
Proprioceptive Neuromuscular Facilitation Kinesio Taping Improves Range of Motion of Ankle Dorsiflexion and Balance Ability in Chronic Stroke Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Outcome Measurements
2.3.1. Ankle DF-ROM
2.3.2. Balance Ability
2.4. Interventions and Procedures
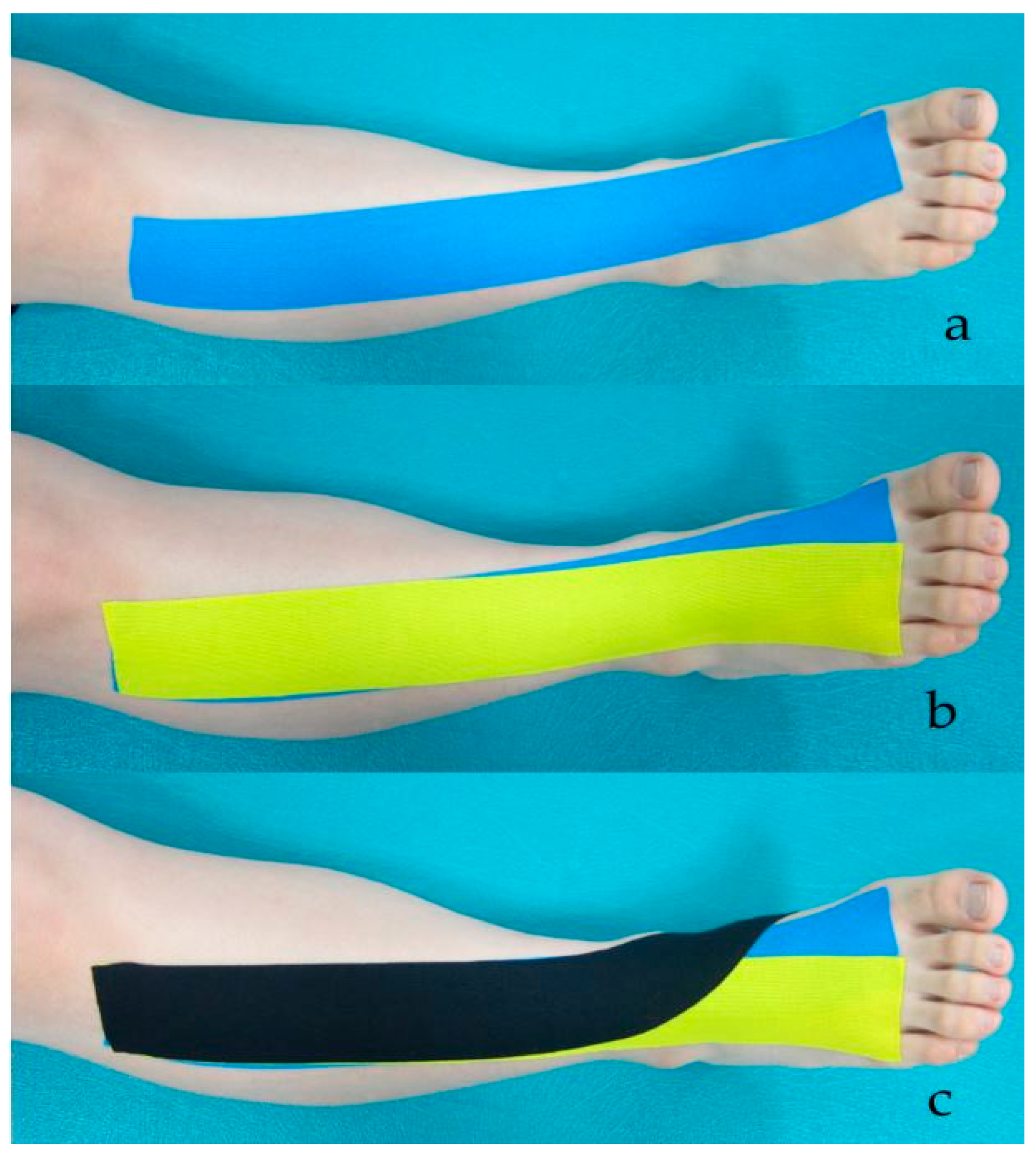
2.4.1. A-KT
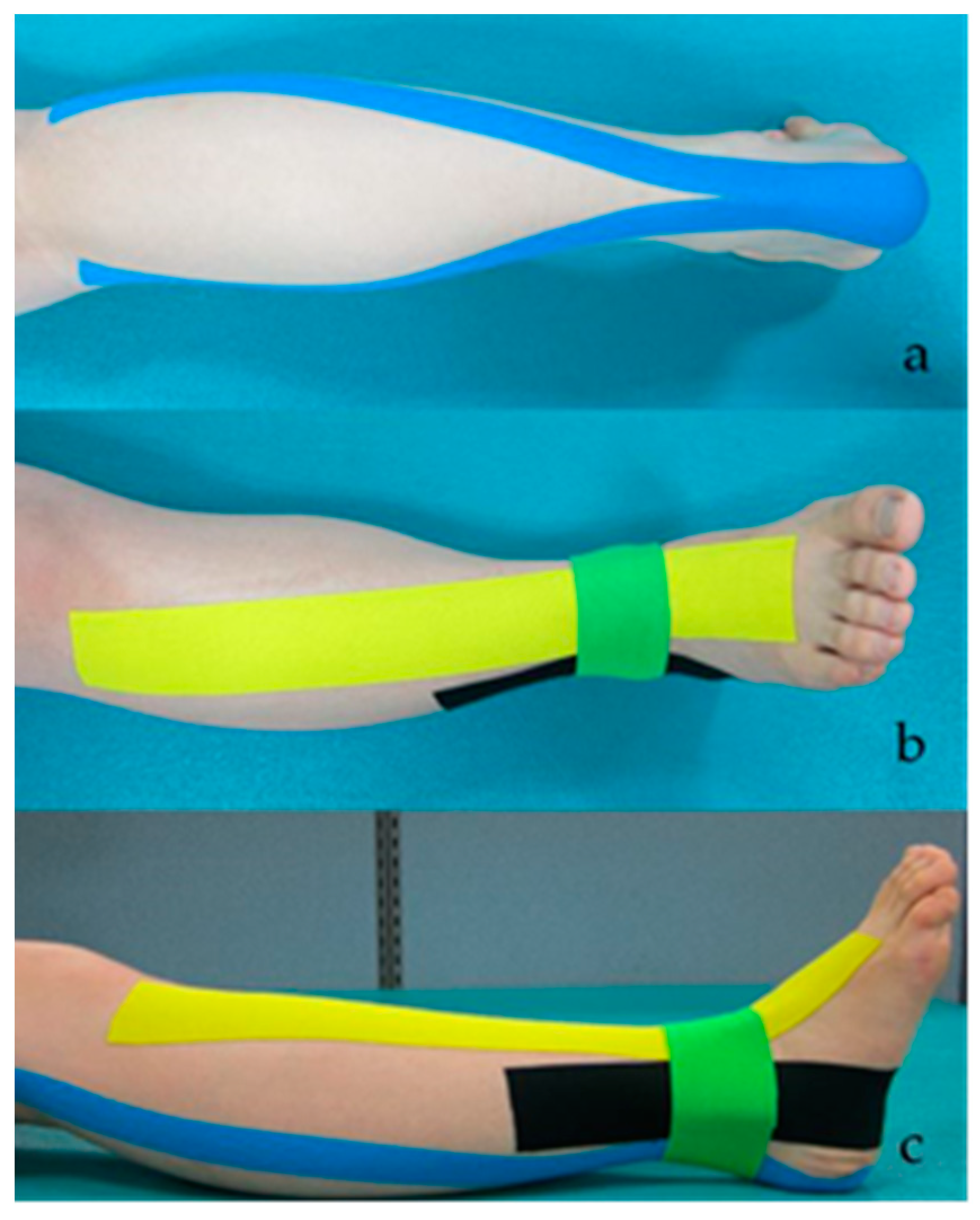
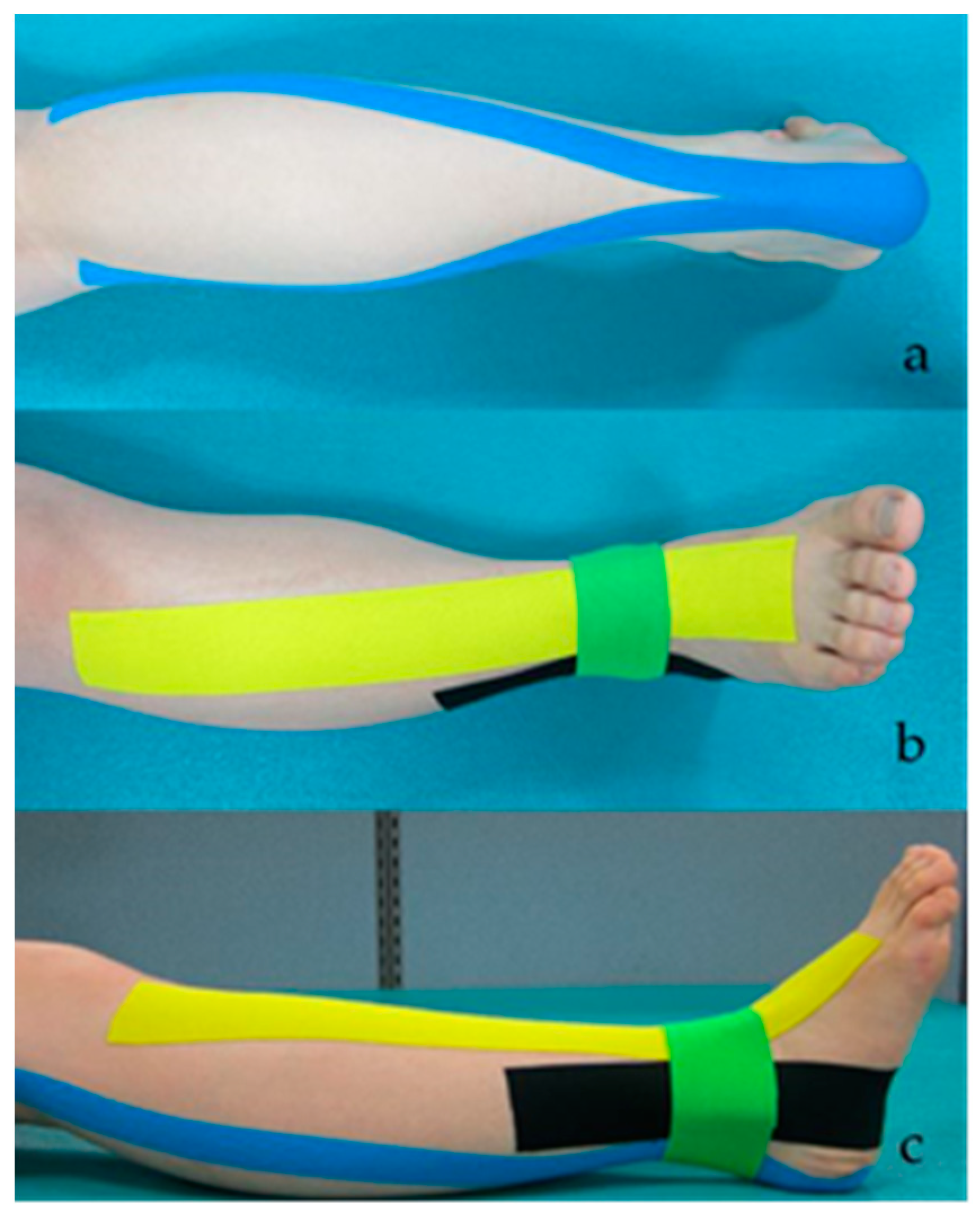
2.4.2. PNF Taping
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Donkor, E.S. Stroke in the 21st Century: A Snapshot of the Burden, Epidemiology, and Quality of Life. Stroke Res Treat. 2018, 2018, 3238165. [Google Scholar] [PubMed] [Green Version]
- Gorst, T.; Rogers, A.; Morrison, S.C.; Cramp, M.; Paton, J.; Freeman, J.; Marsden, J. The prevalence, distribution, and functional importance of lower limb somatosensory impairments in chronic stroke survivors: A cross sectional observational study. Disabil. Rehabil. 2019, 41, 2443–2450. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.T.; Chen, C.L.; Wang, C.M.; Hong, W.H. Leg muscle activation patterns of sit-to-stand movement in stroke patients. Am. J. Phys. Med. Rehbil. 2004, 83, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Zissimopoulos, A.; Fatone, S.; Gard, S. The effect of ankle–foot orthoses on self-reported balance confidence in persons with chronic poststroke hemiplegia. Prosthet. Orthot. Int. 2014, 38, 148–154. [Google Scholar] [CrossRef] [Green Version]
- Anker, L.C.; Weerdesteyn, V.; van Nes, I.J.; Nienhuis, B.; Straatman, H.; Geurts, A.C. The relation between postural stability and weight distribution in healthy subjects. Gait Posture. 2008, 27, 471–477. [Google Scholar] [CrossRef]
- Adegoke, B.; Olaniyi, O.; Akosile, C.O. Weight bearing asymmetry and functional ambulation performance in stroke survivors. Glob. J. Health Sci. 2012, 4, 87–94. [Google Scholar] [CrossRef] [Green Version]
- de Haart, M.; Geurts, A.C.; Huidekoper, S.C.; Fasotti, L.; van Limbeek, J. Recovery of standing balance in postacute stroke patients: A rehabilitation cohort study. Arch. Phys. Med. Rehabil. 2004, 85, 886–895. [Google Scholar] [CrossRef]
