, 117, 828–835. [Google Scholar] [CrossRef]
- Gallo, D.M.; Romero, R.; Bosco, M.; Gotsch, F.; Jaiman, S.; Jung, E.; Suksai, M.; López Ramón y Cajal, C.; Yoon, B.H.; Chaiworapongsa, T. Meconium-stained amniotic fluid. Am. J. Obs. Gynecol. 2023, 228 (Suppl. 5), S1158–S1178. [Google Scholar] [CrossRef]
- Tybulewicz, A.T.; Clegg, S.K.; Fonfe, G.J.; Stenson, B.J. Preterm meconium staining of the amniotic fluid: Associated findings and risk of adverse clinical outcome. Arch. Dis. Childhood. Fetal Neonatal Ed. 2004, 89, F328–F330. [Google Scholar] [CrossRef]
- Chen, S.; Wang, X.Q.; Hu, X.Y.; Guo, L.; He, Y.; Wang, Z.L.; Li, L.Q. Meconium-stained amniotic fluid as a risk factor for necrotizing enterocolitis in very low-birth weight preterm infants: A retrospective cohort study. J. Matern. Fetal Neonatal Med. 2020, 33, 4102–4107. [Google Scholar] [CrossRef] [PubMed]
- Spinillo, A.; Fazzi, E.; Capuzzo, E.; Stronati, M.; Piazzi, G.; Ferrari, A. Meconium-stained amniotic fluid and risk for cerebral palsy in preterm infants. Obstet. Gynecol. 1997, 90, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Hanaoka, S.; Mazor, M.; Athanassiadis, A.P.; Callahan, R.; Hsu, Y.C.; Avila, C.; Nores, J.; Jimenez, C. Meconium-stained amniotic fluid: A risk factor for microbial invasion of the amniotic cavity. Am. J. Obs. Gynecol. 1991, 164, 859–862. [Google Scholar] [CrossRef]
- Mazor, M.; Froimovich, M.; Lazer, S.; Maymon, E.; Glezerman, M. Listeria monocytogenes. The role of transabdominal amniocentesis in febrile patients with preterm labor. Arch. Gynecol. Obs. 1992, 252, 109–112. [Google Scholar] [CrossRef]
- Mylonakis, E.; Paliou, M.; Hohmann, E.L.; Calderwood, S.B.; Wing, E.J. Listeriosis during pregnancy: A case series and review of 222 cases. Medicine 2002, 81, 260–269. [Google Scholar] [CrossRef]
- Brabbing-Goldstein, D.; Nir, D.; Cohen, D.; Many, A.; Maslovitz, S. Preterm meconium-stained amniotic fluid is an ominous sign for the development of chorioamnionitis and for in utero cord compression. J. Matern. Fetal Neonatal Med. 2017, 30, 2042–2045. [Google Scholar] [CrossRef]
- Rao, S.; Pavlova, Z.; Incerpi, M.H.; Ramanathan, R. Meconium-stained amniotic fluid and neonatal morbidity in near-term and term deliveries with acute histologic chorioamnionitis and/or funisitis. J. Perinatol. Off. J. Calif. Perinat. Assoc. 2001, 21, 537–540. [Google Scholar] [CrossRef]
- Wertheimer, A.; Shemer, A.; Hadar, E.; Berezowsky, A.; Wiznitzer, A.; Krispin, E. The effect of meconium-stained amniotic fluid on perinatal outcome in pregnancies complicated by preterm premature rupture of membranes. Arch. Gynecol. Obs. 2020, 301, 1181–1187. [Google Scholar] [CrossRef]
- Khong, T.Y.; Mooney, E.E.; Ariel, I.; Balmus, N.C.; Boyd, T.K.; Brundler, M.A.; Derricott, H.; Evans, M.J.; Faye-Petersen, O.M.; Gillan, J.E.; et al. Sampling and Definitions of Placental Lesions: Amsterdam Placental Workshop Group Consensus Statement. Arch. Pathol. Lab. Med. 2016, 140, 698–713. [Google Scholar] [CrossRef]
- Redline, R.W.; Ravishankar, S.; Bagby, C.M.; Saab, S.T.; Zarei, S. Four major patterns of placental injury: A stepwise guide for understanding and implementing the 2016 Amsterdam consensus. Mod. Pathol. 2021, 34, 1074–1092. [Google Scholar] [CrossRef]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef]
