Risk Prediction Model Development for Late On-Set Breast Cancer Screening in Low- and Middle-Income Societies: A Model Study for North Cyprus

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection:
2.3. Statistical Analysis
2.3.1. Internal Validation
2.3.2. External Validation
3. Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Global cancer statistics, 2002. CA Cancer J. Clin. 2005, 55, 74–108. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer. J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- de Sanjose, S.; Serrano, B.; Castellsague, X.; Brotons, M.; Munoz, J.; Bruni, L.; Bosch, F.X. Human papillomavirus (HPV) and related cancers in the Global Alliance for Vaccines and Immunization (GAVI) countries. A WHO/ICO HPV Information Centre Report. Vaccine 2012, 30, D1-83, vi. [Google Scholar]
- Commission on Social Determinants on Health. Closing the gap in generation: Health equity through action on social determinants of health. Public Health 2008, 372, 1661–1669. [Google Scholar]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Breast Cancer Facts & Figures 2019–2020. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-facts-and-figures/breast-cancer-facts-and-figures-2019-2020.pdf (accessed on 7 July 2020).
- Allemani, C.; Weir, H.K.; Carreira, H.; Harewood, R.; Spika, D.; Wang, X.S.; Bannon, F.; Ahn, J.V.; Johnson, C.J.; Bonaventure, A.; et al. Global surveillance of cancer survival 1995–2009: Analysis of individual data for 25,676,887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet 2015, 385, 977–1010. [Google Scholar] [CrossRef]
- Sankaranarayanan, R.; Swaminathan, R.; Brenner, H.; Chen, K.; Chia, K.S.; Chen, J.G.; Law, S.C.K.; Ahn, Y.-O.; Xiang, Y.B.; Yeole, B.B.; et al. Cancer survival in Africa, Asia, and Central America: A population-based study. Lancet Oncol. 2010, 11, 165–173. [Google Scholar] [CrossRef]
- Riboli, E.; Norat, T. Epidemiological evidence of the protective effect of fruit and vegetable on cancer risk. Am. J. Clin. Nutr. 2003, 78, 559–569. [Google Scholar] [CrossRef]
- Martinez-Gonzales, M.; Sanchez-Villegas, A. The emerging role of Mediterranean diets in cardiovascular epidemiology: Monosaturated fats, olive oil, red wine or the whole pattern? Eur. J. Epidemiol. 2004, 19, 9–13. [Google Scholar] [CrossRef]
- Hincal, E.; Taneri, U.; Djamgoz, M.B. Cancer incidence in North Cyprus (1994–2004) relative to European rates. Asian. Pac. J. Cancer Prev. 2008, 9, 725–732. [Google Scholar]
- Pervaiz, R.; Tulay, P.; Faisal, F.; Serakinci, N. Incidence of Cancer in the Turkish republic of northern Cyprus. Turk. J. Med. Sci. 2017, 47, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Cuzick, J. Breast cancer prevention in the developing world. Breast Cancer Res. 2010, 12, s9. [Google Scholar] [CrossRef] [PubMed]
- Colditz, G.A.; Bohlke, K. Priorities for the primary prevention of breast cancer. CA Cancer J. Clin. 2014, 64, 186–194. [Google Scholar] [CrossRef]
- Youlden, D.R.; Cramb, S.M.; Dunn, N.A.; Muller, J.M.; Pyke, C.M.; Baade, P.D. The descriptive epidemiology of female breast cancer: An international comparison of screening, incidence, survival and mortality. Cancer Epidemiol. 2012, 36, 237–248. [Google Scholar] [CrossRef]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Benbrahim-Tallaa, L.; Bouvard, V.; Bianchini, F.; Striaf, K. Breast-cancer screening—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2015, 372, 2353–2358. [Google Scholar] [CrossRef]
