The Correlation between Social Support and Quality of Life of Seniors without Cognitive Disorders from an Institutional Environment—A Descriptive Cross-Sectional Survey


Abstract
:1. Introduction
2. Materials and Methods
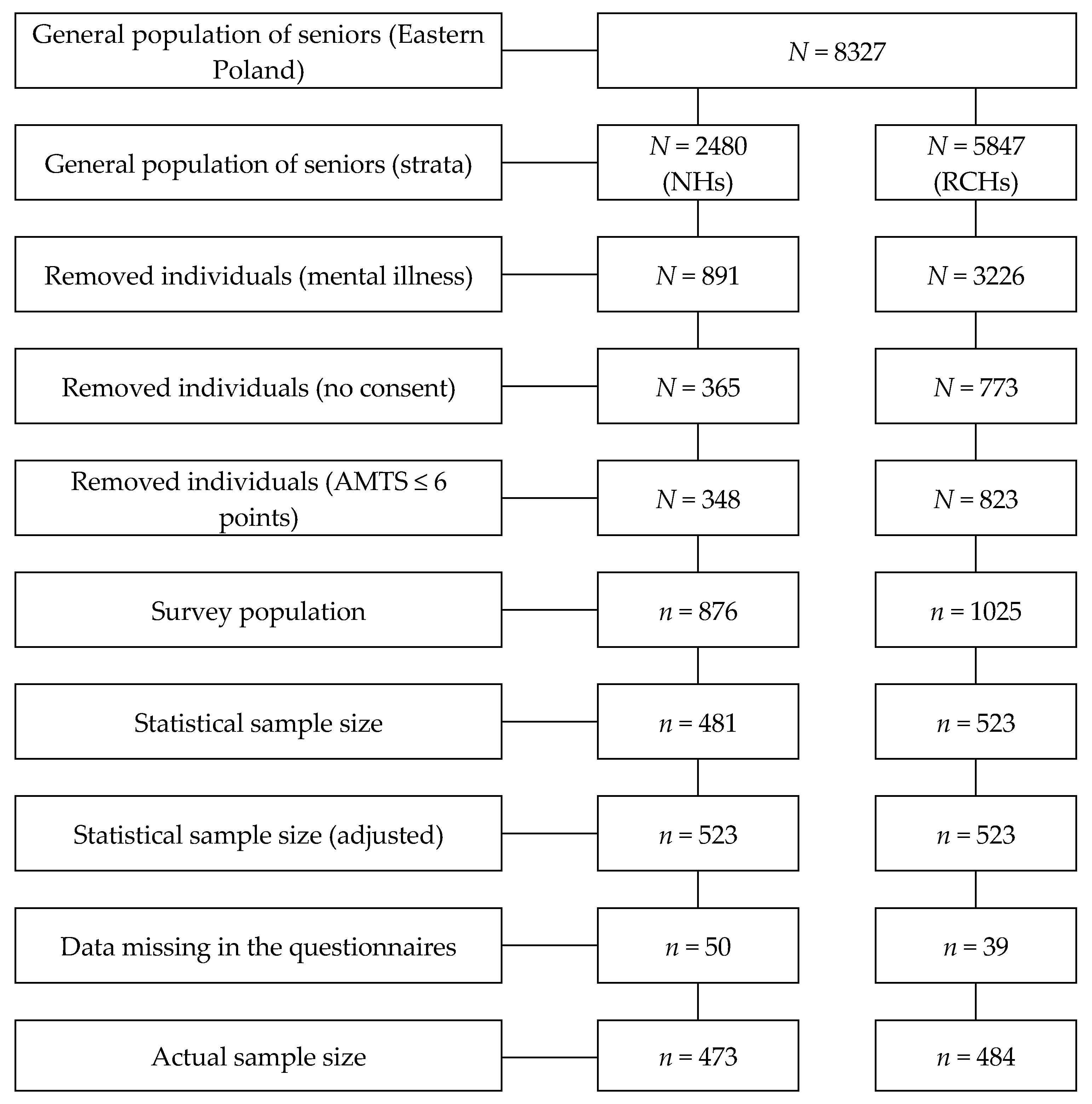
2.1. Respondents
- NH—473 respondents;
- RCH—484 respondents.
- age of ≥ 60 years;
- having a mental state which allowed for the filling in of the questionnaires;
- having written confirmation of willingness to participate in the study.
2.2. Method and Questionnaires
- a.