- Mazor, M.; Hershkovitz, R.; Bashiri, A.; Maymon, E.; Schreiber, R.; Dukler, D.; Katz, M.; Shoham-Vardi, I. Meconium stained amniotic fluid in preterm delivery is an independent risk factor for perinatal complications. Eur. J. Obstet. Gynecol. Reprod. Biol. 1998, 81, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Attali, E.; Kern, G.; Reicher, L.; Fouks, Y.; Gamzu, R.; Yogev, Y.; Many, A. Early Preterm meconium stained amniotic fluid is an independent risk factor for peripartum maternal bacteremia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 258, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, R.S.; Blanco, J.D.; St Clair, P.J.; Castaneda, Y.S. Quantitative bacteriology of amniotic fluid from women with clinical intraamniotic infection at term. J. Infect. Dis. 1982, 145, 1–8. [Google Scholar] [CrossRef]
- Higgins, R.D.; Saade, G.; Polin, R.A.; Grobman, W.A.; Buhimschi, I.A.; Watterberg, K.; Silver, R.M.; Raju, T.N.K.; Chorioamnionitis Workshop, P. Evaluation and Management of Women and Newborns With a Maternal Diagnosis of Chorioamnionitis: Summary of a Workshop. Obstet. Gynecol. 2016, 127, 426–436. [Google Scholar] [CrossRef]
- Leanos-Miranda, A.; Nolasco-Leanos, A.G.; Carrillo-Juarez, R.I.; Molina-Perez, C.J.; Isordia-Salas, I.; Ramirez-Valenzuela, K.L. Interleukin-6 in Amniotic Fluid: A Reliable Marker for Adverse Outcomes in Women in Preterm Labor and Intact Membranes. Fetal Diagn. Ther. 2021, 48, 313–320. [Google Scholar] [CrossRef]
- Sung, J.H.; Choi, S.J.; Oh, S.Y.; Roh, C.R. Should the diagnostic criteria for suspected clinical chorioamnionitis be changed? J. Matern. Fetal Neonatal Med. 2021, 34, 824–833. [Google Scholar] [CrossRef]
- Faye-Petersen, O.M. The placenta in preterm birth. J. Clin. Pathol. 2008, 61, 1261–1275. [Google Scholar] [CrossRef]
- Markovitch, O.; Mazor, M.; Shoham-Vardi, I.; Chaim, W.; Leiberman, J.R.; Glezerman, M. Meconium stained amniotic fluid is associated with maternal infectious morbidity in pre term delivery. Acta Obs. Gynecol. Scand. 1993, 72, 538–542. [Google Scholar] [CrossRef]
- Yamada, N.; Sato, Y.; Moriguchi-Goto, S.; Yamashita, A.; Kodama, Y.; Sameshima, H.; Asada, Y. Histological severity of fetal inflammation is useful in predicting neonatal outcome. Placenta 2015, 36, 1490–1493. [Google Scholar] [CrossRef]
- Etyang, A.K.; Omuse, G.; Mukaindo, A.M.; Temmerman, M. Maternal inflammatory markers for chorioamnionitis in preterm prelabour rupture of membranes: A systematic review and meta-analysis of diagnostic test accuracy studies. Syst. Rev. 2020, 9, 141. [Google Scholar] [CrossRef] [PubMed]
- Eichberger, J.; Resch, E.; Resch, B. Diagnosis of Neonatal Sepsis: The Role of Inflammatory Markers. Front. Pediatr. 2022, 10, 840288. [Google Scholar] [CrossRef]
- Peng, C.C.; Chang, J.H.; Lin, H.Y.; Cheng, P.J.; Su, B.H. Intrauterine inflammation, infection, or both (Triple I): A new concept for chorioamnionitis. Pediatr. Neonatol. 2018, 59, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Newman, T.B.; Puopolo, K.M.; Wi, S.; Draper, D.; Escobar, G.J. Interpreting complete blood counts soon after birth in newborns at risk for sepsis. Pediatrics 2010, 126, 903–909. [Google Scholar] [CrossRef]
- Jain, V.G.; Willis, K.A.; Jobe, A.; Ambalavanan, N. Chorioamnionitis and neonatal outcomes. Pediatr. Res. 2022, 91, 289–296. [Google Scholar] [CrossRef]
- Thomas, W.; Speer, C.P. Chorioamnionitis: Important risk factor or innocent bystander for neonatal outcome? Neonatology 2011, 99, 177–187. [Google Scholar] [CrossRef]
- Jung, E.; Romero, R.; Yeo, L.; Diaz-Primera, R.; Marin-Concha, J.; Para, R.; Lopez, A.M.; Pacora, P.; Gomez-Lopez, N.; Yoon, B.H.; et al. The fetal inflammatory response syndrome: The origins of a concept, pathophysiology, diagnosis, and obstetrical implications. Semin. Fetal Neonatal Med. 2020, 25, 101146. [Google Scholar] [CrossRef]
- Lee, J.; Romero, R.; Lee, K.A.; Kim, E.N.; Korzeniewski, S.J.; Chaemsaithong, P.; Yoon, B.H. Meconium aspiration syndrome: A role for fetal systemic inflammation. Am. J. Obs. Gynecol. 2016, 214, 366.e1–366.e9. [Google Scholar] [CrossRef]
- Pasquier, J.C.; Claris, O.; Rabilloud, M.; Ecochard, R.; Picaud, J.C.; Moret, S.; Buch, D.; Mellier, G. Intentional early delivery versus expectant management for preterm premature rupture of membranes at 28–32 weeks’ gestation: A multicentre randomized controlled trial (MICADO STUDY). Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 233, 30–37. [Google Scholar] [CrossRef]
- Freeman, S.W.; Denoble, A.; Kuller, J.A.; Ellestad, S.; Dotters-Katz, S. Management of Preterm Premature Rupture of Membranes in the Late Preterm Period. Obs. Gynecol. Surv. 2022, 77, 283–292. [Google Scholar] [CrossRef]
- Sgayer, I.; Naskovica, K.; Abu Shaqara, R.; Odeh, M.; Bornstein, J.; Frank Wolf, M. Early planned labor induction vs expectant management in late preterm pre-labor rupture of membranes: Maternal and neonatal outcomes. Ginekol. Pol. 2021, 92, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Tamayev, L.; Mor, L.; Herman, H.G.; Schreiber, L.; Kovo, M.; Bar, J.; Weiner, E. Placental histology of acute versus continuous meconium exposure—Association with obstetric and neonatal outcomes. Placenta 2021, 103, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Furuta, N.; Yaguchi, C.; Itoh, H.; Morishima, Y.; Tamura, N.; Kato, M.; Uchida, T.; Suzuki, K.; Sugihara, K.; Kawabata, Y.; et al. Immunohistochemical detection of meconium in the fetal membrane, placenta and umbilical cord. Placenta 2012, 33, 24–30. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| MSAF Group n = 22 | CAF Group n = 215 | p | |
|---|---|---|---|
| Survival, % (95% CI) | 86.4 (66.7; 95.3) | 89.3 (84.5; 92.8) | 0.67 |
| Gestational age (weeks), mean (95% CI) | 27.6 (26.4; 28.9) | 28.7 (28.3; 29) | 0.11 |
| Birth weight (g), mean (95% CI) | 1074 (889; 1258) | 1174 (1116; 1231) | 0.29 |
| SGA % (95% CI) | 18.2 (6.7; 39.1) | 13.9 (9.9; 19.2) | 0.59 |
| Partial course of antenatal corticosteroid therapy, % (95% CI) | 91 (72.2; 97.5) | 92.5 (88.2; 95.4) | 0.78 |
| Complete course of antenatal corticosteroid therapy, % (95% CI) any | 54.6 (34.7; 73.1) | 56.1 (49.4; 62.6) | 0.89 |
| PPROM, % (95% CI) | 22.7 (10.1; 43.4) | 18.1 (13.6; 23.8) | 0.6 |
| Female sex, % (95% CI) | 46.5 (40; 53.2) | 36.4 (19.7; 57.1) | 0.36 |
| Multiple births, % (95% CI) | 13.6 (4.8; 33.3) | 31.5 (25.6; 38) | 0.08 |
| Cesarean delivery, % (95% CI) | 77.3 (56.6; 89.9) | 88.3 (83.3; 92) | 0.14 |
| Apgar score at 1 min, median (IQR) | 7 (5; 8) | 9 (8; 9) | 0.1 |
| Apgar score at 5 min, median (IQR) | 8 (7; 8) | 9 (8; 9) | 0.16 |
| MSAF Group n = 22 | CAF Group n = 215 | p | |
|---|---|---|---|
| CA grade I-III, % (95% CI) | 54.5 (34.7; 73.1) | 32.6 (26.6; 39.1) | <0.001 |
| FIR grade I-III, % (95% CI) | 50 (30.1; 69.3) | 16.7 (12.3; 22.3) | <0.001 |
| MVM, % (95% CI) | 50 (30.1; 69.3) | 48.4 (41.8; 55) | 0.88 |
| FVM, % (95% CI) | 27.3 (12.8; 48.4) | 13.5 (9.5; 18.7) | 0.08 |
| MSAF Group n = 22 | CAF Group n = 215 | p | |
|---|---|---|---|
| Maternal WBC (G/l) mean (95% CI) | 15.5 (11.9; 19) | 13.3 (12.64; 13.9) | 0.22 |
| Maternal CRP > 15 mg/L, % (95% CI) | 47.4 (27.3; 68.3) | 34.4 (27.4; 42.1) | 0.27 |
| Maternal CRP > 30 mg/L, % (95% CI) | 36.8 (19.1; 59.1) | 15.3 (10.4; 21.8) | 0.02 |
| Neonatal WBC, mean (95% CI) | 11.8 (6.1; 17.5) | 8.9 (8.0; 9.7) | 0.28 |
| Neonatal CRP > 15 mg/L, % (95 CI%) | 31.8 (16.2; 52.9) | 14.4 (10.3; 19.9) | 0.03 |
| Surviving Infants in the MSAF Group n = 19 | Surviving Infants in the CAF Group n = 192 | p | |
|---|---|---|---|
| Need for surfactant therapy, % (95% CI) | 73.7 (50.9; 88.6) | 58.3 (51.3; 65.1) | 0.19 |
| Need for mechanical ventilation, % (95% CI) | 47.4 (27.3; 68.3) | 29.8 (23.7; 36.7) | 0.11 |
| Need for PDA closure, % (95% CI) | 26.3 (11.5; 49.1) | 17.4 (12.6; 23.4) | 0.12 |
| IVH Papile I-IV st., % (95% CI) | 33.3 (16.1; 56.4) | 29.1 (22.9; 36.3) | 0.71 |
| Severe IVH Papile III-IV st., % (95% CI) | 22.2 (8.5; 45.8) | 5.1 (2.6; 9.6) | 0.006 |
| PVL, % (95% CI) | 11.1 (1.9; 34.1) | 6.3 (3.7; 11.8) | 0.44 |
| NEC Bell I-III st., % (95% CI) | 10.5 (1.7; 32.6) | 13 (8.9; 18.6) | 0.76 |
| NEC Bell III st., % (95% CI) | 0 (0; 14.7) | 0,5 (0; 3.2) | 0.75 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balogh, D.C.; Kovács, K.; Kovács, Ő.Z.; Regős, E.; Fintha, A.; Harmath, Á.; Szabó, M.; Gasparics, Á.; Varga, P. Association of Meconium-Stained Amniotic Fluid and Histological Chorioamnionitis with Fetal Inflammatory Response in Preterm Deliveries. Children 2025, 12, 477. https://doi.org/10.3390/children12040477
Balogh DC, Kovács K, Kovács ŐZ, Regős E, Fintha A, Harmath Á, Szabó M, Gasparics Á, Varga P. Association of Meconium-Stained Amniotic Fluid and Histological Chorioamnionitis with Fetal Inflammatory Response in Preterm Deliveries. Children. 2025; 12(4):477. https://doi.org/10.3390/children12040477
Chicago/Turabian StyleBalogh, Dóra Csenge, Kinga Kovács, Őzike Zsuzsanna Kovács, Eszter Regős, Attila Fintha, Ágnes Harmath, Miklós Szabó, Ákos Gasparics, and Péter Varga. 2025. "Association of Meconium-Stained Amniotic Fluid and Histological Chorioamnionitis with Fetal Inflammatory Response in Preterm Deliveries" Children 12, no. 4: 477. https://doi.org/10.3390/children12040477
APA StyleBalogh, D. C., Kovács, K., Kovács, Ő. Z., Regős, E., Fintha, A., Harmath, Á., Szabó, M., Gasparics, Á., & Varga, P. (2025). Association of Meconium-Stained Amniotic Fluid and Histological Chorioamnionitis with Fetal Inflammatory Response in Preterm Deliveries. Children, 12(4), 477. https://doi.org/10.3390/children12040477