
Fathers’ Experiences of Caring for a Child with a Chronic Illness: A Systematic Review
 , , , , , , , , , , ,
, , , , , , , , , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
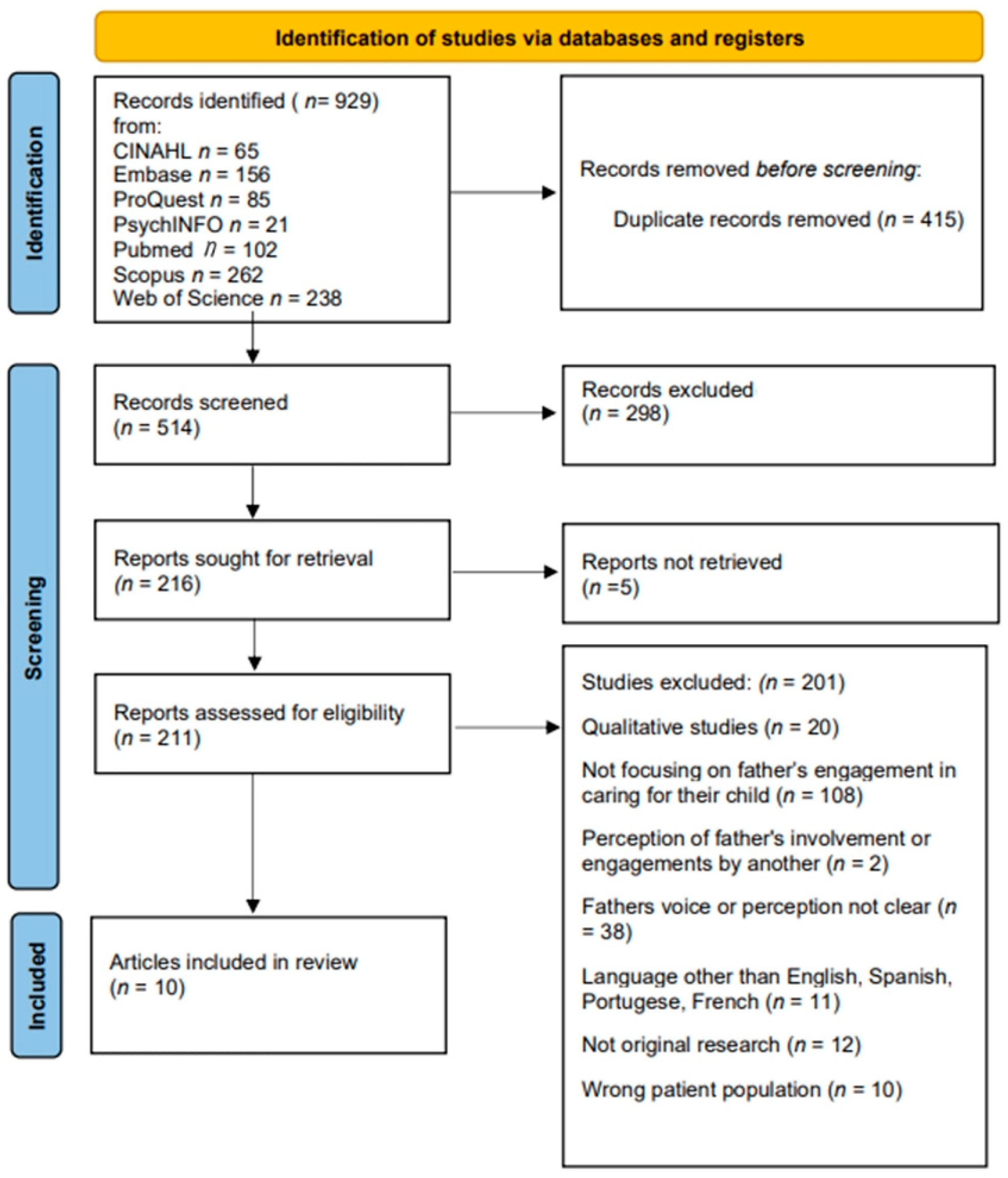
2.1. Design and Search Strategy
2.2. Study Selection
2.3. Quality Assessment
2.4. Review and Extraction
3. Results
3.1. Study Characteristics
3.2. Participant Characteristics
3.3. Areas of Focus
3.3.1. Family Functioning
Fathers’ Role, Relationships, and Communication
Child Characteristics
Mother as Primary Caregiver
3.3.2. Fathers’ Psychological Health
3.3.3. Need for Support
4. Discussion
4.1. Family Functioning
4.2. Father’s Psychological Health
4.3. Need for Support
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Strickland, B.B.; Jones, J.R.; Newacheck, P.W.; Bethell, C.D.; Blumberg, S.J.; Kogan, M.D. Assessing systems quality in a changing health care environment: The 2009-10 national survey of children with special health care needs. Matern. Child Health J. 2015, 19, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Stein, R.E.; Bauman, L.J.; Westbrook, L.E.; Coupey, S.; Ireys, H.T. Framework for identifying children who have chronic conditions: The case for a new definition. J. Pediatr. 1993, 122, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. About Chronic Disease; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2022.