- WHOQoL-BREF questionnaire—is a shorter variant of the WHOQoL-100 scale which allows to determine the subjective quality of life. The scale was created on the basis of the HRQoL concept. It contains 26 questions which relate to the following components of the quality of life:
- ▪
- general quality of life (question number 1)
- ▪
- general health status (question number 2)
- ▪
- physical domain (questions 3, 4, 10, 15, 16–18)
- ▪
- psychological domain (questions 5–7, 11, 19, 26)
- ▪
- social domain (questions 20–22)
- ▪
- environmental domain (questions 8, 9, 12–14, 23–25)
The questions of questionnaires 1 and 2 were subjected to a separate analysis. The scores for individual domains range from 4 to 20, and from 1 to 5 for questions number 1 and 2. The interpretation of results has a positive direction, whereby the higher the score obtained by the respondent, the better his/her quality of life [23]. - b.
- Social Support Scale—the questionnaire was used to measure social support in functional terms (functional support). The scale is based on the concept of social support assuming the existence of its specific types. It consists of 24 questions and provides information about general support and four types of support:
- ▪
- informational support (questions 1–6);
- ▪
- instrumental support (questions 7–12);
- ▪
- appraisal support (questions 13–18);
- ▪
- emotional support (questions 19–24).
The overall score falls within the range of 24 and 120 points and each type of support falls within the range of 6 and 30 points. The interpretation of results has a negative direction—the higher the score, the lower the functional support and its individual types [24]. - c.
- The Courage Social Network Index—the questionnaire was used to measure social support in structural terms (structural support). The questionnaire was created on the basis of a theoretical model of the function of informal networks. It consists of five questions related to different sources of support: Partner, parents, children, grandchildren, relatives, co-workers, neighbours and friends. The overall score ranges from 0 to 100%. Higher percentages correspond to higher structural support (high number of strong emotional ties as well as frequent direct relations with members of the support network). The interpretation of results has a positive direction [25,26].
- d.
- The Hodgkinson’s Abbreviated Mental Test Score was used to assess the cognitive functions of the seniors. The questionnaire consists of 10 questions and instructions addressed to the respondents. Respondents received 1 point for each time they gave a correct answer or followed an instruction. The score of 6 or less points disqualified the respondent from the study.
2.3. Data Analysis
3. Results
3.1. Verification of Hypothesis 1
3.2. Verification of Hypothesis 2
4. Discussion
4.1. Functional Support and Quality of Life
4.2. Structural Support and Quality of Life
4.3. Nursing Homes vs. Residential Care Homes
4.4. Study Limitations
4.5. Recommendations for Long-Term Nursing Practice
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| NH | nursing homes |
| RCH | residential care homes |
| HRQoL | Health Related Quality of Life |
| WHOQoL-BREF questionnaire | The World Health Organization Quality of Life BREF questionnaire |
References
- Rudawska, I. Epidemiologic and demographic trends as a challenge for European health care systems. Probl. Zarz. 2013, 11, 34–52. [Google Scholar] [CrossRef]
- Drageset, J.; Eide, G.E.; Nygaard, H.A.; Bondevik, M.; Nortvedt, M.W.; Natvig, G.K. The impact of social support and sense of coherence on health-related quality of life among nursing home residents—A questionnaire survey in Bergen, Norway. Int. J. Nurs. Stud. 2009, 46, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Sarla, E.; Lambrinou, E.; Kalokairinou, A.; Sourtzi, P. The relatinship between social support and health related quality of life: Systematic review. Nurs. Care Res. 2016, 46, 224–239. [Google Scholar]
- Wu, M.; Yang, Y.; Zhang, D.; Zhao, X.; Sun, Y.; Xie, H.; Jia, J.; Su, Y.; Li, Y. Association between social support and health-related quality of life among Chinese rural elders in nursing homes: The mediating role of resilience. Qual. Life Res. 2018, 27, 783–792. [Google Scholar] [CrossRef]
- Andrew, N.; Ludwin, B.; Smith, R.; Reyes, R.A.; Meeks, S. The relationship between social support and quality of life in newly admitted long-term care residents. Gerontologist 2015, 55 (Suppl. 2), 452. [Google Scholar] [CrossRef] [Green Version]
- Çimen, M.; Akbolat, M. Perceived social support and life satisfaction of residents in a nursing home in Turkey. Int. J. Health Manag. Tour. 2016, 1, 41–56. [Google Scholar]
- Lai, C.K.; Leung, D.D.; Kwong, E.W.; Lee, R.L. Factors associated with the quality of life of nursing home residents in Hong Kong. Int. Nurs. Rev. 2015, 62, 120–129. [Google Scholar] [CrossRef]
- de Belvis, A.G.; Avolio, M.; Spagnolo, A.; Damiani, G.; Sicuro, L.; Cicchetti, A.; Ricciardi, W.; Rosano, A. Factors associated with health-related quality of life: The role of social relationships among the elderly in an Italian region. Public Health 2008, 122, 784–793. [Google Scholar] [CrossRef] [PubMed]
- García, E.L.; Banegas, J.R.; Pérez-Regadera, A.G.; Cabrera, R.H.; Rodríguez-Artalejo, F. Social network and health-related quality of life in older adults: A population-based study in Spain. Qual. Life Res. 2005, 14, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Street, D.; Burge, S.; Quadagno, J.; Barrett, A. The salience of social relationships for resident well-being in assisted living. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2007, 62, S129–S134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almomani, F.M.; McDowd, J.M.; Bani-Issa, W.; Almomani, M. Health-related quality of life and physical, mental, and cognitive disabilities among nursing home residents in Jordan. Qual. Life Res. 2014, 23, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Zhang, X. Social Network Types and Health among Older Adults in Rural China: The Mediating Role of Social Support. Int. J. Environ. Res. Public Health 2019, 16, 410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, H.T.; Liu, L.F.; Chen, C.K.; Hwang, S.J.; Chen, L.K.; Lu, F.H. Correlates of institutionalized senior veterans’ quality of life in Taiwan. Health Qual. Life Outcomes 2010, 8, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurowska, K.; Błaszczuk, W. Wpływ wsparcia na jakość życia mieszkańców Domu Pomocy Społecznej. Psychogeriatria Pol. 2013, 10, 33–40. [Google Scholar]
- Wang, J.; Wang, J.; Cao, Y.; Jia, S.; Wu, B. Perceived Empowerment, Social Support, and Quality of Life Among Chinese Older Residents in Long-Term Care Facilities. J. Aging Health 2018, 30, 1595–1619. [Google Scholar] [CrossRef] [PubMed]
- Strine, T.W.; Chapman, D.P.; Balluz, L.; Mokdad, A.H. Health-related quality of life and health behaviors by social and emotional support. Their relevance to psychiatry and medicine. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Kasprzak, E. Perceived social support and life-satisfaction. Pol. Psychol. Bull. 2010, 41, 144–154. [Google Scholar] [CrossRef] [Green Version]
- Olejniczak, P. Social Support and Its Importance for the Elderly. Piel. Zdr. Publ 2013, 3, 183–188. [Google Scholar]
- Kurowska, K.; Kajut, A. Self-assessment of the quality of life of aged people on the example of the Social Welfare House residents. Psychogeriatria Pol. 2011, 8, 55–62. [Google Scholar]
- Vitorino, L.; Paskulin, L.; Vianna, L. Quality of Life among older adults resident in long-stay care facilities. Rev. Lat. -Am. Enferm. 2012, 20, 1186–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Blazquez, C.; Forjaz, M.J.; Prieto-Flores, M.E.; Rojo-Perez, F.; Fernandez-Mayoralas, G.; Martinez-Martin, P. Health status and well-being of older adults living in the community and in residential care settings: Are differences influenced by age? Aging Ment. Health 2012, 16, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Kamińska, A.; Bryła, A.; Bodys-Cupak, I. Jakość życia ludzi starszych mieszkających w domach rodzinnych i placówkach opiekuńczo-leczniczych. Pielęgniarstwo XXI Wieku 2012, 4, 117–122. [Google Scholar]
