
Can Different Forest Structures Lead to Different Levels of Therapeutic Effects? A Systematic Review and Meta-Analysis

 , , ,
, , ,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. PICO and Eligibility Criteria
- P: All human participants (both healthy and unhealthy).
- I: Spending time in the forest or urban forest with the description of forest environment in terms of stand density and canopy density—stand density, tree density, trees/ha, basal area, canopy density, canopy openness, canopy closure, sky view factor etc.
- C: Studies with a control site or not.
- O: The studies that contained quantitative outcomes related to cognitive restoration, psychological restoration, physiological relaxation, and stress reduction.
2.2. Search Strategy
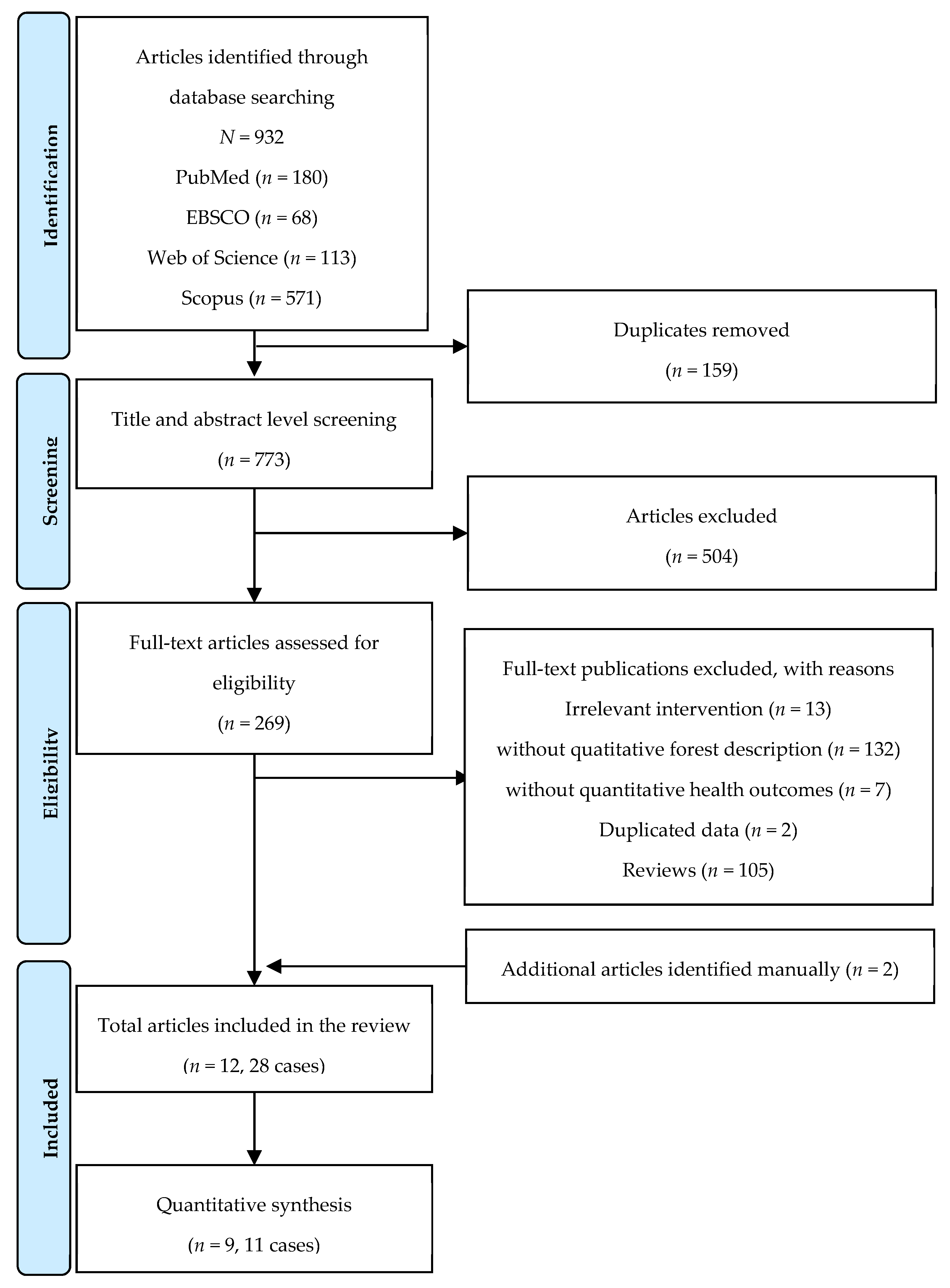
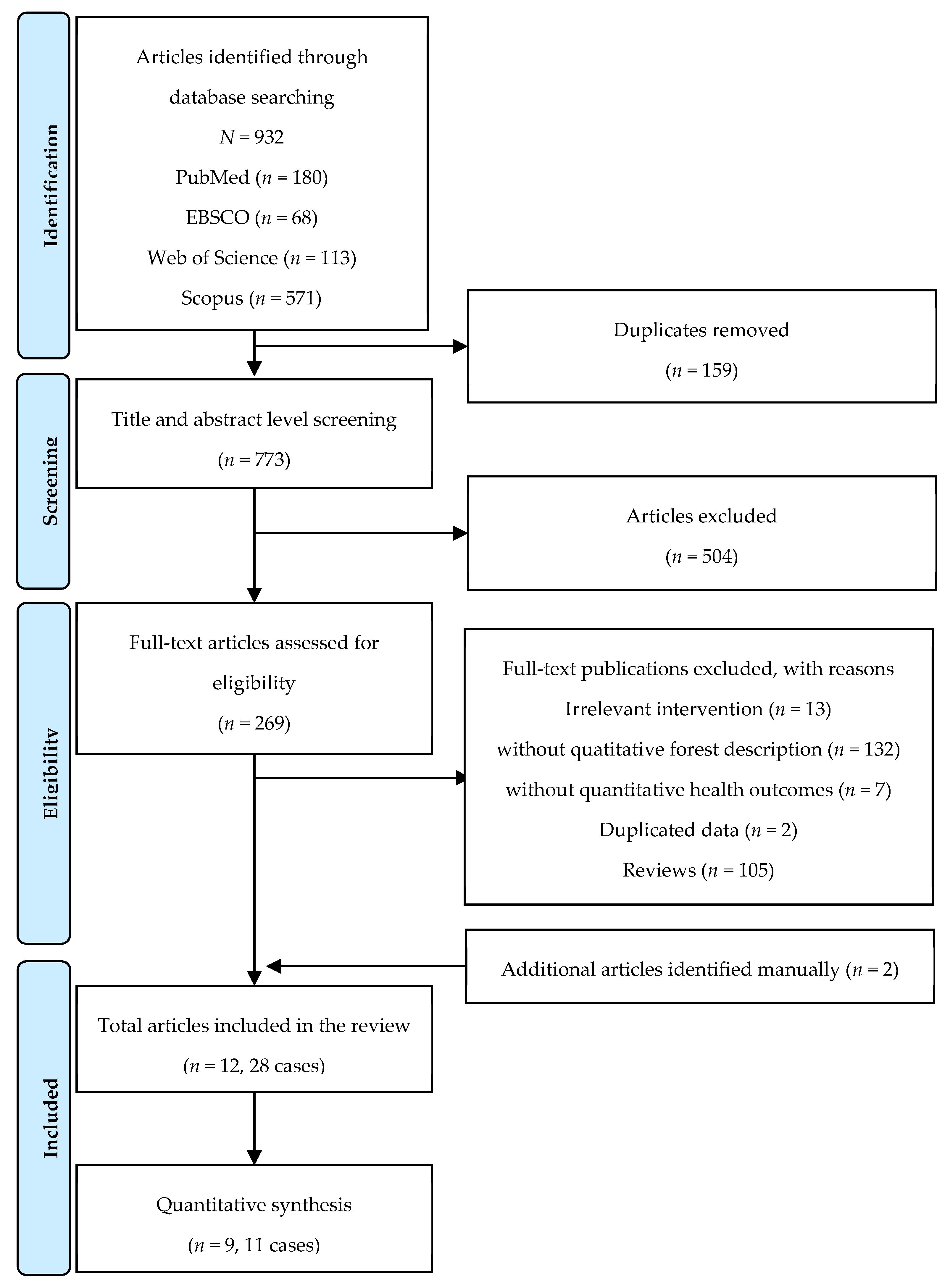
2.3. Study Selection Process
2.4. Data Extraction
- Study information: year of publication, author, country, city, study design, conducted date, time of measurement
- Samples: sample size, gender, and age
- Forest characteristics: longitude, latitude, altitude, stand density (trees/ha), canopy density (%), diameter at breast height (cm), height (m), dominant tree species
- Environmental characteristics: temperature (°C), relative humidity (%), radiant heat
- (°C), wind speed (m/s), illuminance (lx), noise level (dB)
- Intervention: activities, activity duration, and frequency
- Outcome: measurement indices, pre-measurement (M ± SD), post-measurement (M ± SD), change in measurement (M ± SD), inter-trial correlation
2.5. Methodological Quality
2.6. Statistical Analysis
2.6.1. Extracting Estimates of Effect
2.6.2. Estimating Overall Effect Size
2.6.3. Sub-Group Analysis
2.6.4. Sensitivity Analysis
3. Results
3.1. Study Characteristics
3.2. Methodological Quality
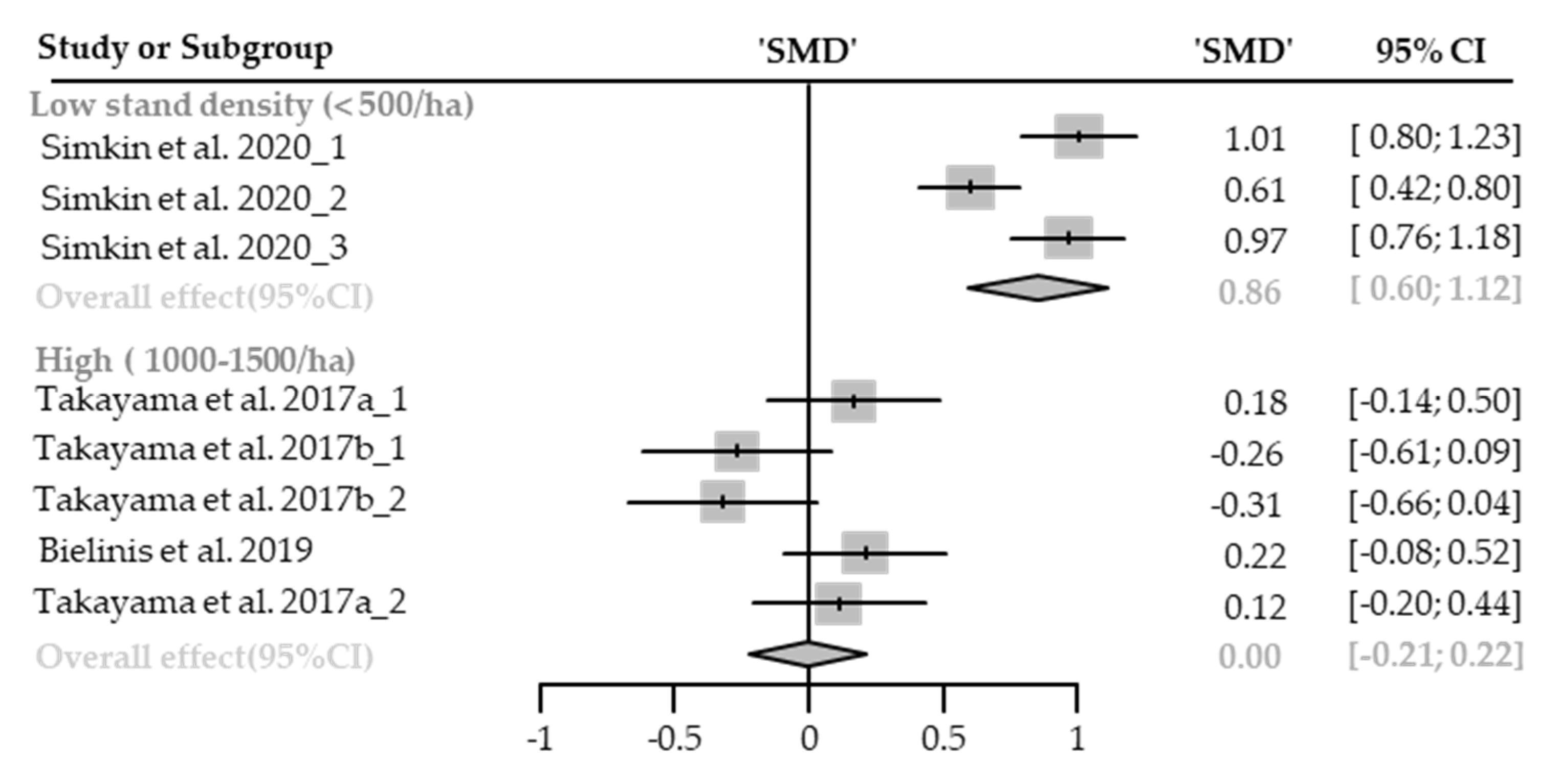
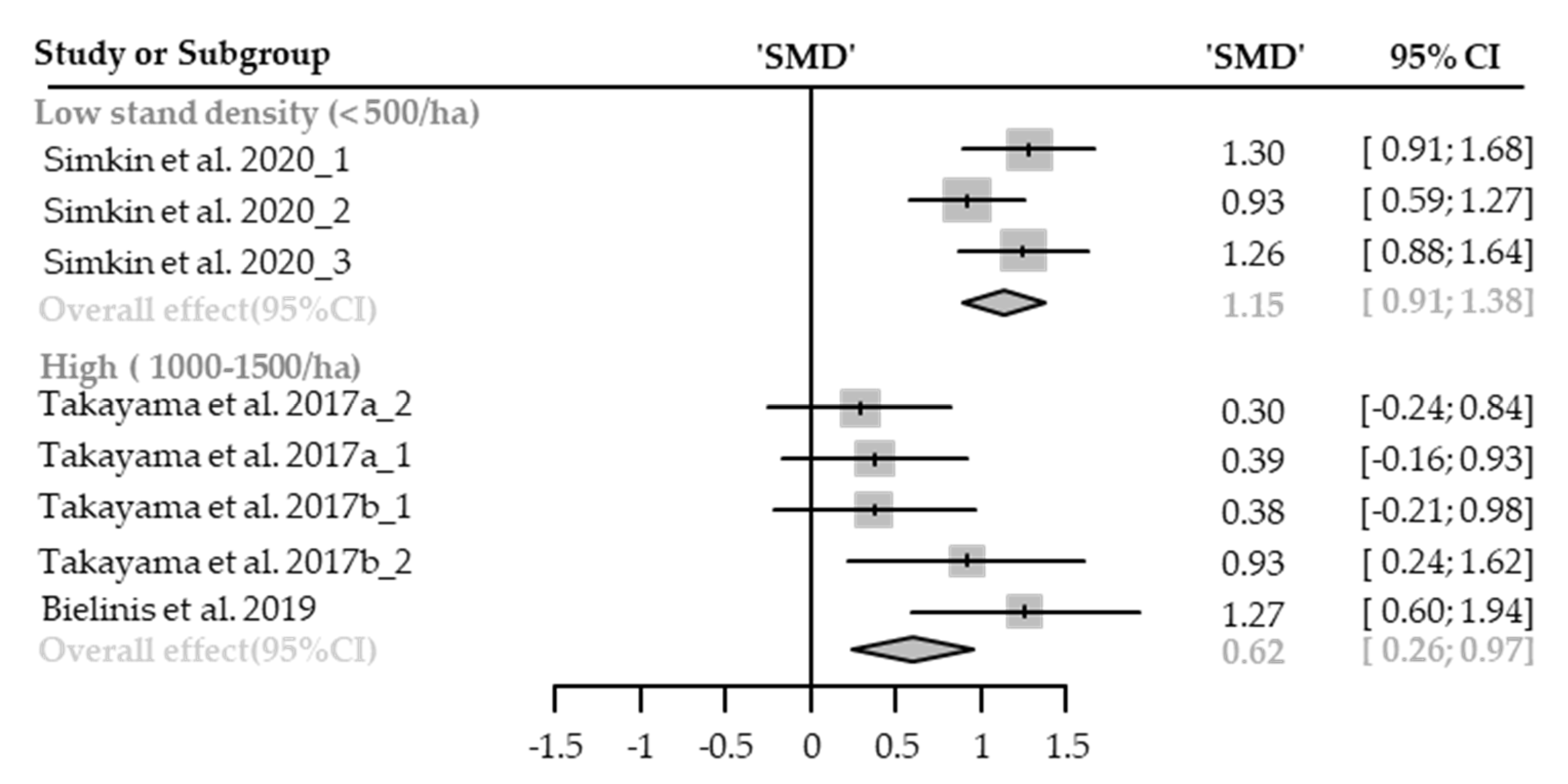
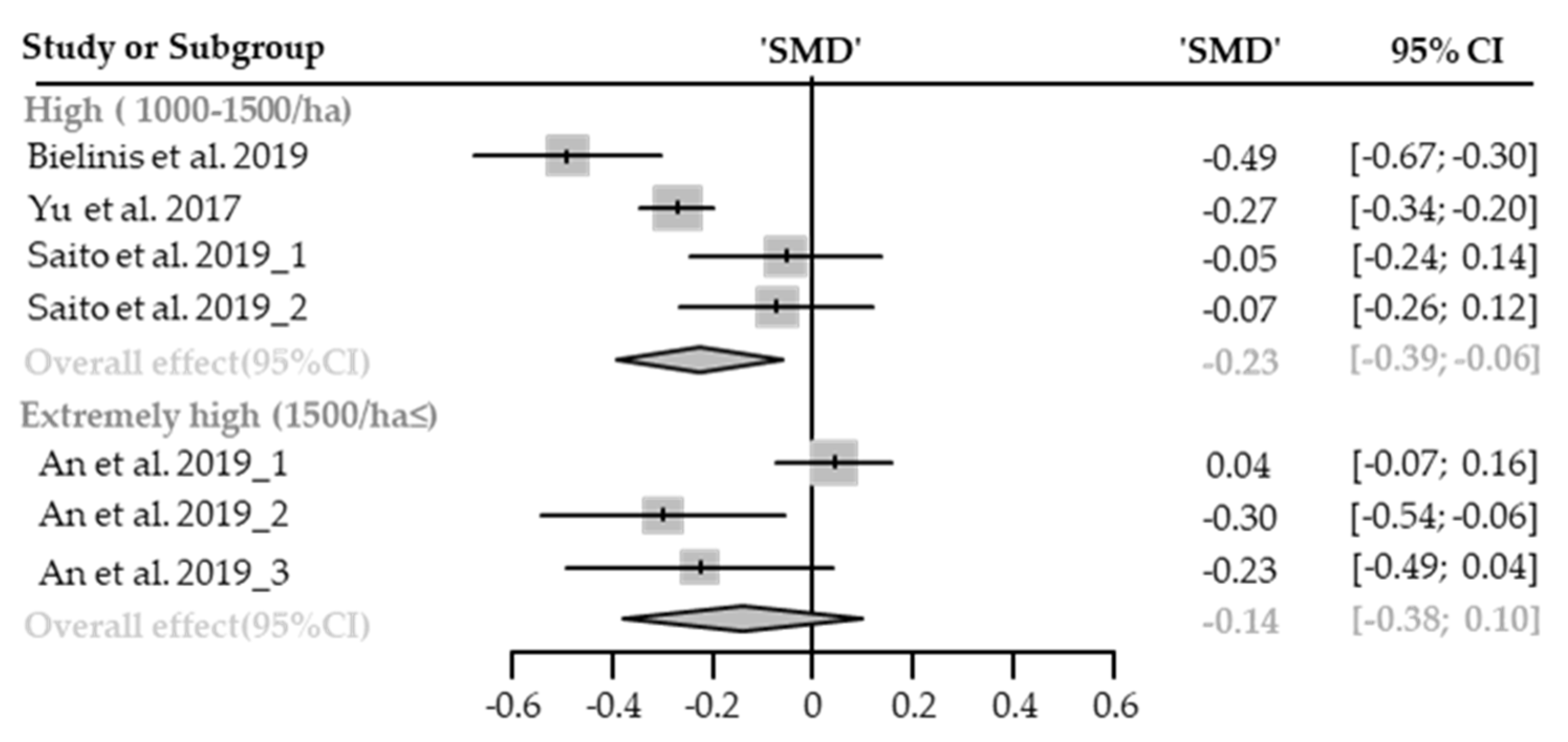
3.3. Stand Density as an Effect Modifier of Therapeutic Effect
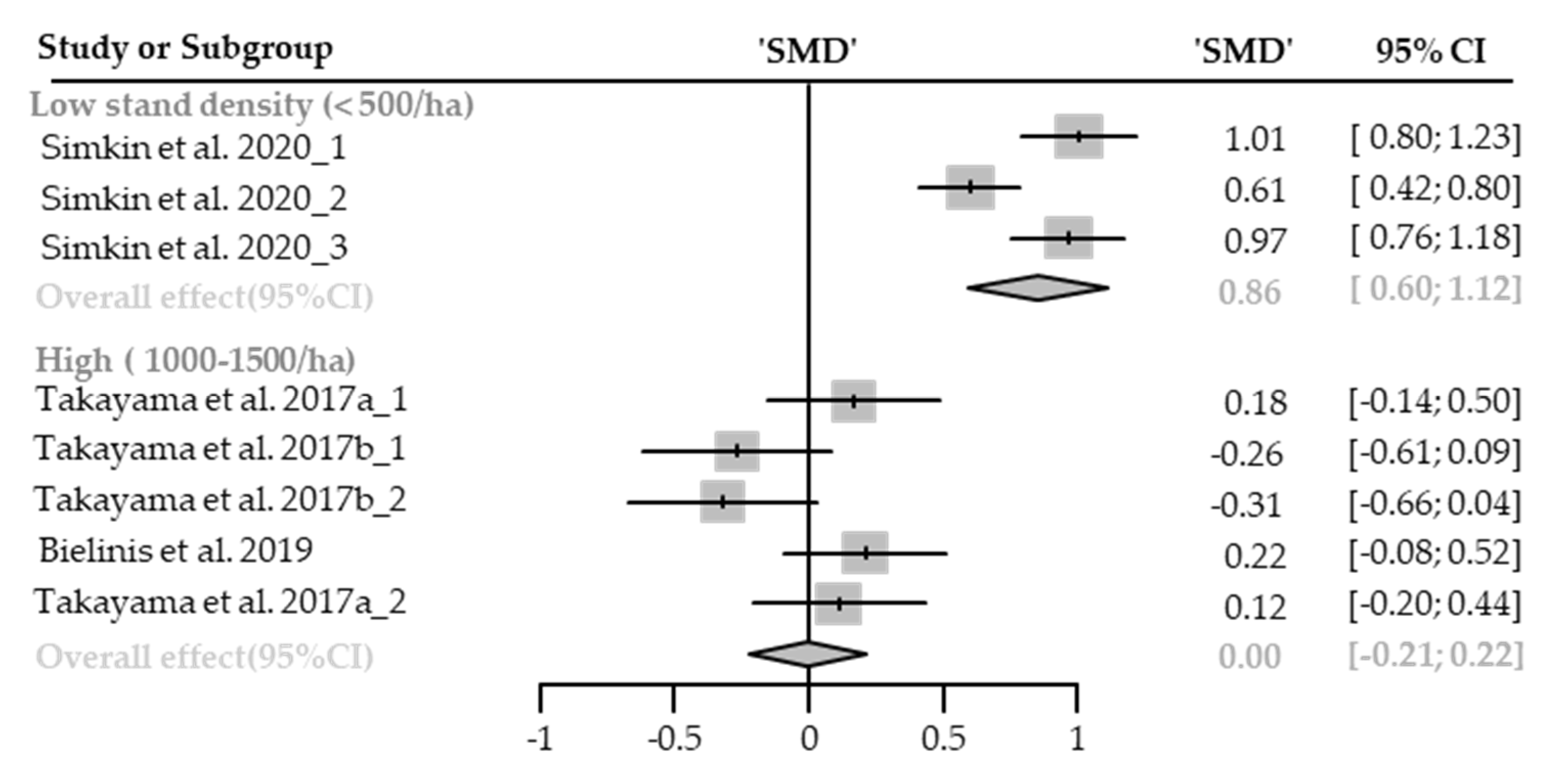
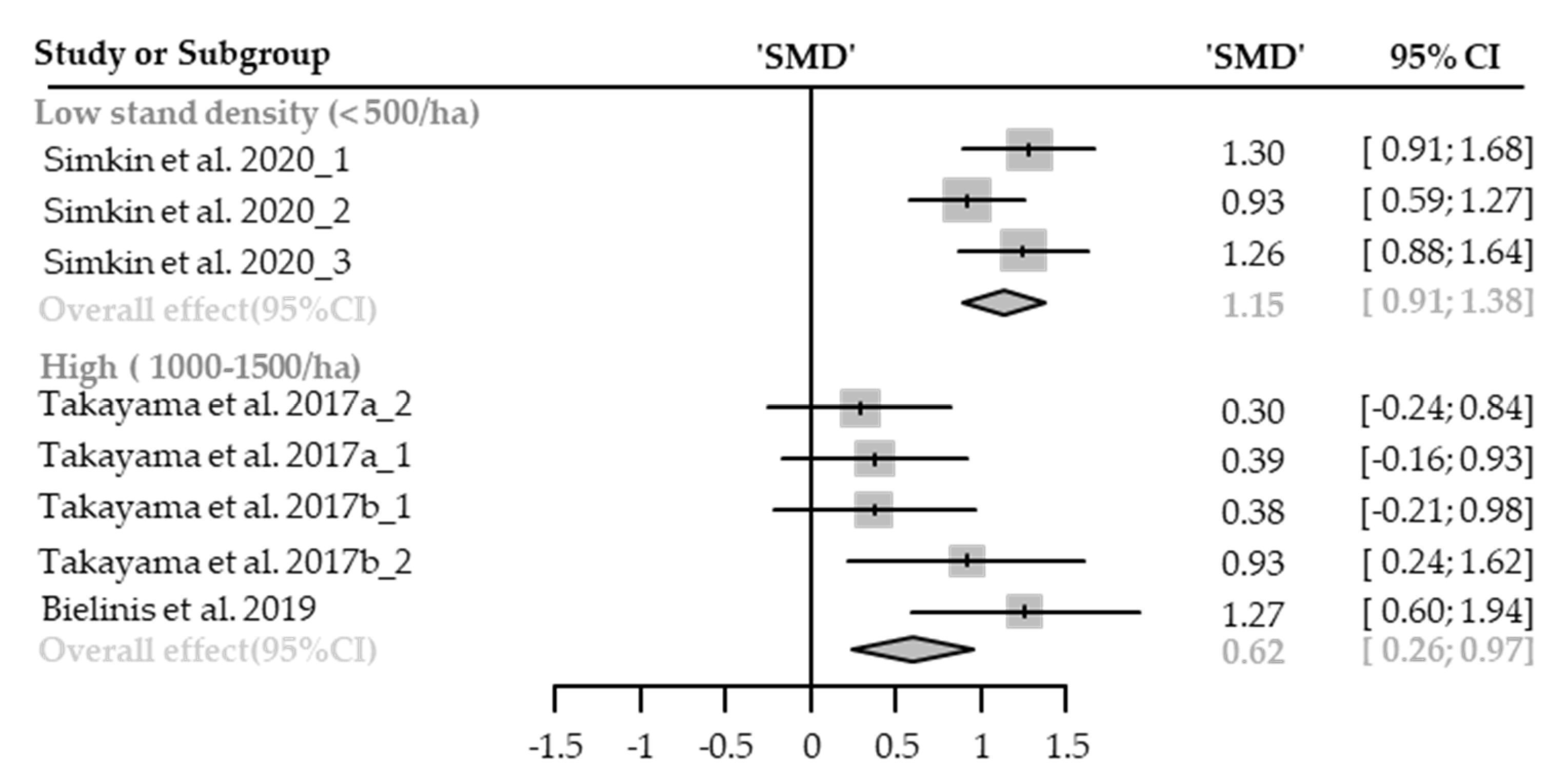
3.3.1. Emotional Restoration
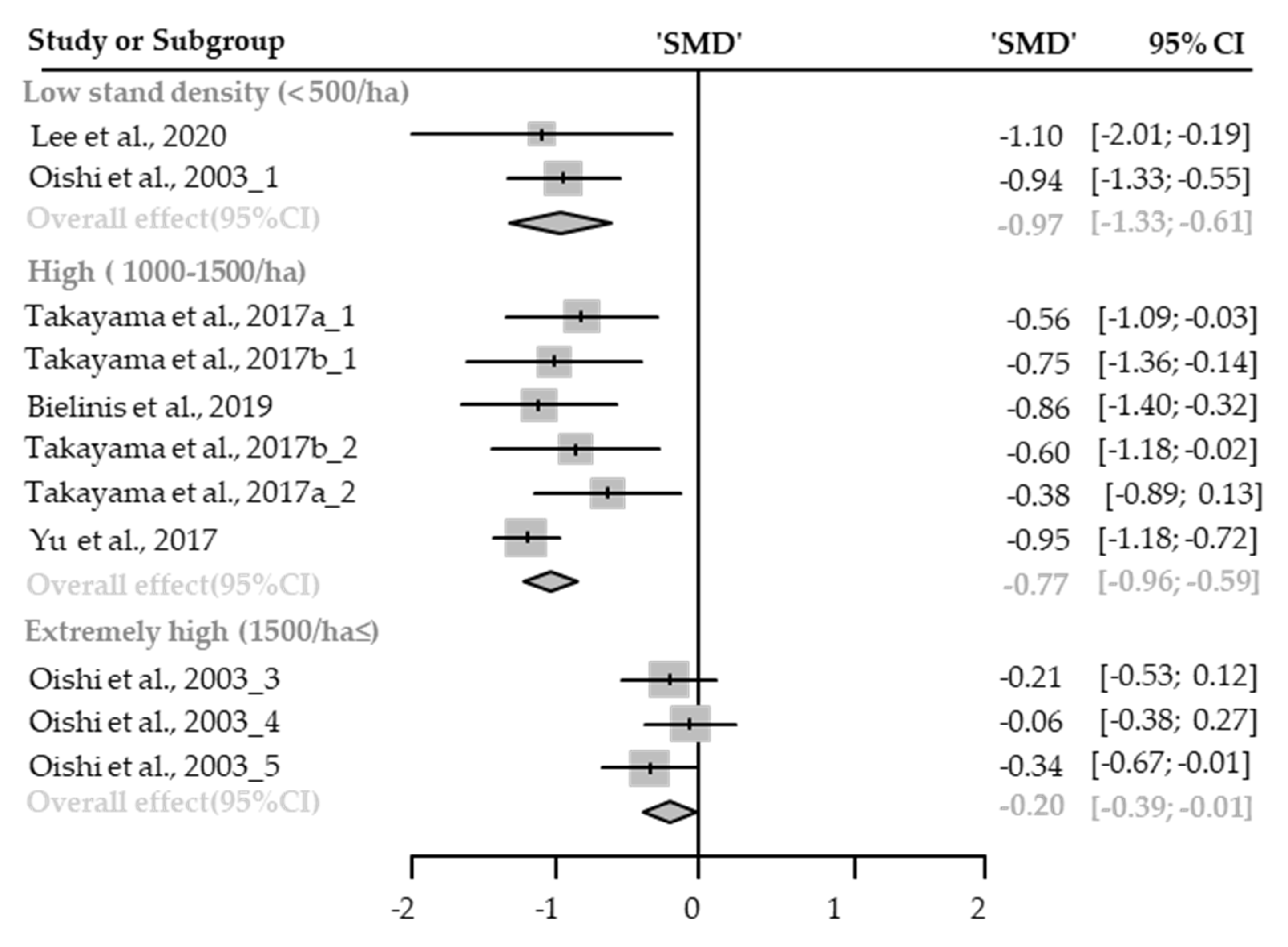
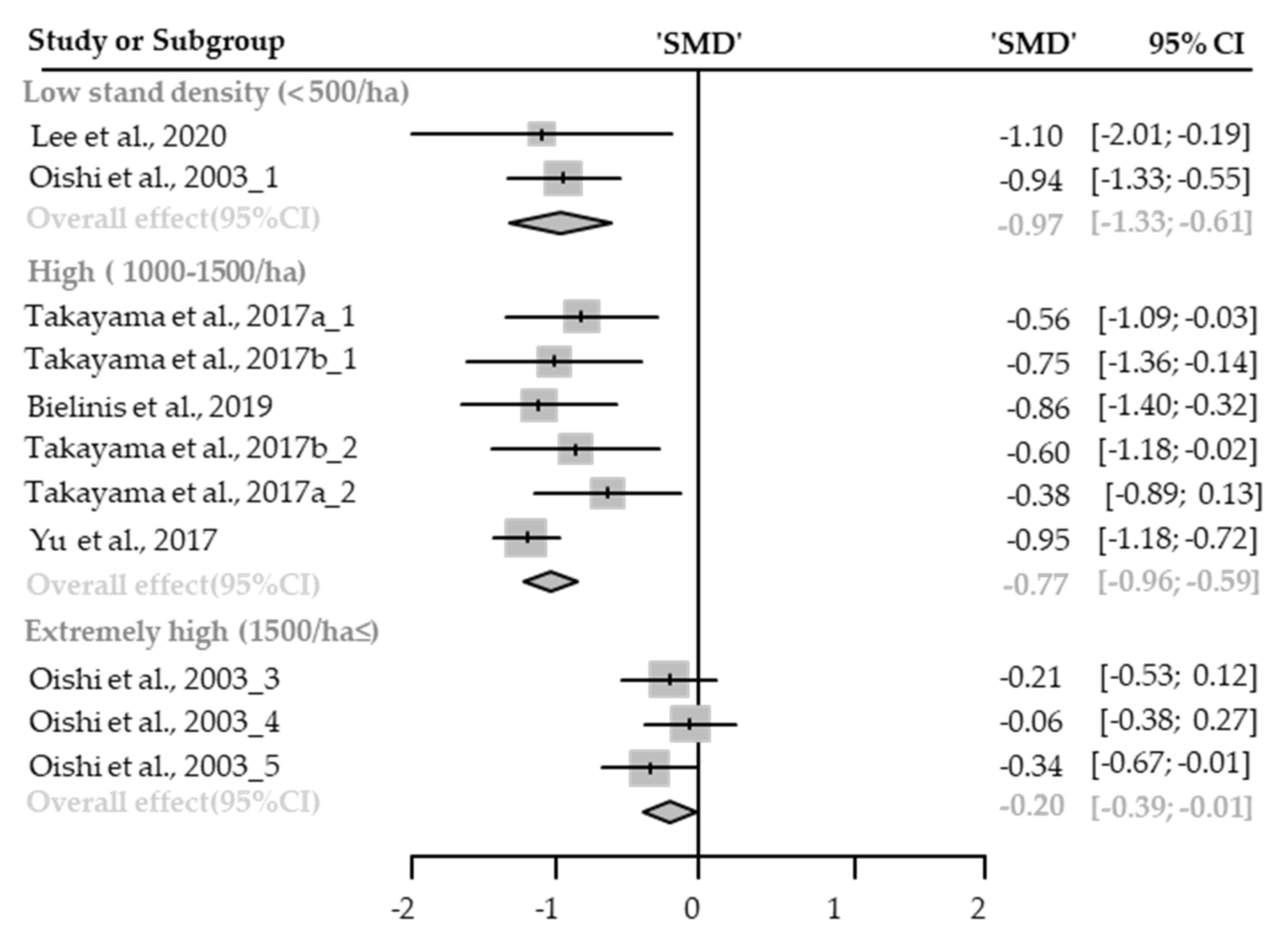
Anxiety
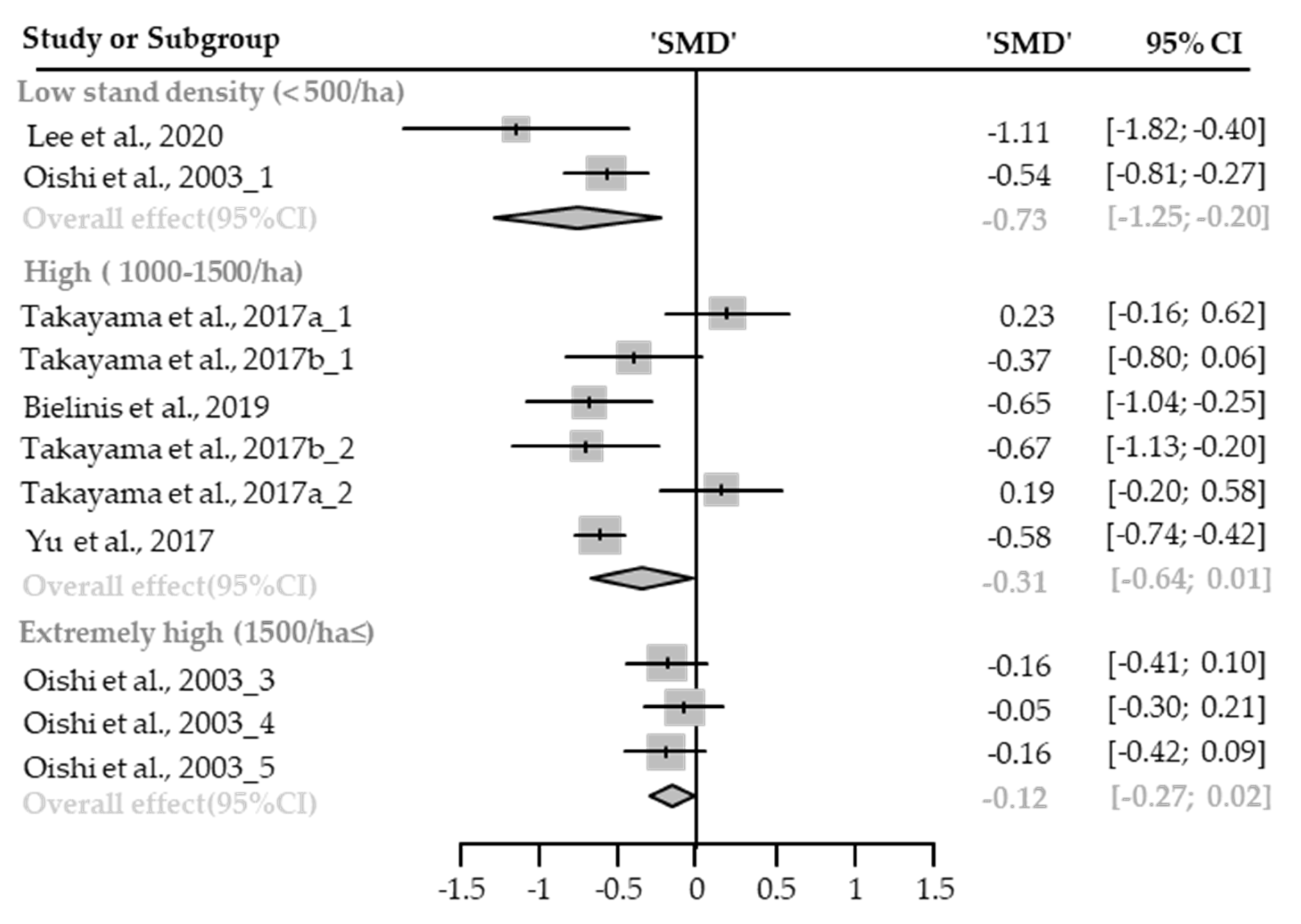
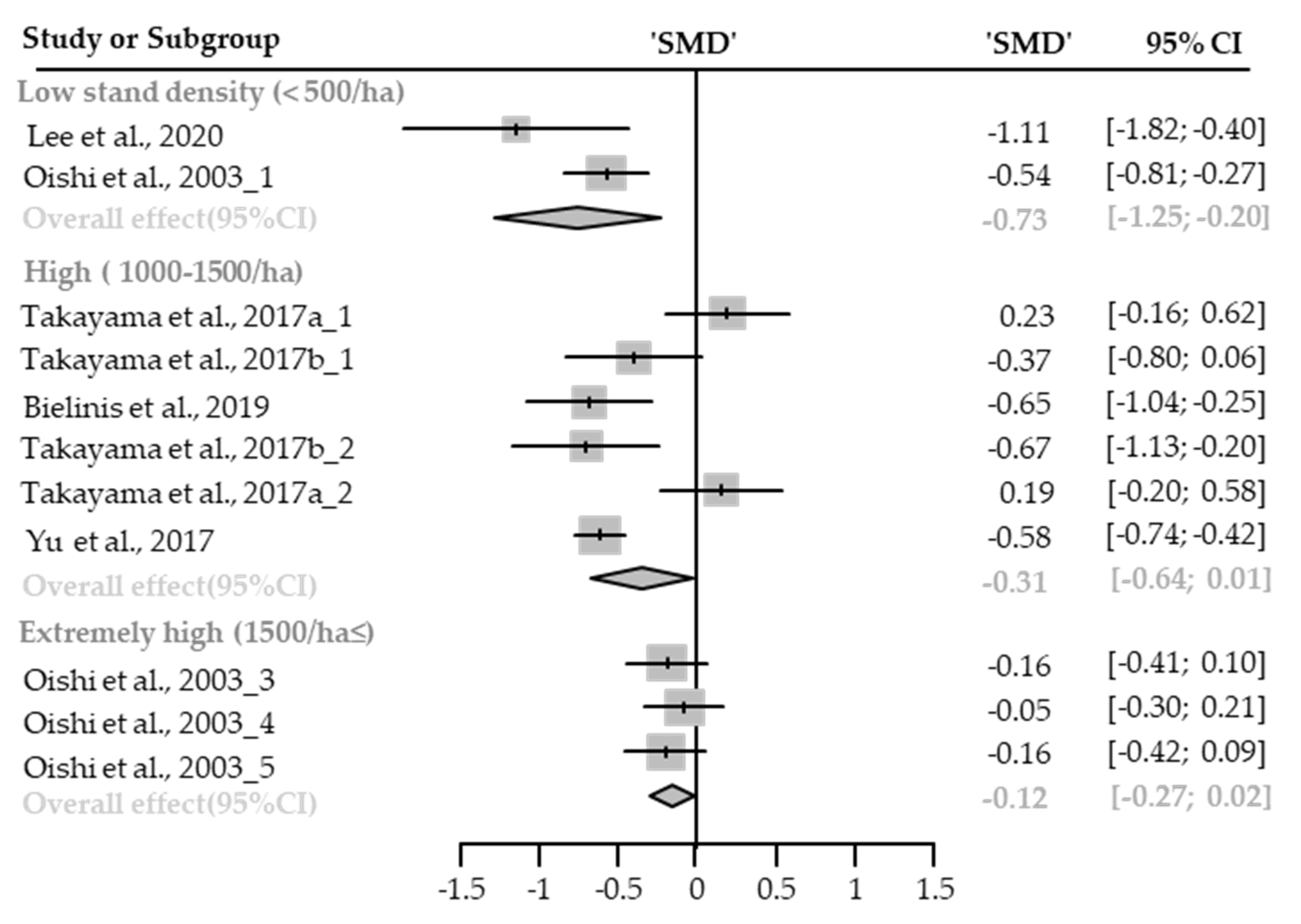
Depression
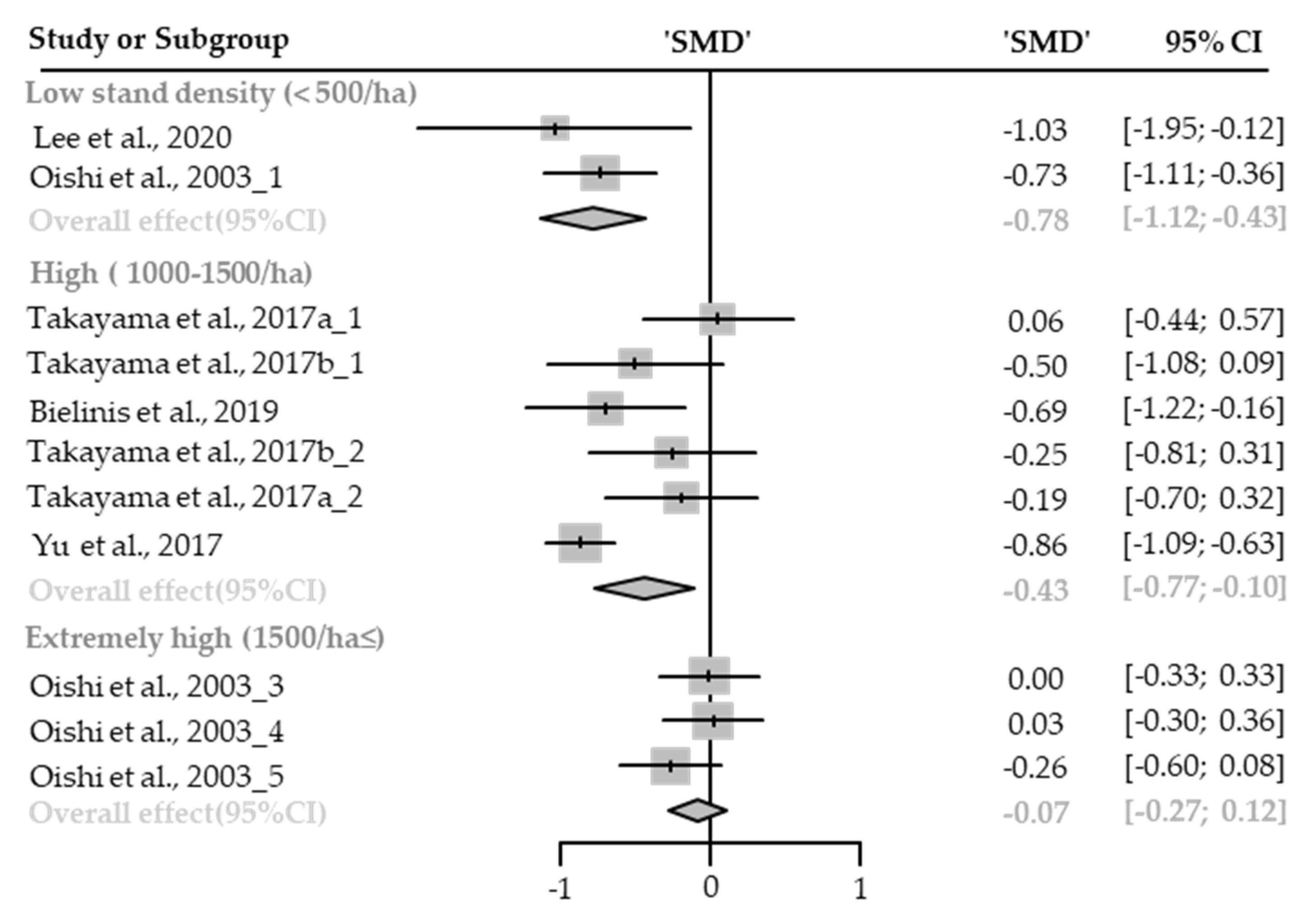
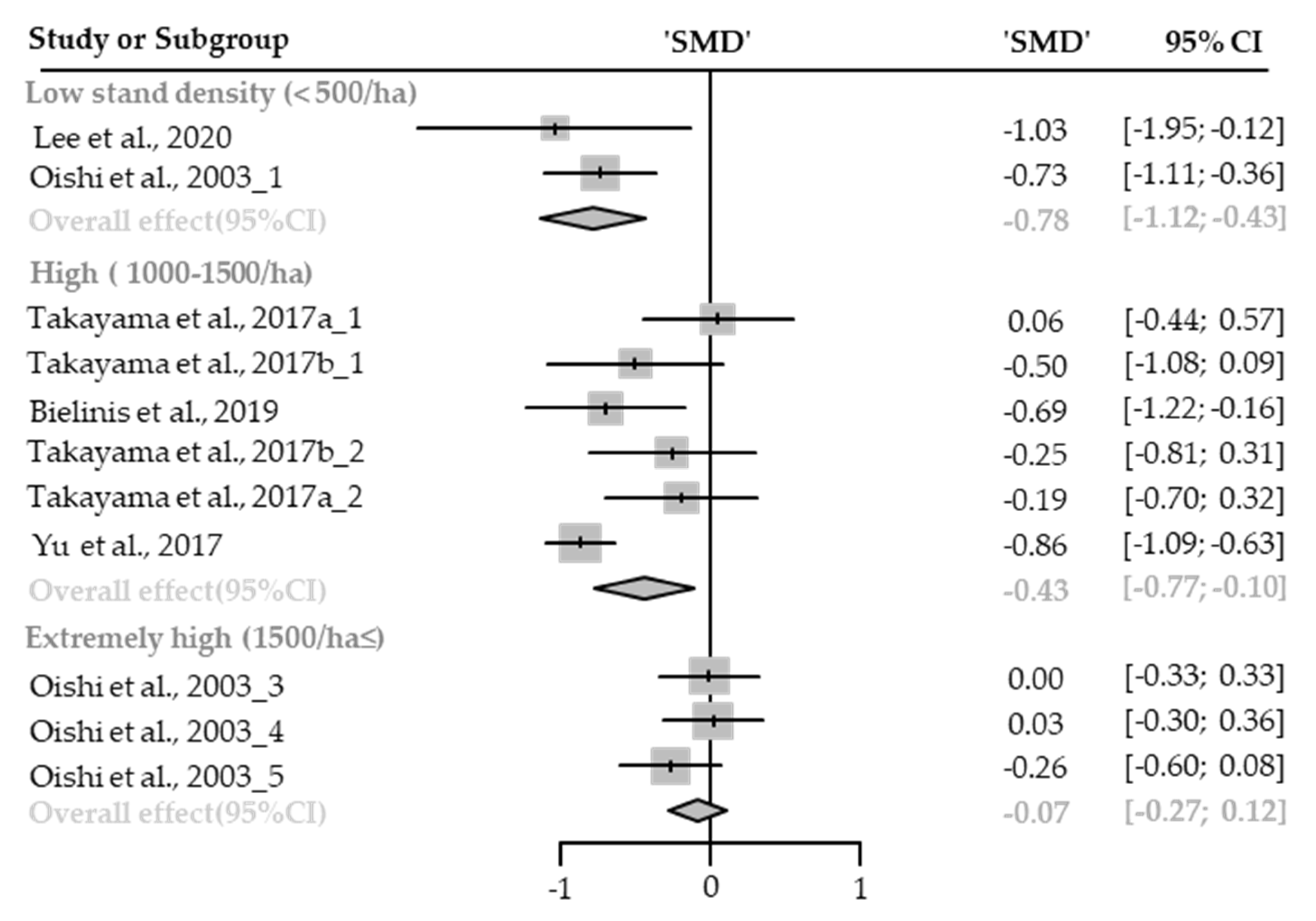
Anger
Confusion
Fatigue
Vigor
Negative Affect
Positive Affect
3.3.2. Cognitive Restoration
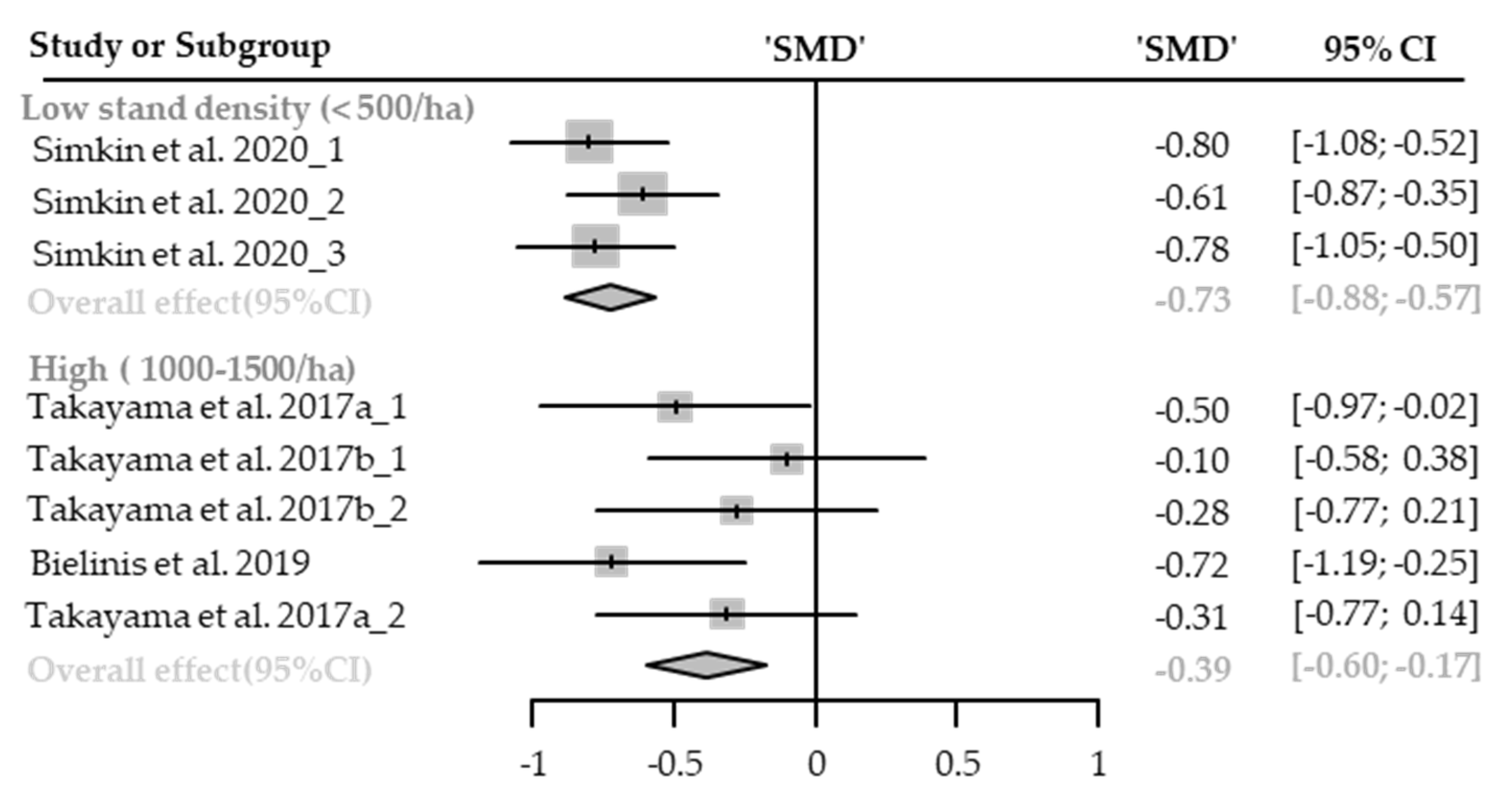
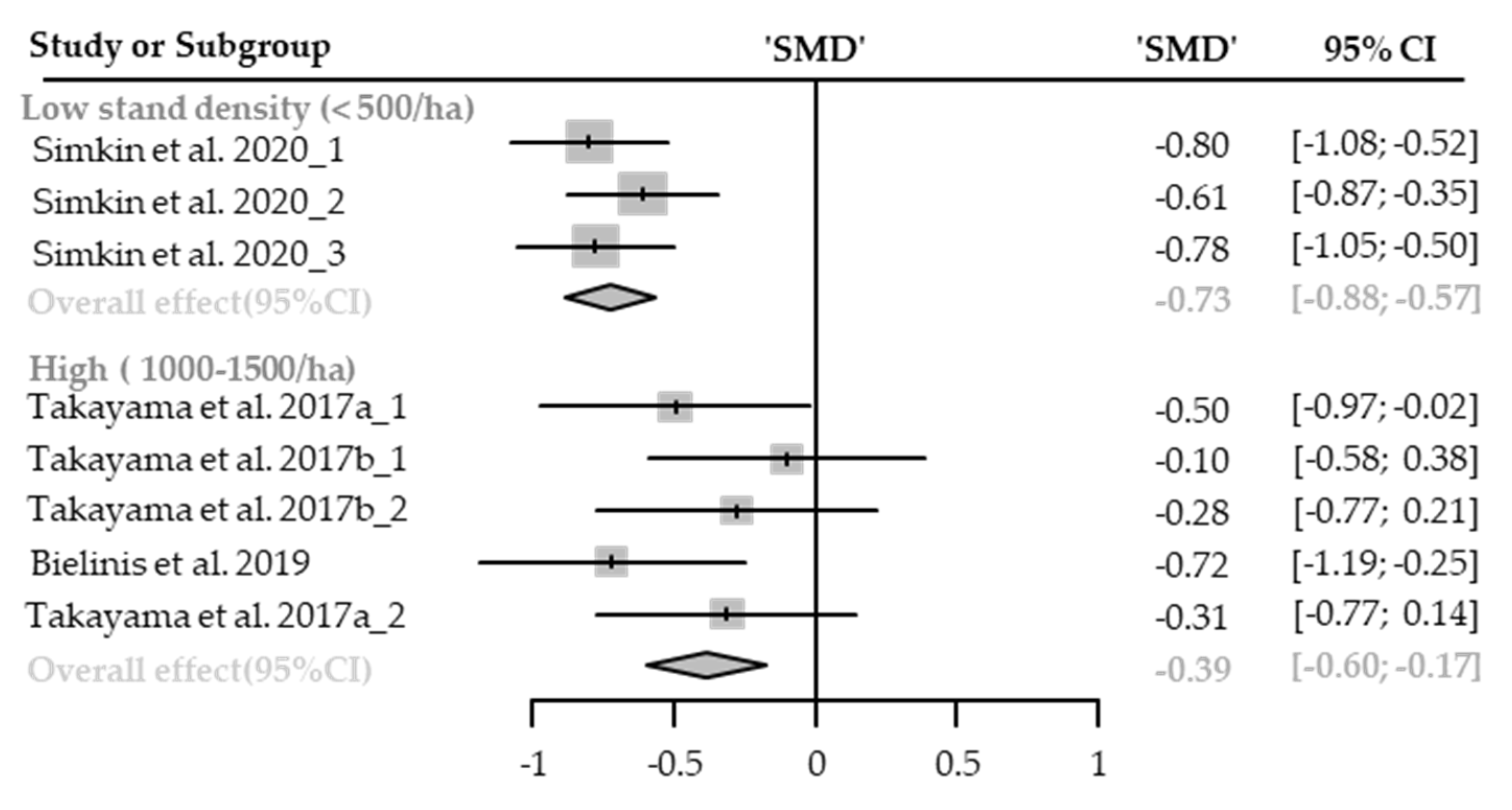
Restorative Experience
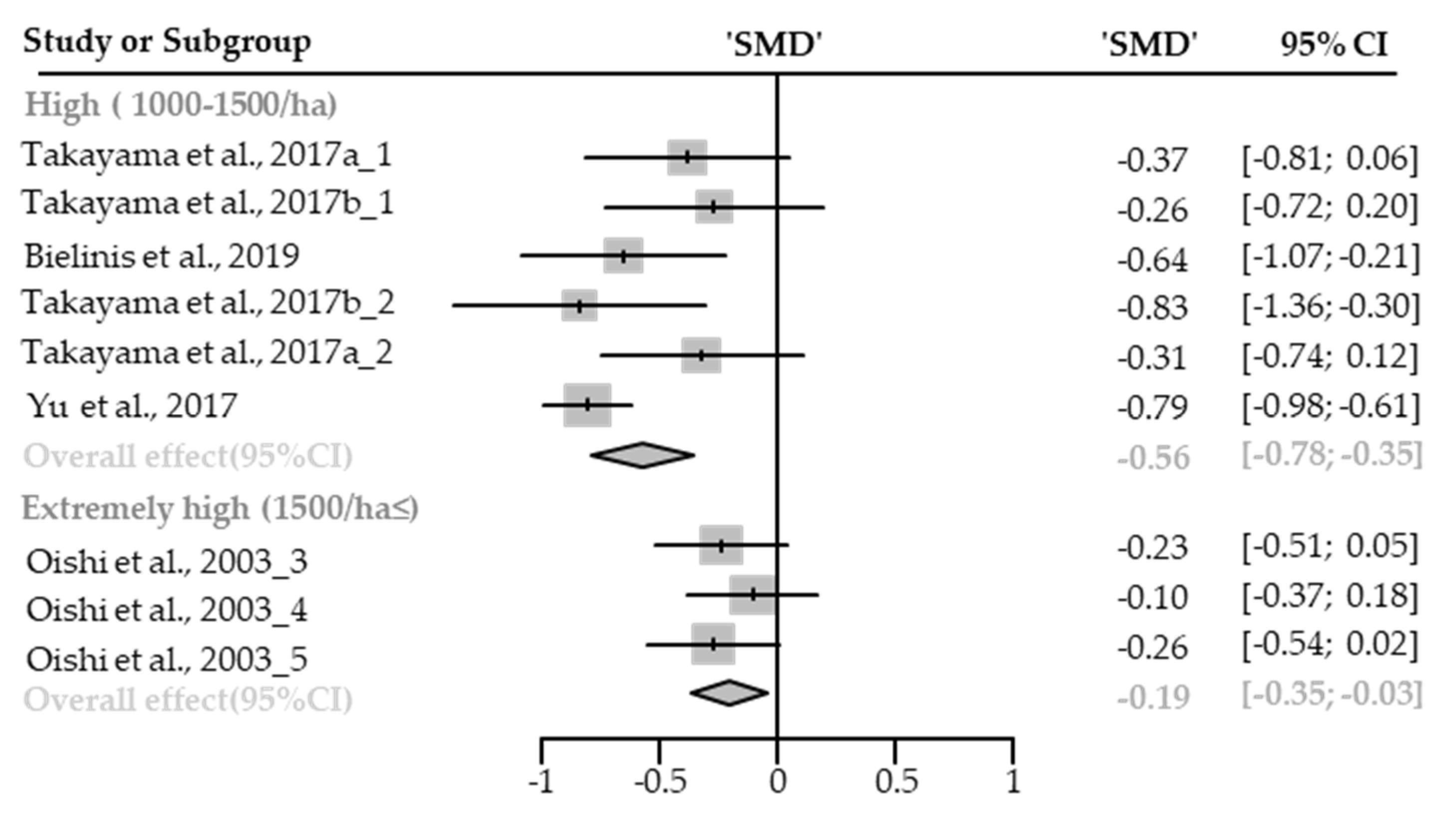
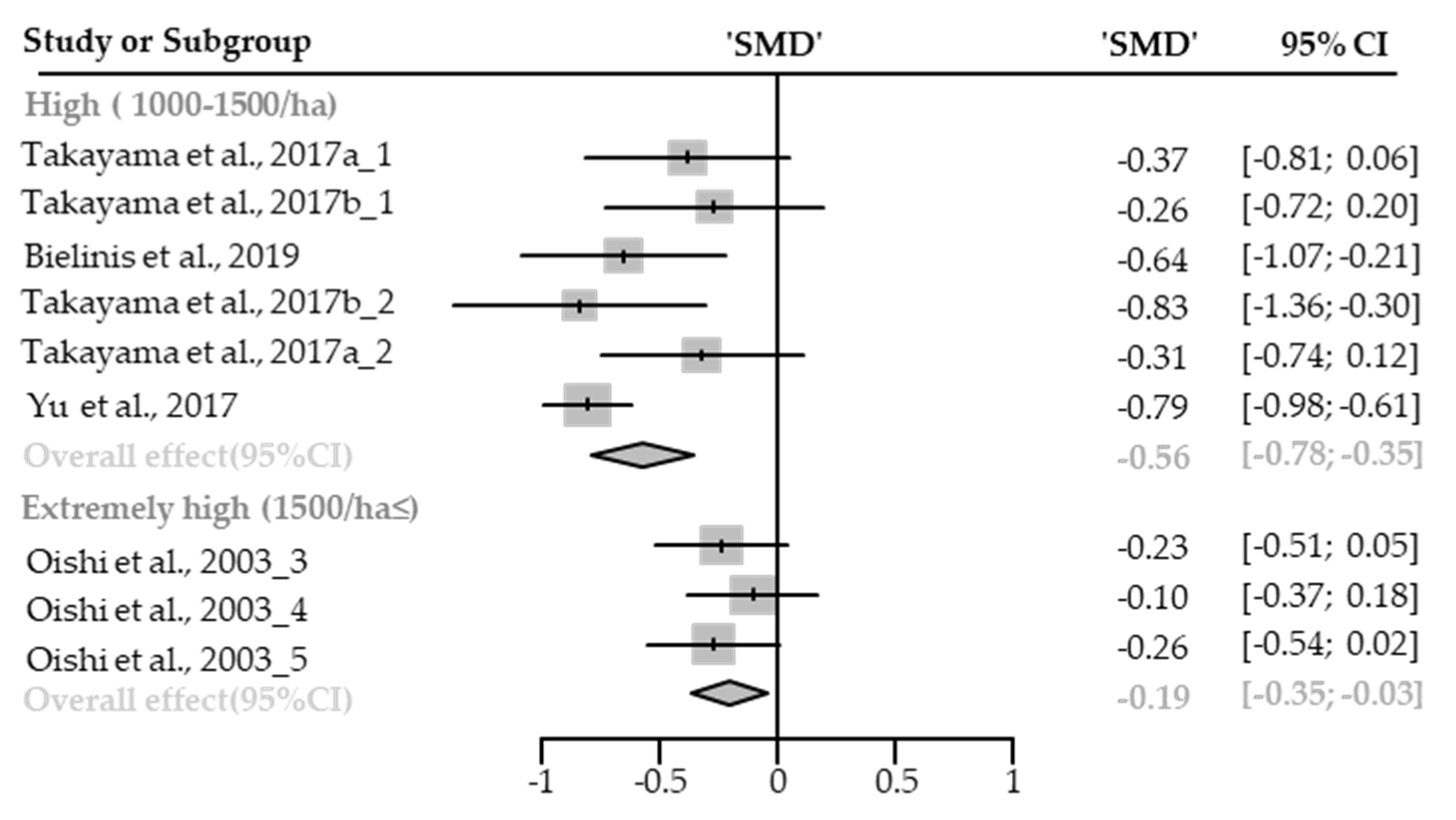
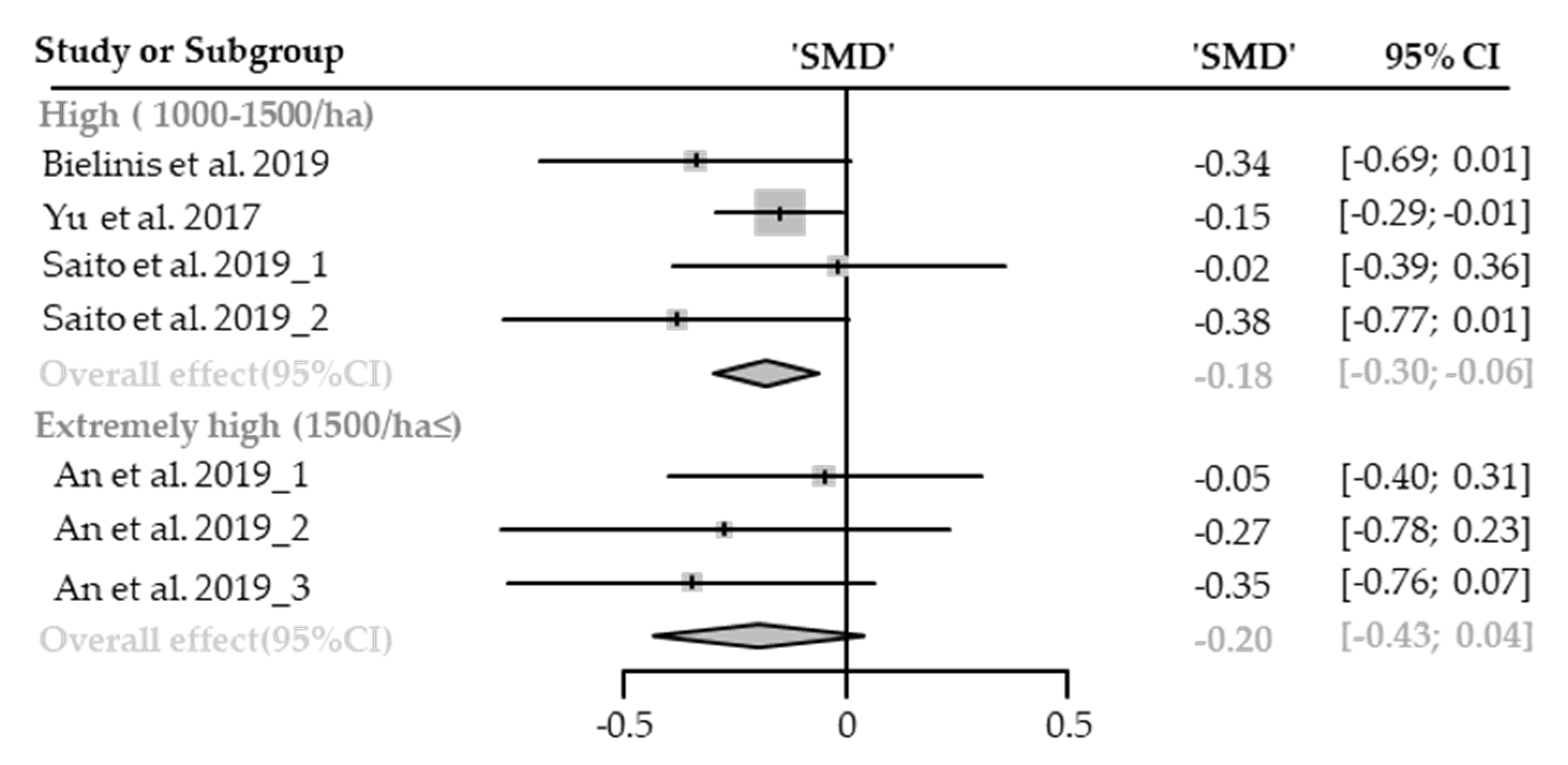
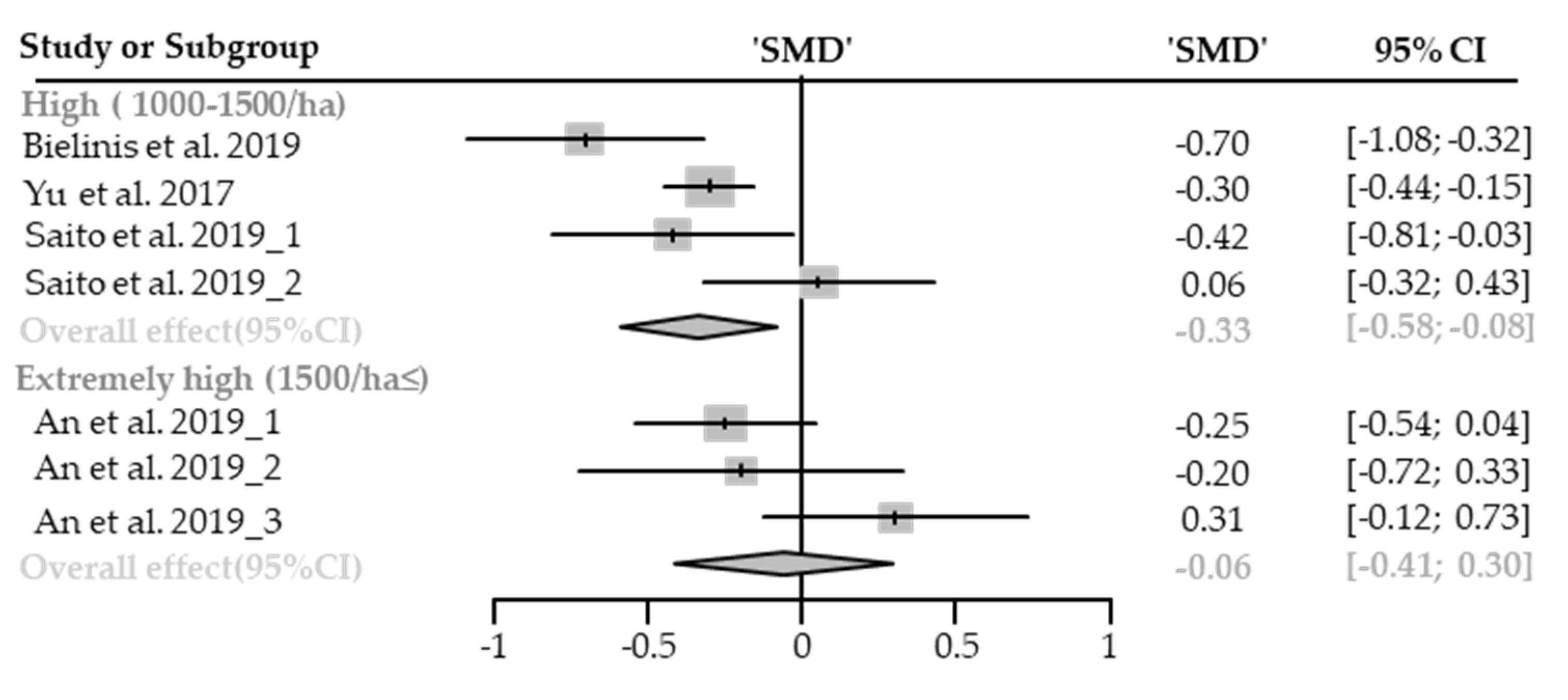
3.3.3. Physiological Relaxation
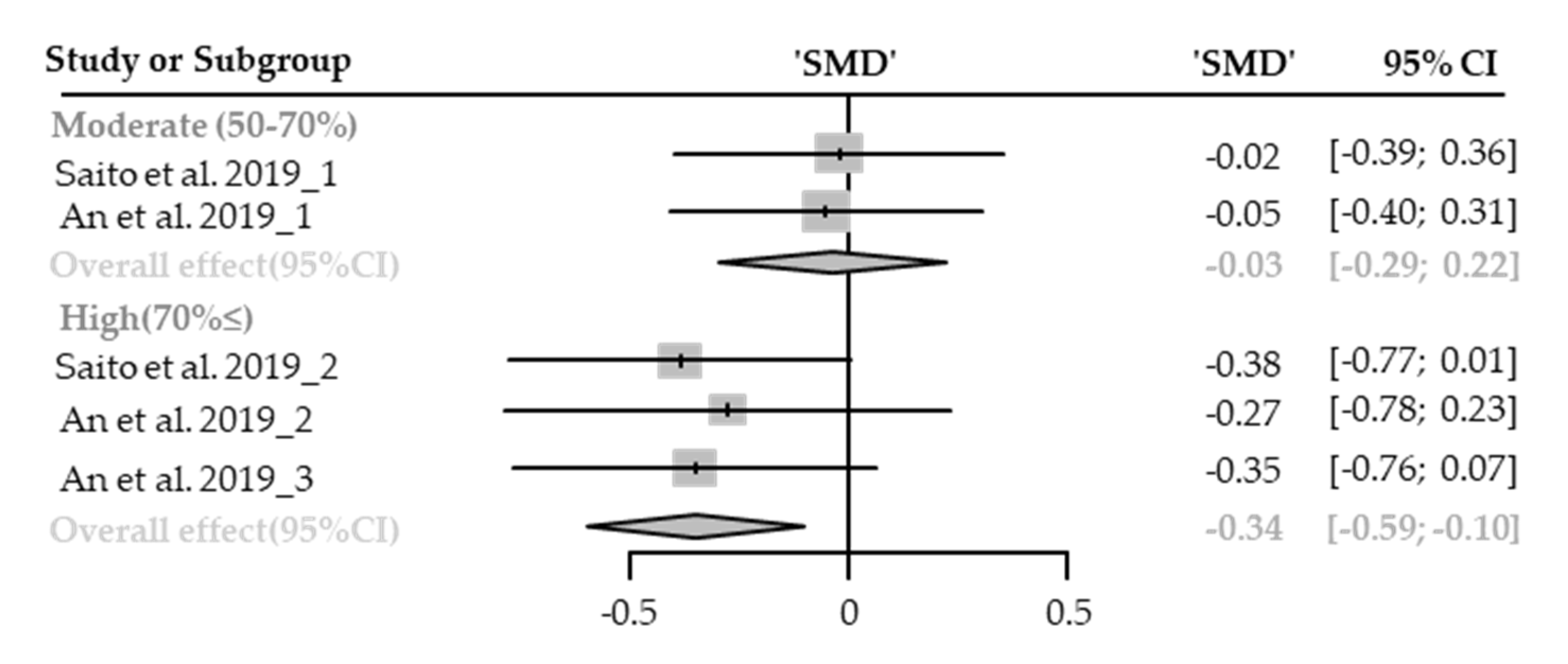
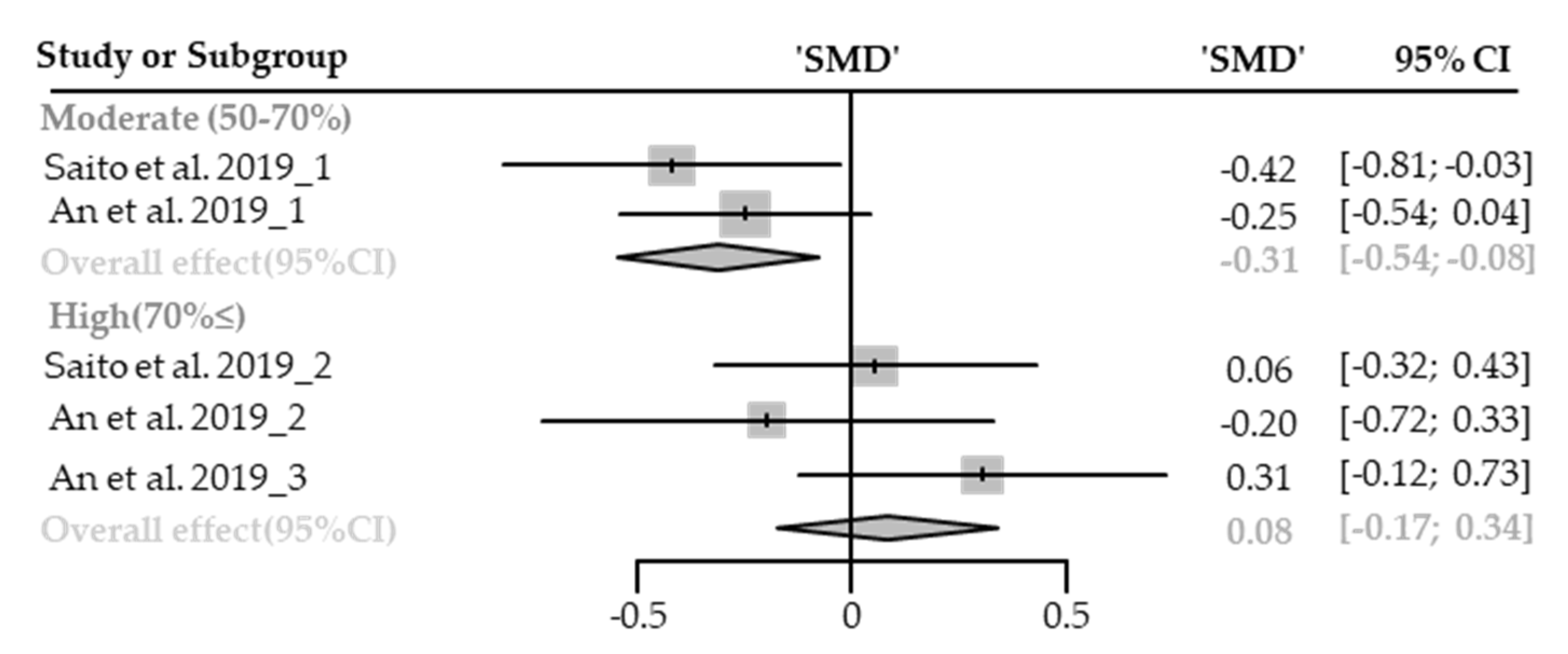
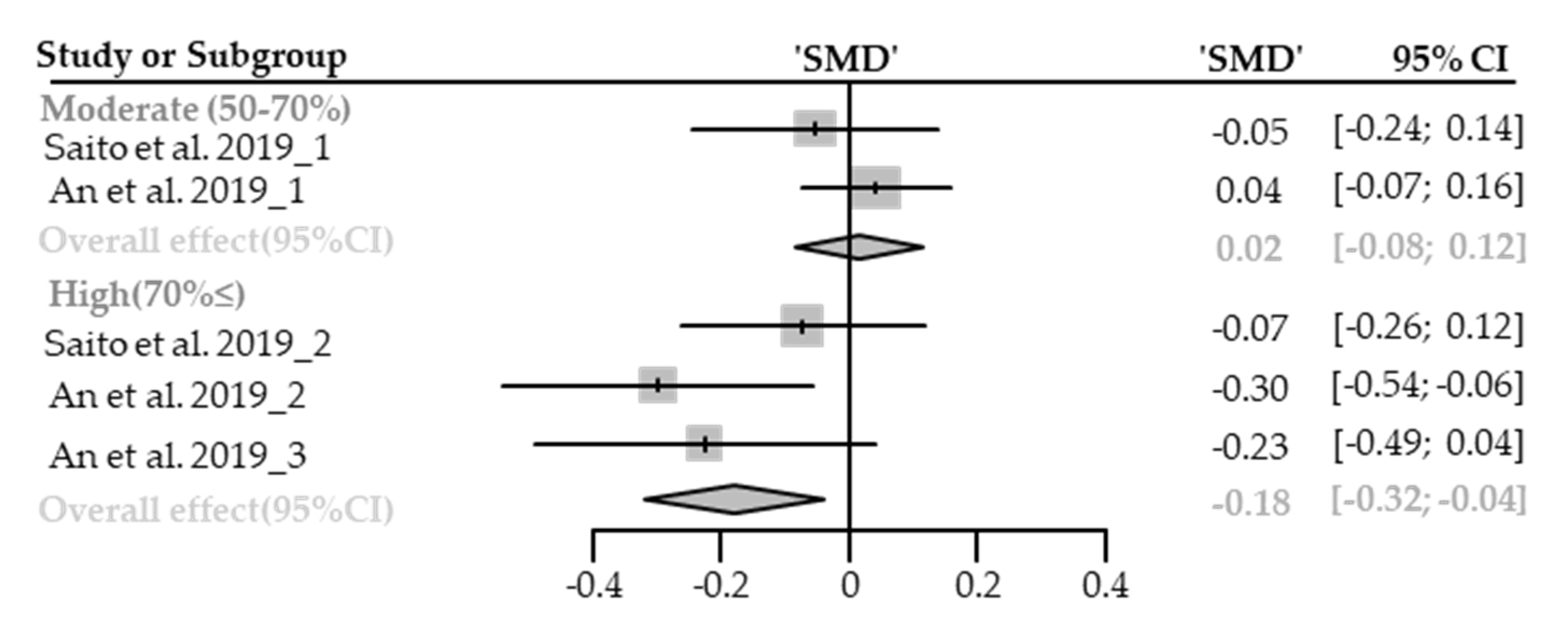
Diastolic Blood Pressure
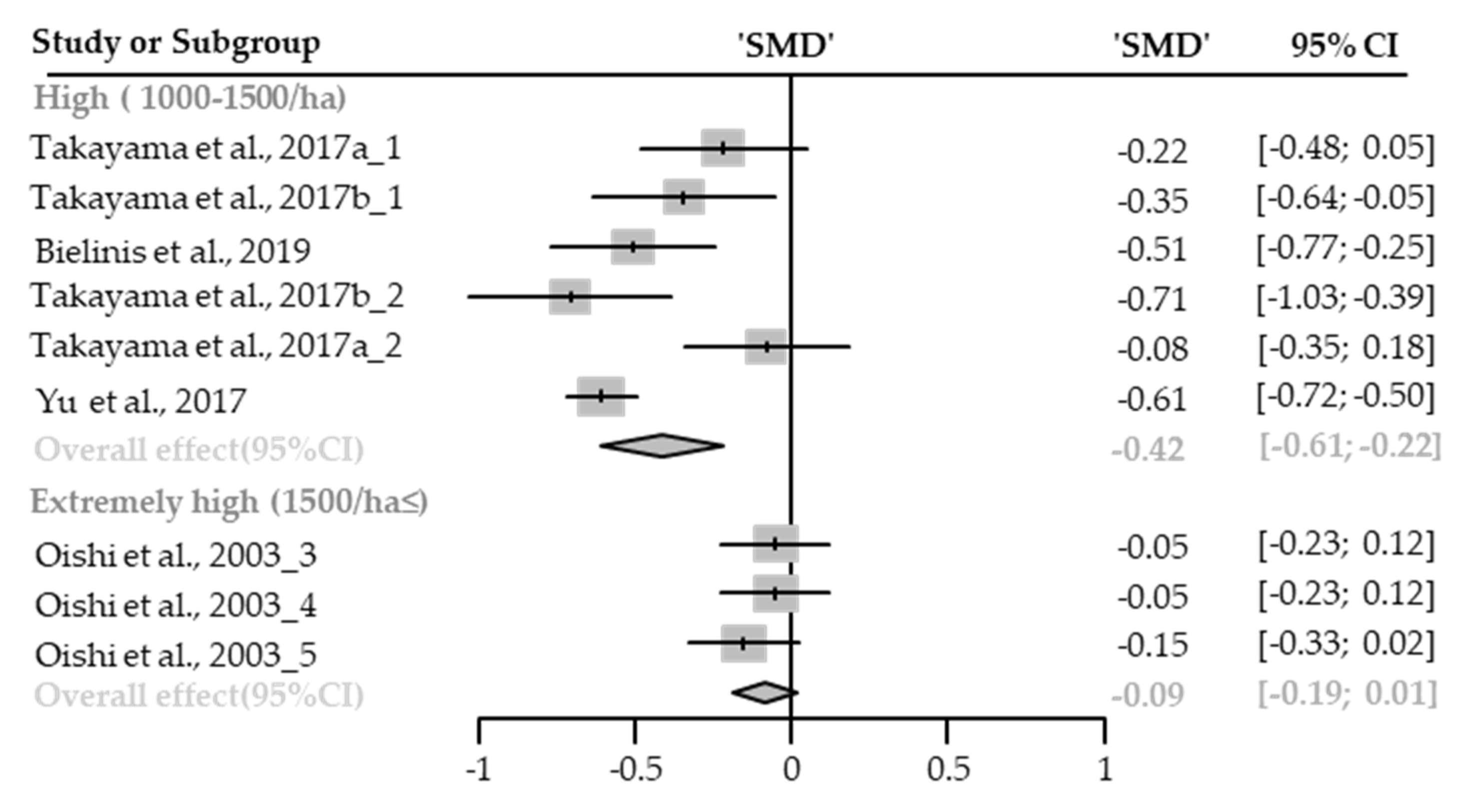
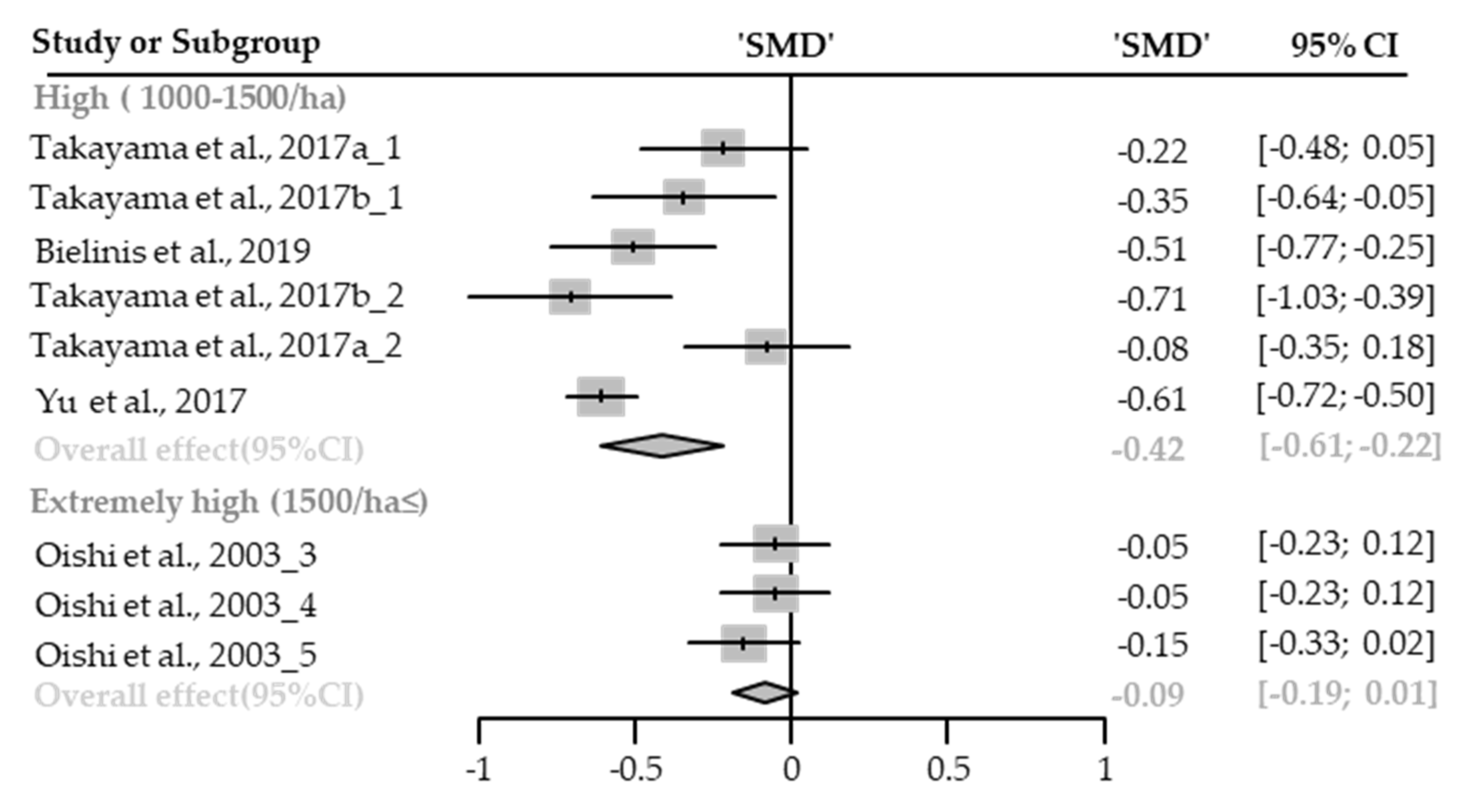
Systolic Blood Pressure
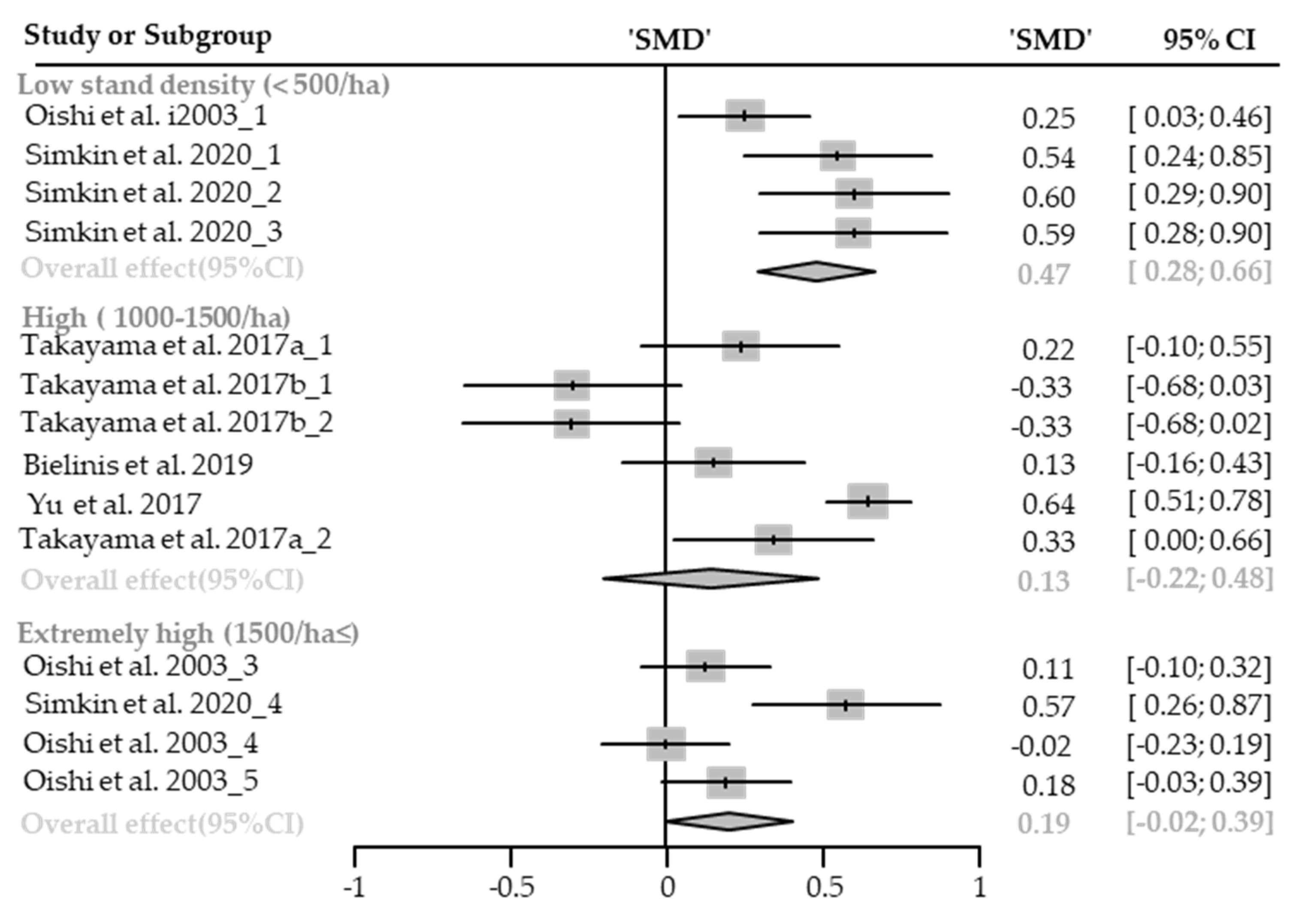
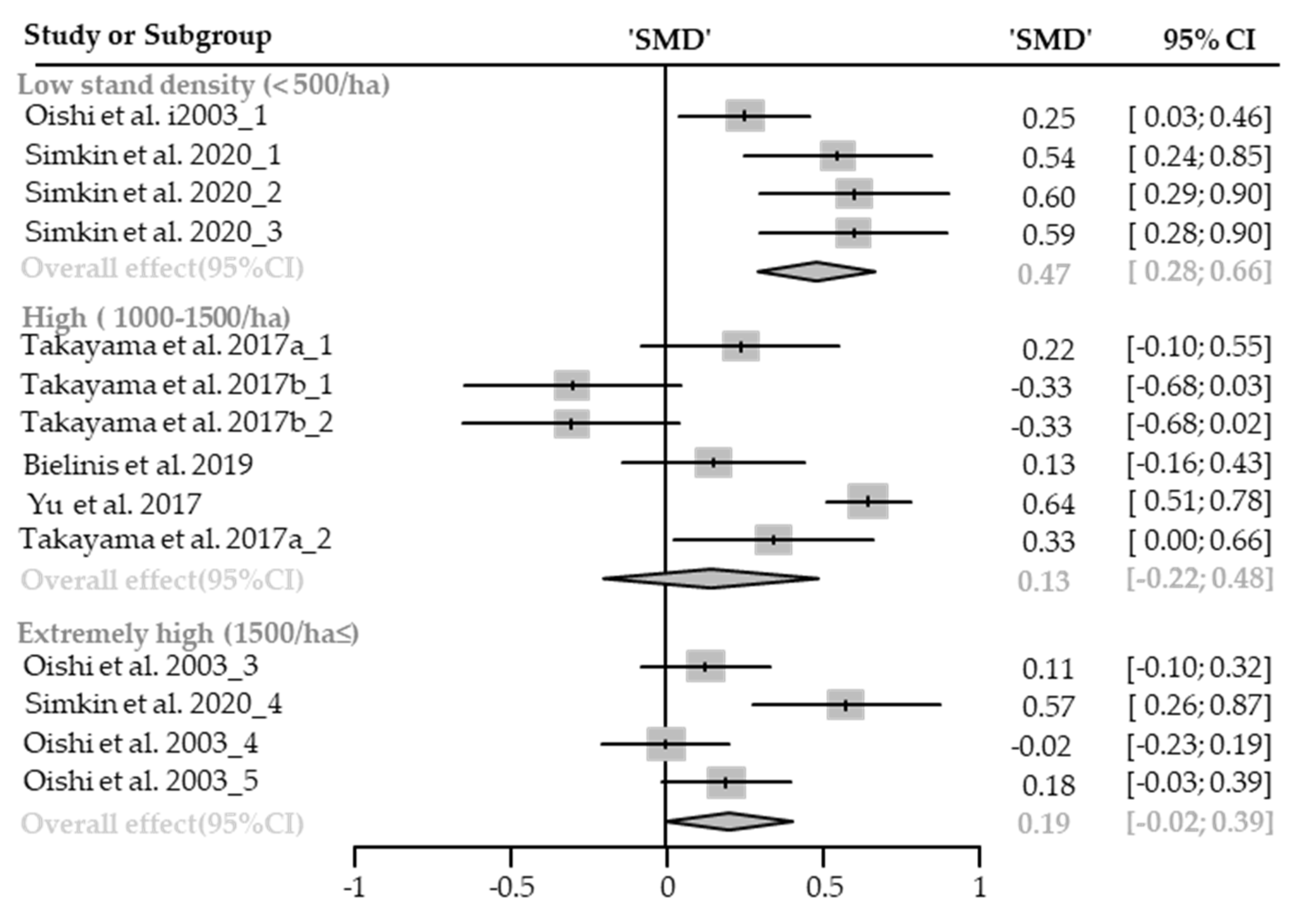
Heart Rate or Pulse Rate
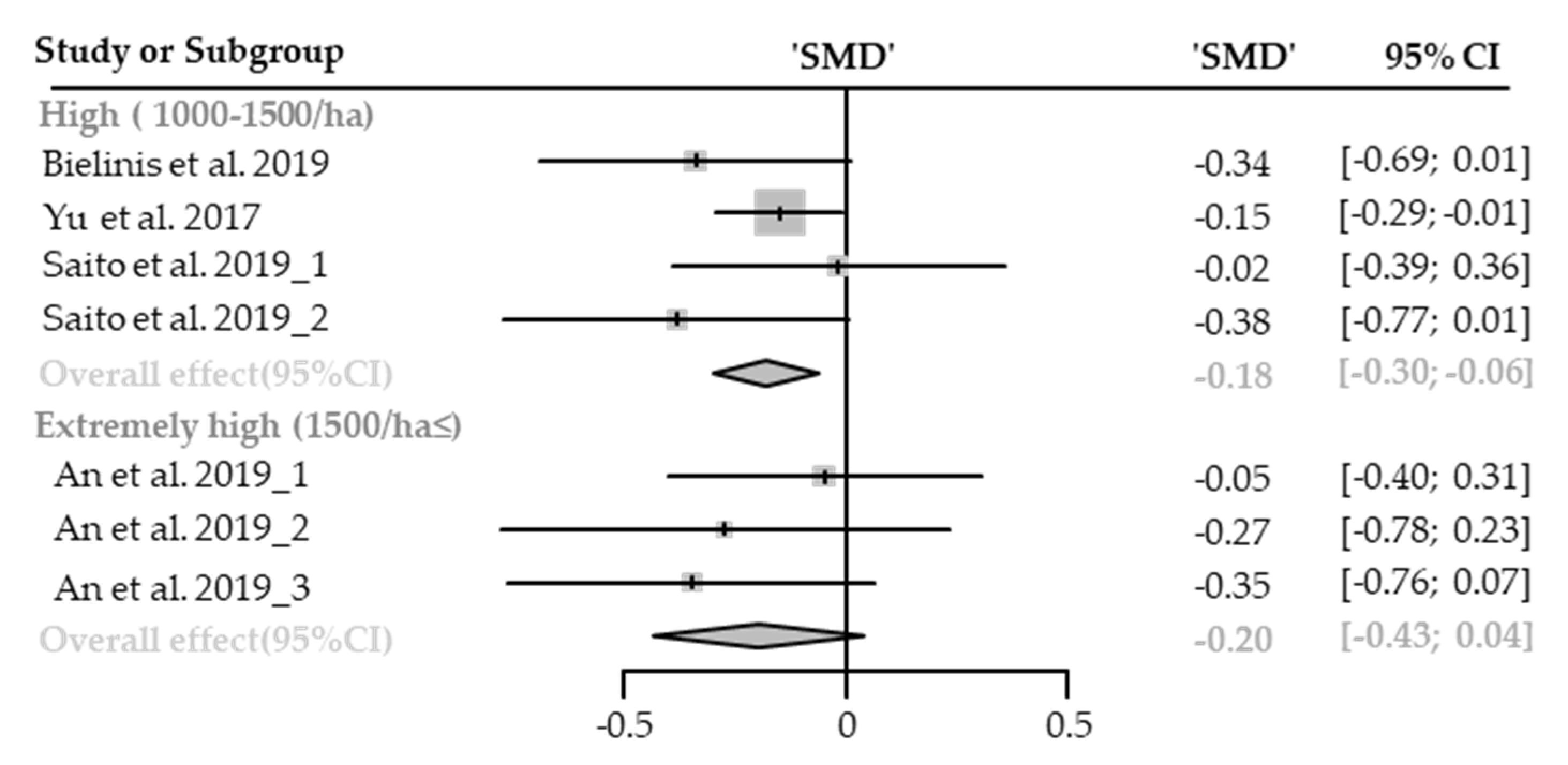
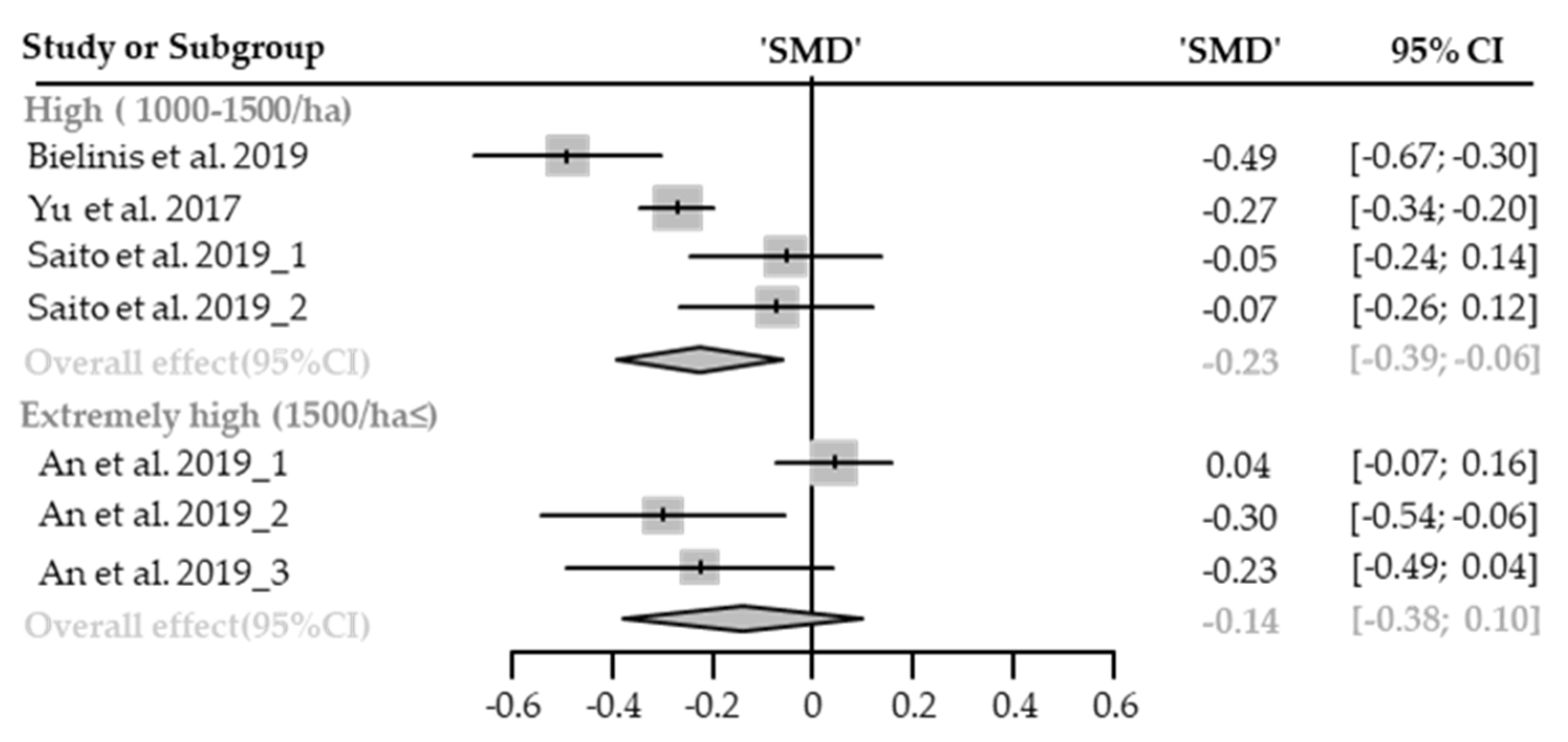
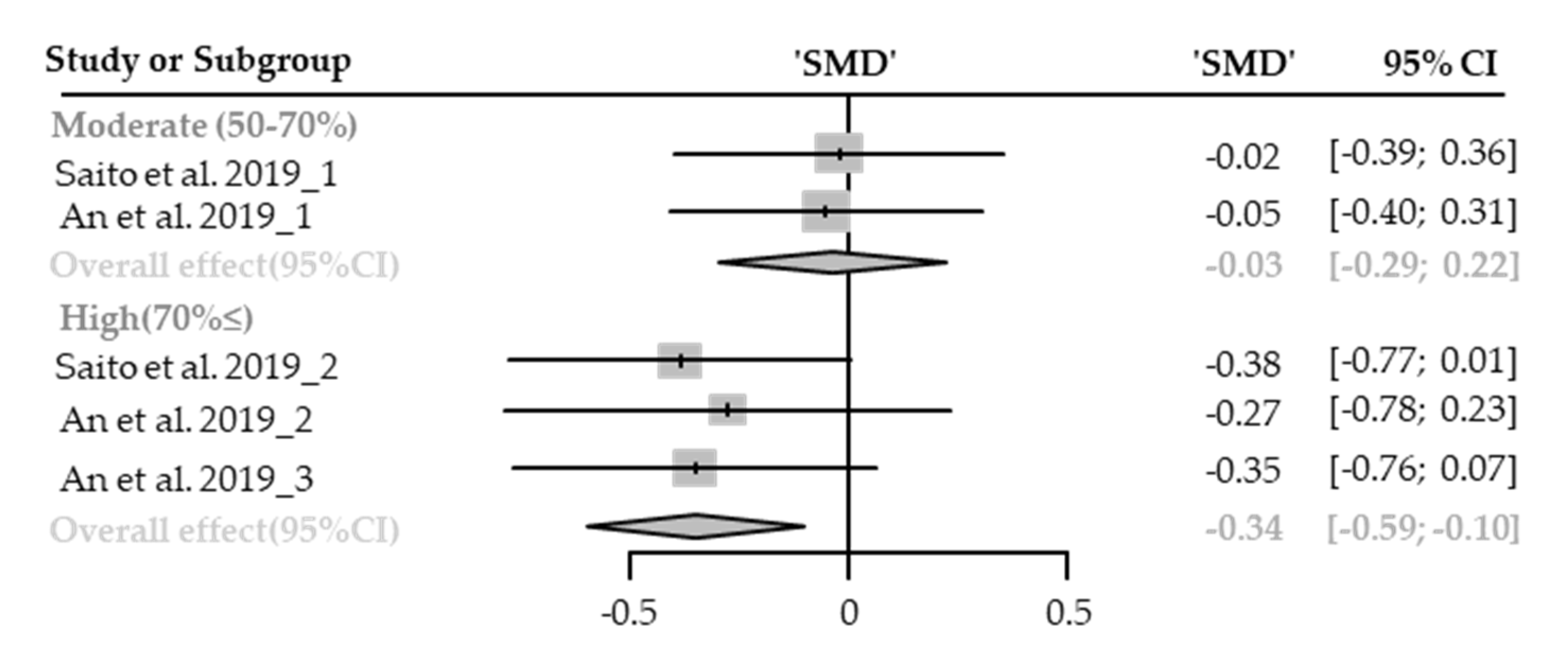
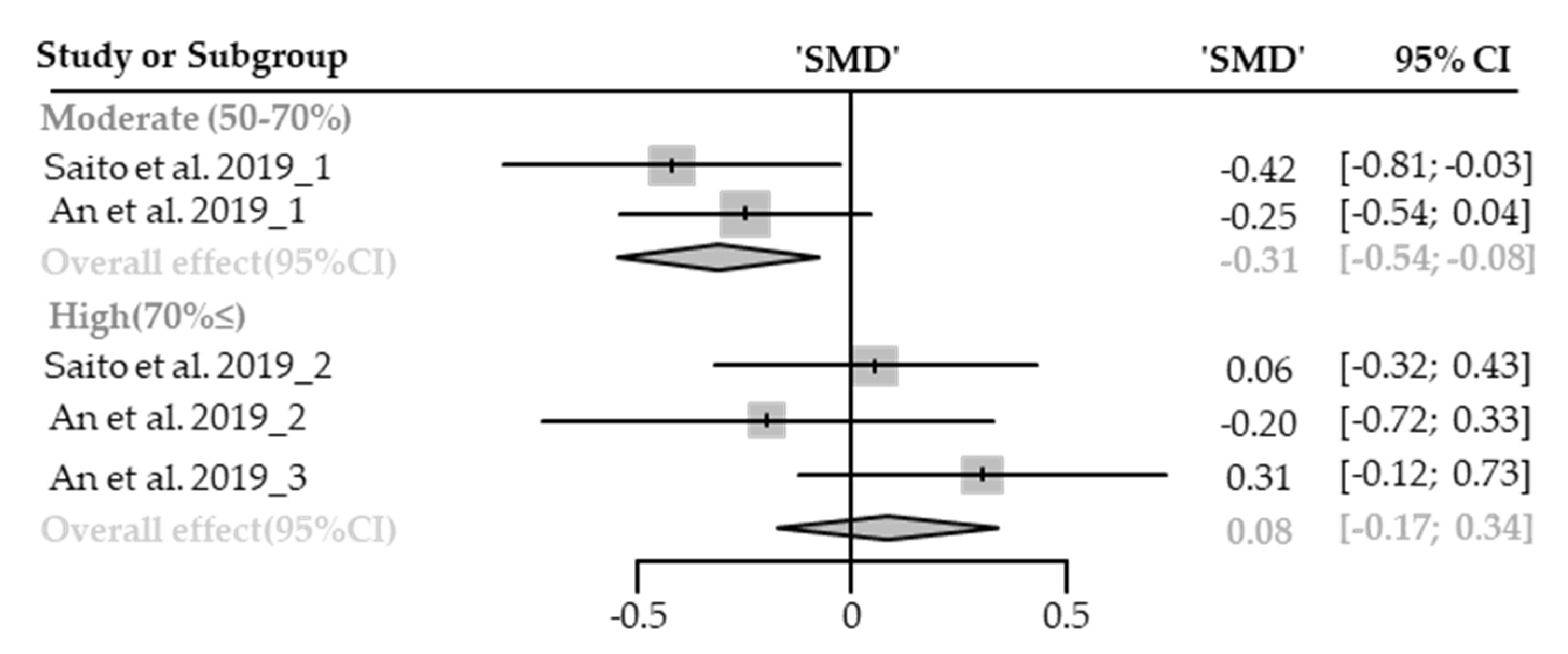
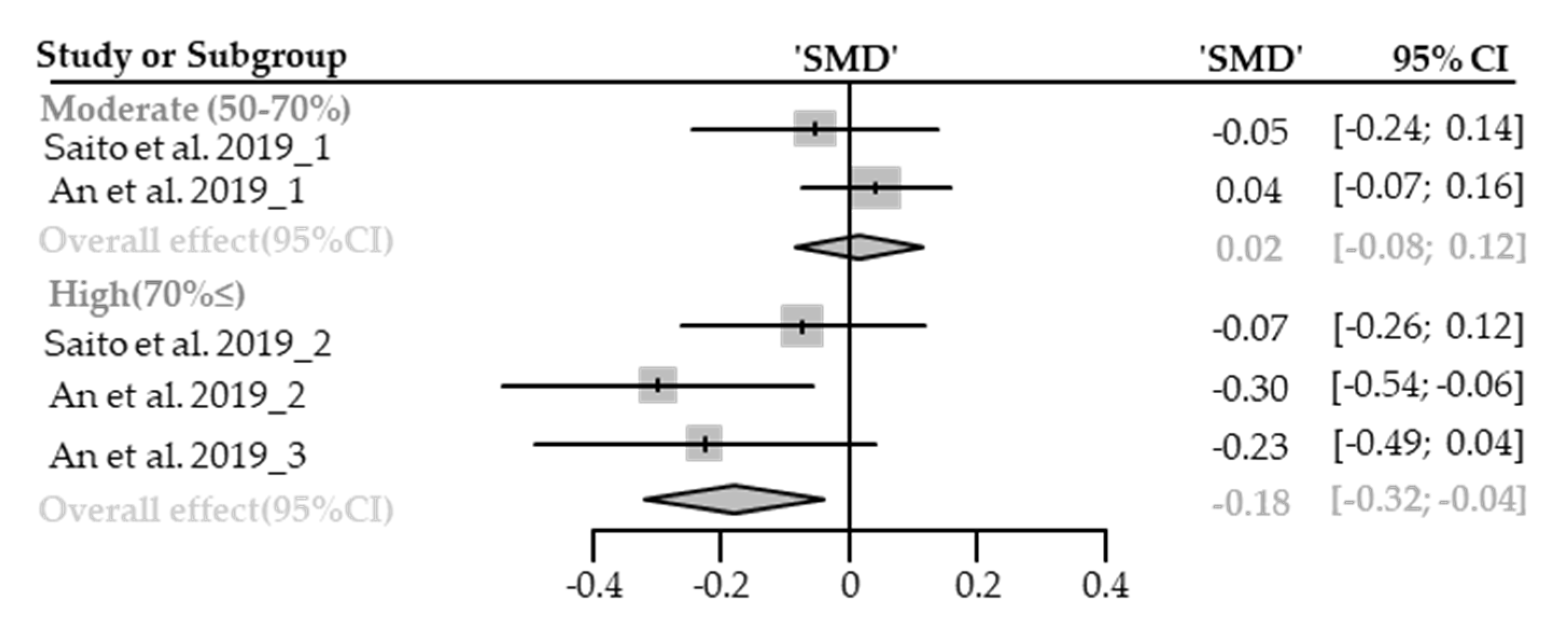
3.4. Canopy Density as an Effect Modifier of Therapeutic Effect
3.4.1. Physiological Relaxation
Diastolic Blood Pressure
Systolic Blood Pressure
Heart Rate or Pulse Rate
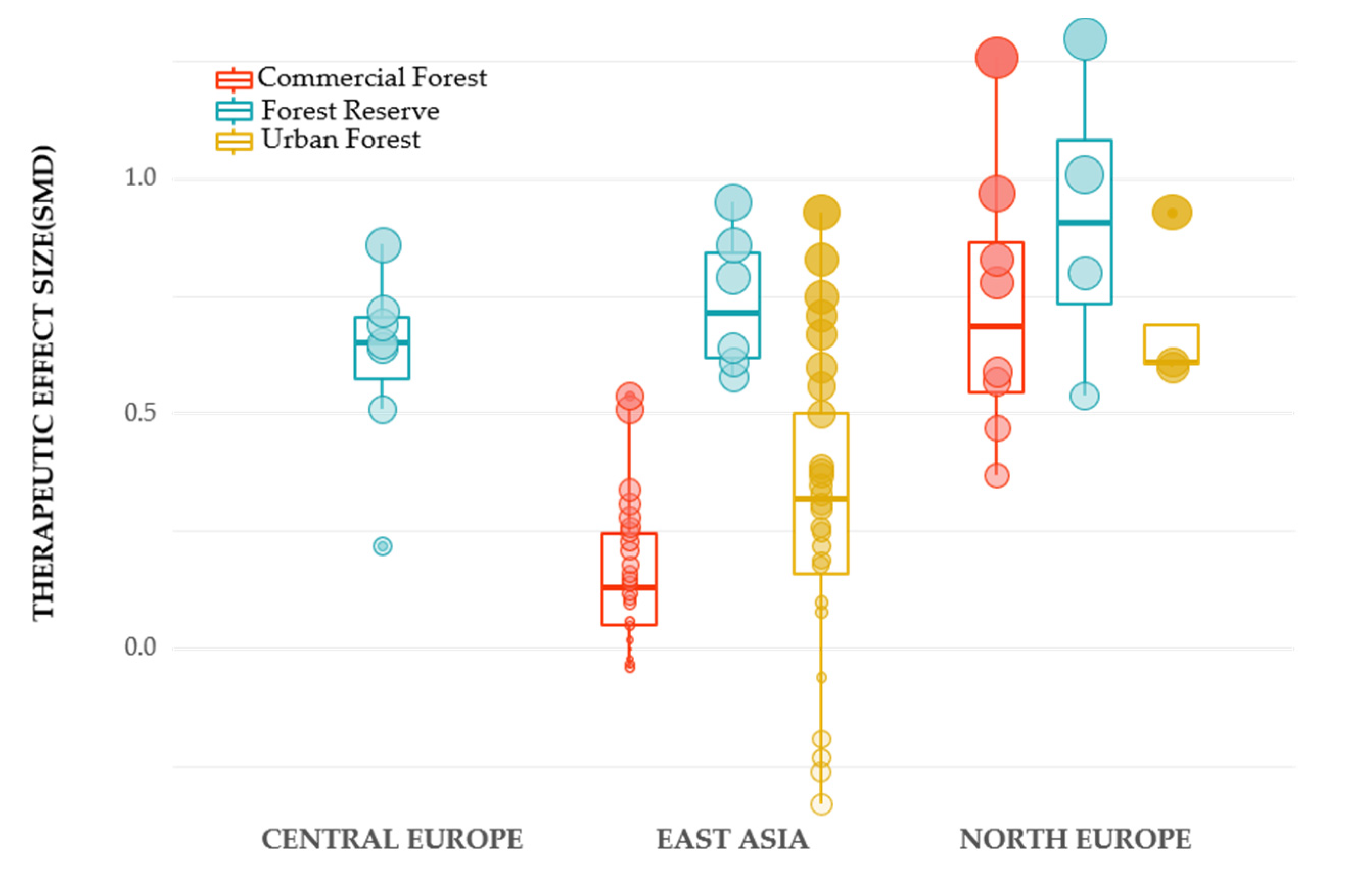
3.5. Other Possible Effect Modifier
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: Cambridge, UK, 1989. [Google Scholar]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Hartig, T.; Mang, M.; Evans, G.W. Restorative effects of natural environment experiences. Environ. Behav. 1991, 23, 3–26. [Google Scholar] [CrossRef]
- Berman, M.G.; Jonides, J.; Kaplan, S. The cognitive benefits of interacting with nature. Psychol. Sci. 2008, 19, 1207–1212. [Google Scholar] [CrossRef]
- Ulrich, R.S. Natural versus urban scenes: Some psychophysiological effects. Environ. Behav. 1981, 13, 523–556. [Google Scholar] [CrossRef]
- Ulrich, R.S. Aesthetic and affective response to natural environment. In Behavior and the Natural Environment; Springer: Boston, MA, USA, 1983; pp. 85–125. [Google Scholar]
- Bratman, G.N.; Daily, G.C.; Levy, B.J.; Gross, J.J. The benefits of nature experience: Improved affect and cognition. Landsc. Urban. Plan. 2015, 138, 41–50. [Google Scholar] [CrossRef]
- Ulrich, R.S.; Simons, R.F.; Losito, B.D.; Fiorito, E.; Miles, M.A.; Zelson, M. Stress recovery during exposure to natural and urban environments. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar] [CrossRef]
- James, P.; Banay, R.F.; Hart, J.E.; Laden, F. A review of the health benefits of greenness. Curr. Epidemiol. Rep. 2015, 2, 131–142. [Google Scholar] [CrossRef] [Green Version]
- Hartig, T.; Mitchell, R.; De Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [Green Version]
- Meyer, K.; Bürger-Arndt, R. How forests foster human health–Present state of research-based knowledge (in the field of Forests and Human Health). Int. For. Rev. 2014, 16, 421–446. [Google Scholar] [CrossRef]
- Miyazaki, Y.; Ikei, H.; Song, C. Forest medicine research in Japan. Nihon Eiseigaku Zasshi. Jpn. J. Hyg. 2014, 69, 122–135. [Google Scholar] [CrossRef] [Green Version]
- Van Herzele, A.; Bell, S.; Hartig, T.; Podesta, M.T.C.; van Zon, R. Health benefits of nature experience: The challenge of linking practice and research. In Forests, Trees and Human Health; Springer: Dordrecht, The Netherlands, 2011; pp. 169–182. [Google Scholar]
- Morris, J.; O’Brien, E. Encouraging healthy outdoor activity amongst under-represented groups: An evaluation of the Active England woodland projects. Urban. For. Urban. Green. 2011, 10, 323–333. [Google Scholar] [CrossRef]
- Tsunetsugu, Y.; Park, B.-J.; Miyazaki, Y. Trends in research related to “Shinrin-yoku” (taking in the forest atmosphere or forest bathing) in Japan. Environ. Health Prev. Med. 2010, 15, 27–37. [Google Scholar] [CrossRef] [Green Version]
- Shin, W.S.; Yeoun, P.S.; Yoo, R.W.; Shin, C.S. Forest experience and psychological health benefits: The state of the art and future prospect in Korea. Environ. Health Prev. Med. 2010, 15, 38. [Google Scholar] [CrossRef] [Green Version]
- Jung, W.H.; Woo, J.-M.; Ryu, J.S. Effect of a forest therapy program and the forest environment on female workers’ stress. Urban. For. Urban. Green. 2015, 14, 274–281. [Google Scholar] [CrossRef]
- Chun, M.H.; Chang, M.C.; Lee, S.-J. The effects of forest therapy on depression and anxiety in patients with chronic stroke. Int. J. Neurosci. 2017, 127, 199–203. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Kagawa, T.; Miyazaki, Y. Effects of Walking in a Forest on Young Women. Int. J. Environ. Res. Public Health 2019, 16, 229. [Google Scholar] [CrossRef] [Green Version]
- Song, C.; Ikei, H.; Park, B.J.; Lee, J.; Kagawa, T.; Miyazaki, Y. Psychological benefits of walking through forest areas. Int. J. Environ. Res. Public Health 2018, 15, 2804. [Google Scholar] [CrossRef] [Green Version]
- Hassan, A.; Tao, J.; Li, G.; Jiang, M.; Aii, L.; Zhihui, J.; Zongfang, L.; Qibing, C. Effects of walking in bamboo forest and city environments on brainwave activity in young adults. Evid.-Based Complement. Altern. Med. 2018, 2018, 1–9. [Google Scholar] [CrossRef]
- Im, S.G.; Choi, H.; Jeon, Y.-H.; Song, M.-K.; Kim, W.; Woo, J.-M. Comparison of effect of two-hour exposure to forest and urban environments on cytokine, anti-oxidant, and stress levels in young adults. Int. J. Environ. Res. Public Health 2016, 13, 625. [Google Scholar] [CrossRef] [Green Version]
- Olafsdottir, G.; Cloke, P.; Schulz, A.; van Dyck, Z.; Eysteinsson, T.; Thorleifsdottir, B.; Vögele, C. Health Benefits of Walking in Nature: A Randomized Controlled Study Under Conditions of Real-Life Stress. Environ. Behav. 2020, 52, 248–274. [Google Scholar] [CrossRef]
- Rajoo, K.S.; Karam, D.S.; Aziz, N.A.A. Developing an effective forest therapy program to manage academic stress in conservative societies: A multi-disciplinary approach. Urban. For. Urban. Green. 2019, 43, 126353. [Google Scholar] [CrossRef]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Hirano, H.; Kagawa, T.; Sato, M.; Miyazaki, Y. Physiological effects of Shinrin-yoku (taking in the atmosphere of the forest) using salivary cortisol and cerebral activity as indicators. J. Physiol Anthr. 2007, 26, 123–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsunetsugu, Y.; Park, B.J.; Ishii, H.; Hirano, H.; Kagawa, T.; Miyazaki, Y. Physiological effects of Shinrin-yoku (taking in the atmosphere of the forest) in an old-growth broadleaf forest in Yamagata Prefecture, Japan. J. Physiol. Anthropol. 2007, 26, 135–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bielinis, E.; Bielinis, L.; Krupińska-Szeluga, S.; Łukowski, A.; Takayama, N. The effects of a short forest recreation program on physiological and psychological relaxation in young Polish adults. Forests 2019, 10, 34. [Google Scholar] [CrossRef] [Green Version]
- Song, C.; Ikei, H.; Miyazaki, Y. Physiological effects of forest-related visual, olfactory, and combined stimuli on humans: An additive combined effect. Urban. For. Urban. Green. 2019, 44, 126437. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Miyazaki, Y. Sustained effects of a forest therapy program on the blood pressure of office workers. Urban. For. Urban. Green. 2017, 27, 246–252. [Google Scholar] [CrossRef]
- Song, C.R.; Ikei, H.; Kagawa, T.; Miyazaki, Y. Effect of Viewing Real Forest Landscapes on Brain Activity. Sustainability 2020, 12, 6601. [Google Scholar] [CrossRef]
- Koselka, E.P.D.; Weidner, L.C.; Minasov, A.; Berman, M.G.; Leonard, W.R.; Santoso, M.V.; de Brito, J.N.; Pope, Z.C.; Pereira, M.A.; Horton, T.H. Walking Green: Developing an Evidence Base for Nature Prescriptions. Int. J. Environ. Res. Public Health 2019, 16, 4338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, J.; Woo, J.-M.; Kim, W.; Lim, S.-K.; Chung, E.-J. The effect of cognitive behavior therapy-based “forest therapy” program on blood pressure, salivary cortisol level, and quality of life in elderly hypertensive patients. Clin. Exp. Hypertens. 2012, 34, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.-P.S.; Hsieh, H. Beyond restorative benefits: Evaluating the effect of forest therapy on creativity. Urban. For. Urban. Green. 2020, 51, 126670. [Google Scholar] [CrossRef]
