
Father’s Knowledge, Attitude and Support to Mother’s Exclusive Breastfeeding Practices in Bangladesh: A Multi-Group Structural Equations Model Analysis

Abstract
1. Introduction
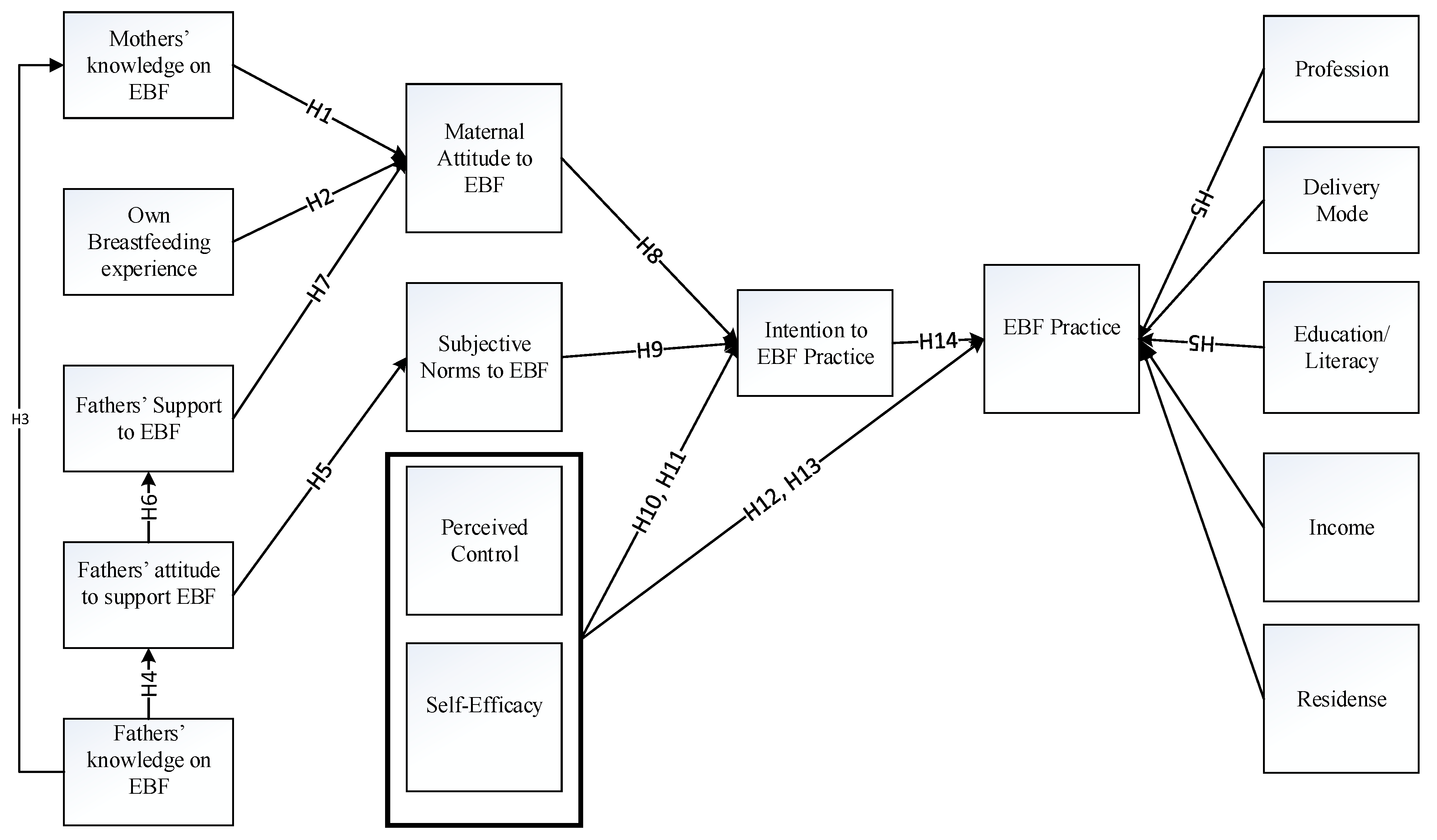
2. The Theoretical Explanations and Hypothesis Development
2.1. Mothers Knowledge and Experience of Exclusive Breastfeeding (EBF)
2.2. Fathers’ Knowledge of EBF
2.3. Fathers’ Attitude to Support EBF
2.4. Fathers’ Support towards EBF
2.5. Maternal Attitude to EBF
2.6. Subjective Norms
2.7. Perceived Behavioral Control (PBC)
2.8. EBF Intention
3. Materials and Methods
3.1. Design
3.2. Settings
3.3. Sampling
3.4. Inclusion Criteria and Exclusion Criteria
3.5. Measurements
3.5.1. Exclusive Breastfeeding and Practices of EBF
3.5.2. Intention to Practice EBF
3.5.3. EBF Attitude
3.5.4. Breastfeeding Knowledge and Experience
3.5.5. Normative Beliefs
3.5.6. Perceived Behavioral Control
4. Data Collection, Management and Ethical Considerations
5. Data Analysis
Evaluation of Multivariate Assumptions
6. Results
6.1. The Characteristics of Participant/Couples
List of Variables
6.2. Evaluation of Multivariate Assumptions
6.3. Measurement Model
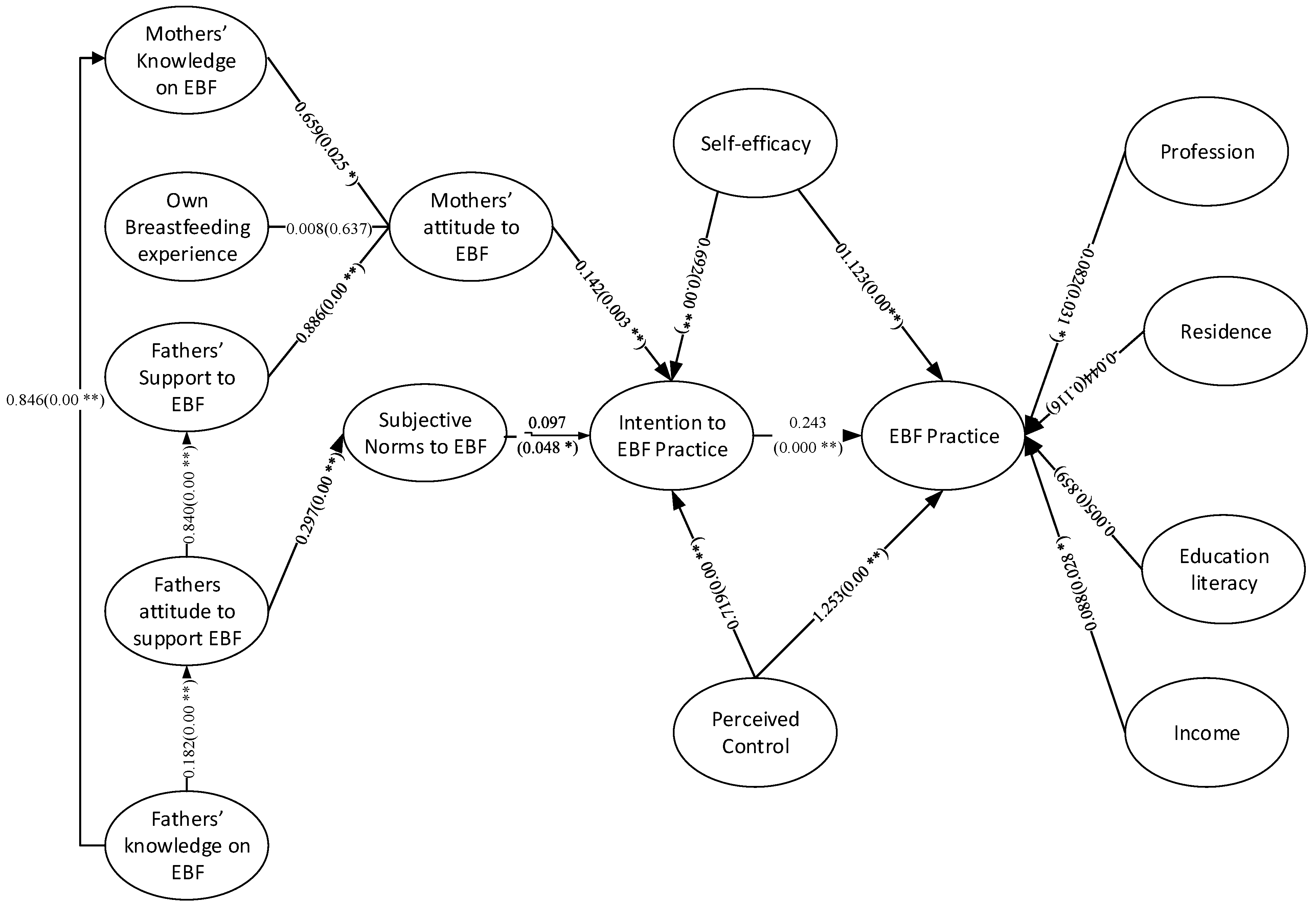
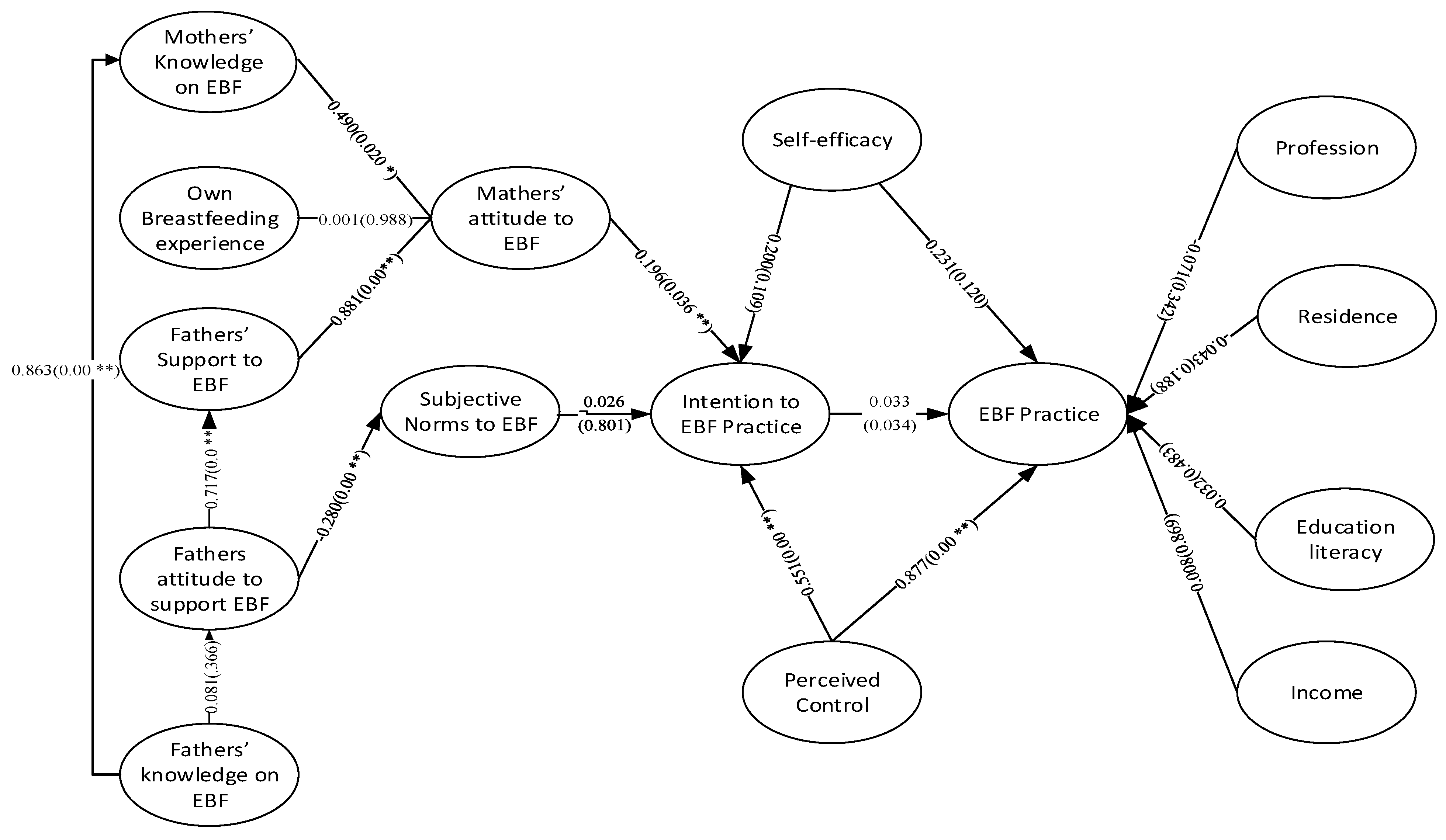
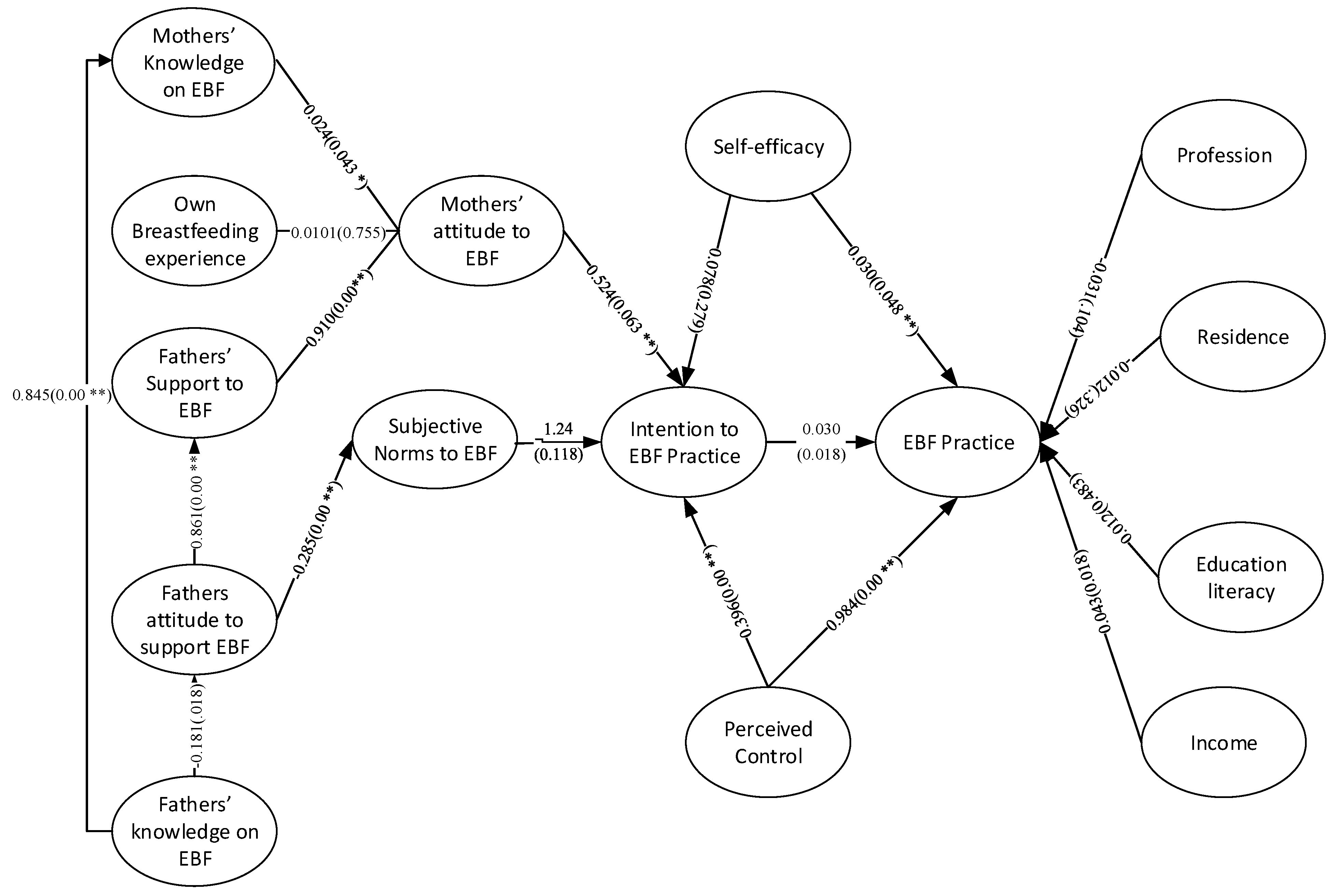
6.4. The Structural Model
7. Discussion
8. Practical Implications of the Research
9. Limitations of the Study
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hypotheses | Path | β | SD | t-Value | p-Value |
|---|---|---|---|---|---|
| H1 | M.Know->M. Att | 0.490 | 0.047 | 1.277 | 0.020 |
| H2 | M.Exp->M.Att | 0.001 | 0.045 | 0.015 | 0.988 |
| H3 | F.Know->M.Know | 0.863 | 0.025 | 34.400 | 0.000 |
| H4 | F.Know->F.Att | 0.081 | 0.089 | 0.905 | 0.366 |
| H5 | F.Att->M.SN | 0.280 | 0.072 | 3.866 | 0.000 |
| H6 | F.Att->F.Supp | 0.717 | 0.061 | 11.836 | 0.000 |
| H7 | F.Supp->M.Att | 0.881 | 0.032 | 27.258 | 0.000 |
| H8 | M.Att->M.Int | 0.196 | 0.105 | 1.861 | 0.036 |
| H9 | M.SN->M.Int | 0.026 | 0.102 | 0.252 | 0.801 |
| H10 | M.SE->M.Int | 0.200 | 0.124 | 1.607 | 0.109 |
| H11 | M.PC->M.Int | 0.551 | 0.071 | 7.703 | 0.000 |
| H12 | M.SE->EBF | 0.231 | 0.148 | 1.556 | 0.120 |
| H13 | M.PC->EBF | 0.877 | 0.077 | 11.350 | 0.000 |
| H14 | M.Int->EBF | 0.033 | 0.060 | 0.552 | 0.034 |
| Control Variables | Profession->EBF | −0.071 | 0.075 | 0.951 | 0.342 |
| Residence->EBF | −0.043 | 0.032 | 1.318 | 0.188 | |
| Education->EBF | 0.032 | 0.045 | 0.702 | 0.483 | |
| Income->EBF | 0.008 | 0.049 | 0.166 | 0.869 |
| Hypotheses | Path | β | SD | t-Value | p-Value |
|---|---|---|---|---|---|
| H1 | M.Know->M. Att | 0.024 | 0.031 | 0.790 | 0.043 |
| H2 | M.Exp->M.Att | 0.010 | 0.032 | 0.312 | 0.755 |
| H3 | F.Know->M.Know | 0.845 | 0.023 | 36.175 | 0.000 |
| H4 | F.Know->F.Att | 0.181 | 0.076 | 2.381 | 0.018 |
| H5 | F.Att->M.SN | 0.285 | 0.074 | 3.873 | 0.000 |
| H6 | F.Att->F.Supp | 0.861 | 0.024 | 36.204 | 0.000 |
| H7 | F.Supp->M.Att | 0.910 | 0.015 | 61.354 | 0.000 |
| H8 | M.Att->M.Int | 0.524 | 0.068 | 7.664 | 0.000 |
| H9 | M.SN->M.Int | 0.124 | 0.079 | 1.564 | 0.118 |
| H10 | M.SE->M.Int | 0.078 | 0.072 | 1.083 | 0.279 |
| H11 | M.PC->M.Int | 0.396 | 0.071 | 5.553 | 0.000 |
| H12 | M.SE->EBF | 0.030 | 0.015 | 1.981 | 0.048 |
| H13 | M.PC->EBF | 0.984 | 0.008 | 129.326 | 0.000 |
| H14 | M.Int->EBF | 0.030 | 0.016 | 1.904 | 0.018 |
| Control Variables | Profession->EBF | −0.031 | 0.019 | 1.628 | 0.104 |
| Residence->EBF | −0.012 | 0.012 | 0.982 | 0.326 | |
| Education->EBF | −0.012 | 0.015 | 0.776 | 0.438 | |
| Income->EBF | 0.043 | 0.018 | 2.376 | 0.018 |
| Mothers’ Demographic Characteristics | Percentage (of Total) | Fathers’ Demographic Characteristics | Percentage (of Total) | ||
|---|---|---|---|---|---|
| Age | 18–25 Years | 12 | 3.6 | 20 | 6.0 |
| 26–33 Years | 172 | 51.8 | 126 | 38.0 | |
| 34–41 Years | 144 | 43.4 | 168 | 50.6 | |
| 42–49 Years | 4 | 1.2 | 18 | 5.4 | |
| Number of Alive Children | 1 Children | 232 | 69.9 | 232 | 69.9 |
| 2 Children’s | 79 | 23.8 | 79 | 23.8 | |
| 3 Children’s | e | 5.7 | 19 | 5.7 | |
| 4 Children’s | 2 | 0.6 | 2 | 0.6 | |
| Resident of the Division | Sylhet | 8 | 2.4 | 8 | 2.4 |
| Mymensingh | 6 | 1.8 | 6 | 1.8 | |
| Khulna | 34 | 10.2 | 34 | 10.2 | |
| Rangpur | 10 | 3.0 | 10 | 3.0 | |
| Chittagong | 45 | 13.6 | 45 | 13.6 | |
| Barisal | 7 | 2.1 | 7 | 2.1 | |
| Rajshahi | 19 | 5.7 | 19 | 5.7 | |
| Dhaka | 203 | 61.1 | 203 | 61.1 | |
| Religion | Christians | 12 | 3.6 | 12 | 3.6 |
| Buddhism | 4 | 1.2 | 4 | 1.2 | |
| Hindu | 43 | 13.0 | 43 | 13.0 | |
| Islam | 273 | 82.2 | 273 | 82.2 | |
| Profession | Searching for work/unemployed | 33 | 9.9 | 8 | 2.4 |
| Housewife | 76 | 22.9 | |||
| Business | 78 | 23.5 | |||
| Employed for wage | 69 | 20.8 | |||
| Public Sector Employee | 116 | 34.9 | 79 | 23.8 | |
| Corporate Employee | 107 | 32.2 | 98 | 29.5 | |
| Education | Less than high school degree (Less than SSC) | 20 | 6.0 | 34 | 10.2 |
| High school degree (HSC) | 66 | 19.9 | 11 | 3.3 | |
| Bachelor degree | 74 | 22.3 | 97 | 29.2 | |
| Masters’ degree and above | 172 | 51.8 | 190 | 57.2 | |
| Income Per Month | <$100 | 115 | 34.6 | 47 | 14.2 |
| $100–$300 | 38 | 11.4 | 58 | 17.5 | |
| $300–$500 | 106 | 31.9 | 101 | 30.4 | |
| $500–$800 | 56 | 16.9 | 105 | 31.6 | |
| >$800 | 17 | 5.1 | 21 | 6.3 |
| Variables | F.Know | F.Att | F.Supp | M.Know | M.Exp | EBF | M.Int | M.Att | M.PC | M.SN | M.SE |
|---|---|---|---|---|---|---|---|---|---|---|---|
| F.Know | 1.000 | 1.000 | |||||||||
| F.Att | 1.000 | 1.191 | 1.089 | ||||||||
| F.Supp | 1.169 | ||||||||||
| M.Know | 1.762 | ||||||||||
| M.Exp | 1.017 | ||||||||||
| EBF | |||||||||||
| M.Int | 1.230 | ||||||||||
| M.Att | 1.108 | ||||||||||
| M.PC | 1.209 | 1.195 | 1.272 | 1.083 | |||||||
| M.SN | 1.586 | 1.838 | |||||||||
| M.SE | 1.026 | 1.431 | 1.030 |
References
- Hossain, M.; Islam, A.; Kamarul, T.; Hossain, G. Exclusive breastfeeding practice during first six months of an infant’s life in Bangladesh: A country based cross-sectional study. Bmc Pediatrics 2018, 18, 93. [Google Scholar] [CrossRef]
- Alnasser, Y.; Almasoud, N.; Aljohni, D.; Almisned, R.; Alsuwaine, B.; Alohali, R.; Almutairi, O.; Alhezayen, R. Impact of attitude and knowledge on intention to breastfeed: Can mHealth based education influence decision to breastfeed exclusively? Ann. Med. Surg. 2018, 35, 6–12. [Google Scholar] [CrossRef]
- Gouveri, E.; Papanas, N.; I Hatzitolios, A.; Maltezos, E. Breastfeeding and diabetes. Curr. Diabetes Rev. 2011, 7, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Bernard, J.Y.; De Agostini, M.; Forhan, A.; Alfaiate, T.; Bonet, M.; Champion, V.; Kaminski, M.; de Lauzon-Guillain, B.; Charles, M.-A.; Heude, B. Breastfeeding Duration and Cognitive Development at 2 and 3 Years of Age in the EDEN Mother–Child Cohort. J. Pediatrics 2013, 163, 36–42.e1. [Google Scholar] [CrossRef]
- Hauck, F.R.; Thompson, J.M.; Tanabe, K.O.; Moon, R.Y.; Vennemann, M.M. Breastfeeding and reduced risk of sudden infant death syndrome: A meta-analysis. Pediatrics 2011, 128, 103–110. [Google Scholar] [CrossRef]
- Hamze, L.; Mao, J.; Reifsnider, E. Knowledge and attitudes towards breastfeeding practices: A cross-sectional survey of postnatal mothers in China. Midwifery 2019, 74, 68–75. [Google Scholar] [CrossRef] [PubMed]
- González-Jiménez, E.; García, P.A.; Aguilar, M.J.; Padilla, C.A.; Álvarez, J. Breastfeeding and the prevention of breast cancer: A retrospective review of clinical histories. J. Clin. Nurs. 2014, 23, 2397–2403. [Google Scholar] [CrossRef] [PubMed]
- Espósito, M.; Córdoba, J.P. Advantages of Breastfeeding During Acute Infections: What The Evidence Says. Curr. Trop. Med. Rep. 2018, 5, 204–210. [Google Scholar] [CrossRef]
- Sankar, M.J.; Sinha, B.; Chowdhury, R.; Bhandari, N.; Taneja, S.; Martines, J.; Bahl, R. Optimal breastfeeding practices and infant and child mortality: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 3–13. [Google Scholar] [CrossRef]
- Bispo, S.; Chikhungu, L.; Rollins, N.; Siegfried, N.; Newell, M.L. Postnatal HIV transmission in breastfed infants of HIV-infected women on ART: A systematic review and meta-analysis. J. Int. Aids Soc. 2017, 20, 21251. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Unicef Global Breastfeeding Scorecard. 2019. Available online: https://apps.who.int/iris/bitstream/handle/10665/326049/WHO-NMH-NHD-19.22-eng.pdf?ua=1 (accessed on 25 April 2020).