- Karthikbabu, S.; Verheyden, G. Relationship between trunk control, core muscle strength and balance confidence in community-dwelling patients with chronic stroke. Top Stroke Rehabil. 2021, 28, 88–95. [Google Scholar] [CrossRef]
- Shahabi, S.; Shabaninejad, H.; Kamali, M.; Jalali, M.; Ahmadi Teymourlouy, A. The effects of ankle-foot orthoses on walking speed in patients with stroke: A systematic review and meta-analysis of randomized controlled trials. Clin. Rehabil. 2020, 34, 145–159. [Google Scholar] [CrossRef]
- Shariat, A.; Najafabadi, M.G.; Ansari, N.N.; Cleland, J.A.; Singh, M.A.F.; Memari, A.H.; Honarpishe, R.; Hakakzadeh, A.; Ghaffari, M.S.; Naghdi, S. The effects of cycling with and without functional electrical stimulation on lower limb dysfunction in patients post-stroke: A systematic review with meta-analysis. NeuroRehabilitation 2019, 44, 389–412. [Google Scholar] [CrossRef]
- Tyson, S.F.; Kent, R.M. Effects of an ankle-foot orthosis on balance and walking after stroke: A systematic review and pooled meta-analysis. Arch. Phys. Med. Rrehabil. 2013, 94, 1377–1385. [Google Scholar] [CrossRef] [PubMed]
- Ohata, K.; Yasui, T.; Tsuboyama, T.; Ichihashi, N. Effects of an ankle-foot orthosis with oil damper on muscle activity in adults after stroke. Gait Posture 2011, 33, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Bulley, C.; Shiels, J.; Wilkie, K.; Salisbury, L. User experiences, preferences and choices relating to functional electrical stimulation and ankle foot orthoses for foot-drop after stroke. Physiotherapy 2011, 97, 226–233. [Google Scholar] [CrossRef] [Green Version]
- Koseoglu, B.F.; Dogan, A.; Tatli, H.U.; Ozcan, D.S.; Polat, C.S. Can kinesio tape be used as an ankle training method in the rehabilitation of the stroke patients? Complement Ther. Clin. Pract. 2017, 27, 46–51. [Google Scholar] [CrossRef]
- Hu, Y.; Zhong, D.; Xiao, Q.; Chen, Q.; Li, J.; Jin, R. Kinesio taping for balance function after stroke: A systematic review and meta-analysis. Evid. Based Complement Alternat Med. 2019, 2019, 8470235. [Google Scholar] [CrossRef] [Green Version]
- Horasart, A.; Klomjai, W.; Bovonsunthonchai, S. Immediate effect of kinesio tape on gait symmetry in patients with stroke: A preliminary study. Human Mov. 2020, 21, 73–81. [Google Scholar] [CrossRef] [Green Version]
