Abstract
Introduction: Preterm birth is the leading cause of perinatal mortality worldwide, with prevalence rates showing little reduction. Although mortality rates have decreased, morbidity rates remain concerningly high. In recent years, there has been a surge in studies examining the etiology, risk factors, and management of preterm birth. The use of vaginal probiotics in pregnant women at risk of preterm birth has garnered attention as a potential approach for improving perinatal outcomes and modulating the vaginal microbiota. However, the efficacy of this intervention remains unclear. Therefore, this study explored the impact of vaginal probiotics on perinatal outcomes and vaginal microbiota composition in pregnant women at risk of preterm birth. Materials and Methods: This was a randomized, prospective, longitudinal, double-blind, placebo-controlled, multicentric trial conducted across seven maternities in Spain from October 2017 to August 2022 in pregnant women at risk of preterm birth. Participants were randomly assigned to receive vaginal probiotics containing four lactobacilli strains or a placebo. The primary outcome was to explore a potential correlation between probiotic use among pregnant women at risk of preterm birth and the actual rate of preterm birth before 37 gestational weeks. Secondary outcomes included an evaluation of preterm birth rates, neonatal morbidity, the vaginal microbiota, and changes in the vaginal microbiota after receiving probiotics. Other secondary outcomes were identifying vaginal microbiota patterns associated with preterm birth and exploring potential therapeutic mechanisms involving probiotics. Trial registration: Clinicaltrials.gov, identifier: NCT03689166. Results: A total of 200 participants were included. Of those, birth data were obtained for 181 women. Demographics were similar between both groups. An analysis of perinatal outcomes found no significant differences in preterm birth rates, prematurity rates, gestational weeks at delivery, neonatal complications, time to birth, or latency time to delivery. Microbiota analysis showed no significant differences in vaginal microbiota changes between groups. No serious or unexpected adverse reactions were reported. Conclusions: There were no statistically significant differences for spontaneous preterm birth between pregnant women receiving probiotics and pregnant women receiving the placebo.
1. Introduction
Preterm birth (PTB) is the leading cause of neonatal death (within the first 28 days of life) and accounts for 27% of neonatal deaths worldwide [1,2]. The risk of neonatal death decreases as gestational age increases, but according to a non-linear relationship. In addition, PTB has severe consequences for preterm neonates, including increased morbidity and a greater rate of long-term consequences, such as impaired psychomotor development and increased risk of chronic diseases in adulthood [3]. The global rate of PTB is estimated to be approximately 11% (fluctuating by 5% in some European countries and 18% in some African countries) [4,5].
Approximately 70% of preterm births are spontaneous, either due to a risk of preterm birth (45%) or due to the premature rupture of membranes (25%); the remaining cases (30%) are a result of maternal or fetal conditions, such as multiple gestations, preeclampsia, antepartum hemorrhage, and fetal growth restriction [6].
Progress in recent years has allowed for an increase in the survival rate of neonates with very low birth weights. However, prematurity rates have not changed significantly [7], and increased survival is associated with many respiratory, visual, auditory, neurological, and cognitive complications, as well as certain psychosocial behaviors [8].
For this reason, recent trends have involved identifying PTB risk factors and developing prevention strategies.
Several studies have revealed the importance of vaginal microbiota composition in determining a healthy reproductive tract [9,10,11]. The vaginal microbiota is often categorized into five distinct community state types (CSTs), which reflect the predominance of a particular bacterium within the vagina. CSTs I, II, III, and V are defined by the dominance of Lactobacillus crispatus, L. gasseri, L. iners, and L. jensenii, respectively. By contrast, CST IV presents a highly diverse microbial composition, where no single bacterium is dominant. This community usually comprises various anaerobic species belonging to the genera of Gardnerella, Prevotella, Fannyhessea, Mobiluncus, Annaerococcus, and Sneathia. CSTs with an overall dominance of Lactobacillus species have been typically associated with healthy states. In contrast, non-Lactobacillus microbiomes are often linked to high levels of pro-inflammatory cytokines and adverse health outcomes, including spontaneous preterm birth (sPTB) [12,13,14,15]. However, CST III characterized by L. iners dominance has also been associated with a higher risk of sPTB, whereas L. crispatus dominance was found to have a protective effect [16,17,18].
One potentially new way to protect against PTB-mediated infection is using probiotic bacteria, particularly Lactobacillus. Probiotics, defined as living microorganisms that, in suitable amounts, benefit the health of the host, are being studied for their ability to replenish vaginal Lactobacillus and modulate immunity.
Several studies have determined the effectiveness of Lactobacillus spp. when dealing with vaginal pathogens such as Gardnerella vaginalis and other microorganisms involved in bacterial vaginosis [19,20,21,22].
Many strains of Lactobacillus have been evaluated, including L. gasseri, L. acidophilus, L. reuteri, L. rhamnosus, L. paracasei, L. plantarum, and so on [19,20,21,22,23,24,25,26,27], either separately or combined. Several strains of Lactobacillus given to women with bacterial vaginosis can reduce symptoms effectively, even when given as a single treatment [28], as well as decrease recurrence with adjuvant antibiotic treatment [29,30,31]. In addition, using probiotics during pregnancy and breastfeeding has been described by several authors as being a safe and effective method for improving the potential immunoprotective role of breast milk and preventing atopic eczema in the neonate [32,33].
Despite the growing interest in the role of the vaginal microbiota in pregnancy outcomes, there is a lack of randomized clinical trials specifically assessing the impact of vaginal probiotic administration in women with a threatened preterm labor episode. Most existing studies have focused on asymptomatic populations or earlier stages of gestation. Therefore, this study aims to address this gap by evaluating whether vaginal probiotics can modify the vaginal microbiota and reduce the incidence of spontaneous preterm birth in a high-risk, symptomatic population.
We hypothesized that vaginal administration of a four-strain probiotic in women with threatened preterm labor would reduce the risk of spontaneous preterm birth through the modulation of the vaginal microbiota.
The aim of this study was to determine whether the use of probiotics in patients at risk of spontaneous PTB reduces the rates of PTB before 37 weeks of gestation due to changes in the vaginal microbiota. This will also help us understand the pathophysiology of spontaneous PTB and the mechanisms regulating the vaginal microbiota in pregnant women.
The secondary study hypothesis was that pregnant women at risk of PTB will exhibit a distinct vaginal microbiota compared to pregnant women without a risk of PTB. Additionally, this study hypothesized that using probiotics will alter the vaginal microbiota of pregnant women at risk of PTB. Furthermore, it was expected that the incidence of PTB before 37 weeks of gestation in pregnant women at risk of PTB may decrease by at least 30% following the probiotic intervention.
This study focuses on the use of probiotics as a preventive strategy during the current pregnancy in women at high risk of preterm birth, with the aim of reducing adverse perinatal outcomes associated with this pregnancy, rather than as a long-term intervention strategy for future gestations.
2. Material and Methods
2.1. Study Design and Participants
This randomized, prospective, longitudinal, double-blind, placebo-controlled, multi-center trial was conducted at seven maternity hospitals across Spain between October 2017 and August 2022 (Hospital Universitari Vall d’Hebron, Hospital Universitari Sant Joan de Reus, Hospital de la Santa Creu i Sant Pau, Hospital Quirón Salud de Barcelona, Hospital Universitari Dexeus, Hospital Universitari Germans Trias i Pujol, and Hospital Universitari Joan XXIII de Tarragona).
Inclusion criteria at randomization were as follows: maternal age of 18 years or older; singleton gestation with a threatened preterm labor episode, defined as ≥4 regular uterine contractions in 30 min, which were confirmed both clinically and via cardiotocography, and associated with a cervical length ≤ 25 mm between 24 and 29 weeks of gestation and ≤15 mm between 30 and 34 weeks of gestation, as well as cervical dilation ≤ 2 cm; and a sonographically normal fetal morphology.
Exclusion criteria were as follow: multiple gestations, clinical chorioamnionitis (diagnosed according to Gibbs’ criteria), and cervical dilation > 2 cm.
2.2. Sample Size
For a significance level of 5%, the number of patients to be included to demonstrate a 30% reduction in the rate of PL < 37 weeks (50% of cases) is 103 cases in every group, with 80% power. This reduction was selected based on the anticipated proportion and the sample size appropriate for our hospital. A total of 103 patients were included in each follow-up group; patients were randomly assigned according to the inclusion and exclusion criteria outlined in the previous section, with a 1:1 ratio, forming two groups: one receiving a placebo (control group) and the other receiving probiotics (treatment group).