- Jaracz, K.; Kalfoss, M.; Górna, K.; Bączyk, G. Quality of life in Polish respondents: Psychometric properties of the Polish WHOQOL-Bref. Scand. J. Caring Sci. 2006, 20, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Kmiecik-Baran, K. Skala wsparcia społecznego. Teoria i właściwości psychometryczne. Przegl. Psychol. 1995, 38, 201–214. [Google Scholar]
- Zawisza, K.; Gałaś, A.; Tobiasz-Adamczyk, B. Polish version of The Courage Social Network Index—The scale for the assessment of social networks. Gerontol. Pol. 2014, 2, 31–41. [Google Scholar]
- Zawisza, K.; Gałaś, A.; Tobiasz-Adamczyk, B.; Chatterji, S.; Haro, J.M.; Miret, M.; Koskinen, S.; Power, M.; Leonardi, M. The Validity of the Instrument to Evaluate Social Network in the Ageing Population: The Collaborative Research on Ageing in Europe Social Network Index. Clin. Psychol. Psychother. 2014, 21, 227–241. [Google Scholar] [CrossRef]
- Hedayati, H.R.; Hadi, N.; Mostafavi, L.; Akbarzadeh, A.; Montazeri, A. Quality of life among nursing home residents compared with the elderly at home. Shiraz E-Med. J. 2014, 15, e22718. [Google Scholar] [CrossRef]
- Vogel, I.; Miksch, A.; Goetz, K.; Ose, D.; Szecsenyi, J.; Freund, T. The impact of perceived social support and sense of coherence on health-related quality of life in multimorbid primary care patients. Chronic Illn. 2012, 8, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, E.R.A.; Gomes, M.J.; Paiva, K.M. Institutionalization and Quality of life in elderly at metropolitan region in Vitória—ES, Brazil. Esc. Anna Nery 2011, 15, 618–623. [Google Scholar] [CrossRef] [Green Version]
- Top, M.; Dikmetaş, E. Quality of life and attitudes to ageing in Turkish older adults at old people’s homes. Health Expect 2015, 18, 288–300. [Google Scholar] [CrossRef] [Green Version]
- Chou, S.C.; Boldy, D.P.; Lee, A.H. Resident satisfaction and its components in residential aged care. Gerontologist 2002, 42, 188–198. [Google Scholar] [CrossRef] [Green Version]
- Andersson, I.; Pettersson, E.; Sidenvall, B. Daily life after moving into a care home—Experiences from older people, relatives and contact persons. J. Clin. Nurs. 2007, 16, 1712–1718. [Google Scholar] [CrossRef]

{kind=link}
| Variables | NH | RCH | ||||||
|---|---|---|---|---|---|---|---|---|
| M | SD | sk. | kurt. | M | SD | sk. | kurt. | |
| General quality of life | 3.34 | 0.84 | −0.22 | −0.09 | 3.42 | 0.90 | −0.60 | 0.66 |
| General health status | 2.93 | 0.98 | −0.05 | −0.80 | 3.24 | 1.00 | −0.08 | −0.51 |
| Physical | 12.00 | 2.84 | 0.05 | 0.07 | 14.44 | 2.89 | 0.00 | −0.79 |
| Psychological | 12.13 | 2.74 | 0.05 | −0.54 | 13.33 | 2.77 | 0.43 | −0.34 |
| Social | 12.23 | 2.49 | −0.24 | −0.26 | 13.71 | 2.56 | 0.19 | −0.19 |
| Environmental | 13.83 | 2.47 | −0.17 | −0.22 | 14.08 | 2.33 | 0.06 | −0.09 |
| Structural support | 40.42 | 24.65 | −0.24 | −0.95 | 63.38 | 11.02 | −0.29 | −0.17 |
| Functional support | 47.07 | 12.51 | 0.76 | 0.19 | 39.83 | 10.62 | 1.13 | 1.31 |
| Informational support | 11.00 | 3.34 | 0.59 | 0.06 | 9.83 | 3.30 | 0.84 | 0.24 |
| Instrumental support | 13.22 | 3.92 | 0.42 | −0.25 | 11.19 | 3.44 | 0.59 | 0.15 |
| Appraisal support | 13.62 | 3.78 | 0.44 | −0.05 | 11.12 | 3.55 | 1.01 | 1.03 |
| Emotional support | 9.23 | 3.30 | 1.10 | 0.71 | 7.69 | 2.60 | 2.10 | 4.36 |
| Type of Social Support | Test | General Quality of Life | General Health Status | ||
|---|---|---|---|---|---|
| NH | RCH | NH | RCH | ||
| Structural support | r | 0.21 | 0.22 | 0.08 | 0.19 |
| p | <0.001 | <0.001 | 0.084 | <0.001 | |
| Functional support | r | −0.33 | −0.19 | −0.21 | −0.16 |
| p | <0.001 | <0.001 | <0.001 | 0.001 | |
| Informational support | r | −0.20 | −0.08 | −0.12 | −0.12 |
| p | <0.001 | 0.070 | 0.009 | 0.010 | |