- Sankaranarayanan, R.; Ramadas, K.; Qiao, Y.L. Managing the changing burden of cancer in Asia. BMC Med. 2014, 12, 3. [Google Scholar] [CrossRef] [PubMed]
- Independent UK Panel on Breast Cancer Screening. The benefits and harms of breast cancer screening: An independent review. Lancet 1786. [Google Scholar]
- WHO. WHO Position Paper on Mammography Screening; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Niens, L.M.; Zelle, S.G.; Gutierrez-Delgado, C.; Pena, G.R.; Balarezo, B.R.H.; Stellar, E.R.; Rutten, F.F.H. Cost-effectiveness of breast cancer control strategies in Central America: The cases of Costa Rica and Mexico. PLoS ONE 2014, 9, e95836. [Google Scholar] [CrossRef]
- Okonkwo, Q.L.; Draisma, G.; der Kinderen, A.; Brown, M.L.; de Koning, H.J. Breast cancer screening policies in developing countries: A cost-effectiveness analysis for India. J. Natl. Cancer Inst. 2008, 100, 1290–1300. [Google Scholar] [CrossRef][Green Version]
- Zelle, S.G.; Nyarko, K.M.; Bosu, W.K.; Aikins, M.; Niens, L.M.; Lauer, J.A.; Sepulveda, C.R.; Hontelez, J.A.C.; Baltussen, R. Costs, effects and cost-effectiveness of breast cancer control in Ghana. Trop Med. Int. Health 2012, 17, 1031–1043. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.O.; Cazap, E.; El Saghir, N.S.; Yip, C.H.; Khaled, H.M.; Otero, I.V.; Adebamowo, C.A.; Badwe, R.A.; Harford, J.B. Optimisation of Breast Cancer Management in Low-Resource and Middle-Resource Countries: Executive Summary of the Breast Health Global Initiative Consensus, 2010. Lancet Oncol. 2011, 12, 387–398. [Google Scholar] [CrossRef]
- Unger-Saldana, K. Challenges to the early diagnosis and treatment of breast cancer in developing countries. World J. Clin. Oncol. 2014, 5, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Denny, L.; de Sanjose, S.; Mutebi, M.; Anderson, B.O.; Kim, J.; Jeronimo, J.; Herrero, R.; Yeates, K.; Ginsburg, O.; Sankaranarayanan, R. Interventions to close the divide for women with breast and cervical cancer between low-income and middle-income countries and high-income countries. Lancet 2017, 389, 861–870. [Google Scholar] [CrossRef]
- Kelsey, J.L.; Bernstein, L. Epidemiology and prevention of breast cancer. Annu. Rev. Public Health 1996, 17, 47–67. [Google Scholar] [CrossRef] [PubMed]
- Welsh, M.L.; Burst, D.S.; Bowles, A.E.J.; Anderson, M.L.; Elmore, J.G.; Li, C.I. Population-based estimates of the relation between breast cancer risk, tumour subtype and family history. Breast Cancer Res. Treat 2009, 114, 549–558. [Google Scholar] [CrossRef]
- Brandt, A.; Bermejo, J.; Sundquist, J.; Hemminki, K. Age of onset in familial breast cancer as background data for medical surveillance. Br. J. Cancer 2010, 102, 42–47. [Google Scholar] [CrossRef] [PubMed]
- McCormack, V.A.; Silva, d.S.I. Breast Density and parenchymal patterns as markers of breast cancer risk: A meta-analysis. Cancer Epidemiol. Biomarkers Prev. 2006, 15, 1159–1169. [Google Scholar] [CrossRef]
- Amir, E.; Freedman, O.C.; Seruga, B.; Evans, D.G. Assessing women at high risk of breast cancer: A review of risk assessment models. J. Natl. Cancer Inst. 2010, 102, 680–691. [Google Scholar] [CrossRef]
- Antoniou, A.C.; Hardy, R.; Walker, L.; Evans, D.G.; Shenton, A.; Pichert, G.; Izatt, L.; Rose, S.; Douglas, F.; Eccles, D.; et al. Predicting the likelihood of carrying a BRCA1 or BRCA2 mutation: Validation of BOADICEA, BRCAPRO, IBIS, Myriad and the Manchester scoring system using data from UK genetics clinics. J. Med. Genet. 2008, 45, 425–431. [Google Scholar] [CrossRef]