- Jia, B.B.; Yang, Z.X.; Mao, G.X.; Lyu, Y.D.; Wen, X.L.; Xu, W.H.; Lyu, X.L.; Cao, Y.B.; Wang, G.F. Health effect of forest bathing trip on elderly patients with chronic obstructive pulmonary disease. Biomed. Environ. Sci. 2016, 29, 212–218. [Google Scholar] [PubMed]
- Mao, G.; Cao, Y.; Wang, B.; Wang, S.; Chen, Z.; Wang, J.; Xing, W.; Ren, X.; Lv, X.; Dong, J.; et al. The salutary influence of forest bathing on elderly patients with chronic heart failure. Int. J. Environ. Res. Public Health 2017, 14, 368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, G.X.; Cao, Y.B.; Yang, Y.; Chen, Z.M.; Dong, J.H.; Chen, S.S.; Wu, Q.; Lyu, X.L.; Jia, B.B.; Yan, J.; et al. Additive Benefits of Twice Forest Bathing Trips in Elderly Patients with Chronic Heart Failure. Biomed. Environ. Sci. 2018, 31, 159–162. [Google Scholar]
- Peterfalvi, A.; Meggyes, M.; Makszin, L.; Farkas, N.; Miko, E.; Miseta, A.; Szereday, L. Forest bathing always makes sense: Blood pressure-lowering and immune system-balancing effects in late spring and winter in central europe. Int. J. Environ. Res. Public Health 2021, 18, 2067. [Google Scholar] [CrossRef] [PubMed]
- Mukaida, N.; Harada, A.; Matsushima, K. Interleukin-8 (IL-8) and monocyte chemotactic and activating factor (MCAF/MCP-1), chemokines essentially involved in inflammatory and immune reactions. Cytokine Growth Factor Rev. 1998, 9, 9–23. [Google Scholar] [CrossRef]
- Lyu, B.; Zeng, C.; Xie, S.; Li, D.; Lin, W.; Li, N.; Jiang, M.; Liu, S.; Chen, Q. Benefits of a three-day bamboo forest therapy session on the psychophysiology and immune system responses of male college students. Int. J. Environ. Res. Public Health 2019, 16, 4991. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Kawada, T. Effect of forest therapy on the human psycho-neuro-endocrino-immune network. Nihon Eiseigaku Zasshi. Jpn. J. Hyg. 2011, 66, 645–650. [Google Scholar] [CrossRef] [Green Version]
- Li, Q. Effect of forest bathing trips on human immune function. Environ. Health Prev. Med. 2010, 15, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Lee, D.C. Cardiac and pulmonary benefits of forest walking versus city walking in elderly women: A randomised, controlled, open-label trial. Eur. J. Integr. Med. 2014, 6, 5–11. [Google Scholar] [CrossRef]
- Mao, G.X.; Cao, Y.B.; Lan, X.G.; He, Z.H.; Chen, Z.M.; Wang, Y.Z.; Hu, X.L.; Lv, Y.D.; Wang, G.F.; Yan, J. Therapeutic effect of forest bathing on human hypertension in the elderly. J. Cardiol. 2012, 60, 495–502. [Google Scholar] [CrossRef] [Green Version]
- Guan, H.; Wei, H.; He, X.; Ren, Z.; An, B. The tree-species-specific effect of forest bathing on perceived anxiety alleviation of young-adults in urban forests. Ann. For. Res. 2017, 60, 327–341. [Google Scholar] [CrossRef]
- Fujisawa, M.; Takayama, N.; Morikawa, T. Study on physiological response and subjective appraisal brought visually by a light environment of a forest. Pap. Environ. Inf. Sci. 2012, 26, 103–106. [Google Scholar]
- Joung, D.; Song, C.; Ikei, H.; Okuda, T.; Igarashi, M.; Koizumi, H.; Park, B.J.; Yamaguchi, T.; Takagaki, M.; Miyazaki, Y. Physiological and psychological effects of olfactory stimulation with D-Limonene. Adv. Hortic. Sci. 2014, 28, 90–94. [Google Scholar]
- Ikei, H.; Song, C.R.; Miyazaki, Y. Physiological effect of olfactory stimulation by Hinoki cypress (Chamaecyparis obtusa) leaf oil. J. Physiol. Anthropol. 2015, 34, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Hansen, M.M.; Jones, R.; Tocchini, K. Shinrin-yoku (forest bathing) and nature therapy: A state-of-the-art review. Int. J. Environ. Res. Public Health 2017, 14, 851. [Google Scholar] [CrossRef] [Green Version]
- Tyrväinen, L.; Ojala, A.; Korpela, K.; Lanki, T.; Tsunetsugu, Y.; Kagawa, T. The influence of urban green environments on stress relief measures: A field experiment. J. Environ. Psychol. 2014, 38, 1–9. [Google Scholar] [CrossRef]
- Zeng, C.; Lyu, B.; Deng, S.; Yu, Y.; Li, N.; Lin, W.; Li, D.; Chen, Q. Benefits of a Three-Day Bamboo Forest Therapy Session on the Physiological Responses of University Students. Int. J. Environ. Res. Public Health 2020, 17, 3238. [Google Scholar] [CrossRef] [PubMed]
- Zhu, S.X.; Hu, F.F.; He, S.Y.; Qiu, Q.; Su, Y.; He, Q.; Li, J.Y. Comprehensive Evaluation of Healthcare Benefits of Different Forest Types: A Case Study in Shimen National Forest Park, China. Forests 2021, 12, 207. [Google Scholar] [CrossRef]
- Yamada, A.; Sato, Y.; Horike, T.; Miyanaga, M.; Wang, D.-H. Effects of a Forest Walk on Urinary Dityrosine and Hexanoyl-Lysine in Young People: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 4990. [Google Scholar] [CrossRef]
- Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Suzuki, H.; Li, Y.J.; Wakayama, Y.; et al. Visiting a forest, but not a city, increases human natural killer activity and expression of anti-cancer proteins. Int. J. Immunopathol. Pharmacol. 2008, 21, 117–127. [Google Scholar] [CrossRef]
- Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Shimizu, T.; Li, Y.J.; Wakayama, Y.; et al. A forest bathing trip increases human natural killer activity and expression of anti-cancer proteins in female subjects. J. Biol. Regul. Homeost. Agents 2008, 22, 45–55. [Google Scholar] [PubMed]
- Kim, G.; Park, S.; Kwak, D. Is It Possible to Predict the Concentration of Natural Volatile Organic Compounds in Forest Atmosphere? Int. J. Environ. Res. Public Health 2020, 17, 7875. [Google Scholar] [CrossRef] [PubMed]
- Song, C.R.; Ikei, H.; Miyazaki, Y. Physiological Effects of Nature Therapy: A Review of the Research in Japan. Int. J. Environ. Res. Public Health 2016, 13, 781. [Google Scholar] [CrossRef] [PubMed]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; et al. Physiological and Psychological Effects of Forest Therapy on Middle-Aged Males with High-Normal Blood Pressure. Int. J. Environ. Res. Public Health 2015, 12, 2532–2542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bedimo-Rung, A.L.; Mowen, A.J.; Cohen, D.A. The significance of parks to physical activity and public health: A conceptual model. Am. J. Prev. Med. 2005, 28, 159–168. [Google Scholar] [CrossRef]
- Chiang, Y.C.; Li, D.; Jane, H.A. Wild or tended nature? The effects of landscape location and vegetation density on physiological and psychological responses. Landsc. Urban. Plan. 2017, 167, 72–83. [Google Scholar] [CrossRef]
- Lin, W.; Chen, Q.; Zhang, X.; Tao, J.; Liu, Z.; Lyu, B.; Li, N.; Li, D.; Zeng, C. Effects of Different Bamboo Forest Spaces on Psychophysiological Stress and Spatial Scale Evaluation. Forests 2020, 11, 616. [Google Scholar] [CrossRef]
- Gao, T.; Zhang, T.; Zhu, L.; Gao, Y.; Qiu, L. Exploring psychophysiological restoration and individual preference in the different environments based on virtual reality. Int. J. Environ. Res. Public Health 2019, 16, 3102. [Google Scholar] [CrossRef] [Green Version]
- Matthew, A.; Birgitta, G. Variations in perceptions of danger, fear and preference in a simulated natural environment. J. Environ. Psychol. 2010, 30, 473–481. [Google Scholar]
- Heyman, E.; Gunnarsson, B.; Stenseke, M.; Henningsson, S.; Tim, G. Openness as a key-variable for analysis of management trade-offs in urban woodlands. Urban. For. Urban. Green. 2011, 10, 281–293. [Google Scholar] [CrossRef]
- Lis, A.; Iwankowski, P. Why is dense vegetation in city parks unpopular? The mediative role of sense of privacy and safety. Urban. For. Urban. Green. 2021, 59, 126988. [Google Scholar] [CrossRef]
- An, K.W.; Kim, E.I.; Joen, K.S.; Setsu, T. Effects of forest stand density on human’s physiopsychological changes. J. Fac. Agric. Kyushu Univ. 2004, 49, 283–291. [Google Scholar] [CrossRef]
- Jiang, B.; Chang, C.-Y.; Sullivan, W.C. A dose of nature: Tree cover, stress reduction, and gender differences. Landsc. Urban. Plan. 2014, 132, 26–36. [Google Scholar] [CrossRef]
- Antonio, T.; Luca, S.; Giuseppe, C.; Piermaria, C.; Luigi, P.; Mariagrazia, A. Restorative urban forests: Exploring the relationships between forest stand structure, perceived restorativeness and benefits gained by visitors to coastal Pinus pinea forests. Ecol. Indic. 2018, 90, 594–605. [Google Scholar]
- Hussain, R.I.; Walcher, R.; Eder, R.; Allex, B.; Wallner, P.; Hutter, H.-P.; Bauer, N.; Arnberger, A.; Zaller, J.G.; Frank, T. Management of mountainous meadows associated with biodiversity attributes, perceived health benefits and cultural ecosystem services. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef]
- Arnberger, A.; Eder, R.; Allex, B.; Ebenberger, M.; Hutter, H.P.; Wallner, P.; Bauer, N.; Zaller, J.G.; Frank, T. Health-related effects of short stays at mountain meadows, a river and an urban site—Results from a field experiment. Int. J. Environ. Res. Public Health 2018, 15, 2647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bum-Jin, P.; Katsunori, F.; Tamami, K.; Norimasa, T.; Takahide, K.; Yoshifumi, M. Relationship between psychological responses and physical environments in forest settings. Landsc. Urban. Plan. 2011, 102, 24–32. [Google Scholar]
- Chang, L.; Changan, S.; Minkai, S.; Yu, Y.; Pengcheng, L. Effects of brightness levels on stress recovery when viewing a virtual reality forest with simulated natural light. Urban. For. Urban. Green. 2020, 56, 126865. [Google Scholar]
- Kasetani, T.; Takayama, N.; Park, B.-J.; Furuya, K.; Kagawa, T.; Miyazaki, Y. Relation between light/thermal environment in the forest walking road and subjective estimations for taking in the atmosphere of the forest. J. Jpn. Inst. Lands Arch. 2008, 71, 713–716. [Google Scholar] [CrossRef] [Green Version]
- Bach Pages, A.; Peñuelas, J.; Clarà, J.; Llusià, J.; Campillo i López, F.; Maneja, R. How should forests be characterized in regard to human health? Evidence from existing literature. Int. J. Environ. Res. Public Health 2020, 17, 1027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herzog, T.R.; Kutzli, G.E. Preference and perceived danger in field/forest settings. Environ. Behav. 2002, 34, 819–835. [Google Scholar] [CrossRef]
- Herzog, T.R.; Kropscott, L.S. Legibility, mystery, and visual access as predictors of preference and perceived danger in forest settings without pathways. Environ. Behav. 2004, 36, 659–677. [Google Scholar] [CrossRef] [Green Version]
- Herzog, T.R.; Chernick, K.K. Tranquility and danger in urban and natural settings. J. Environ. Psychol. 2000, 20, 29–39. [Google Scholar] [CrossRef]