2.3. Procedures, Randomization, and Masking
Standard management of women at risk of PTB included hospitalization due to tocolytic treatment and fetal lung maturation. Vaginal, endocervical, urinary, and vagino-rectal SGB cultures, as well as occasional amniocentesis (according to each hospital’s protocol), were performed to exclude subclinical chorioamnionitis.
After considering the inclusion and exclusion criteria, a total of 103 patients were randomized according to a 1:1 ratio into two groups: an intervention group (group A) receiving probiotics and a control group (group B) receiving the placebo.
Randomization was performed using a random number list (RNL) generated by the Statistics Unit of Vall d’Hebron Research Institute (VHIR) and stored in an electronic notebook. The clinicians overseeing this study were blinded to the list details.
The placebo group functioned as the negative control, given that there is currently no established or approved probiotic treatment for the prevention of preterm birth. Therefore, a positive control group was not applicable in this study design.
The probiotic intervention consisted of a combination of 4 Lactobacillus strains (Lactobacillus crispatus LBV88, Lactobacillus rhamnosus LBV96, Lactobacillus jensenii LBV116, and Lactobacillus gasseri LBV150) with fructooligosaccharides in a capsule. The placebo consisted of maltodextrin (244 mg), a vegetable capsule (75 mg), and optionally magnesium stearate and silicon dioxide (6 mg) for a total capsule weight of 325 mg. Both the placebo and the probiotic capsules had an identical appearance. Treatment was administered vaginally.
Once the group had been assigned, the patients started the intervention with two vaginal capsules of the probiotic or placebo until 36.6 weeks of gestation. The maximum treatment duration was from 24.0 to 36.6 weeks of gestation, and the minimum treatment duration was from 34.6 to 36.6 weeks of gestation. Upon admission, treatment with vaginal progesterone was initiated, or a pessary was placed according to each hospital’s protocol.
Vaginal microbiota samples were collected from 60 patients from a subset of participants recruited at Vall d’Hebron Hospital, as part of a pre-specified microbiome sub-study. All participants were randomized based on the strict inclusion and exclusion criteria described above. The selection of this subgroup was based on logistical feasibility and laboratory availability for microbiome analysis at this center.
Both groups underwent the same follow-up protocol at each site: monthly visits until delivery or until 37 weeks of gestation. An abdominal ultrasound to assess fetal biometrics and a transvaginal ultrasound to assess cervical length were performed at each visit. Additionally, at Hospital Vall d’Hebron, a new analysis of the vaginal microbiota was performed one month after the start of the intervention.
Given that both groups underwent the same follow-up procedures and received capsules identical in appearance and administration schedule, the comparison between the groups under equivalent conditions provides a valid assessment of the effect (or lack thereof) of the probiotic intervention.
2.4. Outcomes
The primary outcome was to explore a potential correlation between the use of probiotics in pregnant women at risk of PTB and the actual PTB rate before 37 weeks of gestation. The secondary outcomes were to assess the rate of PTB < 28, 30, 32, and 34 weeks of gestation in both groups; to assess neonatal morbidity; to analyze the vaginal microbiota of pregnant women at risk of PTB; to assess changes in the vaginal microbiota after using probiotics; to identify vaginal microbiota patterns related to PTB; and to investigate a potential therapeutic mechanism involving probiotics for reducing the risk of PTB.
2.5. Statistical Analysis
Data were analyzed using the statistical package IBM SPSS Statistics, version 27.0 for Windows 19.0.
The efficacy analysis was conducted using an intention-to-treat approach. Patients in the study group were randomly assigned to one of the two intervention groups.
Secondly, re-sampling using the bootstrap method in which preterm births were randomly assigned in the same proportion as in the whole study population was performed. Average differences between the groups were calculated.
A descriptive analysis was conducted for the entire study population and for those who reached birth. For the entire study population, given that it was a randomized clinical trial and following the CONSORT guidelines [34], a hypothesis test was not conducted on baseline data because, by definition, both groups were equivalent except for the intervention. Therefore, any observed differences in descriptive measurements in the general criteria were attributed to the randomization procedure.
When comparing groups in terms of reaching birth and gestational age at birth, statistical hypotheses were assessed using the Chi-squared test or the Fisher test for qualitative variables and the Mann–Whitney U test for quantitative variables.
Birth and post-partum data were also collected. The results of all analyses were evaluated considering a type I error level set at 0.05. p-values are reported with four decimal places.
In the descriptive analysis, qualitative variables are expressed as the absolute number of cases and percentage in each category. Quantitative variables are expressed as the mean (standard deviation), the median (interquartile range), and the minimum and maximum.
Ethics Statement: The protocol was approved by the local Ethics Committee of each participating hospital (registration number: PR(AMI)359/2014 and date of issue: 1 December 2014). The study protocol was registered in Clinicaltrials.gov on 11 February 2018 (Identifier: NCT03689166 and URL address: https://clinicaltrials.gov/study/NCT03689166 (accessed on 16 September 2022)) [35]. All participants provided their written informed consent.
2.6. DNA Extraction and 16S rRNA Sequencing
Cervicovaginal swabs were collected in Deltalab tubes during a speculum examination (Deltalab Amies; Copan Italia, LQ Amines) and stored at −80 °C until they were processed. Before DNA extraction, the liquid content of the swab was transferred into a 2 mL tube with a screw tap and centrifuged at the maximum speed (18.213× g) for 15 min. After centrifugation, the supernatant was removed using a 200 μL pipette, and the remaining pellet in combination with the original swab was kept for further processing following the recommendations of the International Human Microbiome Standards [36] and as previously described [37,38]. The integrity and quality of the DNA were assessed using a NanoDrop ND-1000 spectrophotometer (Nucliber, Madrid, Spain) and a 1% agarose gel.
For profiling the microbial composition, genomic DNA was used to amplify the V4 region of the 16SrRNA gene using polymerase chain reaction (PCR). Sequences of the primers used for targeting the region were as follows: 5′-{AATGATACGGCGACCACCGAGATCTACACTATGGTAATTGT}{GTGCCAGCMGCCGCGGTAA}-3′ and 5′-{CAAGCA GAAGACGGCATACGAGAT} {Golay barcode}{AGTCAGTCAGCC} {GGACTACHVGGGTWTCTAAT}-3′ [38,39]. Amplicons were then purified using the QIAquick PCR Purification Kit (Qiagen, Barcelona, Spain) and pooled in equal concentrations. Pooled amplicons were purified a second time using HighPrepTM PCR magnetic beads (Magbio, Genomics Inc., Rockville, MD, USA) and sent to the Illumina MiSeq platform (UAB, Spain) for sequencing following the standard Illumina protocols [15]. Additionally, for microbial load determination, the V4 region of the 16S rRNA gene was amplified using real-time quantitative PCR (qPCR) following a previously described method [40].
2.7. Microbiota Analysis
At Vall d’Hebron Hospital, vaginal samples were collected to analyze the microbial composition from a selected group of 55 patients at randomization. Samples were collected from both groups at baseline and four weeks after starting the intervention.
The 16S rRNA raw sequence data were preprocessed using the QIIME2 (v.2020.2.0) bioinformatics pipeline [41]. The sequence reads were denoised, filtered out from chimeras, and de-replicated into amplicon sequence variants (ASVs) using the DADA2 tool, version 2020.2.0 [42]. Each ASV was taxonomically assigned to the species level using the QIIME2 naive-bayes feature classifier with GSR-DB 16S as the reference database [43]. The range of the n-gram parameter was set to [7], and the confidence threshold was set to “disable”.
Community state types (CSTs) were assigned to each sample based on the taxon with the largest abundance as previously described.
The multivariable association with linear models (MaAslin2, v.1.12.0) [44], ANCOM-BC2 (v. 2.0.2) [45], and the Wilcoxon signed-rank test were used to assess the differences in abundance between microbiota data and clinical variables. The use of different methodologies is highly recommended to increase the robustness of the results [46]. The following parameters were used to set up MaAslin2: normalization = 9“TSS”, transform = “LOG”, analysis_method = “LM”, standardize = “TRUE”, max_significance = 0.05, min_abundance = 0.0001, and min_prevalence = 0.1. ANCOM-BC2 was used with the following parameters: p_adj_method = “holm”, prv_ct = 0, struct_zero = “TRUE”, neg_lb = “TRUE”, alpha = 0.05, dunnet = “TRUE”, and trend = “TRUE”. Unlike MaAsLin2, in ANCOM-BC2, we did not include any filtering (prv_ct = 0) in order to identify potential structural zeros. Intervention with probiotics, the time point, and sPTB were included as fixed effects. Subject identification was added as a random effect.
Differences in microbial load and alpha diversity among groups were assessed using the non-parametric Wilcoxon signed-rank test (paired comparison). Alpha diversity indexes (Chao1, Shannon, and Simpson) were calculated using the vegan package (v. 2.6-4) in R [47]. The PERMANOVA test was used to analyze the associations between the microbial composition (beta diversity) and host factors using the adonis2 function of the vegan package with the following settings: setting permutation = 10,000, by = “terms”, and seed = 123. Beta diversities were calculated using Bray–Curtis dissimilarities between samples (calculated with the vegan package) and visualized using principal component analysis (PCA) ordinations.
Bacterial species were not removed from the analysis through cleaning processes. Additionally, no environmental controls or mock communities were used as controls for the microbiota analyses.
3. Results
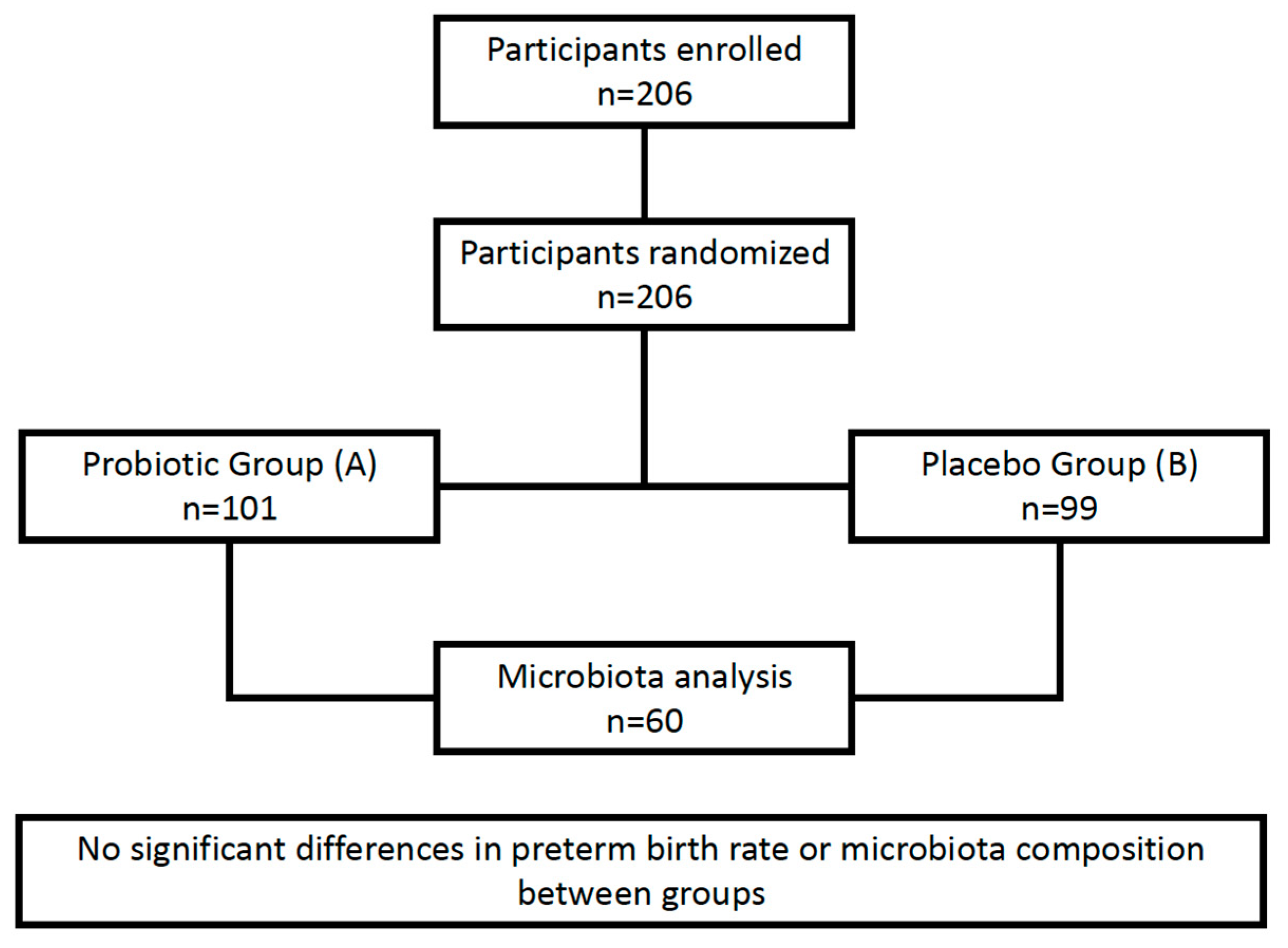
During the recruitment period, 271 patients were assessed for eligibility, of whom 65 were excluded, mainly due to cervical dilation > 2 cm, multiple gestation, or clinical signs of chorioamnionitis. A total of 200 participants were recruited: 101 women (50.50%) were assigned to the intervention group (group A), and 99 (49.50%) were assigned to the placebo group (group B). Delivery data were available for 181 participants: 91 (50.28%) in group A and 90 (49.72%) in group B. Nineteen participants were lost during the follow-up period. The main reasons were loss of contact or delivery at a different hospital (Chart 1).

Chart 1.
Flowchart of the PROPEV trial, illustrating the study design and participant progression through the trial phases.
The demographic characteristics of all patients are shown in Table 1.

Table 1.
Patient demographics.
Although no statistically significant differences were observed for the primary outcome of preterm birth < 37 weeks, a trend toward a lower rate of preterm birth < 34 weeks was noted in the placebo group (17.8% vs. 9.0%, p = 0.0844), and a statistically significant difference was observed for preterm birth < 32 weeks (12.2% vs. 3.3%, p = 0.0260). However, these results should be interpreted with caution, as multiple comparisons were performed across various gestational age thresholds. After applying Bonferroni correction, the p-values did not retain statistical significance. Therefore, these findings may reflect chance variation rather than a true effect of the intervention and should be considered exploratory. Further studies with larger sample sizes are needed to confirm whether these trends are clinically meaningful (Table 2).
Table 2.
Distribution of characteristics at hospital discharge after birth.
The composite outcome was defined as spontaneous premature births before 37 weeks of gestation, cases with a low birth weight, or the presence of any other neonatal complication (neonatal death, admission to NICU, hyaline membrane, cerebral hemorrhage, prenatal sepsis, or necrotizing enterocolitis). The distribution of neonatal morbidities was similar across both groups, and no statistically significant differences were observed between both groups (Table 3).
Table 3.
Distribution of neonatal morbidity. (NICU, neonatal intensive care unit).