- Rockhill, B.; Spiegelman, D.; Byrne, C.; Hunter, D.J.; Colditz, G.A. Validation of the Gail et al. model of breast cancer risk prediction and implications for chemoprevention. J. Natl. Cancer Inst. 2001, 93, 358–366. [Google Scholar] [CrossRef]
- Antoniou, A.C.; Cunningham, A.P.; Peto, J.; Evans, D.G.; Lalloo, F.; Narod, S.A.; Risch, H.A.; Eyfjord, J.E.; Hopper, J.L.; Southey, M.C.; et al. The BOADICEA model of genetic susceptibility to breast and ovarian cancers: Updates and extensions. Br. J. Cancer 2008, 98, 1457–1466. [Google Scholar] [CrossRef] [PubMed]
- Humphrey, L.L.; Helfand, M.; Chan, B.K.; Woolf, S.H. Breast cancer screening: A summary of the evidence for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2002, 137, 347–360. [Google Scholar] [CrossRef] [PubMed]
- Costantino, J.P.; Gail, M.H.; Pee, D.; Anderson, S.; Redmond, C.K.; Benichou, J.; Wieand, H.S. Validation studies for models pro-jecting the risk of invasive and total breast cancer incidence. J. Natl. Cancer Inst. 1999, 91, 1541–1548. [Google Scholar] [CrossRef]
- Schonfeld, S.J.; Pee, D.; Greenlee, R.T.; Hartge, P.; Lacey Jr, J.V.; Park, Y.; Schatzin, A.; Visvanathan, K.; Pfieffer, R.M. Effect of changing breast cancer incidence rates on the calibration of the Gail model. J. Clin. Oncol. 2010, 28, 2411–2417. [Google Scholar] [CrossRef] [PubMed]
- Pickle, L.M.; Johnson, K.A. Estimating the long-term probability of developing breast cancer. J. Natl. Cancer Inst. 1989, 81, 1854–1855. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Harrell, F.E., Jr.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Schumacher, M.; Hollander, N.; Sauerbrei, W. Resampling and cross-validation techniques: A tool to reduce bias caused by model building? Stat. Med. 1997, 16, 2813–2827. [Google Scholar] [CrossRef]
- Terry, M.B.; Liao, Y.; Whittemore, A.S.; Leoce, N.; Buchsbaum, R.; Zeinomar, N.; Dite, G.S.; Chung, W.K.; Knight, J.A.; Southey, M.C.; et al. 10-year performance of four models of breast cancer risk: A validation study. Lancet Oncol. 2019, 20, 504–517. [Google Scholar] [CrossRef]
- Lichtenstein, P.; Holm, N.V.; Verkasalo, P.K.; Lliadou, A.; Kaprio, J.; Koskenvuo, M.; Pukkala, E.; Skytthe, A.; Hemminki, K. Environmental and Heritable Factors in the Causation of Cancer—Analyses of Cohorts of Twins from Sweden, Denmark, and Finland. N. Engl. J. Med. 2000, 343, 78–85. [Google Scholar] [CrossRef]
- Barnard, M.; Boeke, C.; Tamimi, R. Established breast cancer risk factors and risk of intrinsic tumor subtypes. Biochem. Biophys. Acta 2015, 1856, 73–85. [Google Scholar] [CrossRef]
- Collaborative Group on Hormonal Factors in Breast Cancer. Familial breast cancer: Collaborative reanalysis of individual data from 52 epidemiological studies including 58,209 women with breast cancer and 101,986 women without the disease. Lancet 2001, 358, 1389–1399. [Google Scholar] [CrossRef]
- Pharoah, P.D.; Day, N.E.; Duffy, S.; Easton, D.F.; Ponder, B.A. Family history and the risk of breast cancer: A systematic review and meta-analysis. Int. J. Cancer 1997, 71, 800–809. [Google Scholar] [CrossRef]
- Turnbull, C.; Rahman, N. Genetic Predisposition to Breast Cancer: Past, Present, and Future. Ann. Rev. Genomics Hum. Genet. 2008, 9, 321–345. [Google Scholar] [CrossRef]
- Kaminska, M.; Ciszewski, T.; Lopacka-Szatan, K.; Miotla, P.; Staroslawska, E. Breast cancer risk factors. Prz. Menopauzalny 2015, 14, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.S.; Zhao, Z.; Yang, Z.N. