
Factors Affecting Death and Severe Injury in Child Motor Vehicle Passengers



Abstract
:1. Introduction
2. Materials and Methods
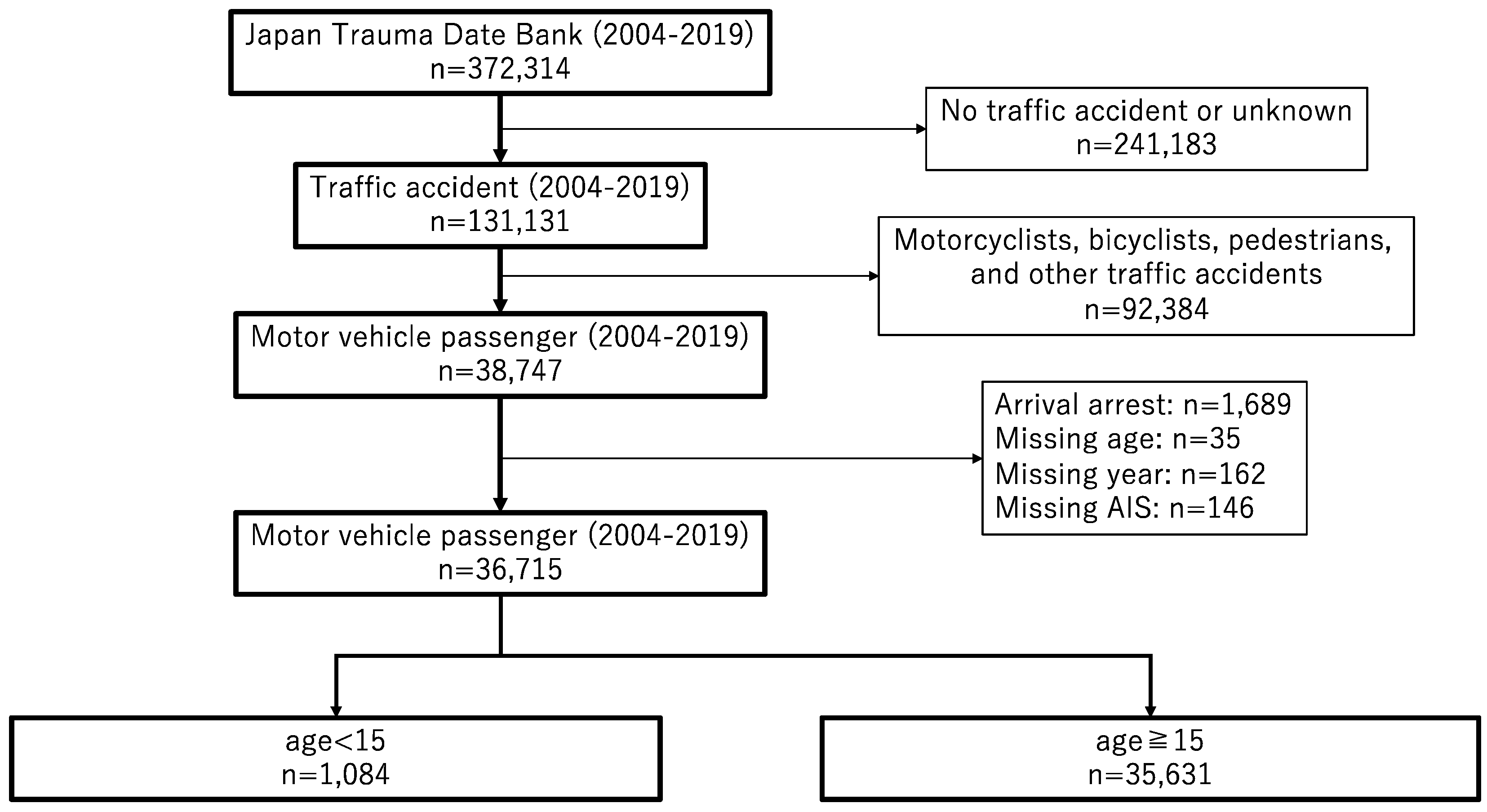
2.1. Study Design and Patient Selection
2.2. Statistical Analysis
2.3. Endpoint
3. Results
3.1. Comparison of Patients’ Outcomes
3.2. Comparison of Patients with and without Severe Injuries
3.3. Factors Affecting the Outcome
3.4. Factors Affecting Severe Injuries
4. Discussion
5. Conclusions
6. Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Global Status Report on Road Safety 2018. Available online: http://apps.who.int/iris/bitstream/handle/10665/277370/WHO-NMH-NVI-18.20-eng.pdf?ua=1 (accessed on 23 August 2021).
- Nagata, I.; Abe, T.; Uchida, M.; Saitoh, D.; Tamiya, N. Ten-year inhospital mortality trends for patients with trauma in Japan: A multicentre observational study. BMJ Open 2018, 8, e018635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hondo, K.; Shiraishi, A.; Fujie, S.; Saitoh, D.; Otomo, Y. In-hospital trauma mortality has decreased in Japan possibly due to trauma education. J. Am. Coll. Surg. 2013, 217, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Moore, L.; Turgeon, A.F.; Lauzier, F.; Emond, M. Evolution of patient outcomes over 14 years in a mature, inclusive Canadian trauma system. World J. Surg. 2015, 39, 1397–1405. [Google Scholar] [CrossRef]
- Ishii, W.; Hitosugi, M.; Takeda, A.; Baba, M.; Iizuka, R. Factors influencing vehicle passenger fatality have changed over 10 years: A nationwide hospital-based study. Sci. Rep. 2020, 10, 3316. [Google Scholar] [CrossRef] [Green Version]
- Statistics of Japan; e-Stat is a Portal Site for Japanese Government Statistics. Available online: https://www.e-stat.go.jp/en/stat-search/files?page=1&layout=datalist&toukei=00450011&tstat=000001028897&cycle=7&year=19890&month=0&tclass1=000001053058&tclass2=000001053061&tclass3=000001053072&result_back=1&tclass4val=0 (accessed on 28 June 2021).
- Ministry of Health. Labour and Welfare. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/jinkou/geppo/nengai20/index.html (accessed on 13 August 2021).
- Traffic Safety Measures in Japan. Available online: https://www.mlit.go.jp/road/management-e/e_pdf/0403_5.pdf (accessed on 6 August 2021).
- Cabinet Office, Government of Japan. Basic Traffic Safety Plan. Available online: https://www8.cao.go.jp/koutu/kihon/keikaku11/pdf/kihon_keikaku.pdf (accessed on 23 August 2021).
- Cabinet Office, Government of Japan. Basic Traffic Safety Plan. Available online: https://www8.cao.go.jp/koutu/taisaku/r02kou_haku/zenbun/genkyo/feature/feature_01_2.html (accessed on 23 August 2021).
- Kahani, A.T.; Shariat-Mohaymany, A.; Ranjbari, A. Analysis of factors associated with traffic injury severity on rural roads in Iran. J. Inj. Violence Res. 2012, 4, 36–41. [Google Scholar] [CrossRef]
- Chang, L.Y.; Wang, H.W. Analysis of traffic injury severity: An application of non-parametric classification tree techniques. Accid. Anal. Prev. 2006, 38, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Radwan, E. Analyses of rear-end crashes based on classification tree models. Traffic Inj. Prev. 2006, 7, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Durbin, D.R.; Hoffman, B.D. Child passenger safety. Pediatrics 2018, 142, e20182461. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.L.; Nance, M.L.; Arbogast, K.B. Passenger compartment intrusion as a predictor of significant injury for children in motor vehicle crashes. J. Trauma 2009, 66, 504–507. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Oda, J.; Kimura, A.; Sakamoto, Y.; Shiraishi, A.; Tanaka, K.; Tohira, H.; Nakahara, S.; Hayashi, M.; Masuno, T.; et al. Japan Trauma Date Bank Report 2020. Available online: https://www.jtcr-jatec.org/traumabank/dataroom/data/JTDB2020e.pdf (accessed on 23 August 2020).
- Japan Trauma Care and Research. Japan Trauma Data Bank Annual Report 2011–2015. Available online: http//www.jtcrjatec.org/traumabank/dataroom/date/JTDB2016.pdf (accessed on 27 June 2020).
- Yumoto, T.; Mitsuhashi, T.; Yamakawa, Y.; Iida, A.; Nosaka, N.; Tsukahara, K.; Naito, H.; Nakao, A. Impact of Cushing’s sign in the prehospital setting on predicting the need for immediate neurosurgical intervention in trauma patients: A nationwide retrospective observational study. Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 147. [Google Scholar] [CrossRef] [Green Version]
- Japan Trauma Care and Research. Japan Trauma Datebank. Available online: https//www.jtcr-jatec.org/traumabank/index.htm (accessed on 27 June 2021).
- Zeedyk, M.S.; Wallace, L.; Carcary, B.; Jones, K.; Larter, K. Children and road safety: Increasing knowledge does not improve behaviour. Br. J. Educ. Psychol. 2001, 71, 573–594. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, G. Progress in pedestrian safety research. Int. J. Inj. Control. Saf. Promot. 2020, 27, 35–43. [Google Scholar] [CrossRef]
- Alonso, F.; Esteban, C.; Tortosa, F.; Useche, S. Perception of Road Safety in Children’s Environment. Am. J. Educ. Res. 2017, 5, 273–278. [Google Scholar] [CrossRef]
- Casado-Sanz, N.; Guirao, B.; Gálvez-Pérez, D. Population ageing and rural road accidents: Analysis of accident severity in traffic crashes with older pedestrians on Spanish crosstown roads. Res. Transp. Bus. Manag. 2019, 30, 100377. [Google Scholar] [CrossRef]
- Boufous, S.; Finch, C.; Hayen, A.; Williamson, A. The impact of environmental, vehicle and driver characteristics on injury severity in older drivers hospitalized as a result of a traffic crash. J. Saf. Res. 2008, 39, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toida, C.; Muguruma, T.; Gakumazawa, M. Ten-year in-hospital mortality trends among paediatric injured patients in Japan: A nationwide observational study. Clin. Med. 2020, 9, 3273. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Fujita, T.; Nakahara, S.; Sakamoto, T. Seating position and patterns of severely injured body parts among child passengers in motor vehicle crashes: Japan as a distinct case. Int. J. Inj. Contr. Saf. Promot. 2018, 25, 427–432. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Neurological Disorders: Public Health Challenges; World Health Organization: Geneva, Switzerland, 2006; p. 164. [Google Scholar]
- Kojima, M.; Endo, A.; Shiraishi, A.; Otomo, Y. Age-related characteristics and outcomes for patients with severe trauma: Analysis of Japan’s nationwide trauma registry. Ann. Emerg. Med. 2019, 73, 281–290. [Google Scholar] [CrossRef]
- Dewan, M.C.; Mummareddy, N.; Wellons, J.C.; Bonfield, C.M. Epidemiology of global pediatric traumatic brain injury: Qualitative review. World Neurosurg. 2016, 91, 497–509.e1. [Google Scholar] [CrossRef]
- Taylor, C.A.; Bell, J.M.; Breiding, M.J.; Xu, L. Traumatic brain injury-related emergency department visits, hospitalizations, and deaths—United States, 2007 and 2013. MMWR Surveill. Summ. 2017, 66, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Lichte, P.; Andruszkow, H.; Kappe, M.; Horst, K.; Pishnamaz, M.; Hildebrand, F.; Lefering, R.; Pape, H.C.; Kobbe, P. Increased in-hospital mortality following severe head injury in young children: Results from a nationwide trauma registry. Eur. J. Med. Res. 2015, 20, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, R.J.; Curtis, K.; Foster, K. A 10-year review of child injury hospitalisations, health outcomes and treatment costs in Australia. Inj. Prev. 2018, 24, 344–350. [Google Scholar] [CrossRef] [Green Version]
- Rebecca, M.; Kate, C.; Shanley, C.; Andrew, H.; Soundappan, S.; Kellie, W.; Daniel, C. Comparative analysis of trends in paediatric trauma outcomes in New South Wales, Australia. Injury 2013, 44, 97–103. [Google Scholar] [CrossRef]
- Tesfay, K.; Assefa, M.; Zenebe, D.; Gebremicael, M.; Kebede, G.; Gebrekirstos, H. Road traffic injured patients with severe GCS and organ injury had a poor prognosis: A retrospective cohort study. BMC Public Health 2019, 19, 749. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Injury Prevention and Control: Motor Vehicle Safety. Available online: https://www.cdc.gov/transportationsafety/child_passenger_safety/cps-factsheet.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fmotorvehiclesafety%2Fchild_passenger_safety%2Fcps-factsheet.html (accessed on 13 October 2021).