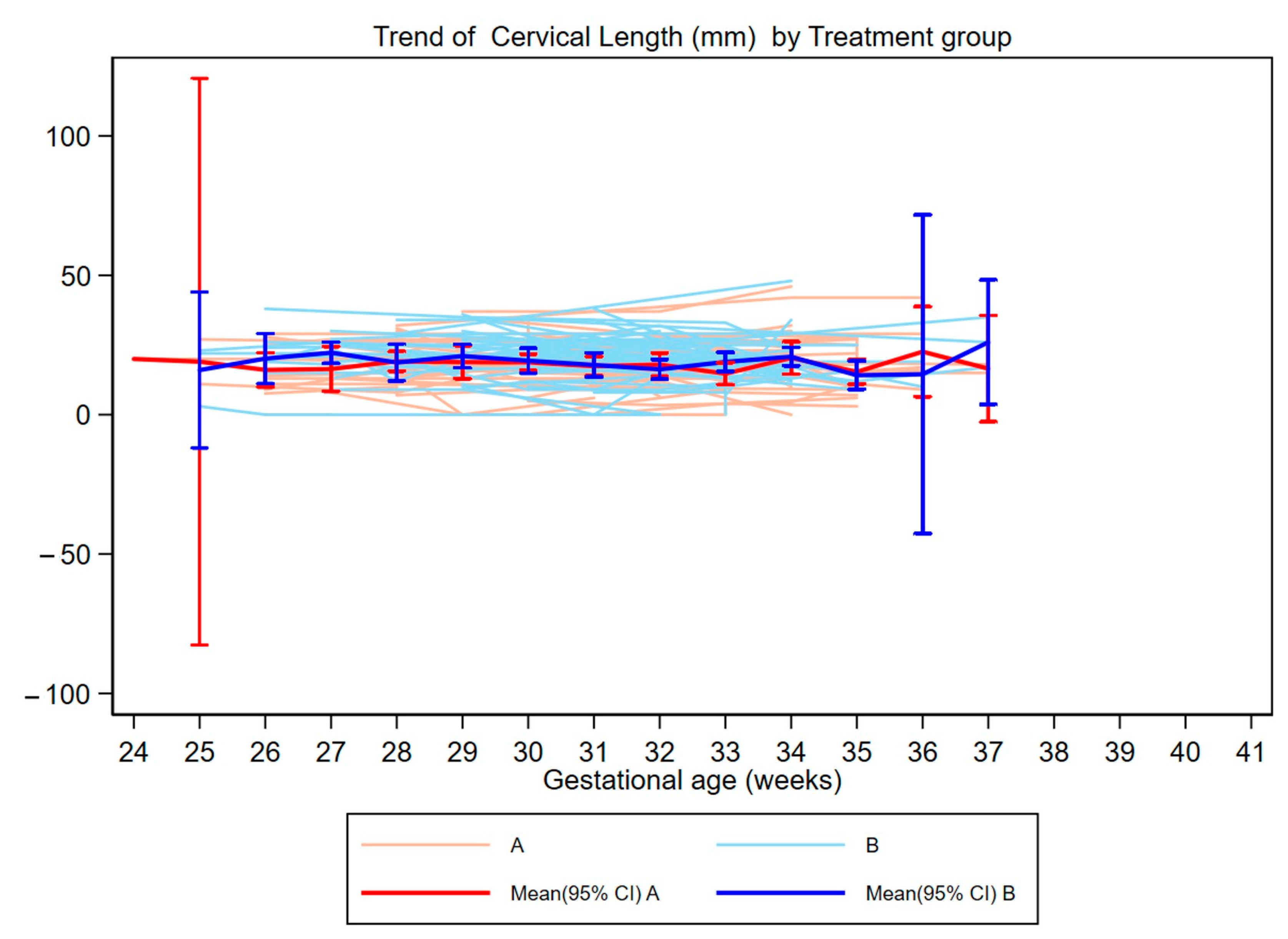
Furthermore, when we compared the evolution of cervical length throughout gestation in both groups, no differences were observed (Figure 1).

Figure 1.
Individual trajectories of cervical length percentiles throughout pregnancy, grouped by intervention. Each line represents a single participant. Group A: probiotic treatment; Group B: placebo.
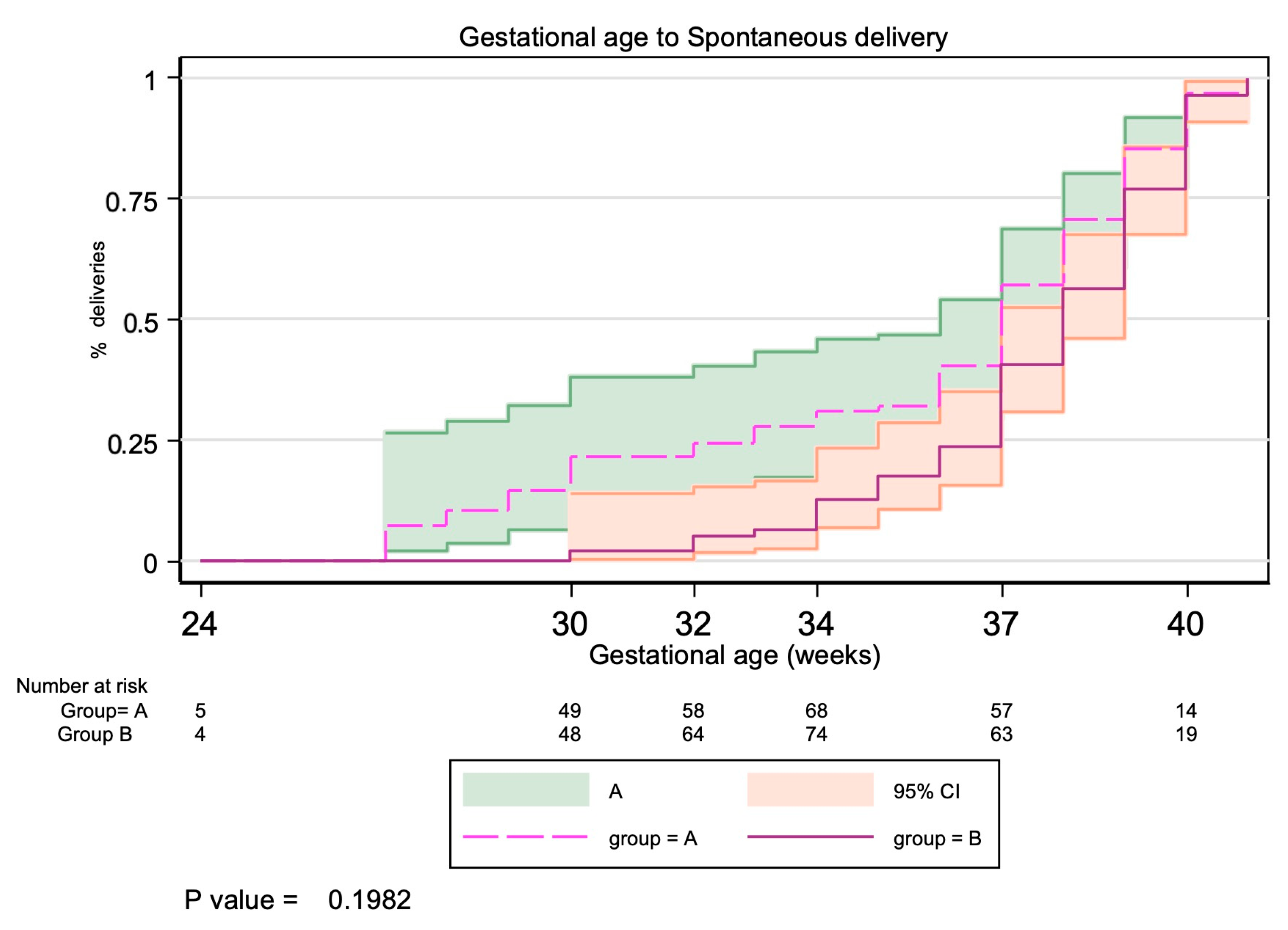
We performed a survival analysis to assess time to birth from 24 weeks of gestation, accounting for the fact that each woman entered the study at a different gestational age. Results are shown in Figure 2. Births induced before 37 weeks of gestation were removed from this analysis. A survival model for truncated data was used, comparing only women who remained at risk of preterm birth at each time point. This approach corrected for variability in the timing of study entry and follow-up across participants. No significant differences were observed between the probiotic and placebo groups (Figure 3).
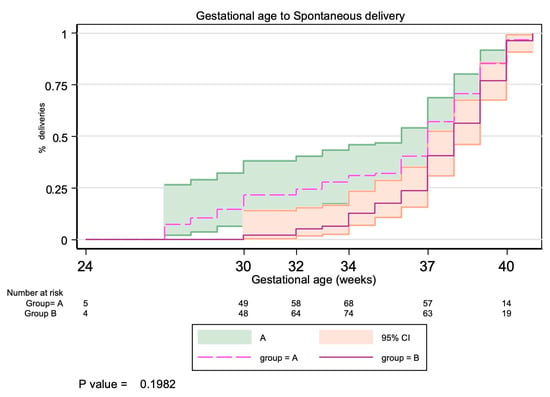
Figure 2.
Kaplan–Meier analysis of time to spontaneous delivery (weeks) by intervention group. Group A: probiotic treatment; Group B: placebo. The x-axis displays selected gestational age milestones that are clinically relevant in obstetrics: 24 weeks (viability threshold), 30 and 32 weeks (key time points at which the risk of severe neonatal morbidity begins to decrease), 34 weeks (late preterm), 37 weeks (term), and 40 weeks (full-term pregnancy).