- Bae, Y.H.; Kim, H.G.; Min, K.S.; Lee, S.M. Effects of lower-leg kinesiology taping on balance ability in stroke patients with foot drop. Evid.-Based Complementary Altern. Med. 2015, 2015, 125629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheng, Y.; Kan, S.; Wen, Z.; Chen, W.; Qi, Q.; Qu, Q.; Yu, B. Effect of kinesio taping on the walking ability of patients with foot drop after stroke. Evi. Based Complement Alternat. Med. 2019, 2019, 2459852. [Google Scholar]
- Wang, M.; Pei, Z.W.; Xiong, B.D.; Meng, X.M.; Chen, X.L.; Liao, W.J. Use of Kinesio taping in lower-extremity rehabilitation of post-stroke patients: A systematic review and meta-analysis. Complement Ther. Clin. Pract. 2019, 35, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.I.; Park, Y.H.; Sung, Y.B.; Nam, C.W. Effects of kinesio taping for ankle joint and ankle-foot orthosis on muscle stimulation and gait ability in patients with stroke suffering foot drop. Adv. Sci. Technol. 2015, 116, 261–265. [Google Scholar]
- Hegazy, R.M.; Alkhateeb, A.M.; Abdelmonem, A.F.; Mohammed, A. Immediate effect of kinesiotape versus ankle foot orthosis on gait parameters in stroke patients. Turk. J. Physiother Rehabil. 2021, 32, 3. [Google Scholar]
- Rojhani-Shirazi, Z.; Amirian, S.; Meftahi, N. Effects of ankle kinesio taping on postural control in stroke patients. J. Stroke Cerebrovasc. Dis. 2015, 24, 2565–2571. [Google Scholar] [CrossRef]
- Lee, D.; Bae, Y. Short-Term Effect of Kinesio Taping of Lower-Leg Proprioceptive Neuromuscular Facilitation Pattern on Gait Parameter and Dynamic Balance in Chronic Stroke with Foot Drop. Healthcare 2020, 9, 271. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.S.; Jung, J.H.; In, T.S.; Cho, H.Y. Influences of kinesio taping with therapeutic exercise in patients with low back pain. Healthcare 2021, 9, 927. [Google Scholar] [CrossRef]
- Kim, B.R.; Kang, T.W. The effects of proprioceptive neuromuscular facilitation lower-leg taping and treadmill training on mobility in patients with stroke. Int. J. Rehabil. Res. 2018, 41, 343–348. [Google Scholar] [CrossRef]