- Mendes, E.V. Interview: The chronic conditions approach by the Unified Health System. Cien. Saude Colet. 2018, 23, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Beacham, B.L.; Deatrick, J.A. Children with Chronic Conditions: Perspectives on Condition Management. J. Pediatr. Nurs. 2015, 30, 25–35. [Google Scholar] [CrossRef]
- Duarte, D.; Silva, K.; Tavares, T.; Jamal, C.; Silva, P.; Rosângela de Sena, R. Care of children with a chronic condition in primary care: Challenges to the healthcare model. Texto Contexto Enferm. 2015, 24, 1009–1017. [Google Scholar] [CrossRef]
- Silva, N.; Pereira, M.; Otto, C.; Ravens-Sieberer, U.; Canavarro, M.C.; Bullinger, M. Do 8- to 18-year-old children/adolescents with chronic physical health conditions have worse health-related quality of life than their healthy peers? a meta-analysis of studies using the KIDSCREEN questionnaires. Qual. Life Res. 2019, 28, 1725–1750. [Google Scholar] [CrossRef]
- Barthel, D.; Ravens-Sieberer, U.; Nolte, S.; Thyen, U.; Klein, M.; Walter, O.; Meyrose, A.-K.; Rose, M.; Otto, C. Predictors of health-related quality of life in chronically ill children and adolescents over time. J. Psychosom. Res. 2018, 109, 63–70. [Google Scholar] [CrossRef]
- Canadian Institute of Child Health (CICH). The Health of Canada’s Children and Youth: A CICH Profile; CICH: Ottawa, ON, Canada, 2018. [Google Scholar]
- Brazilian Institute of Geography and Statistics (IBGE). An Overview of Health in Brazil: Access and Use of Services, Health Conditions and Risk Factors and Health Protection: 2008; IBGE: Rio de Janeiro, Brazil, 2010.
- Australian Bureau of Statistics (ABS). Microdata: National Health Survey 2017–2018. 2019. Available online: https://www.abs.gov.au/statistics/microdata-tablebuilder/available-microdata-tablebuilder/national-health-survey#data-item-lists (accessed on 20 April 2022).
- Cipolletta, S.; Marchesin, V.; Benini, F. Family Functioning as a Constituent Aspect of a Child’s Chronic Illness. J. Pediatr. Nurs. 2015, 30, e19–e28. [Google Scholar] [CrossRef]
- Smith, J.; Cheater, F.; Bekker, H. Parents’ experiences of living with a child with hydrocephalus: A cross-sectional interview-based study. Health Expect. 2015, 18, 1709–1720. [Google Scholar] [CrossRef]
- Tavares, K.O.; Carvalho, M.D.; Pelloso, S.M. What being a mother of a child with cystic fibrosis is like. Rev. Gaucha. Enferm. 2010, 31, 723–729. [Google Scholar] [CrossRef]
- Fairfax, A.; Brehaut, J.; Colman, I.; Sikora, L.; Kazakova, A.; Chakraborty, P.; Potter, B.K.; Canadian Inherited Metabolic Diseases Research Network; in collaboration with the Canadian Inherited Metabolic Diseases Research Network. A systematic review of the association between coping strategies and quality of life among caregivers of children with chronic illness and/or disability. BMC Pediatr. 2019, 19, 215. [Google Scholar] [CrossRef] [PubMed]
- van der Lee, J.H.; Mokkink, L.B.; Grootenhuis, M.A.; Heymans, H.S.; Offringa, M. Definitions and measurement of chronic health conditions in childhood: A systematic review. JAMA 2007, 297, 2741–2751. [Google Scholar] [CrossRef] [PubMed]
- Harrist, A.W.; Henry, C.S.; Liu, C.; Morris, A.S. (Eds.) APA Handbook of Contemporary FAMILY psychology: Foundations, Methods, and Contemporary Issues across the Lifespan American Psychological Association; APA: Washington, DC, USA, 2019. [Google Scholar]
- Marofi, M.; Bahrami, N.; Pahlavanzadeh, S. Effect of a supportive training program on anxiety in children with chronic kidney problems and their mothers’ caregiver Burden. Iran. J. Nurs. Midwifery Res. 2019, 24, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Salvador, M.D.S.; Gomes, G.C.; De Oliveira, P.K.; Busanello, J.; Xavier, D.M. Strategies of Families in the Care of Children with Chronic Diseases. Texto Context.-Enferm. 2015, 24, 662–669. [Google Scholar] [CrossRef]
- Javalkar, K.; Rak, E.; Phillips, A.; Haberman, C.; Ferris, M.; Van Tilburg, M. Predictors of Caregiver Burden among Mothers of Children with Chronic Conditions. Children 2017, 4, 39. [Google Scholar] [CrossRef]
- Katz, L.F.; Fladeboe, K.; King, K.; Gurtovenko, K.; Kawamura, J.; Friedman, D.; Compas, B.; Gruhn, M.; Breiger, D.; Lengua, L.; et al. Trajectories of child and caregiver psychological adjustment in families of children with cancer. Health Psychol. 2018, 37, 725–735. [Google Scholar] [CrossRef]
- Yogman, M.; Garfield, C.F.; Committee on Psychosocial Aspects of Child and Family Health. Fathers’ Roles in the Care and Development of Their Children: The Role of Pediatricians. Pediatrics 2016, 138, e20161128. [Google Scholar] [CrossRef]
- Schoppe-Sullivan, S.J.; Fagan, J. The Evolution of Fathering Research in the 21st Century: Persistent Challenges, New Directions. J. Marriage Fam. 2020, 82, 175–197. [Google Scholar] [CrossRef]
- Khanna, A.K.; Prabhakaran, A.; Patel, P.; Ganjiwale, J.D.; Nimbalkar, S.M. Social, Psychological and Financial Burden on Caregivers of Children with Chronic Illness: A Cross-sectional Study. Indian J. Pediatr. 2015, 82, 1006–1011. [Google Scholar] [CrossRef]
- Aromataris, E.; Munn, Z. Joanna Briggs Institute Manual for Evidence Synthesis. Joanna Briggs Inst. Man. Evid. Synth. 2020. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Bowden, M.R.; Ee, L.C.; Krishnan, U.; O’Loughlin, E.V.; Hardikar, W.; Carmody, D.; Hainsworth, C.; Jermyn, V.; Lee, M.-M.; Sawyer, J.; et al. Family Impact and Infant Emotional Outcomes Following Diagnosis of Serious Liver Disease or Transplantation in Infancy. J. Craniofacial Surg. 2017, 64, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Bowden, M.R.; Stormon, M.; Hardikar, W.; Ee, L.C.; Krishnan, U.; Carmody, D.; Jermyn, V.; Lee, M.M.; O’Loughlin, E.V.; Sawyer, J.; et al. Family adjustment and parenting stress when an infant has serious liver disease: The Australian experience. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.; Masek, B.; Barreto, E.; Baer, L.; Lapey, A.; Budge, E.; McQuaid, E.L. Fathers and Asthma Care: Paternal Involvement, Beliefs, and Management Skills. J. Pediatr. Psychol. 2015, 40, 768–780. [Google Scholar] [CrossRef]
- Gavin, L.; Wysocki, T. Associations of Paternal Involvement in Disease Management with Maternal and Family Outcomes in Families with Children with Chronic Illness. J. Pediatr. Psychol. 2006, 31, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Haugstvedt, A.; Wentzel-Larsen, T.; Rokne, B.; Graue, M. Perceived family burden and emotional distress: Similarities and differences between mothers and fathers of children with type 1 diabetes in a population-based study. Pediatr. Diabetes 2011, 12, 107–114. [Google Scholar] [CrossRef]
- Katz, S.; Krulik, T. Fathers of Children with Chronic Illness: Do They Differ from Fathers of Healthy Children? J. Fam. Nurs. 1999, 5, 292–315. [Google Scholar] [CrossRef]
- Öjmyr-Joelsson, M.; Nisell, M.; Frenckner, B.; Rydelius, P.-A.; Christensson, K. A Gender Perspective on the Extent to which Mothers and Fathers Each Take Responsibility for Care of a Child with High and Intermediate Imperforate Anus. J. Pediatr. Nurs. 2009, 24, 207–215. [Google Scholar] [CrossRef]
- Teasdale, A.; Limbers, C. Avoidant coping moderates the relationship between paternal involvement in the child’s type 1 diabetes (T1D) care and parenting stress. J. Child Health Care 2018, 22, 606–618. [Google Scholar] [CrossRef]
- Wysocki, T.; Gavin, L. Paternal Involvement in the Management of Pediatric Chronic Diseases: Associations with Adherence, Quality of Life, and Health Status. J. Pediatr. Psychol. 2006, 31, 501–511. [Google Scholar] [CrossRef]
- Seiffge-Krenke, I. “Come on, say something, dad!”: Communication and coping in fathers of diabetic adolescents. J. Pediatr. Psychol. 2002, 27, 439–450. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Grimshaw, J. A Knowledge Synthesis Chapter. Canadian Institute of Health Research (CIHR). Available online: https://cihr-irsc.gc.ca/e/documents/knowledge_synthesis_chapter_e.pdf (accessed on 2 May 2022).
- van Nimwegen, K.J.; Kievit, W.; van der Wilt, G.J.; Schieving, J.H.; Willemsen, M.A.; Donders, A.R.; Verhaak, C.M.; Grutters, J.P. Parental quality of life in complex paediatric neurologic disorders of unknown aetiology. Eur. J. Paediatr. Neurol. 2016, 20, 723–731. [Google Scholar] [CrossRef]
- Toledano-Toledano, F.; Moral de la Rubia, J. Factors associated with anxiety in family caregivers of children with chronic diseases. Biopsychosoc. Med. 2018, 12, 20. [Google Scholar] [CrossRef] [PubMed]
- Abrams, H.R.; Leeds, H.S.; Russell, H.V.; Hellsten, M.B. Factors Influencing Family Burden in Pediatric Hematology/Oncology Encounters. J. Patient-Cent. Res. Rev. 2019, 6, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Picardi, A.; Gigantesco, A.; Tarolla, E.; Stoppioni, V.; Cerbo, R.; Cremonte, M.; Alessandri, G.; Lega, I.; Nardocci, F. Parental Burden and its Correlates in Families of Children with Autism Spectrum Disorder: A Multicentre Study with Two Comparison Groups. Clin. Pr. Epidemiol. Ment. Health 2018, 14, 143–176. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, C.; George, S.; Somerville, R.; Linnane, B.; Fitzpatrick, P. Caregiver burden of parents of young children with cystic fibrosis. J. Cyst. Fibros. 2018, 17, 125–131. [Google Scholar] [CrossRef]
- Pinquart, M. Parenting stress in caregivers of children with chronic physical condition-A meta-analysis. Stress Health 2018, 34, 197–207. [Google Scholar] [CrossRef]
- Koch, A.; Kozhumam, A.S.; Seeler, E.; Docherty, S.L.; Brandon, D. Multiple Roles of Parental Caregivers of Children with Complex Life-Threatening Conditions: A Qualitative Descriptive Analysis. J. Pediatr. Nurs. 2021, 61, 67–74. [Google Scholar] [CrossRef]
- Williams, P.D.; Williams, K.A.; Williams, A.R. Parental caregiving of children with cancer and family impact, economic burden: Nursing perspectives. Issues Compr. Pediatr. Nurs. 2014, 37, 39–60. [Google Scholar] [CrossRef]


{kind=link}
| JBI Checklist Questions | Bowden et al., 2017 [27] | Bowden et al., 2015 [28] | Friedman et al., 2015 [29] | Gavin and Wysocki, 2006 [30] | Haugstvedt et al., 2011 [31] | Katz and Krulik, 1999 [32] | Ojmyr-Joelsson et al., 2009 [33] | Teasdale and Limbers, 2018 [34] | Wysocki and Gavin, 2006 [35] |
|---|---|---|---|---|---|---|---|---|---|
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| NA | NA | NA | NA | NA | NA | NA | NA | NA |
| NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| JBI Checklist Questions | Seiffge-Krenke, 2002 [36] |
|---|---|
| No |
| Yes |
| Yes |
| Yes |
| Yes |
| Yes |
| Yes |
| Yes |
| Yes |
| Yes |
| Yes |
| Author(s), Date | Design | Child age and Sex | Diagnosis + Acuity | Country/Region and Community (rural, urban, etc.) | Sample Size of Fathers | Instruments (e.g., DADS) |
|---|---|---|---|---|---|---|
| 1. Bowden et al. (2017) [27] | Cross- Sectional design | 2–700 days; 15 male, 27 female | Infants recently diagnosed with serious liver disease; biliary atresia most common | Australia | 42 families, 37 at follow-up | Family Assessment Device (FAD), Impact on Family Scale (IFS), Depression Anxiety Stress Scale (DASS), Dads’ Active Disease Support scale (DADS), Child Behavior Checklist (CBCL) |
| 2. Bowden et al. (2015) [28] | Cross-sectional design | Infants <2 years (2–700 days); 15 male, 27 female | Serious liver disease (liver disease that may require transplantation in the future) | Four metropolitan children’s hospitals in Australia; Sydney (2), Brisbane (1), Melbourne (1) | 42 two-parent families | FAD, IFS, DASS, DADS |
| 3. Friedman et al. (2015) [29] | Cross-sectional design | 5–9 years; nonspecific sex | Physician-diagnosed asthma requiring daily controller medication | USA | 63 dads, 63 moms | DADS, Beliefs about Medication Questionnaire (BMQ), Family Asthma Management System Scale (FAMSS), TrackCap, Smartinhaler, Asthma Functioning Severity Scale (AFSS), Asthma Control Test (ACT), Pediatric Asthma Caregiver QOL Questionnaire |
| 4. Gavin and Wysocki (2006) [30] | Cross- sectional design | 2–18 years; 94 male, 96 female | 6 chronic illnesses: asthma (at least mild persistent in sensitivity), cystic fibrosis, type 1 diabetes, phenylketonuria (PKU), inflammatory bowel disease, spina bifida | USA | n = 190 hetero-sexual couples | Demographics, DADS, FAD, IFS, Dyadic Adjustment Scale (DAS), Only Maternal perception—Parenting Stress Index brief form, Brief symptom Inventory (BSI)-not included in SR |
| 5. Haugstvedt et al. (2011) [31] | Cross-sectional design | Mean age 10.6 y (SD 3.6, range 1.6–15.9), mean age at diagnosis 6.7 y (SD 3.5, range 1.1–14.3), mean duration of diabetes 3.9 y (SD 2.9, range 0.3–14.2) | Type 1 diabetes | Norway, Hordaland County | 97 fathers | The fathers completed the Hopkins Symptom Checklist-25 items (HSCL-25), measuring emotional distress, and the Family Burden Scale, which includes five questions measuring perceived family burden related to the child’s diabetes. Information collected from the fathers included routines for blood glucose measurements, hypoglycemic events, and comorbid somatic diseases. These included the frequency of perceived problematic hypoglycemic episodes during the past year, experience with nocturnal hypoglycemia at least once, and experience with hypoglycemia with unconsciousness at least once and the number of blood glucose measurements per day. |
| 6. Katz and Krulik (1999) [32] | Cross-sectional design | 6 months-7 years; chronic illness 44 male, 36 female; healthy 40 male, 40 female | Diagnosed as suffering from a chronic illness (≥6 months), receiving daily medical treatment at home (cancer, nephrological diseases, diabetes, asthma, and juvenile rheumatoid arthritis) | Israel | 160 dads (80 of children with chronic illness; 80 of “healthy children”) | Sociodemographic and illness-related questionnaire, shortened version of the Social Readjustment Rating Scale (SRRS), Self-esteem scale, Social Support Questionnaire, Marital Adjustment Test, Father’s involvement in the care of the child |
| 7. Öjmyr-Joelsson et al. (2009) [33] | Cross-sectional design | 8–13 years; 9 male, 16 female | Imperforate anus | Stockholm, Sweden | 20 dads, 25 moms | Study-specific questionnaire, Swedish version of the CBCL |
| 8. Seiffge-Krenke (2002) [36] | Cohort study design | Mean age 13.9 y; diabetic 47 female, 53 male; nondiabetic 56 female, 44 male | Diabetes | Germany | 133 dads [75 fathers of healthy FHA adolescents + 58 fathers of diabetics FDA adolescents]. Drop-out rates were low with FDA 17% and FHA at 13%. | F-Copes, Family Environment Scale (FES), Family Interaction Task (FIT), transcripts of family conversations |
| 9. Teasdale and LImbers (2018) [34] | Cross-sectional design | 2–10 years, nonspecific sex | Type 1 diabetes | International (USA, India, Canada, Italy, UK, Venezuela, and other countries with only 1 or 2 participants) | 249 dads | Parenting Stress Index (PSI), Pediatric Inventory for Parents (PIP), DADS, COPE Inventory, Self-Care Inventory (SCI-R) |
| 10. Wysocki and Gavin (2006) [35] | Cross-sectional study | 2–18 years; 94 male, 96 female | 6 conditions: asthma (at least mild persistent in sensitivity), cystic fibrosis, type 1 diabetes, PKU, inflammatory bowel disease, spina bifida | USA | 190 hetero-sexual couples | Demographics, DADS, disease-specific structured interview to assess medical treatment adherence (based off Diabetes Self-Management Profile), PedsQOL, subjective health status index from child’s primary healthcare provider, healthcare utilization |
| Author/s | Outcomes |
|---|---|
| 1. Bowden et al. (2017) [27] |
|
| 2. Bowden et al. (2015) [28] |
|
| 3. Friedman et al. (2015) [29] |
|
| 4. Gavin and Wysocki (2006) [30] |
|
| 5. Haugstvedt et al. (2011) [31] |
|
| 6. Katz and Krulik (1999) [32] |
|
| 7. Öjmyr-Joelsson et al. (2009) [33] |
|
| 8. Seiffge-Krenke (2002) [36] |
|
| 9. Teasdale and Limbers (2018) [34] |
|
| 10. Wysocki and Gavin (2006) [35] |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spurr, S.; Danford, C.A.; Roberts, K.J.; Sheppard-LeMoine, D.; Machado Silva-Rodrigues, F.; Darezzo Rodrigues Nunes, M.; Darmofal, L.; Ersig, A.L.; Foster, M.; Giambra, B.; et al. Fathers’ Experiences of Caring for a Child with a Chronic Illness: A Systematic Review. Children 2023, 10, 197. https://doi.org/10.3390/children10020197
Spurr S, Danford CA, Roberts KJ, Sheppard-LeMoine D, Machado Silva-Rodrigues F, Darezzo Rodrigues Nunes M, Darmofal L, Ersig AL, Foster M, Giambra B, et al. Fathers’ Experiences of Caring for a Child with a Chronic Illness: A Systematic Review. Children. 2023; 10(2):197. https://doi.org/10.3390/children10020197
Chicago/Turabian StyleSpurr, Shelley, Cynthia A. Danford, Karyn J. Roberts, Debbie Sheppard-LeMoine, Fernanda Machado Silva-Rodrigues, Michelle Darezzo Rodrigues Nunes, Leslie Darmofal, Anne L. Ersig, Mandie Foster, Barbara Giambra, and et al. 2023. "Fathers’ Experiences of Caring for a Child with a Chronic Illness: A Systematic Review" Children 10, no. 2: 197. https://doi.org/10.3390/children10020197
APA StyleSpurr, S., Danford, C. A., Roberts, K. J., Sheppard-LeMoine, D., Machado Silva-Rodrigues, F., Darezzo Rodrigues Nunes, M., Darmofal, L., Ersig, A. L., Foster, M., Giambra, B., Lerret, S., Polfuss, M., Smith, L., & Somanadhan, S. (2023). Fathers’ Experiences of Caring for a Child with a Chronic Illness: A Systematic Review. Children, 10(2), 197. https://doi.org/10.3390/children10020197