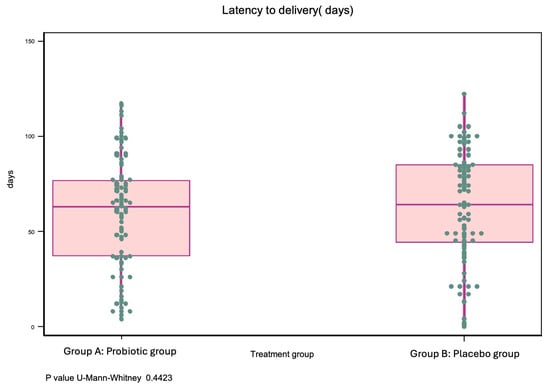
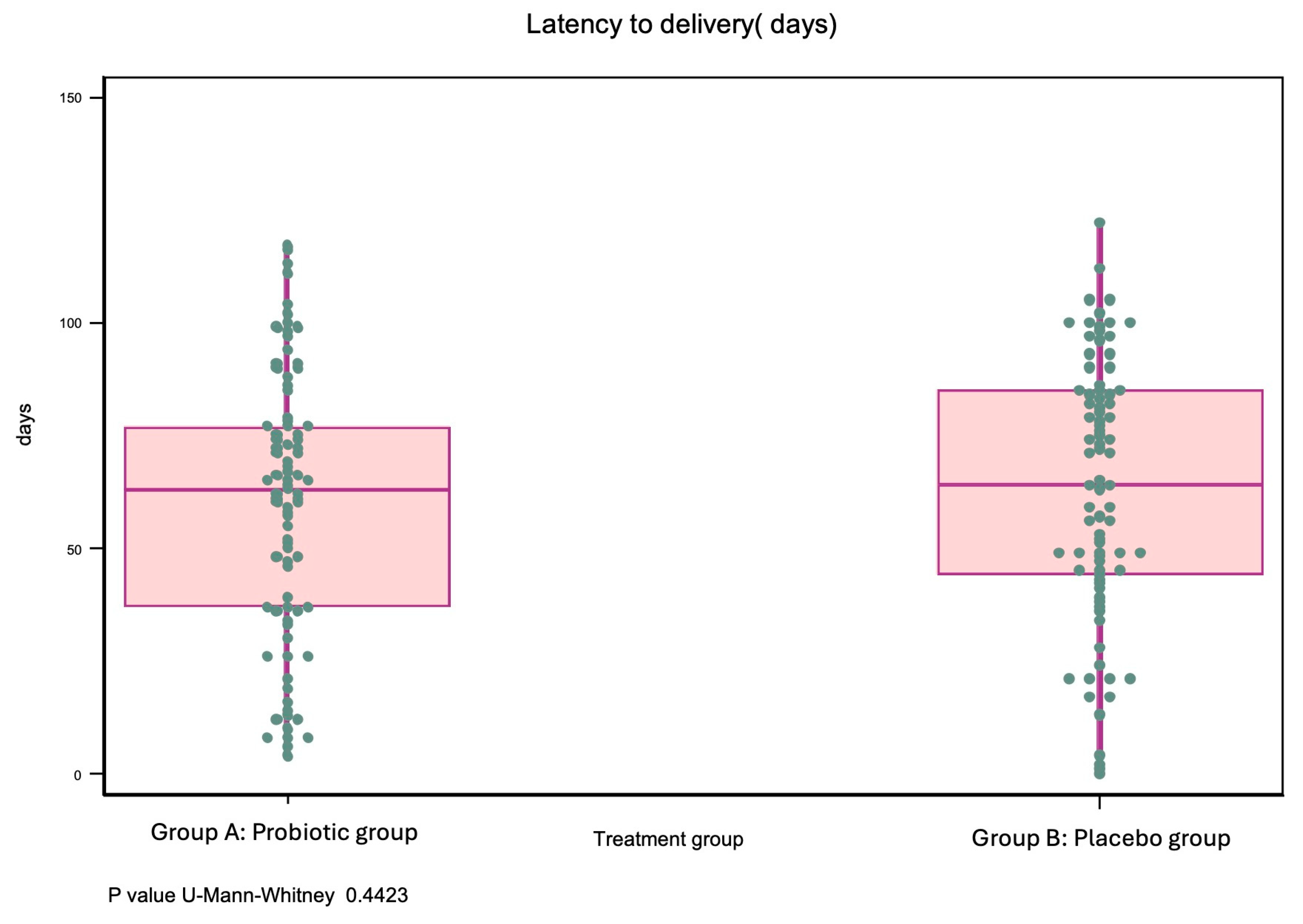
Figure 3.
Latency time to delivery (in days) from randomization by intervention group. Group A: the probiotic group; Group B: the placebo group.
3.1. Microbiota Analysis
One of the secondary endpoints was the modification of vaginal microbiota in pregnant women at risk of PTB receiving probiotics. To determine this endpoint, a sample of the vaginal microbiota was collected in patients recruited at Hospital Vall d’Hebron.
At the time of enrollment, the vaginal microbiota of high-risk pregnant women was predominantly composed of 10 genera, accounting for 98% of the total sequencing data. Among those genera, Lactobacillus was the most abundant (78.42%), followed by Gardnerella (9.2%), Bifidobacterium (4.3%), Fannyhessea (1.8%), and Prevotella (1.8%). The most common community state type (CST) was dominated by L. iners (45%, CST III), followed by L. crispatus (25%, CST I) and a highly diverse community (18%, CST IV). CST IV was mainly composed of G. vaginalis (38%), B. dentium-moukalabense (10.6%), F. vaginae (8.8%), and B. longum (8.8%). CST II, which was dominated by L. gasseri, was found in 25% of the participants, and only one participant was clustered into the CST V group, which was dominated by L. jensenii. No differences in the proportion of CSTs between groups was observed (p-value = 0.69, Fisher’s exact) before intervention (Table 4).
Table 4.
Community state type (CST) frequency in both groups after the intervention.
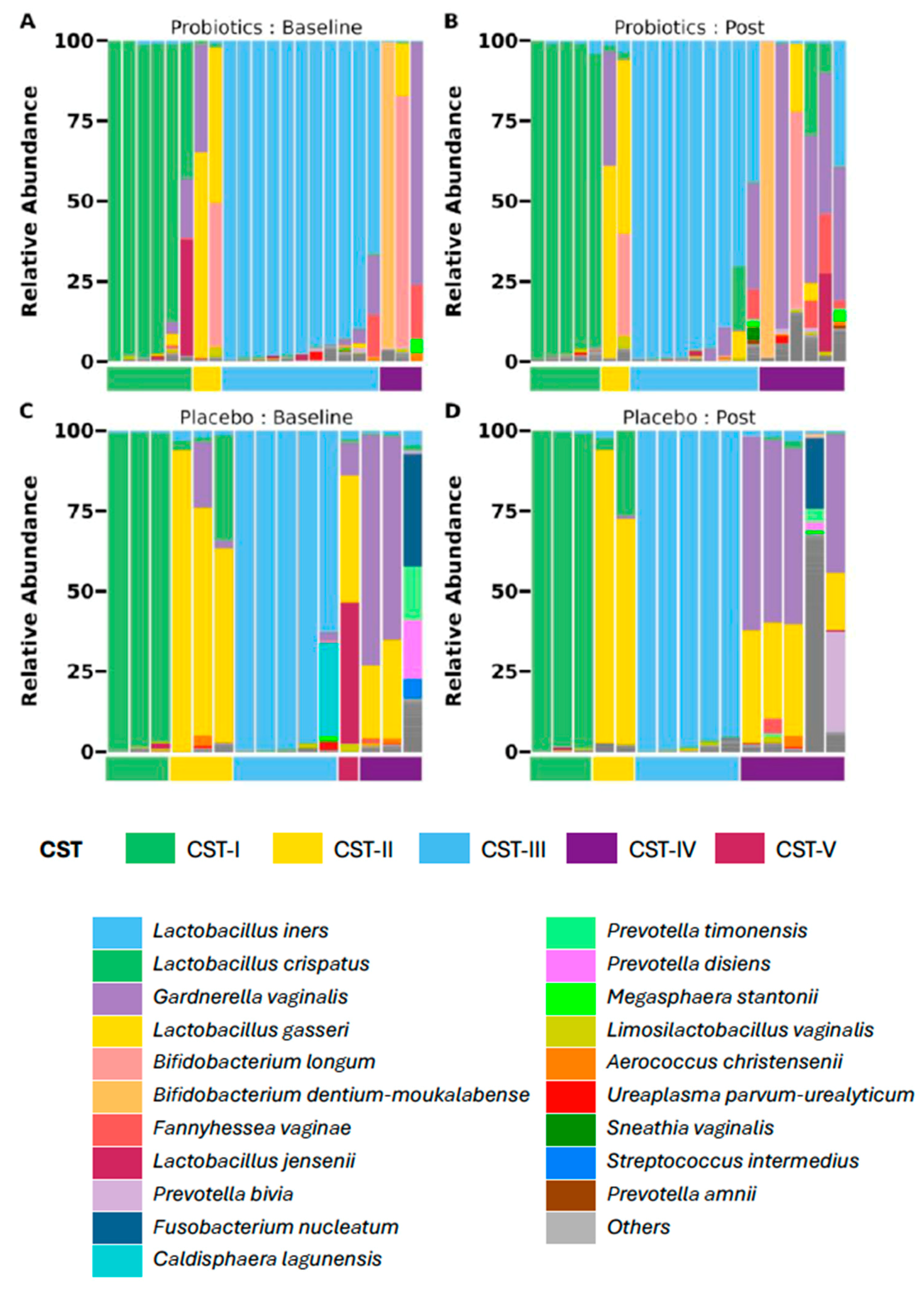
After the intervention, the microbial profiles in both the placebo and probiotic groups remained stable (Figure 4). No significant differences were found in beta diversity, alpha diversity, or microbial load. Consistently, no differentially abundant genera or species were observed between women who received probiotics as compared to those who received the placebo, according to the MaAsLin2, ANCOM-BC2, and Wilcoxon tests. Interestingly, over the 4-week follow-up, although the CST III microbial profile remained predominant, CST IV (29%) was established as the second most predominant, shifting CST II (20%) to the third position (Table 4). This change is explained because six women had a CST shift, five of them shifting from Lactobacillus-dominated CST to CST IV, with no differences between groups in the frequency of shifts or the number of transitions to or from a specific CST group.
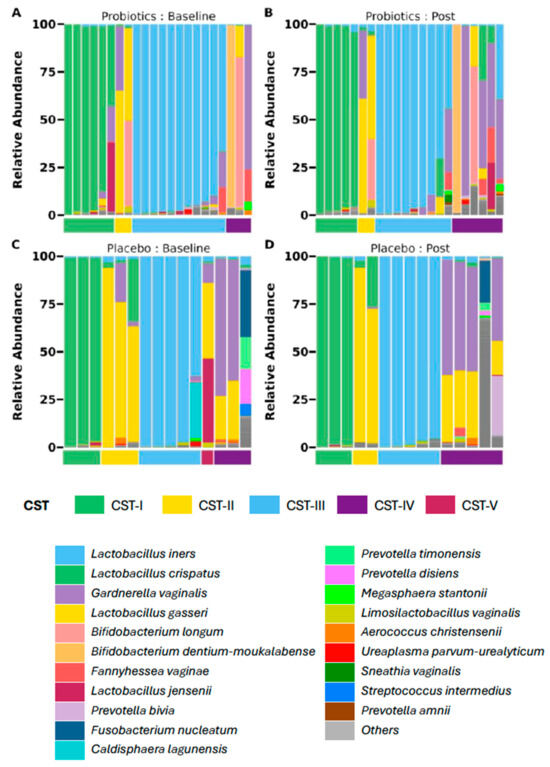
Figure 4.
Vaginal microbial profiles before and after the intervention by study group. Each panel displays community state types (CSTs) and dominant bacterial species per participant at baseline (A,C) and after 4 weeks (B,D). Only paired samples are shown (probiotics: n = 22 and placebo: n = 15). Top panels (A,B): probiotic group (n = 22); Bottom panels (C,D) ): placebo group (n = 15).
3.2. Safety Management
Adverse events are shown in the tables according to the MedDRA classification, version 26.0 (see Table 5).
Table 5.
Adverse effects.
During the clinical trial, a total of 24 adverse events (AEs) were reported by 16 patients (active intervention = 10 events; placebo = 14 events). Two of these were serious adverse events: a gastric ulcer (placebo group) and a prolongation of hospitalization that led to inclusion in the study (active intervention group). All patients recovered from the AEs without consequences. In terms of causality, 13 events (54.2%) were considered unrelated to the intervention, 5 (20.8%) were deemed unlikely related to the intervention, 5 (20.8%) were potentially related to the intervention, and 1 event (4.2%) was considered likely related to the intervention.
During the trial, the most frequent adverse events were as follows: gestational diabetes (N = 2; 8.3%), hospitalization due to threatened preterm birth (N = 3; 12.5%), and COVID-19 (N = 2; 8.3%).
No serious unexpected adverse event reaction (SUSAR) was reported during the trial.
4. Discussion
The primary aim of this study was to determine if vaginal probiotics containing multiple strains of Lactobacillus could effectively reduce preterm birth rates in pregnant women with a high risk of preterm birth. This research holds particular relevance, as preterm birth remains a leading cause of neonatal morbidity and mortality globally. In this trial, the comparison between the probiotic and placebo groups showed no significant differences in preterm birth rates. These findings support the results of earlier studies that also found no substantial benefit with probiotic use in this context [48,49,50,51], suggesting that, while probiotics benefit other health conditions, their efficacy in preventing preterm birth remains unclear. Likewise, no significant differences between groups were found in the analysis of perinatal outcomes, including gestational age at birth and neonatal health indicators, further supporting the initial conclusion [52].
Another critical aim of this study was to explore whether the use of probiotics could modify the composition of vaginal microbiota, given the well-established association between low levels of Lactobacillus and an increased risk of preterm birth. These results suggest that the vaginal microbiota in the late second and early third trimester may be relatively stable and resistant to external modulation, even with daily administration of a multi-strain probiotic. This microbial resilience may explain the lack of statistically and biologically significant differences between groups and underscores the complexity of intervening in established microbial ecosystems during pregnancy. These results are consistent with other studies that also failed to demonstrate a clear change in vaginal flora following a probiotic intervention [53]. This suggests that the probiotics used were not potent enough to shift the microbial balance, or the existing microbial environment was resilient to change.
A significant strength of this study is its focus on a specific high-risk population: pregnant women at a high risk of preterm birth. By targeting this group, this study aims to provide insights directly applicable to those most likely to benefit from effective interventions. This study has several limitations. First, the sample size for the microbiota sub-analysis was relatively small and limited to a single center. This was primarily due to organizational constraints and laboratory availability, as microbiota sampling and processing were only feasible at one site. Second, environmental, nutritional, and behavioral factors that could influence microbiota composition were not controlled for. Finally, the timing of the intervention, which was administered when microbial communities were likely already well established, may have reduced the potential for significant modulation.
Nonetheless, the safety profile of the probiotic was confirmed, with no significant adverse effects reported, suggesting that while probiotics may not prevent preterm birth, they are safe in pregnant women.
This underscores the complex and multifaceted nature of preterm birth, highlighting the existing gaps in understanding its underlying causes and effective prevention strategies. The findings of this study contribute to this body of knowledge by providing additional evidence that vaginal probiotics do not reduce preterm birth rates. However, future studies should be undertaken to investigate probiotics as a preventive treatment initiated during the first trimester of pregnancy. This further emphasizes the need for continued research to identify and clarify the mechanisms behind preterm birth and to develop effective interventions and preventive measures. Exploring other therapeutic approaches, possibly in combination with probiotics or entirely new interventions, might be necessary to make significant progress in the reduction in preterm birth rates. It is important to note that this intervention was designed specifically to address risks in the current pregnancy, not as a long-term or interpregnancy preventive approach.
5. Conclusions
Our study did not reveal any statistical differences in the rate of spontaneous preterm birth between pregnant women receiving probiotics and those receiving a placebo. Furthermore, following a regimen with a four-strain probiotic, no statistically significant differences in the vaginal microbiota of women were detected between both groups, although subtle trends were observed. These trends suggest a potential depletion of Lactobacilli populations, a factor often linked to an increased risk of spontaneous preterm birth. Importantly, no safety concerns were identified, indicating a good safety profile of the investigational product.
Although the probiotic intervention did not prove effective in reducing preterm birth in this high-risk symptomatic population, its safety and tolerability support further investigation in other clinical settings, such as earlier in pregnancy or in combination with established preventive strategies.
Author Contributions
Formal analysis, L.-A.G.M., Z.S., E.C. and C.M.; investigation, E.d.B., M.V. (Mireia Vargas), M.M., L.P. (Linda Puerto), C.G.-G., B.M., L.P. (Laia Pratcorona), S.R., M.V. (Mercè Vidal), M.D., A.C., C.M. and M.G.; methodology, E.d.B., M.V. (Mireia Vargas), M.M., C.M. and M.G.; supervision, M.D., E.C., C.M. and M.G.; Writing—original draft, E.d.B., C.M. and M.G.; Writing—review and editing, C.M. and M.G. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Spanish Clinical Research Network (SCReN), which is funded by the ISCIII-General Subdirectorate for Evaluation and Promotion of Research through projects PT17/0017/0030 and PT20/00078. Both projects were integrated into the 2013–2016 National Plan for Scientific and Technical Research and Innovation and co-financed by the European Regional Development Fund (ERDF), “A way of making Europe”. This work was also supported by Project FIS PI 19/00287 (Maria Goya as a principal investigator), which was funded by Instituto de Salud Carlos III (ISCIII) and co-funded by the European Union. Laboratorios Ordesa S.L funded the PROPEV study. L.-A.G.M. was supported by Instituto de Salud Carlos III/FEDER (PI20/00130).
Institutional Review Board Statement
The protocol was approved by the local Ethics Committee of each participating hospital (registration number: PR(AMI)359/2014 and date of issue: 1 December 2014). The study protocol was registered in Clinicaltrials.gov on 11 February 2018 (Identifier: NCT03689166 and URL address: https://clinicaltrials.gov/study/NCT03689166 (accessed on 16 September 2022)).
Informed Consent Statement
All participants provided their written informed consent.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Acknowledgments
We thank Mar Jimenez-Quesada for her help with the English version of this report.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| PTB | preterm birth |
| CSTs | composted tannery sludge |
| sPTB | spontaneous preterm birth |
| AEs | adverse events |
| SUSAR | serious unexpected adverse event reaction |
| BMI | body mass index |
References
- WHO. Low Birth Weight. Available online: https://www.who.int/data/nutrition/nlis/info/low-birth-weight (accessed on 20 May 2024).
- Lawn, J.E.; Gravett, M.G.; Nunes, T.M.; Rubens, C.E.; Stanton, C.; the GAPPS Review Group. Global report on preterm birth and stillbirth (1 of 7): Definitions, description of the burden and opportunities to improve data. BMC Pregnancy Childbirth 2010, 10, S1. [Google Scholar] [CrossRef] [PubMed]
- Mwaniki, M.K.; Atieno, M.; Lawn, J.E.; Newton, C.R. Long-term neurodevelopmental outcomes after intrauterine and neonatal insults: A systematic review. Lancet 2012, 379, 445–452. [Google Scholar] [CrossRef] [PubMed]
- WHO. Born Too Soon: The Global Action Report on Preterm Birth. Available online: https://www.who.int/publications/i/item/9789241503433 (accessed on 20 May 2024).
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.B.; Narwal, R.; Adler, A.; Garcia, C.V.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef] [PubMed]
- Slattery, M.M.; Morrison, J.J. Preterm delivery. Lancet 2002, 360, 1489–1497. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Iams, J.D.; Romero, R.; Culhane, J.F.; Goldenberg, R.L. Primary, secondary, and tertiary interventions to reduce the morbidity and mortality of preterm birth. Lancet 2008, 371, 164–175. [Google Scholar] [CrossRef]
- France, M.; Alizadeh, M.; Brown, S.; Ravel, J. Towards a deeper understanding of the vaginal microbiota. Nat. Microbiol. 2022, 7, 367–378. [Google Scholar] [CrossRef]
- Kwon, M.S.; Lee, H.K. Host and Microbiome Interplay Shapes the Vaginal Microenvironment. Front. Immunol. 2022, 13, 919728. [Google Scholar] [CrossRef]
- Plesniarski, A.; Siddik, A.B.; Su, R.C. The Microbiome as a Key Regulator of Female Genital Tract Barrier Function. Front. Cell. Infect. Microbiol. 2021, 11, 790627. [Google Scholar] [CrossRef]
- Bayar, E.; Bennett, P.R.; Chan, D.; Sykes, L.; MacIntyre, D.A. The pregnancy microbiome and preterm birth. Semin. Immunopathol. 2020, 42, 487–499. [Google Scholar] [CrossRef]
- Fettweis, J.M.; Serrano, M.G.; Edwards, D.J.; Girerd, P.H.; Parikh, H.I.; Huang, B.; Arodz, T.J.; Edupuganti, L.; Glascock, A.L.; Xu, J.; et al. The vaginal microbiome and preterm birth. Nat. Med. 2019, 25, 1012–1021. [Google Scholar] [CrossRef] [PubMed]
- Gudnadottir, U.; Debelius, J.W.; Du, J.; Hugerth, L.W.; Danielsson, H.; Schuppe-Koistinen, I.; Fransson, E.; Brusselaers, N. The vaginal microbiome and the risk of preterm birth: A systematic review and network meta-analysis. Sci. Rep. 2022, 12, 7926. [Google Scholar] [CrossRef] [PubMed]
- Serrano, M.G.; Parikh, H.I.; Edwards, D.J.; Arodz, T.J.; Edupuganti, L.; Huang, B.; Girerd, P.H.; Bokhari, Y.A.; Bradley, S.P.; Brooks, J.L. Racioethnic diversity in the dynamics of the vaginal microbiome during pregnancy. Nat. Med. 2019, 25, 1001–1011. [Google Scholar] [CrossRef] [PubMed]
- Mls, J.; Stráník, J.; Kacerovský, M. Lactobacillus iners-dominated vaginal microbiota in pregnancy. Ceska Gynekol. 2019, 84, 463–467. [Google Scholar]
- Petricevic, L.; Domig, K.J.; Nierscher, F.J.; Sandhofer, M.J.; Fidesser, M.; Krondorfer, I.; Husslein, P.; Kneifel, W.; Kiss, H. Characterisation of the vaginal Lactobacillus microbiota associated with preterm delivery. Sci. Rep. 2014, 4, 5136. [Google Scholar] [CrossRef]
- Zhou, Q.; Yu, Y.; Zhou, J.; Liu, J.; Gao, J. Relationship of Lactobacillus Vaginal Microbiota Changes and the Risk of Preterm Birth: A Systematic Review and Meta-Analysis. J. Womens Health 2024, 33, 228–238. [Google Scholar] [CrossRef]
- Biggs, W.S.; Williams, R.M. Common Gynecologic Infections. Prim. Care Clin. Off. Pract. 2009, 36, 33–51. [Google Scholar] [CrossRef]
- Boris, S.; Suárez, J.E.; Vázquez, F.; Barbés, C. Adherence of Human Vaginal lactobacilli to Vaginal epithelial Cells and Interaction with Uropathogens. Infect. Immun. 1998, 66, 1985–1989. [Google Scholar] [CrossRef]
- Mastromarino, P.; Brigidi, P.; Macchia, S.; Maggi, L.; Pirovano, F.; Trinchieri, V.; Conte, U.; Matteuzzi, D. Characterization and selection of vaginal Lactobacillus strains for the preparation of vaginal tablets. J. Appl. Microbiol. 2002, 93, 884–893. [Google Scholar] [CrossRef]
- Atassi, F.; Brassart, D.; Grob, P.; Graf, F.; Servin, A.L. Lactobacillus strains isolated from the vaginal microbiota of healthy women inhibit Prevotella bivia and Gardnerella vaginalis in coculture and cell culture. FEMS Immunol. Med. Microbiol. 2006, 48, 424–432. [Google Scholar] [CrossRef]
- Coudeyras, S.; Jugie, G.; Vermerie, M.; Forestier, C. Adhesion of Human Probiotic Lactobacillus rhamnosus to Cervical and Vaginal Cells and Interaction with Vaginosis-Associated Pathogens. Infect. Dis. Obs. Gynecol. 2008, 2008, 549640. [Google Scholar]