- Islam, M.A.; Hassan, M.R.; Rana, M. Financial Deepening, Foreign Direct Investment and Economic growth: An ARDL Approach Evidence from Bangladesh. Jahangirnagar J. Bus. Stud. 2019, 8, 169–190. [Google Scholar]
- National Institute of Population Research; Training; Mitra; Associates; ICF International. Bangladesh Demographic and Health Survey 2014. 2016. Available online: http://worldpopulationreview.com/countries/bangladesh-population/cities/ (accessed on 12 May 2020).
- Exclusive Breastfeeding Rate Falls to 47pc. Available online: http://www.newagebd.net/article/33415/exclusive-breastfeeding-rate-falls-to-47pc (accessed on 25 April 2020).
- Blackstone, S.R.; Sanghvi, T. Predictors of exclusive breastfeeding across three time points in Bangladesh: An examination of the 2007, 2011 and 2014 Demographic and Health Survey. Int. Health 2018, 10, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Dun-Dery, E.J.; Laar, A.K. Exclusive breastfeeding among city-dwelling professional working mothers in Ghana. Int. Breastfeed. J. 2016, 11, 23. [Google Scholar] [CrossRef]
- deMontigny, F.; Gervais, C.; Larivière-Bastien, D.; St-Arneault, K. The role of fathers during breastfeeding. Midwifery 2018, 58, 6–12. [Google Scholar] [CrossRef]
- Thomas, C.; O’Riordan, M.A.; Furman, L. Effect of the knowledge and attitudes of a support person on maternal feeding choice. J. Hum. Lact. 2017, 33, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Ng, R.W.L.; Shorey, S.; He, H.-G. Integrative Review of the Factors That Influence Fathers’ Involvement in the Breastfeeding of Their Infants. J. Obstet. Gynecol. Neonatal Nurs. 2019, 48, 16–26. [Google Scholar] [CrossRef]
- Rempel, L.A.; Rempel, J.K.; Moore, K.C. Relationships between types of father breastfeeding support and breastfeeding outcomes. Matern. Child Nutr. 2017, 13, e12337. [Google Scholar] [CrossRef]
- Bartle, N.C.; Harvey, K. Explaining infant feeding: The role of previous personal and vicarious experience on attitudes, subjective norms, self-efficacy, and breastfeeding outcomes. Br. J. Health Psychol. 2017, 22, 763–785. [Google Scholar] [CrossRef]
- Asadullah, M.N.; Mansoor, N.; Randazzo, T.; Wahhaj, Z. Is son preference disappearing from Bangladesh? World Dev. 2021, 140, 105353. [Google Scholar] [CrossRef]
- Leng, R.N.W.; Shorey, S.; Yin, S.L.K.; Chan, C.P.P.; He, H.-G. Fathers’ Involvement in Their Wives’/Partners’ Breastfeeding: A Descriptive Correlational Study. J. Hum. Lact. 2019, 35, 801–812. [Google Scholar] [CrossRef]
- Reddy, S.M.; Montambault, J.; Masuda, Y.J.; Keenan, E.; Butler, W.; Fisher, J.R.; Asah, S.T.; Gneezy, A. Advancing conservation by understanding and influencing human behavior. Conserv. Lett. 2017, 10, 248–256. [Google Scholar] [CrossRef]
- Yang, S.-F.; Schmied, V.; Burns, E.; Salamonson, Y. Breastfeeding knowledge and attitudes of baccalaureate nursing students in Taiwan: A cohort study. Women Birth 2019, 32, e334–e340. [Google Scholar] [CrossRef] [PubMed]
- Haghighi, M.; Varzandeh, R. Maternal knowledge and attitude toward exclusive breastfeeding in six months after birth in Shiraz, Iran. Int. J. Pediatrics 2016, 4, 3759–3767. [Google Scholar]
- Walsh, K. Prior employment as a causal mechanism within entrepreneurial ecosystems. Reg. Stud. Reg. Sci. 2019, 6, 637–645. [Google Scholar] [CrossRef]
- Wagner, S.; Kersuzan, C.; Gojard, S.; Tichit, C.; Nicklaus, S.; Thierry, X.; Charles, M.A.; Lioret, S.; de Lauzon-Guillain, B. Breastfeeding initiation and duration in France: The importance of intergenerational and previous maternal breastfeeding experiences—Results from the nationwide ELFE study. Midwifery 2019, 69, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Ambikapathi, R.; Gunaratna, N.; Passarelli, S. Fathers’ Nutrition Knowledge is Associated with Household’s, Women’s, and Child’s Dietary Diversity in the Agriculture to Nutrition Study in Ethiopia. 2019. Available online: https://www.africaportal.org/publications/fathers-nutrition-knowledge-associated-households-womens-and-childs-dietary-diversity-agriculture-nutrition-study-ethiopia/ (accessed on 11 February 2021).
- Bich, T.H.; Cuong, N.M. Changes in knowledge, attitude and involvement of fathers in supporting exclusive breastfeeding: A community-based intervention study in a rural area of Vietnam. Int. J. Public Health 2017, 62, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Al Namir, H.M.A.; Brady, A.-M.; Gallagher, L. Fathers and breastfeeding: Attitudes, involvement and support. Br. J. Midwifery 2017, 25, 426–440. [Google Scholar] [CrossRef]
- Rempel, L.A.; Rempel, J.K. The breastfeeding team: The role of involved fathers in the breastfeeding family. J. Hum. Lact. 2011, 27, 115–121. [Google Scholar] [CrossRef]
- Sherriff, N.; Hall, V.; Panton, C. Engaging and supporting fathers to promote breast feeding: A concept analysis. Midwifery 2014, 30, 667–677. [Google Scholar] [CrossRef]
- Niela-Vilén, H.; Melender, H.-L.; Axelin, A.; Löyttyniemi, E.; Salanterä, S. Predictors of Breastfeeding Initiation and Frequency for Preterm Infants in the NICU. J. Obstet. Gynecol. Neonatal Nurs. 2016, 45, 346–358. [Google Scholar] [CrossRef] [PubMed]
- Srinivas, G.L.; Benson, M.; Worley, S.; Schulte, E. A clinic-based breastfeeding peer counselor intervention in an urban, low-income population: Interaction with breastfeeding attitude. J. Hum. Lact. 2015, 31, 120–128. [Google Scholar] [CrossRef] [PubMed]
- de Jager, E.; Skouteris, H.; Broadbent, J.; Amir, L.; Mellor, K. Psychosocial correlates of exclusive breastfeeding: A systematic review. Midwifery 2013, 29, 506–518. [Google Scholar] [CrossRef] [PubMed]
- de Jager, E.; Broadbent, J.; Fuller-Tyszkiewicz, M.; Nagle, C.; McPhie, S.; Skouteris, H. A longitudinal study of the effect of psychosocial factors on exclusive breastfeeding duration. Midwifery 2015, 31, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Moukarzel, S.; Abou Jaoudeh, M.; Farhat, A.; Saade, M.; Mamas, C.; Daly, A.J. Exploring the latitude of attitude: Intentions to breastfeed among adolescents in Lebanese schools. Matern. Child Nutr. 2020, 16, e12888. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.L.; Wang, T.; Liao, J.; Huang, C. Efficacy of the theory of planned behavior in predicting breastfeeding: Meta-analysis and structural equation modeling. Appl. Nurs. Res. 2016, 29, 37–42. [Google Scholar] [CrossRef]
- Wallston, K.A. Control Beliefs: Health Perspectives. In International Encyclopedia of the Social & Behavioral Sciences, 2nd ed.; Wright, J.D., Ed.; Elsevier: Oxford, UK, 2015; pp. 819–821. [Google Scholar]
- Giles, M.; Connor, S.; McClenahan, C.; Mallett, J.; Stewart-Knox, B.; Wright, M. Measuring young people’s attitudes to breastfeeding using the Theory of Planned Behaviour. J. Public Health 2007, 29, 17–26. [Google Scholar] [CrossRef][Green Version]
- Pertl, M.; Hevey, D.; Thomas, K.; Craig, A.; Ní Chuinneagáin, S.; Maher, L. Differential effects of self-efficacy and perceived control on intention to perform skin cancer-related health behaviours. Health Educ. Res. 2010, 25, 769–779. [Google Scholar] [CrossRef]
- Fila, S.A.; Smith, C. Applying the theory of planned behavior to healthy eating behaviors in urban Native American youth. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 11. [Google Scholar] [CrossRef]
- Osibogun, O.O.; Olufunlayo, T.F.; Oyibo, S.O. Knowledge, attitude and support for exclusive breastfeeding among bankers in Mainland Local Government in Lagos State, Nigeria. Int. Breastfeed. J. 2018, 13, 38. [Google Scholar] [CrossRef]
- Hardin-Fanning, F.; Ricks, J.M. Attitudes, social norms and perceived behavioral control factors influencing participation in a cooking skills program in rural Central Appalachia. Glob. Health Promot. 2017, 24, 43–52. [Google Scholar] [CrossRef]
- Ajzen, I. From intentions to actions: A theory of planned behavior. In Action Control; Springer: Berlin\Heidelberg, Germany, 1985; pp. 11–39. [Google Scholar]
- Kothari, C.R.; Garg, G. Research Methodology: Methods and Techniques; New Age International Publisher: New Delhi, India, 2013. [Google Scholar]
- World Development Indicators. 2019. Available online: https://databank.worldbank.org/ (accessed on 13 April 2020).
- Population of Cities in Bangladesh. 2019. Available online: http://worldpopulationreview.com/countries/bangladesh-population/cities/ (accessed on 25 April 2020).
- Jager, J.; Putnick, D.L.; Bornstein, M.H. More than just convenient: The scientific merits of homogeneous convenience samples. Monogr. Soc. Res. Child Dev. 2017, 82, 13–30. [Google Scholar] [CrossRef]
- Pierce, M.; McManus, S.; Jessop, C.; John, A.; Hotopf, M.; Ford, T.; Hatch, S.; Wessely, S.; Abel, K.M. Says who? The significance of sampling in mental health surveys during COVID-19. Lancet Psychiatry 2020, 7, 567–568. [Google Scholar] [CrossRef]
- Paul, A. HIV/AIDS in Bangladesh and Present Research. In HIV/AIDS in Bangladesh; Global Perspectives on Health Geography; Springer: Berlin, Germany, 2020; pp. 1–25. [Google Scholar]
- Ahmed, T.; Rizvi, S.J.R.; Rasheed, S.; Iqbal, M.; Bhuiya, A.; Standing, H.; Bloom, G.; Waldman, L. Digital Health and Inequalities in Access to Health Services in Bangladesh: Mixed Methods Study. Jmir Mhealth Uhealth 2020, 8, e16473. [Google Scholar] [CrossRef] [PubMed]
- Hassan, T.; Alam, M.M.; Wahab, A.; Hawlader, M.D. Prevalence and associated factors of internet addiction among young adults in Bangladesh. J. Egypt. Public Health Assoc. 2020, 95, 3. [Google Scholar] [CrossRef] [PubMed]
- Ke, J.; Ouyang, Y.-Q.; Redding, S.R. Family-centered breastfeeding education to promote primiparas’ exclusive breastfeeding in China. J. Hum. Lact. 2018, 34, 365–378. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Ouyang, Y.-Q.; Redding, S.R. Previous breastfeeding experience and its influence on breastfeeding outcomes in subsequent births: A systematic review. Women Birth 2019, 32, 303–309. [Google Scholar] [CrossRef] [PubMed]
- WHO Infants under Six Months of Age Exclusively Breastfed. Available online: http://www.who.int/gho/child_health/prevention/breastfeeding_text/en/ (accessed on 19 September 2020).
- Emmanuel, A.; Clow, S.E. A questionnaire for assessing breastfeeding intentions and practices in Nigeria: Validity, reliability and translation. Bmc Pregnancy Childbirth 2017, 17, 174. [Google Scholar] [CrossRef] [PubMed]
- Nommsen-Rivers, L.A.; Dewey, K.G. Development and validation of the infant feeding intentions scale. Matern. Child Health J. 2009, 13, 334–342. [Google Scholar] [CrossRef]
- de la Mora, A.; Russell, D.W.; Dungy, C.I.; Losch, M.; Dusdieker, L. The Iowa Infant Feeding Attitude Scale: Analysis of Reliability and Validity1. J. Appl. Soc. Psychol. 1999, 29, 2362–2380. [Google Scholar] [CrossRef]
- Guo, Y.; Kopec, J.A.; Cibere, J.; Li, L.C.; Goldsmith, C.H. Population survey features and response rates: A randomized experiment. Am. J. Public Health 2016, 106, 1422–1426. [Google Scholar] [CrossRef]
- Blackstock, O.J.; Moore, B.A.; Berkenblit, G.V.; Calabrese, S.K.; Cunningham, C.O.; Fiellin, D.A.; Patel, V.V.; Phillips, K.A.; Tetrault, J.M.; Shah, M. A cross-sectional online survey of HIV pre-exposure prophylaxis adoption among primary care physicians. J. Gen. Intern. Med. 2017, 32, 62–70. [Google Scholar] [CrossRef]
- Stolzmann, K.; Meterko, M.; Miller, C.J.; Belanger, L.; Seibert, M.N.; Bauer, M.S. Survey response rate and quality in a mental health clinic population: Results from a randomized survey comparison. J. Behav. Health Serv. Res. 2019, 46, 521–532. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis, 6th ed.; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2006. [Google Scholar]
- O’brien, R.M. A caution regarding rules of thumb for variance inflation factors. Qual. Quant. 2007, 41, 673–690. [Google Scholar] [CrossRef]
- Kock, N. Common method bias in PLS-SEM: A full collinearity assessment approach. Int. J. E-Collab. 2015, 11, 1–10. [Google Scholar] [CrossRef]
- Vishwanath, A. Common Method Bias. Int. Encycl. Commun. Res. Methods 2017, 1–5. [Google Scholar] [CrossRef]
- Bozionelos, N. Evidence on Common Method Bias: Time to Begin to Think of Leaving the Myth Behind? Acad. Manag. Proc. 2018, 2018, 17866. [Google Scholar] [CrossRef]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM); Sage Publications: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Khayer, A.; Talukder, M.S.; Bao, Y.; Hossain, M.N. Cloud computing adoption and its impact on SMEs’ performance for cloud supported operations: A dual-stage analytical approach. Technol. Soc. 2020, 60, 101225. [Google Scholar] [CrossRef]
- Teo, A.-C.; Tan, G.W.-H.; Ooi, K.-B.; Hew, T.-S.; Yew, K.-T. The effects of convenience and speed in m-payment. Ind. Manag. Data Syst. 2015, 115, 311–331. [Google Scholar] [CrossRef]
- Bhowmik, J.; Biswas, R.; Woldegiorgis, M. Antenatal care and skilled birth attendance in Bangladesh are influenced by female education and family affordability: BDHS 2014. Public Health 2019, 170, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Su, M.; Ouyang, Y.-Q. Father’s role in breastfeeding promotion: Lessons from a quasi-experimental trial in China. Breastfeed. Med. 2016, 11, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Ooi, K.-B.; Lee, V.-H.; Tan, G.W.-H.; Hew, T.-S.; Hew, J.-J. Cloud computing in manufacturing: The next industrial revolution in Malaysia? Expert Syst. Appl. 2018, 93, 376–394. [Google Scholar] [CrossRef]
- Henseler, J. Partial least squares path modeling. In Advanced Methods for Modeling Markets; Springer: Berlin/Heidelberg, Germany, 2017; pp. 361–381. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Structural Equation Models with Unobservable Variables and Measurement Error: Algebra and Statistics; SAGE Publications Sage CA: Los Angeles, CA, USA, 1981. [Google Scholar]
- Henseler, J.; Ringle, C.M.; Sarstedt, M. A new criterion for assessing discriminant validity in variance-based structural equation modeling. J. Acad. Mark. Sci. 2015, 43, 115–135. [Google Scholar] [CrossRef]
- Henseler, J.; Ringle, C.M.; Sinkovics, R.R. The use of partial least squares path modeling in international marketing. In New Challenges to International Marketing; Emerald Group Publishing Limited: Bingley, UK, 2009; pp. 277–319. [Google Scholar] [CrossRef]
- Ab Hamid, M.; Sami, W.; Sidek, M.M. Discriminant validity assessment: Use of Fornell & Larcker criterion versus HTMT criterion. J. Phys. Conf. Ser. 2017, 890, 012163. [Google Scholar]
- Radzyminski, S.; Callister, L.C. Mother’s beliefs, attitudes, and decision making related to infant feeding choices. J. Perinat. Educ. 2016, 25, 18. [Google Scholar] [CrossRef]
- Haider, R.; Thorley, V. Supporting Exclusive Breastfeeding Among Factory Workers and Their Unemployed Neighbors: Peer Counseling in Bangladesh. J. Hum. Lact. 2020, 36, 414–425. [Google Scholar] [CrossRef]




| Variables | Delivery Mode | p-Value | ||
|---|---|---|---|---|
| Cesarean Delivery n = 121 n (%) | Vaginal Delivery n = 211 n (%) | |||
| Age | 18–25 Years | 5 (41.7%) | 7 (58.3%) | 0.425 |
| 26–33 Years | 59 (34.3%) | 113 (65.7%) | ||
| 34–41 Years | 56 (38.9%) | 88 (61.1%) | ||
| 42–49 Years | 1 (25.0%) | 3 (75.0%) | ||
| Number of Living Children | 1 Children | 83 (35.8%) | 149 (6.2%) | 0.547 |
| 2 Children’s | 31 (39.2%) | 48 (60.8%) | ||
| 3 Children’s | 7 (36.8%) | 12 (63.2%) | ||
| 4 Children’s | 0 (0.0%) | 2 (100.0%) | ||
| Resident of the Division | Sylhet | 3 (37.5%) | 5 (62.5%) | 0.290 |
| Mymensingh | 1 (16.7%) | 5 (83.3%) | ||
| Khulna | 14 (41.2%) | 20 (58.8%) | ||
| Rangpur | 3 (30.0%) | 7 (70.0%) | ||
| Chittagong | 18 (40.0%) | 27 (60.0%) | ||
| Barisal | 0 (0.0%) | 7 (100.0%) | ||
| Rajshahi | 8 (42.1%) | 11 (57.9%) | ||
| Dhaka | 74 (36.5%) | 129 (63.5%) | ||
| Religion | Christians | 3 (25.0%) | 9 (75.0%) | 0.683 |
| Buddhism | 1 (25.0%) | 3 (75.0%) | ||
| Hindu | 18 (41.9%) | 25 (58.1%) | ||
| Islam | 99 (36.3%) | 174 (63.7%) | ||
| Profession | Searching for work | 11 (33.3%) | 22 (66.7%) | 0.947 |
| Housewife | 28 (36.8%) | 48 (63.2%) | ||
| Public Sector Employee | 41 (35.3%) | 75 (64.7%) | ||
| Corporate Employee | 41 (38.3%) | 66 (61.7%) | ||
| Education | Less than high school degree (Less than SSC) | 9 (45.0%) | 11 (55.0%) | 0.699 |
| High school degree (HSC) | 21 (31.8%) | 45 (68.2%) | ||
| Bachelor degree | 26 (35.1%) | 48 (64.9%) | ||
| Masters’ degree and above | 65 (37.8%) | 107 (62.2%) | ||
| Income Per Month | <$100 | 41 (36.3%) | 72 (63.7%) | 0.410 |
| $100–$300 | 18 (47.4%) | 20 (52.6%) | ||
| $300–$500 | 38 (35.8%) | 68 (64.2%) | ||
| $500–$800 | 20 (35.7%) | 36 (64.3%) | ||
| >$800 | 4 (23.5%) | 13 (76.5%) | ||
| F.Know | Fathers’ Knowledge on EBF | M.Int | Mothers’ Intention to EBF Practice |
| F.Att | Fathers’ Attitude to Support EBF | M. Att | Mother’s attitude to EBF |
| F.Supp | Fathers’ Support to EBF | M.PC | Mothers’ Perceived Control |
| M.Know | Mothers’ Knowledge on EBF | M.SN | Mothers’ subjective norms |
| M.Exp | Mothers’ Own Breastfeeding Experience | M.SE | Mothers’ Self-Efficacy |
| EBF | EBF Practice |
| Constructs | F.Know | F.Att | F.Supp | M.Know | M.Exp | EBF | M.Int | M.Att | M.PC | M.SN | M.SE |
|---|---|---|---|---|---|---|---|---|---|---|---|
| F.Know | 0.817 | ||||||||||
| F.Att | −0.181 | 0.762 | |||||||||
| F.Supp | 0.419 | −0.109 | 0.789 | ||||||||
| M.Know | 0.711 | −0.226 | 0.268 | 0.830 | |||||||
| M.Exp | 0.063 | 0.070 | 0.057 | 0.018 | 1.000 | ||||||
| EBF | 0.339 | −0.224 | 0.243 | 0.368 | 0.011 | 0.759 | |||||
| M.Int | 0.124 | −0.122 | 0.311 | 0.191 | −0.056 | 0.401 | 0.796 | ||||
| M.Att | −0.148 | 0.370 | −0.107 | −0.101 | 0.011 | −0.157 | 0.385 | 0.772 | |||
| M.PC | 0.346 | −0.248 | 0.237 | 0.416 | 0.005 | 0.821 | 0.415 | −0.149 | 0.768 | ||
| M.SN | 0.500 | −0.355 | 0.348 | 0.607 | 0.068 | 0.253 | 0.035 | −0.290 | 0.292 | 0.799 | |
| M.SE | −0.181 | −0.120 | −0.044 | 0.062 | 0.009 | −0.118 | −0.158 | −0.202 | −0.090 | 0.486 | 0.808 |
| Constructs | Item Loading Range | Cronbach’s Alpha | rho_A | Composite Reliability | AVE |
|---|---|---|---|---|---|
| F.Know | 0.763–0.857 | 0.929 | 0.931 | 0.941 | 0.668 |
| F.Att | 0.722–0.799 | 0.952 | 0.953 | 0.957 | 0.581 |
| F.Supp | 0.722–0.842 | 0.853 | 0.881 | 0.892 | 0.623 |
| M.Know | 0.761–0.889 | 0.935 | 0.938 | 0.946 | 0.689 |
| M.Exp | 1.000–1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
| EBF | 0.707–0.817 | 0.918 | 0.920 | 0.931 | 0.576 |
| M.Int | 0.754–0.84 | 0.855 | 0.858 | 0.896 | 0.634 |
| M.Att | 0.726–0.814 | 0.955 | 0.955 | 0.959 | 0.596 |
| M.PC | 0.722–0.817 | 0.900 | 0.902 | 0.920 | 0.590 |
| M.SN | 0.772–0.824 | 0.887 | 0.889 | 0.914 | 0.639 |
| M.SE | 0.773–0.866 | 0.735 | 0.755 | 0.849 | 0.653 |
| Constructs | F.Know | F.Att | F.Supp | M.Know | M.Exp | EBF | M.Int | M.Att | M.PC | M.SN | M.SE |
|---|---|---|---|---|---|---|---|---|---|---|---|
| F.Know | |||||||||||
| F.Att | 0.193 | ||||||||||
| F.Supp | 0.465 | 0.114 | |||||||||
| M.Know | 0.761 | 0.239 | 0.295 | ||||||||
| M.Exp | 0.067 | 0.088 | 0.068 | 0.047 | |||||||
| EBF | 0.363 | 0.237 | 0.271 | 0.390 | 0.044 | ||||||
| M.Int | 0.169 | 0.148 | 0.361 | 0.237 | 0.061 | 0.452 | |||||
| M.Att | 0.170 | 0.385 | 0.115 | 0.149 | 0.048 | 0.171 | 0.425 | ||||
| M.PC | 0.375 | 0.269 | 0.265 | 0.452 | 0.045 | 1.082 | 0.472 | 0.165 | |||
| M.SN | 0.547 | 0.386 | 0.393 | 0.661 | 0.072 | 0.276 | 0.128 | 0.314 | 0.323 | ||
| M.SE | 0.220 | 0.142 | 0.076 | 0.090 | 0.025 | 0.147 | 0.196 | 0.243 | 0.112 | 0.592 |
| Hypotheses | Path | β | SD | t-Value | p-Value |
|---|---|---|---|---|---|
| H1 | M.Know->M. Att | 0.659 | 0.016 | 1.152 | 0.025 |
| H2 | M.Exp->M.Att | 0.008 | 0.018 | 0.472 | 0.637 |
| H3 | F.Know->M.Know | 0.846 | 0.013 | 63.446 | 0.000 |
| H4 | F.Know->F.Att | 0.182 | 0.031 | 5.823 | 0.000 |
| H5 | F.Att->M.SN | 0.297 | 0.033 | 9.126 | 0.000 |
| H6 | F.Att->F.Supp | 0.840 | 0.018 | 46.282 | 0.000 |
| H7 | F.Supp->M.Att | 0.886 | 0.013 | 69.099 | 0.000 |
| H8 | M.Att->M.Int | 0.142 | 0.047 | 3.035 | 0.003 |
| H9 | M.SN->M.Int | 0.097 | 0.049 | 1.980 | 0.048 |
| H10 | M.SE->M.Int | 0.692 | 0.105 | 6.574 | 0.000 |
| H11 | M.PC->M.Int | 0.719 | 0.095 | 7.572 | 0.000 |
| H12 | M.SE->EBF | 1.123 | 0.092 | 12.176 | 0.000 |
| H13 | M.PC->EBF | 1.253 | 0.078 | 15.965 | 0.000 |
| H14 | M.Int->EBF | 0.243 | 0.036 | 6.804 | 0.000 |
| Control Variables | Profession->EBF | −0.082 | 0.038 | 2.165 | 0.031 |
| Residence->EBF | −0.044 | 0.028 | 1.574 | 0.116 | |
| Education->EBF | −0.005 | 0.031 | 0.178 | 0.859 | |
| Income->EBF | 0.088 | 0.040 | 2.198 | 0.028 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ouyang, Y.-Q.; Nasrin, L. Father’s Knowledge, Attitude and Support to Mother’s Exclusive Breastfeeding Practices in Bangladesh: A Multi-Group Structural Equations Model Analysis. Healthcare 2021, 9, 276. https://doi.org/10.3390/healthcare9030276
Ouyang Y-Q, Nasrin L. Father’s Knowledge, Attitude and Support to Mother’s Exclusive Breastfeeding Practices in Bangladesh: A Multi-Group Structural Equations Model Analysis. Healthcare. 2021; 9(3):276. https://doi.org/10.3390/healthcare9030276
Chicago/Turabian StyleOuyang, Yan-Qiong, and Layla Nasrin. 2021. "Father’s Knowledge, Attitude and Support to Mother’s Exclusive Breastfeeding Practices in Bangladesh: A Multi-Group Structural Equations Model Analysis" Healthcare 9, no. 3: 276. https://doi.org/10.3390/healthcare9030276
APA StyleOuyang, Y.-Q., & Nasrin, L. (2021). Father’s Knowledge, Attitude and Support to Mother’s Exclusive Breastfeeding Practices in Bangladesh: A Multi-Group Structural Equations Model Analysis. Healthcare, 9(3), 276. https://doi.org/10.3390/healthcare9030276