- Diana, D.; Corinne, P.; Florin, J.; Erika-Andrada, B. Safety seat and seat belt use among child motor vehicle occupants, Cluj-Napoca, Romania. Inj. Prev. 2020, 26, 18–23. [Google Scholar] [CrossRef]
- Burda, J.E.; Sofroniew, M.V. Reactive gliosis and the multicellular response to CNS damage and disease. Neuron 2014, 81, 229–248. [Google Scholar] [CrossRef] [Green Version]
- Nahmani, M.; Turrigiano, G.G. Adult cortical plasticity following injury: Recapitulation of critical period mechanisms? Neuroscience 2014, 283, 4–16. [Google Scholar] [CrossRef] [Green Version]
- Purcell, N.; Reiss, R.; Eaton, J.; Kumwenda, K.; Quinsey, C.; Charles, A. Survival and Functional Outcomes at Discharge After Traumatic Brain Injury in Children versus Adults in Resource-Poor Setting. World Neurosurg. 2020, 137, e597–e602. [Google Scholar] [CrossRef]
- Luerssen, T.G.; Klauber, M.R.; Marshall, L.F. Outcome from head injury related to patient’age: A longitudinal prospective study of adult and pediatric head injury. J. Neurosurg. 1988, 68, 409–416. [Google Scholar] [CrossRef]
- Emami, P.; Czorlich, P.; Fritzsche, F.S.; Westphal, M.; Rueger, J.M.; Lefering, R.; Hoffmann, M. Impact of Glasgow Coma Scale score and pupil parameters on mortality rate and outcome in pediatric and adult severe traumatic brain injury: A retrospective, multicenter cohort study. J. Neurosurg. 2017, 126, 760–767. [Google Scholar] [CrossRef]
- Ghajar, J.; Hariri, R.J. Management of pediatric head injury. Pediatr. Clin. North. Am. 1992, 39, 1093–1125. [Google Scholar] [CrossRef]
- Nudo, R.J. Recovery after brain injury: Mechanisms and principles. Front. Hum. Neurosci. 2013, 7, 887. [Google Scholar] [CrossRef] [Green Version]
- Su, Y.R.S.; Veeravagu, A.; Grant, G. Neuroplasticity after traumatic brain injury. In Translational Research in Traumatic Brain Injury; Laskowitz, D., Grant, G., Eds.; CRC Press/Taylor and Francis Group: Boca Raton, FL, USA, 2016; Chapter 8. [Google Scholar] [PubMed]
- Sauber-Schatz, E.K.; West, B.A.; Bergen, G. Vital signs: Restraint use and motor vehicle occupant death rates among children aged 0-12 years- United States, 2002–2011. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 113–118. [Google Scholar] [PubMed]
- Berg, M.D.; Cook, L.; Corneli, H.M.; Vernon, D.D.; Dean, J.M. Effect of seating position and restraint use on injuries to children in motor vehicle crashes. Pediatrics 2000, 105, 831–835. [Google Scholar] [CrossRef] [PubMed]
- Lennon, A.; Siskind, V.; Haworth, N. Rear seat safer: Seating position, restraint use and injuries in children in traffic crashes in Victoria, Australia. Accid. Anal. Prev. 2008, 40, 829–834. [Google Scholar] [CrossRef] [Green Version]
- Durbin, D.R.; Arbogast, K.B.; Mol, E.K. Seat belt syndrome in children: A case report and review of the literature. Pediatr. Emerg. Care 2001, 17, 474–477. [Google Scholar] [CrossRef] [PubMed]
- Sauber-Schatz, E.K.; Thomas, A.M.; Cook, L.J. Motor vehicle crashes, medical outcomes, and hospital charges among children aged 1–12 years-crash outcome data evaluation system, 11 states, 2005–2008. MMWR Surveill. Summ. 2015, 64, 1–32. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Non-Fatal | Fatal | ||
|---|---|---|---|
| (n = 875) | (n = 29) | p Value | |
| Age (years) | 6.6 ± 4.1 | 3.4 ± 4.2 | <0.0001 |
| Sex, n (%) | 0.2412 | ||
| Male | 54.5 | 65.5 | |
| Female | 45.5 | 34.5 | |
| Seating position (%) | 0.7982 | ||
| Front seat passenger | 26.3 | 24.1 | |
| Rear seat passenger | 73.7 | 75.9 | |
| Systolic blood pressure (mmHg) | 116.4 ± 20.1 | 85.1 ± 41.3 | <0.001 |
| Diastolic blood pressure (mmHg) | 69.1 ± 16.2 | 55.0 ± 28.8 | <0.001 |
| Heart rate (beats/min) | 113.9 ± 28.8 | 120.4 ± 46.9 | 0.026 |
| Respiration rate (breaths/min) | 25.9 ± 9.7 | 19.5 ± 16.9 | 0.001 |
| Body temperature (°C) | 36.8 ± 0.8 | 34.8 ± 1.8 | <0.001 |
| Glasgow coma scale | 13.2 ± 3.1 | 4.3 ± 1.7 | <0.001 |
| FAST positive (%) | 11.5 | 10.0 | 0.833 |
| Non-Fatal | Fatal | ||
|---|---|---|---|
| (n = 875) | (n = 29) | p Value | |
| AIS, median (IQR) | |||
| Head ** | 1.0 (0.0–3.0) | 1.0 (0.0–3.0) | <0.001 |
| Face * | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | <0.001 |
| Neck | 0.0 (0.0–1.0) | 0.0 (0.0–1.0) | 0.912 |
| Chest ** | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.002 |
| Abdomen | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.584 |
| Spine ** | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.014 |
| Upper extremities | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.093 |
| Lower extremities | 0.0 (0.0–1.0) | 0.0 (0.0–1.0) | 0.085 |
| ISS, median (IQR) ** | 10.0 (5.0–17.0) | 25.5 (25.0–10.25) | <0.001 |
| RTS, median (IQR) * | 7.84 (6.90–7.84) | 3.80 (1.53–4.84) | <0.001 |
| TRISSPs, median (IQR) * | 0.99 (0.97–0.99) | 0.54 (0.15–0.82) | <0.001 |
| Age < 15 (2004 to 2019) | Age < 15 (2004 to 2019) | ||
|---|---|---|---|
| AIS ≥ 3 | AIS < 3 | ||
| (n = 651) | (n = 433) | p-Value | |
| Age (years) | 6.4 ± 4.3 | 6.3 ± 4.0 | 0.694 |
| Sex, n (%) | 0.544 | ||
| Male | 56.4 | 54.5 | |
| Female | 43.6 | 45.5 | |
| Seating position (%) | 0.111 | ||
| Front seat passenger | 25.2 | 29.7 | |
| Rear seat passenger | 74.8 | 70.3 | |
| Systolic blood pressure (mmHg) | 116.1 ± 23.5 | 111.7 ± 19.7 | 0.002 |
| Diastolic blood pressure (mmHg) | 68.8 ± 18.0 | 67.6 ± 12.9 | 0.268 |
| Heart rate (beats/min) | 116.7 ± 30.8 | 109.3 ± 27.3 | <0.001 |
| Respiration rate (breaths/min) | 26.2 ± 10.6 | 24.2 ± 9.1 | 0.003 |
| Body temperature (°C) | 36.7 ± 1.0 | 36.8 ± 0.7 | 0.180 |
| Glasgow coma scale | 12.2 ± 3.8 | 14.5 ± 1.5 | <0.001 |
| FAST positive (%) | 13.7 | 4.9 | <0.001 |
| Death rate (%) | 4.5 | 0.4 | 0.001 |
| Age < 15 (2004 to 2019) | Age < 15 (2004 to 2019) | ||
|---|---|---|---|
| AIS ≥ 3 | AIS < 3 | ||
| (n = 651) | (n = 433) | p Value | |
| ISS, median (IQR) * | 16.0 (10.0–22.0) | 1.0 (1.0–4.0) | <0.001 |
| RTS, median (IQR) ** | 7.55 (6.61–7.84) | 7.84 (7.55–7.84) | <0.001 |
| TRISSPs, median (IQR) ** | 0.99 (0.96–0.99) | 1.00 (1.00–1.00) | <0.001 |
| (n = 904) | ||||
|---|---|---|---|---|
| OR | Lower 95% CI | Upper 95% CI | p-Value | |
| Max AIS Head | 0.287 | 0.116 | 0.714 | 0.007 |
| GCS | 1.964 | 1.291 | 2.988 | 0.002 |
| BT | 2.578 | 1.228 | 5.415 | 0.012 |
| (n = 1084) | ||||
|---|---|---|---|---|
| OR | Lower 95% CI | Upper 95% CI | p-Value | |
| sBP | 1.012 | 1.002 | 1.022 | 0.016 |
| GCS | 0.705 | 0.636 | 0.783 | <0.001 |
| FAST | 3.236 | 1.631 | 6.423 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishii, W.; Hitosugi, M.; Baba, M.; Kandori, K.; Arai, Y. Factors Affecting Death and Severe Injury in Child Motor Vehicle Passengers. Healthcare 2021, 9, 1431. https://doi.org/10.3390/healthcare9111431
Ishii W, Hitosugi M, Baba M, Kandori K, Arai Y. Factors Affecting Death and Severe Injury in Child Motor Vehicle Passengers. Healthcare. 2021; 9(11):1431. https://doi.org/10.3390/healthcare9111431
Chicago/Turabian StyleIshii, Wataru, Masahito Hitosugi, Mineko Baba, Kenji Kandori, and Yusuke Arai. 2021. "Factors Affecting Death and Severe Injury in Child Motor Vehicle Passengers" Healthcare 9, no. 11: 1431. https://doi.org/10.3390/healthcare9111431
APA StyleIshii, W., Hitosugi, M., Baba, M., Kandori, K., & Arai, Y. (2021). Factors Affecting Death and Severe Injury in Child Motor Vehicle Passengers. Healthcare, 9(11), 1431. https://doi.org/10.3390/healthcare9111431