- Hendrickson, J.; Patterson, K.K.; Inness, E.L.; McIlroy, W.E.; Mansfield, A. Relationship between asymmetry of quiet standing balance control and walking post-stroke. Gait Posture 2014, 39, 177–181. [Google Scholar] [CrossRef]
- Crossover Randomised Controlled Trial: Comparative Studies. Available online: https://www.gov.uk/guidance/crossover-randomised-controlled-trial-comparative-studies (accessed on 21 August 2021).
- Han, C.; Jo, S.A.; Jo, I.; Kim, E.; Park, M.H.; Kang, Y. An adaptation of the Korean mini-mental state examination (K-MMSE) in elderly Koreans: Demographic influence and population-based norms (the AGE study). Arch Gerontol. Geriatr. 2008, 47, 302–310. [Google Scholar] [CrossRef]
- Bessone, V.; Höschele, N.; Schwirtz, A.; Seiberl, W. Validation of a new inertial measurement unit system based on different dynamic movements for future in-field applications. Sports Biomech. 2019, 13, 1–16. [Google Scholar] [CrossRef]
- Ancans, A.; Greitans, M.; Cacurs, R.; Banga, B.; Rozentals, A. Wearable Sensor Clothing for Body Movement Measurement during Physical Activities in Healthcare. Sensors 2021, 21, 2068. [Google Scholar] [CrossRef]
- Yoon, J.D.; Lee, J.N. The Effects of Ankle Mobilization with Movements on the Ankle Range of Motion, Balance, and Gait of Patients after Total Knee Arthroplasty. J. Kor. Acad. Ortho Manu Phys. Ther. 2021, 27, 51–62. [Google Scholar]
- Bessone, V.; Petrat, J.; Schwirtz, A. Ground reaction forces and kinematics of ski jump landing using wearable sensors. Sensors 2019, 19, 2011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Testerman, C.; Vander Griend, R. Evaluation of ankle instability using the Biodex Stability System. Foot Ankle Int. 1999, 20, 317–321. [Google Scholar] [CrossRef]
- Cakar, E.; Durmus, O.; Tekin, L.; Dincer, U.; Kiralp, M. The ankle-foot orthosis improves balance and reduces fall risk of chronic spastic hemiparetic patients. Eur. J. Phys. Rehabil. Med. 2010, 46, 363–368. [Google Scholar] [PubMed]
- Cachupe, W.J.; Shifflett, B.; Kahanov, L.; Wughalter, E.H. Reliability of biodex balance system measures. Meas. Phys. Educ. Exerc. Sci. 2001, 5, 97–108. [Google Scholar] [CrossRef]