- Phukan, N.; Parsamand, T.; Brooks, A.E.S.; Nguyen, T.N.M.; Simoes-Barbosa, A. The adherence of Trichomonas vaginalis to host ectocervical cells is influenced by lactobacilli. Sex. Transm. Infect. 2013, 89, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Juárez Tomás, M.S.; Ocaña, V.S.; Wiese, B.; Nader-Macías, M.E. Growth and lactic acid production by vaginal Lactobacillus acidophilus CRL 1259, and inhibition of uropathogenic Escherichia coli. J. Med. Microbiol. 2003, 52, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Vielfort, K.; Sjölinder, H.; Roos, S.; Jonsson, H.; Aro, H. Adherence of clinically isolated lactobacilli to human cervical cells in competition with Neisseria gonorrhoeae. Microbes Infect. 2008, 10, 1325–1334. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.; Petrova, M.I.; Claes, I.J.J.; Verhoeven, T.L.A.; Busschaert, P.; Vaneechoutte, M.; Lievens, B.; Lambrichts, I.; Siezen, R.J.; Balzarini, J.; et al. The Highly Autoaggregative and Adhesive Phenotype of the Vaginal Lactobacillus plantarum Strain CMPG5300 Is Sortase Dependent. Appl. Env. Microbiol. 2013, 79, 4576–4585. [Google Scholar] [CrossRef]
- Rossi, A.; Rossi, T.; Bertini, M.; Caccia, G. The use of Lactobacillus rhamnosus in the therapy of bacterial vaginosis. Evaluation of clinical efficacy in a population of 40 women treated for 24 months. Arch. Gynecol. Obstet. 2010, 281, 1065–1069. [Google Scholar] [CrossRef]
- Marcone, V.; Calzolari, E.; Bertini, M. Effectiveness of vaginal administration of Lactobacillus rhamnosus following conventional metronidazole therapy: How to lower the rate of bacterial vaginosis recurrences. New Microbiol. 2008, 31, 429–433. [Google Scholar]
- Marcone, V.; Rocca, G.; Lichtner, M.; Calzolari, E. Long-term vaginal administration of Lactobacillus rhamnosus as a complementary approach to management of bacterial vaginosis. Int. J. Gynaecol. Obs. Off. Organ. Int. Fed. Gynaecol. Obstet. 2010, 110, 223–226. [Google Scholar] [CrossRef]
- Larsson, P.G.; Brandsborg, E.; Forsum, U.; Pendharkar, S.; Andersen, K.K.; Nasic, S.; Hammarström, L.; Marcotte, H. Extended antimicrobial treatment of bacterial vaginosis combined with human lactobacilli to find the best treatment and minimize the risk of relapses. BMC Infect. Dis. 2011, 11, 223. [Google Scholar] [CrossRef]
- Rautava, S.; Kalliomäki, M.; Isolauri, E. Probiotics during pregnancy and breast-feeding might confer immunomodulatory protection against atopic disease in the infant. J. Allergy Clin. Immunol. 2002, 109, 119–121. [Google Scholar] [CrossRef]
- Huurre, A.; Laitinen, K.; Rautava, S.; Korkeamäki, M.; Isolauri, E. Impact of maternal atopy and probiotic supplementation during pregnancy on infant sensitization: A double-blind placebo-controlled study. Clin. Exp. Allergy. 2008, 38, 1342–1348. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Effect of Probiotics on the Preterm Delivery Rate in Pregnant Women at High Risk for Preterm Birth (PROPEV). Available online: https://clinicaltrials.gov/study/NCT03689166 (accessed on 16 September 2022).
- International Human Microbiome Standards (IHMS). International Human Microbiome Standards (IHMS). Available online: http://www.human-microbiome.org (accessed on 16 March 2023).
- Costea, P.I.; Zeller, G.; Sunagawa, S.; Pelletier, E.; Alberti, A.; Levenez, F.; Tramontano, M.; Driessen, M.; Hercog, R.; Jung, F.E.; et al. Towards standards for human fecal sample processing in metagenomic studies. Nat. Biotechnol. 2017, 35, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- Cuenca, S.; Soler, Z.; Serrano-Gómez, G.; Xie, Z.; Barquinero, J.; Roca, J.; Sirvent, J.M.; Manichanh, C. Dysbiosis: An Indicator of COVID-19 Severity in Critically Ill Patients. Int. J. Mol. Sci. 2022, 23, 15808. [Google Scholar] [CrossRef]
- Husain, S.; Wilks, M.; Mupita, M.; Reddy, S.; Hennessy, E.; Macfarlane, A.; Millar, M. Diversity and stability of cultured vaginal lactobacilli in pregnant women from a multi-ethnic urban UK population. J. Appl. Microbiol. 2014, 117, 258–265. [Google Scholar] [CrossRef]
- Vargas, M.; Yañez, F.; Elias, A.; Bernabeu, A.; Goya, M.; Xie, Z.; Farrás, A.; Sánchez, O.; Soler, Z.; Blasquez, C.; et al. Cervical pessary and cerclage placement for preterm birth prevention and cervicovaginal microbiome changes. Acta Obstet. Gynecol. Scand. 2022, 101, 1403–1413. [Google Scholar] [CrossRef]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.A.; Holmes, S.P. DADA2: High-resolution sample inference from Illumina amplicon data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef]
- Molano, L.A.G.; Vega-Abellaneda, S.; Manichanh, C. GSR-DB: A manually curated and optimized taxonomical database for 16S rRNA amplicon analysis. mSystems 2024, 9, e0095023. [Google Scholar] [CrossRef]
- Mallick, H.; Rahnavard, A.; McIver, L.J.; Ma, S.; Zhang, Y.; Nguyen, L.H.; Tickle, T.L.; Weingart, G.; Ren, B.; Schwager, E.H.; et al. Multivariable association discovery in population-scale meta-omics studies. PLoS Comput. Biol. 2021, 17, e1009442. [Google Scholar] [CrossRef]
- Lin, H.; Peddada, S.D. Multigroup analysis of compositions of microbiomes with covariate adjustments and repeated measures. Nat. Methods 2024, 21, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Nearing, J.T.; Douglas, G.M.; Hayes, M.G.; MacDonald, J.; Desai, D.K.; Allward, N.; Jones, C.M.A.; Wright, R.J.; Dhanani, A.S.; Comeau, A.M.; et al. Microbiome differential abundance methods produce different results across 38 datasets. Nat. Commun. 2022, 13, 342. [Google Scholar] [CrossRef] [PubMed]
- Oksanen, J.; Blanchet, F.G.; Friendly, M.; Kindt, R.; Legendre, P.; McGlinn, D.; Minchin, P.R.; O’Hara, R.B.; Simpson, G.L.; Solymos, P.; et al. Vegan: Community Ecology Package. Available online: https://github.com/vegandevs/vegan (accessed on 20 May 2024).
- Jarde, A.; Lewis-Mikhael, A.-M.; Moayyedi, P.; Stearns, J.C.; Collins, S.M.; Beyene, J.; McDonald, S.D. Pregnancy outcomes in women taking probiotics or prebiotics: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2018, 18, 14. [Google Scholar] [CrossRef] [PubMed]
- Vanda, R.; Dastani, T.; Taghavi, S.-A.; Sadeghi, H.; Lambert, N.; Bazarganipour, F. Pregnancy outcomes in pregnant women taking oral probiotic undergoing cerclage compared to placebo: Two blinded randomized controlled trial. BMC Pregnancy Childbirth 2024, 24, 311. [Google Scholar] [CrossRef]
- Petricevic, L.; Rosicky, I.; Kiss, H.; Janjic, N.; Kaufmann, U.; Holzer, I.; Farr, A. Effect of vaginal probiotics containing Lactobacillus casei rhamnosus (Lcr regenerans) on vaginal dysbiotic microbiota and pregnancy outcome, prospective, randomized study. Sci. Rep. 2023, 13, 7129. [Google Scholar] [CrossRef]
- Yefet, E.; Colodner, R.; Strauss, M.; Letova, Y.G.Z.; Nachum, Z. A Randomized Controlled Open Label Crossover Trial to Study Vaginal Colonization of Orally Administered Lactobacillus reuteri RC-14 and Rhamnosus GR-1 in Pregnant Women at High Risk for Preterm Labor. Nutrients. 2020, 12, 1141. [Google Scholar] [CrossRef]
- McDougall, A.; Nguyen, R.; Nguyen, P.Y.; Allen, C.; Cheang, S.; Makama, M.; Mills, K.; Hastie, R.; Ammerdorffer, A.; Gulmezoglu, A.M.; et al. The effects of probiotics administration during pregnancy on preeclampsia and associated maternal, fetal, and newborn outcomes: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2024, 6, 101322. [Google Scholar] [CrossRef]
- Husain, S.; Allotey, J.; Drymoussi, Z.; Wilks, M.; Fernandez-Felix, B.; Whiley, A.; Dodds, J.; Thangaratinam, S.; McCourt, C.; Prosdocimi, E.; et al. Effects of oral probiotic supplements on vaginal microbiota during pregnancy: A randomised, double-blind, placebo-controlled trial with microbiome analysis. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 275–284. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).