| Instrumental support | r | −0.24 | −0.34 | −0.11 | −0.17 |
| p | <0.001 | <0.001 | 0.016 | <0.001 | |
| Appraisal support | r | −0.31 | −0.01 | −0.19 | −0.08 |
| p | <0.001 | 0.807 | <0.001 | 0.097 | |
| Emotional support | r | −0.27 | 0.01 | −0.16 | 0.00 |
| p | <0.001 | 0.755 | 0.001 | 0.928 | |
| Type of Social Support | Test | Physical | Psychological | Social | Environmental | ||||
|---|---|---|---|---|---|---|---|---|---|
| NH | RCH | NH | RCH | NH | RCH | NH | RCH | ||
| Structural support | r | 0.21 | 0.10 | 0.33 | 0.20 | 0.30 | 0.30 | 0.24 | 0.36 |
| p | <0.001 | 0.035 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| Functional support | r | −0.39 | −0.03 | −0.46 | −0.17 | −0.38 | −0.15 | −0.48 | −0.24 |
| p | <0.001 | 0.492 | <0.001 | <0.001 | <0.001 | 0.001 | <0.001 | <0.001 | |
| Informational support | r | −0.28 | −0.07 | −0.31 | −0.20 | −0.25 | −0.15 | −0.32 | −0.24 |
| p | <0.001 | 0.107 | <0.001 | <0.001 | <0.001 | 0.001 | <0.001 | <0.001 | |
| Instrumental support | r | −0.32 | −0.11 | −0.34 | −0.28 | −0.34 | −0.19 | −0.37 | −0.33 |
| p | <0.001 | 0.020 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| Appraisal support | r | −0.34 | −0.03 | −0.44 | −0.04 | −0.25 | −0.05 | −0.42 | −0.11 |
| p | <0.001 | 0.481 | <0.001 | 0.337 | <0.001 | 0.253 | <0.001 | 0.013 | |
| Emotional support | r | −0.24 | 0.15 | −0.38 | 0.06 | −0.29 | 0.01 | −0.38 | −0.03 |
| p | <0.001 | 0.001 | <0.001 | 0.211 | <0.001 | 0.905 | <0.001 | 0.525 | |
| Quality of Life | NH | RCH | Test | 95% CI | d | ||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | t | p | LL | UL | ||
| General quality of life | 3.34 | 0.84 | 3.42 | 0.90 | −1.55 | 0.121 | −0.20 | 0.02 | 0.10 |
| General health status | 2.93 | 0.98 | 3.24 | 1.00 | −4.85 | <0.001 | −0.43 | −0.18 | 0.31 |
| Physical | 12.00 | 2.84 | 14.44 | 2.89 | −13.18 | <0.001 | −2.80 | −2.08 | 0.85 |
| Psychological | 12.13 | 2.74 | 13.33 | 2.77 | −6.78 | <0.001 | −1.56 | −0.86 | 0.44 |
| Social | 12.23 | 2.49 | 13.71 | 2.56 | −9.02 | <0.001 | −1.79 | −1.15 | 0.58 |
| Environmental * | 13.83 | 2.47 | 14.08 | 2.33 | −1.57 | 0.117 | −0.55 | 0.06 | 0.10 |
| Social Support | NH | RCH | Test | 95% CI | d | ||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | t | p | LL | UL | ||
| Structural support * | 40.42 | 24.65 | 63.38 | 11.02 | −18.53 | <0.001 | −25.40 | −20.53 | 1.21 |
| Functional support * | 47.07 | 12.51 | 39.83 | 10.62 | 9.58 | <0.001 | 5.76 | 8.73 | 0.63 |
| Informational support | 11.00 | 3.34 | 9.83 | 3.30 | 5.39 | <0.001 | 0.74 | 1.59 | 0.35 |
| Instrumental support * | 13.22 | 3.92 | 11.19 | 3.44 | 8.46 | <0.001 | 1.56 | 2.51 | 0.55 |
| Appraisal support | 13.62 | 3.78 | 11.12 | 3.55 | 10.36 | <0.001 | 2.01 | 2.95 | 0.68 |
| Emotional support * | 9.23 | 3.30 | 7.69 | 2.60 | 7.95 | <0.001 | 1.17 | 1.93 | 0.52 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chruściel, P.; Dobrowolska, B. The Correlation between Social Support and Quality of Life of Seniors without Cognitive Disorders from an Institutional Environment—A Descriptive Cross-Sectional Survey. Healthcare 2020, 8, 212. https://doi.org/10.3390/healthcare8030212
Chruściel P, Dobrowolska B. The Correlation between Social Support and Quality of Life of Seniors without Cognitive Disorders from an Institutional Environment—A Descriptive Cross-Sectional Survey. Healthcare. 2020; 8(3):212. https://doi.org/10.3390/healthcare8030212
Chicago/Turabian StyleChruściel, Paweł, and Beata Dobrowolska. 2020. "The Correlation between Social Support and Quality of Life of Seniors without Cognitive Disorders from an Institutional Environment—A Descriptive Cross-Sectional Survey" Healthcare 8, no. 3: 212. https://doi.org/10.3390/healthcare8030212
APA StyleChruściel, P., & Dobrowolska, B. (2020). The Correlation between Social Support and Quality of Life of Seniors without Cognitive Disorders from an Institutional Environment—A Descriptive Cross-Sectional Survey. Healthcare, 8(3), 212. https://doi.org/10.3390/healthcare8030212