- Alghadir, A.H.; Al-Eisa, E.S.; Anwer, S.; Sarkar, B. Reliability, validity, and responsiveness of three scales for measuring balance in patients with chronic stroke. BMC Neurol. 2018, 18, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Shumway-Cook, A.; Baldwin, M.; Polissar, N.L.; Gruber, W. Predicting the probability for falls in community-dwelling older adults. Phys. Ther. 1997, 77, 812–819. [Google Scholar] [CrossRef] [Green Version]
- Jonsdottir, J.; Cattaneo, D. Reliability and validity of the dynamic gait index in persons with chronic stroke. Arch. Phys. Med. Rehabil. 2007, 88, 1410–1415. [Google Scholar] [CrossRef]
- Park, D.; Lee, J.H.; Kang, T.W.; Cynn, H.S. Immediate effects of talus-stabilizing taping on balance and gait parameters in patients with chronic stroke: A cross-sectional study. Top Stroke Rehabil. 2018, 25, 417–423. [Google Scholar] [CrossRef]
- Kase, K.; Wallis, J.; Kase, T. Clinical therapeutic applications of the kinesio taping method. Dalls Kinesio Taping Assoc. 2003, 20–27. [Google Scholar]
- Serrão, J.C.; Mezêncio, B.; Claudino, J.G.; Soncin, R.; Miyashiro, P.L.; Sousa, E.P.; Borges, E.; Zanetti, V.; Phillip, I.; Mochizuki, L.; et al. Effect of 3 Different Applications of Kinesio Taping Denko® on Electromyographic Activity: Inhibition or Facilitation of the Quadriceps of Males During Squat Exercise. J. Sports Sci. Med. 2016, 15, 403–409. [Google Scholar]
- Shin, Y.J.; Lee, J.H.; Choe, Y.W.; Kim, M.K. Immediate effects of ankle eversion taping on gait ability of chronic stroke patients. J. Bodyw. Mov. Ther. 2019, 23, 671–677. [Google Scholar] [CrossRef]
- De Oliveira, C.B.; de Medeiros, Í.R.T.; Ferreira, N.A.; Greters, M.E.; Conforto, A.B. Balance control in hemiparetic stroke patients: Main tools for evaluation. J. Rehabil. Res. Dev. 2008, 45, 1215–1226. [Google Scholar] [CrossRef]
- Geurts, A.C.; De Haart, M.; Van Nes, I.J.; Duysens, J. A review of standing balance recovery from stroke. Gait Posture 2005, 22, 267–281. [Google Scholar] [CrossRef]
- Kim, S.G.; Kim, W.S. Effect of ankle range of motion (ROM) and lower-extremity muscle strength on static balance control ability in young adults: A regression analysis. Med. Sci. Monit. 2018, 24, 3168–3175. [Google Scholar] [CrossRef]
- Kim, K.H.; Lee, Y.J. Immediate effects of kinesio taping of tibialis anterior and ankle joint on mobility and balance ability for chronic hemiparesis: Randomized controlled cross-sectional design. Phys. Med. Rehabil. Kurortmedzin 2020, 23, 350–357. [Google Scholar] [CrossRef]
- Pickerill, M.L.; Harter, R.A. Validity and reliability of limits-of-stability testing: A comparison of 2 postural stability evaluation devices. J. Athl. Train 2011, 46, 600–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, S.H.; Lim, C.G. Immediate Effects of ankle non-elastic taping on balance and gait ability in patients with chronic stroke: A randomized, controlled trial. J. Manip. Physiol. Ther. 2020, 43, 922–929. [Google Scholar] [CrossRef] [PubMed]
- Lokhande, M.V.; Shetye, J.; Mehta, A.; Deo, A. Assessment of knee joint proprioception in weight bearing and in non-weight bearing positions in normal subjects. JKIMSU 2013, 2, 94–101. [Google Scholar]
- Mohammadi, R.; Khorasgani, M.A.; Tabatabaei, M.; Grampurohit, N. Effects of elastic therapeutic taping on joint position sense of the ankle in stroke survivors. Am. J. Phys. Med. Rehabil. 2019, 98, 830–834. [Google Scholar] [CrossRef] [PubMed]
- Saltzman, C.L.; Nawoczenski, D.A. Complexities of foot architecture as a base of support. J. Orthop. Sports Phys. Ther. 1995, 21, 354–360. [Google Scholar] [CrossRef] [PubMed]
- An, C.M.; Won, J.I. Effects of ankle joint mobilization with movement and weight-bearing exercise on knee strength, ankle range of motion, and gait velocity in patients with stroke: A pilot study. J. Phys. Ther. Sci. 2016, 28, 689–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manaf, H.; Justine, M.; Omar, M. Functional balance and motor impairment correlations with gait parameters during Timed Up and Go test across three attentional loading conditions in stroke survivors. Stroke Res. Treat 2014, 2014, 439304. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.P.; Tou, J.I.S.; Mimi, M.T.; Ng, S.S. Reliability and validity of the timed up and go test with a motor task in people with chronic stroke. Arch. Phys. Med. Rehabil. 2017, 98, 2213–2220. [Google Scholar] [CrossRef] [PubMed]
- The Brunnstrom Stages of Stroke Recovery. Available online: https://www.saebo.com/blog/the-stages-of-stroke-recovery/ (accessed on 10 October 2021).

{kind=link}
{kind=link}
| Sex (male/female) | 8/10 |
| Diagnosis (infarction/hemorrhage) | 11/7 |
| Paretic side (left/right) | 10/8 |
| Age (years) | 60.61 ± 13.11 |
| Height (cm) | 165.44 ± 6.17 |
| Weight (kg) | 66.80 ± 6.75 |
| MMSE (score) | 27.12 ± 2.30 |
| Onset time (months) | 11.72 ± 4.02 |
| Range of motion of ankle dorsiflexion (degree) | 7.69 ± 1.02 |
| Brunnstrom motor recovery stage (4/5) | 5/13 |
| Variables | Barefoot | Ankle KT (Δ% *) | PNF-KT (Δ% **) | F | p |
|---|---|---|---|---|---|
| Ankle DF-ROM (°) | 7.69 ± 1.02 | 8.62 ± 1.20 (12.0) | 9.60 ± 1.25 (24.8) | 82.87 | <0.001 abc |
| Static balance (point) | 1.02 ± 0.34 | 0.77 ± 0.37 (24.5) | 0.63 ± 0.34 (38.2) | 26.75 | <0.001 abc |
| TUG (s) | 20.54 ± 4.86 | 19.49 ± 4.33 (5.1) | 18.04 ± 3.64 (12.1) | 15.78 | <0.001 abc |
| Dynamic gait index (point) | 16.61 ± 1.42 | 17.72 ± 16.38 (6.6) | 19.83 ± 0.92 (19.3) | 33.14 | <0.001 abc |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, D.; Bae, Y. Proprioceptive Neuromuscular Facilitation Kinesio Taping Improves Range of Motion of Ankle Dorsiflexion and Balance Ability in Chronic Stroke Patients. Healthcare 2021, 9, 1426. https://doi.org/10.3390/healthcare9111426
Park D, Bae Y. Proprioceptive Neuromuscular Facilitation Kinesio Taping Improves Range of Motion of Ankle Dorsiflexion and Balance Ability in Chronic Stroke Patients. Healthcare. 2021; 9(11):1426. https://doi.org/10.3390/healthcare9111426
Chicago/Turabian StylePark, Donghwan, and Youngsook Bae. 2021. "Proprioceptive Neuromuscular Facilitation Kinesio Taping Improves Range of Motion of Ankle Dorsiflexion and Balance Ability in Chronic Stroke Patients" Healthcare 9, no. 11: 1426. https://doi.org/10.3390/healthcare9111426
APA StylePark, D., & Bae, Y. (2021). Proprioceptive Neuromuscular Facilitation Kinesio Taping Improves Range of Motion of Ankle Dorsiflexion and Balance Ability in Chronic Stroke Patients. Healthcare, 9(11), 1426. https://doi.org/10.3390/healthcare9111426