- Van der Jagt, A.P.N.; Craig, T.; Anable, J.; Brewer, M.J.; Pearson, D.G. Unearthing the picturesque: The validity of the preference matrix as a measure of landscape aesthetics. Landsc. Urban. Plan. 2014, 124, 1–13. [Google Scholar] [CrossRef]
- Kuper, R. Restorative potential, fascination, and extent for designed digital landscape models. Urban. For. Urban. Green. 2017, 28, 118–130. [Google Scholar] [CrossRef]
- Edwards, D.; Jay, M.; Jensen, F.S.; Lucas, B.; Marzano, M.; Montagné, C.; Peace, A.; Weiss, G. Public preferences for structural attributes of forests: Towards a pan-European perspective. For. Policy Econ. 2012, 19, 12–19. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155. [Google Scholar] [CrossRef]
- An, B.-Y.; Wang, D.; Liu, X.-J.; Guan, H.-M.; Wei, H.-X.; Ren, Z.-B. The effect of environmental factors in urban forests on blood pressure and heart rate in university students. J. For. Res. 2019, 24, 27–34. [Google Scholar] [CrossRef]
- Bach, A.; Maneja, R.; Zaldo-Aubanell, Q.; Romanillos, T.; Llusià, J.; Eustaquio, A.; Palacios, O.; Penuelas, J. Human absorption of monoterpenes after a 2-h forest exposure: A field experiment in a Mediterranean holm oak forest. J. Pharm. Biomed. Anal. 2021, 200, 114080. [Google Scholar] [CrossRef] [PubMed]
- Elsadek, M.; Liu, B.; Lian, Z.; Xie, J. The influence of urban roadside trees and their physical environment on stress relief measures: A field experiment in Shanghai. Urban. For. Urban. Green. 2019, 42, 51–60. [Google Scholar] [CrossRef]
- Lee, J.H.; Park, J.S.; Choi, S. Environmental influence in the forested area toward human health: Incorporating the ecological environment into art psychotherapy. J. Mt. Sci. 2020, 17, 992–1000. [Google Scholar] [CrossRef]
- Oishi, Y.; Kanehama, S.; Hiyane, A.; Taguchi, H. Comparison of Forest Image and Mood Psychological Examination in a Forest Environment Using Profile of Mood States and Semantic Differential Method. J. Jpn. For. Soc. 2003, 85, 70–77. [Google Scholar]
- Saito, H.; Horiuchi, M.; Takayama, N.; Fujiwara, A. Effects of managed forest versus unmanaged forest on physiological restoration from a stress stimulus, and the relationship with individual traits. J. For. Res. 2019, 24, 77–85. [Google Scholar] [CrossRef]
- Simkin, J.; Ojala, A.; Tyrväinen, L. Restorative effects of mature and young commercial forests, pristine old-growth forest and urban recreation forest—A field experiment. Urban. For. Urban. Green. 2020, 48, 126567. [Google Scholar] [CrossRef]
- Takayama, N.; Fujiwara, A.; Saito, H.; Horiuchi, M. Management Effectiveness of a Secondary Coniferous Forest for Landscape Appreciation and Psychological Restoration. Int. J. Environ. Res. Public Health 2017, 14, 800. [Google Scholar] [CrossRef] [Green Version]
- Takayama, N.; Saito, H.; Fujiwara, A.; Horiuchi, M. The effect of slight thinning of managed coniferous forest on landscape appreciation and psychological restoration. Prog. Earth Planet. Sci. 2017, 4, 17. [Google Scholar] [CrossRef] [Green Version]
- Yu, C.-P.; Lin, C.-M.; Tsai, M.-J.; Tsai, Y.-C.; Chen, C.-Y. Effects of short forest bathing program on autonomic nervous system activity and mood states in middle-aged and elderly individuals. Int. J. Environ. Res. Public Health 2017, 14, 897. [Google Scholar] [CrossRef]
- Zhou, C.; Yan, L.; Yu, L.; Wei, H.; Guan, H.; Shang, C.; Chen, F.; Bao, J. Effect of Short-term Forest Bathing in Urban Parks on Perceived Anxiety of Young-adults: A Pilot Study in Guiyang, Southwest China. Chin. Geogr. Sci. 2019, 29, 139–150. [Google Scholar] [CrossRef] [Green Version]
- FAO. Forests for Human Health and Well-Being—Strengthening the Forest–Health–Nutrition Nexus; Forestry Working Paper No. 18; FAO: Rome, Italy, 2020; pp. 23–39. [Google Scholar]
- Jäppinen, J.; Tyrväinen, L.; Reinikainen, M.; Ojala, A. Nature for Health and Well-Being in Finland–results and recommendations from the Argumenta project Ecosystem Services and Human Health (2013–2014). Rep. Finn. Environ. Inst. 2014, 35, 104. [Google Scholar]
- Maller, C.; Townsend, M.; St Leger, L.; Henderson-Wilson, C.; Pryor, A.; Prosser, L.; Moore, M. The Health Benefits of Contact with Nature in a Park Context: A Review of Relevant Literature; Deakin University and Parks Victoria: Melbourne, Australia, 2008. [Google Scholar]
- Li, Q. Forest Bathing: How Trees Can. Help You Find Health and Happiness; Penguin: London, UK, 2018. [Google Scholar]
- Kotte, D.; Li, Q.; Shin, W.S.; Michalsen, A. International Handbook of Forest Therapy; Cambridge Scholars Publishing: Cambridge, UK, 2019. [Google Scholar]
- Corazon, S.; Stigsdotter, U.; Claudi Jensen, A.G.; Nilsson, K. Development of the nature-based therapy concept for patients with stress-related illness at the Danish Healing Forest Garden Nacadia. J. Ther. Hortic. 2010, 20, 33–51. [Google Scholar]
- Stamps, A.E. Mystery, complexity, legibility and coheren.n.nce: A meta-analysis. J. Environ. Psychol. 2004, 24, 1–16. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PICO | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Participants | Humans who are healthy or not | Studies not including human participants |
| Intervention | Activities Spending time in the forest or urban forest (e.g., forest walking, forest viewing, forest bathing, forest therapy) Undertaken area Studies should describe forest environment in terms of stand density or canopy density (e.g., stand density, tree density, trees/ha, basal area, canopy density, canopy openness, canopy closure, sky view factor, etc.) | Studies with the intervention that does not match with defined activities Studies not reporting stand density nor canopy density |
| Comparator | Studies with a control site or not | NA |
| Outcome | Studies should report quantitative outcomes related to cognitive restoration, psychological restoration, physiological relaxation, stress reduction. | Studies not including quantitative outcomes |
| PICO | Keywords |
|---|---|
| Intervention Activities | “forest therapy” OR “forest bathing” OR “shinrin-yoku” OR “shinrin yoku” OR “forest walk” OR “forest walking” OR “forest recreation” OR “nature therapy” OR “forest trip” OR “forest visit” OR (“trip” NEAR “forest”) OR (“visit” NEAR “forest”) OR (“spending time” NEAR “forest”) OR (“walking” NEAR “forest”) OR (“viewing” NEAR “forest”) |
| Undertaken Area | “stand density” OR “tree density” OR “strains/ha” OR “stands/ha” OR “trees/ha” OR “basal area” OR “canopy density” OR “canopy openness” OR “canopy closure” OR “sky view factor” OR “gap light analysis” OR (“managed” NEAR “forest”) OR (“unmanaged” NEAR “forest”) OR (“thinned” NEAR “forest”) OR (“unthinned” NEAR “forest”) OR “thinned condition” OR “unthinned condition” OR “thinning intensity” OR (“light environment” NEAR “tree vegetation”) OR (“light environment” NEAR “trees”) OR (“environmental factor” NEAR “forest”) OR (“environmental factor” NEAR “tree vegetation”) OR (“environmental factor” NEAR “trees”) OR (“microclimate” NEAR “forest”) OR (“microclimate” NEAR “tree vegetation”) OR (“microclimate” NEAR “trees”) OR (“physical environment” NEAR “forest”) OR (“physical environment” NEAR “tree vegetation”) OR (“physical environment” NEAR “trees”) OR (“forest” NEAR “structure”) OR “forest landscapes” OR “forest sites” OR “forests” |
| Outcome | “health” OR “well-being” OR “well-being” OR “psychological” OR “physiological” OR “psycho-physiological” OR “restorativeness” OR “restorative effect” OR “restorative experience” OR “psychological restoration” OR “PRS” OR “perceived restorativeness schedule” OR “ROS” OR “restorative outcome scale” OR “mood” OR “affective state” OR “POMS” OR “profile and mood state questionnaire” OR “PANAS” OR “positive and negative affect schedule” OR “anxiety” OR “STAI” OR “Spielberger state-trait anxiety inventory” OR “self-reporting anxiety scale” OR “depression” OR “BDI” OR “Beck depression inventory” OR “self-reporting depression scale” OR “vitality” OR “SVS” OR “subjective vitality scale” OR “psychological relaxation” OR “physiological relaxation” OR “psycho-physiological relaxation” OR “psychological response” OR “physiological response” OR “blood pressure” OR “SBP” OR “systolic blood pressure” OR “DBP” OR “diastolic blood pressure” OR “pulse rate” OR “heart rate” OR “HRV” OR “heart rate variability” OR “SDNN” OR “RMSSD” OR “LF” OR “HF” OR “LF/HF” OR “skin conductance” OR “SCR” OR “brain wave” OR “prefrontal activity” OR “SpO2” OR “EEG” OR stress reduction” OR “stress recovery” OR “stress restoration” OR “cortisol” OR “saliva” |
| First Author and Year | Sample Size (M/F) | Participant Characteristics | Stand Density (Trees/ha) | DBH (cm) | Canopy Density | Forest Characteristics | Environmental Characteristics | Outcome Measurement | Activity Type | Time of Measure | Study Design | |||||
| An 2019 [84] | 13 (7/6) | Healthy university students Age: 21.8 ± 1.9 | 3 different forest sites (no control assigned) | Location: 4351′ N, 12518′ E | Temp: 18 °C (10–25 °C) Relative humidity: 45% Wind speed: 3.33 m/s | SBP; DBP; HR | Staying (30 min) | Sep, 2017 (8:30–12:00) | Randomized Cross-over | |||||||
| 1667/ha | 13.26 | 0.56 | Betula platyphylla | Illuminance: 4617 lx | SBP(/); DBP(/); HR(/) | |||||||||||
| 1867/ha | 10.35 | 0.75 | Acer triflorum | Illuminance: 1124 lx | SBP(/); DBP(/); HR(+) | |||||||||||
| 1993/ha | 14.39 | 0.78 | Quercus mongolica | Illuminance: 1012 lx | SBP(+/); DBP(+/); HR(+/) | |||||||||||
| Bach 2021 [85] | 10 (6/4) | Healthy university students with no abnormalities in the respiratory or immune system Age: 36.4 ± 6.5 | One forest site and urban site (control) | Location: N, 2 E Altitude: 860–972 m Dominant species: Quercus ilex | Temp: 23.87 ± 0.18 °C Relative humidity: 53.7% | Blood concentration of Alpha-pinene(/); Beta-pinene(/); Alpha-phellandrene(/); Limonene(/); All monoterpene(/) | Walking (120 min) | July, 2018 (10:00–12:00) | Randomized Controlled Trial | |||||||
| 10500/ha | 6.43 | 0.95 | ||||||||||||||
| Bielinis 2019 [27] | 21 (12/9) | Healthy university students and non-student volunteers with no mental or physical diseases or metabolic syndromes Age: 23.9 ± 2.7 | One forest group (no control) | Location: N, 20 E Dominant species: Picea abies and Pinus sylvestris | Temp: 25 °C Relative humidity: 46% Wind speed: 6.11 m/s Noise: 38.08 ± 5.19 dB Illuminance: 37755.24 lx | SBP(+); DBP(/); PR(+); MAP(+); POMS(Confusion(+) Fatigue(+/) Anger(+) Anxiety(+) Depression(+) Vigor(/)); PANAS(PA(/) NA(+)); ROS(+); SVS(+) | Staying (60 min) | May, 2018 (15:45–16:15) | Uncontrolled Before and After | |||||||
| 1200/ha | NA | NA | ||||||||||||||
| Elsadek 2019 [86] | 346 (200/164) | Healthy university students with no mental or physical diseases Age: 23.0 ± 4.6 | 3 different forest sites and urban site(control) | Location: N, E | POMS; STAI; ROS; SVS; PET | Walking (15 min) | May, 2018 (10:00–15:30) | Randomized Crossover | ||||||||
| NA | NA | 0.13 | Urban road (control) | Temp: 31.8 °C Relative humidity: 42.8% Wind speed: 0.66 m/s | POMS(Anxiety(−) Depression(−) Anger(−) Fatigue(−) Confusion(−) Vigor(−)); STAI(−); ROS(−); SVS(−) | |||||||||||
| 0.49 | Prunus serrulata | Temp: 31.2 °C Relative humidity: 47.0% Wind speed: 0.23 m/s | POMS(Anxiety(+) Depression(+) Anger(+) Fatigue(+) Confusion(+) Vigor(+)); STAI(+); ROS(+); SVS(+) | |||||||||||||
| 0.89 | Plantanus hispanica | Temp: 29.0 °C Relative humidity: 50.9% Wind speed: 0.15m/s | POMS(Anxiety(+) Depression(+) Anger(+) Fatigue(+) Confusion(+) Vigor(+)); STAI(+); ROS(+); SVS(+) | |||||||||||||
| 0.94 | Metasequoia glyptroboides | Temp: 28.1 °C Relative humidity: 52.9% Wind speed: 0.11 m/s | POMS(Anxiety(+) Depression(+) Anger(+) Fatigue(+) Confusion(+) Vigor(+)); STAI(+); ROS(+); SVS(+) | |||||||||||||
| Lee 2020 [87] | 16 (5/11) | Housewives, freelancers and office workers Age: 41.6 ± 1.8 | One forest site and one outdoor site(control) | Location: N, 128 E Dominant species: Pinus rigida and Quercus aliena | NA | DEP(+/); ANX(+/); AGG(/); ST-IN-S(+); ST-V-RG-P(+) | Staying (120 min) | May–Aug, 2017 | Controlled Before and After | |||||||
| 156/ha | 27.4 | NA | ||||||||||||||
| Oishi 2003 [88] | 44 (23/21) | Healthy residents including students and workers Age: 24.4 ± 9.9 | 5 different forest sites and one site outside the forest(control) | Location: 39 N, E | POMS | Staying (10 min) | Jul–Sep, 2001 (8:45–13:10) | Non-Randomized Cross-over | ||||||||
| 250/ha | 23 | NA | Pinus densiflora | Temp: 19.67 ± 3.31 °C Relative humidity: 68.9% | POMS(Anxiety(+) Depression(+) Anger(+) Fatigue(+) Confusion(+) Vigor(+)) | |||||||||||
| 750/ha | 34.9 | Cyptomeria japonica | Temp: 20.29 ± 3.66 °C Relative humidity: 69.3% | POMS(Anxiety(+) Depression(+) Anger(+) Fatigue(+) Confusion(+) Vigor(+)) | ||||||||||||
| 1700/ha | 10.6 | Quercus serrata | Temp: 19.91 ± 3.40 °C Relative humidity: 75.8% | POMS(Anxiety(+) Depression(+) Anger(+) Fatigue(+) Confusion(+) Vigor(+)) | ||||||||||||
| 2275/ha | 10.4 | Pinus densiflora Machilus thunbergii | Temp: 20.17 ± 3.19 °C Relative humidity: 73.3% | POMS(Anxiety(+) Depression(+) Anger(+) Fatigue(+) Confusion(+) Vigor(+)) | ||||||||||||
| 2875/ha | 9.5 | Pinus densiflora Quercus serrata | Temp: 18.63 ± 3.16 °C Relative humidity: 76.4% | POMS(Anxiety(+) Depression(+) Anger(+) Fatigue(+) Confusion(+) Vigor(+)) | ||||||||||||
| Saito 2019 [89] | 17 (17/-) | healthy male volunteer had no history of cardiovascular disease or mental illness Age: 40.2 ± 6.2 | 2 different forest sites: managed forest and unmanaged forest(control) | Location: N, 138 E | Wind speed: m/s | SBP; DBP; MAP; HR; HF; LF/HF; saliva cortisol | Staying (15 min) | July, 2014 | Randomized Crossover | |||||||
| 1024/ha | 19.78 | 0.62 | Mixed forest (Broadleaf trees: 82% Coniferous trees: 18%) | Temp: 24.3 ± 2.8 °C Relative humidity: 73.3% Illuminance: 255.0 ± 97.6 lx | SBP(+); DBP(+); MAP(+); HR(/); HF(+/); LF/HF(+); saliva cortisol(+) | |||||||||||
| 1208/ha | 15.75 | 0.91 | Mixed forest (Broadleaf trees: 50% Coniferous trees: 50%) | Temp: 24.2 ± 2.8 °C Relative humidity: 70.0% Illuminance: 119.2 ± 48.5 lx | SBP(+); DBP(+); MAP(+); HR; HF(−/); LF/HF(−); saliva cortisol(+/) | |||||||||||
| Simkin 2020 [90] | 66 (41/59) | City workers aged from 26–65 Age: 43.4 ± 10.7 | 4 different forest sites (no control assigned) | Picea abies-dominated forests in Finland | ROS; SVS; PANAS | Staying (15 min) and Walking (45 min) | Aug–Oct, 2016 April–June, 2017 (15:00–17:00) | Randomized Crossover | ||||||||
| 374/ha | 35 | NA | Location: N, 25 E (stand age > 120) | Temp: 12.8 ± 4.4 °C Relative humidity: 39–96% | ROS(+); SVS(+); PANAS(+) | |||||||||||
| 424/ha | 30 | Location: N, 24 E (stand age: 95) | Temp: 15.8 ± 4.2 °C Relative humidity: 29–100% | ROS(+); SVS(+); PANAS(+) | ||||||||||||
| 520/ha | 28 | Location: N, 25 E (stand age: 100) | Temp: 15.9 ± 5.8 °C Relative humidity: 39–91% | ROS(+); SVS(+); PANAS(+) | ||||||||||||
| 1746/ha | 16 | Location: N, 25 E (stand age: 40) | Temp: 15.3 ± 4.8 °C Relative humidity: 27–98% | ROS(+); SVS(+); PANAS(+) | ||||||||||||
| Takayama 2017a [91] | 18 (18/-) | Healthy male volunteer without history of cardiovascular disease or mental illness Age: 40.2 ± 6.4 | 2 different forest sites: managed forest and unmanaged forest(control) | Location: N, 13886′ E | POMS; PANAS; ROS; PRS | Staying (15 min) | July, 2014 | Randomized Crossover | ||||||||
| 1056/ha | 23.12 | 0.62 | Larix kaempferi 66%, Cornus controversa 10% Pinus densiflora 7% | Temp: 24.3 ± 7.9 °C Relative humidity: 73 ± 39% Wind velocity: /s Radiant Heat: 25.5 ± 10.5 °C Illuminance: 255.0 ± 97.6 lx Noise: 41.5 ± 3.8 dB | POMS(Anxiety(+) Depression(/) Anger(/) Fatigue(+/) Confusion(+) Vigor(+)); PANAS(PA(/)NA(+)); ROS(+) | |||||||||||
| 1212/ha | 18.54 | 0.91 | Larix kaempferi 66% Cornus controversa 7% Pinus densiflora 7% | Temp: 24.2 ± 7.6 °C Relative humidity: 70 ± 34% Wind velocity: m/s Radiant Heat: 25.3 ± 9.8 °C Illuminance: 119.2 ± 48.5 lx Noise: 39.0 ± 3.9 dB | POMS(Anxiety(+) Depression(/) Anger(/) Fatigue(/) Confusion(+) Vigor(+)); PANAS(PA(/)NA(+/)) ROS(/) | |||||||||||
| Takayama 2017 [92] | 15 (11/4) | University students and mid-aged faculties without had no history of cardiovascular disease or mental illness Age: 35.9 ± 8.2 | 2 different forest sites: thinned forest and unthinned forest(control) | Location: 35°41′ N, 138°86′ E | POMS; PANAS; ROS; PRS | Staying (15 min) | Oct, May, 2013 | Randomized Crossover | ||||||||
| 1056/ha | 23.12 | 0.52 | Larix kaempferi 66%, Cornus controversa 10% Pinus densiflora 7% | Temp: 18.6 ± 0.92 °C Relative humidity: 92% Wind velocity: m/s Radiant Heat: 18.8 °C Illuminance: 336172 lx | POMS(Anxiety(+) Depression(+) Anger(+) Fatigue(+/) Confusion(+) Vigor(/)); PANAS(PA(/)NA(/)) ROS(+/) | |||||||||||
| 1200/ha | 22.76 | 0.59 | Larix kaempferi 66%, Cornus controversa 10% Pinus densiflora 7% | Temp: 17.1.52 °C Relative humidity: 38% Wind velocity: m/s Radiant Heat: 21.8 °C Illuminance: 668 lx | POMS(Anxiety(+) Depression(+) Anger(/) Fatigue(+) Confusion(+) Vigor(/)); PANAS(PA(/)NA(/)) ROS(+) | |||||||||||
| Yu [93] | 123 (43/85) | Middle-aged and elderly subjects aged 45 to 86 years No disease (n = 69), hypertension (n = 25), diabetes (n = 9), heart disease (n = 8) Age: 60.0 ± 7.4 | One forest site (no control) | Location: N, 121 E Dominant species: Cryptomeria japonica | Temp: 22.6 °C Relative humidity: 87.4% Wind speed: 0.1 m/s | PR(+); SBP(+); DBP(+); HF(/); LF/HF(/); POMS(Anxiety(+) Depression(+) Anger(+) Fatigue(+) Confusion(+) Vigor(+)); STAI(+) | Walking (180 min) | July, 2016 (8:30–12:00) | Uncontrolled Before and After | |||||||
| 1200/ha | NA | NA | ||||||||||||||
| Zhou 2019 [94] | 43 (8/35) | University students free from diagnosed cardiovascular, allergic, physical disease, or mental diseases Age: 20.8 ± 0.9 | 2 different forest sites (no control assigned) | Location: N– N 106 E–107 E | Temp: 22.6 °C Relative humidity: 87.4% Wind speed: 0.1 m/s | Anti-anxiety scores | walking (60 min) | Dec, 2016 | Randomized Cross-over | |||||||
| NA | NA | 0.20–0.75 | Cinnamomum camphora Quercus fabri Platanus acerifolia | Anti-anxiety scores (financial states(+); exam pressure(+); campus life(/); love affair relationship(+)) | ||||||||||||
| 0.50–0.75 | Cinnamomum camphora Celtis sinensis Catalpa bungei Celtis sinensis | Anti-anxiety scores(financial states(+); exam pressure(+); campus life(+); love affair relationship(/)) | ||||||||||||||
| Study | Pre-Intervention | At Intervention | Post-Intervention | Overall Risk of Bias | |||||
|---|---|---|---|---|---|---|---|---|---|
| First Author | Year | Bias Due to Confounding | Bias in Selection of Participants into the Study | Bias in Classification of Interventions | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of the Reported Result | |
| An | 2019 | Low | Low | Low | Low | Low | Low | Moderate | Moderate |
| Bach | 2021 | Low | Low | Low | Low | Low | Low | Low | Low |
| Bielinis | 2019 | Low | Moderate | Low | Low | Low | Moderate | Moderate | Moderate |
| Elsadek | 2019 | Low | Moderate | Low | No Information | No Information | Moderate | Moderate | No information |
| Lee | 2020 | Serious | Moderate | Low | Low | Low | Moderate | Moderate | Serious |
| Oishi | 2003 | Serious | Moderate | Low | Low | Low | Moderate | Moderate | Serious |
| Saito | 2019 | Low | Low | Low | Low | Low | Low | Moderate | Moderate |
| Simkin | 2020 | Low | Low | Low | Low | Low | Moderate | Moderate | Moderate |
| Takayama | 2017a | Low | Low | Low | Low | Low | Moderate | Serious | Serious |
| Takayama | 2017b | Low | Low | Low | Low | Low | Moderate | Moderate | Moderate |
| Yu | 2017 | Low | Moderate | Low | Low | Low | Moderate | Moderate | Moderate |
| Zhou | 2019 | Low | Low | Low | Low | Low | Moderate | Moderate | Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, E.; Park, S.; Kim, S.; Choi, Y.; Cho, J.; Cho, S.-i.; Chun, H.-r.; Kim, G. Can Different Forest Structures Lead to Different Levels of Therapeutic Effects? A Systematic Review and Meta-Analysis. Healthcare 2021, 9, 1427. https://doi.org/10.3390/healthcare9111427
Kim E, Park S, Kim S, Choi Y, Cho J, Cho S-i, Chun H-r, Kim G. Can Different Forest Structures Lead to Different Levels of Therapeutic Effects? A Systematic Review and Meta-Analysis. Healthcare. 2021; 9(11):1427. https://doi.org/10.3390/healthcare9111427
Chicago/Turabian StyleKim, Eunsoo, Sujin Park, Soojin Kim, Yeji Choi, Junghee Cho, Sung-il Cho, Hae-ryoung Chun, and Geonwoo Kim. 2021. "Can Different Forest Structures Lead to Different Levels of Therapeutic Effects? A Systematic Review and Meta-Analysis" Healthcare 9, no. 11: 1427. https://doi.org/10.3390/healthcare9111427
APA StyleKim, E., Park, S., Kim, S., Choi, Y., Cho, J., Cho, S.-i., Chun, H.-r., & Kim, G. (2021). Can Different Forest Structures Lead to Different Levels of Therapeutic Effects? A Systematic Review and Meta-Analysis. Healthcare, 9(11), 1427. https://doi.org/10.3390/healthcare9111427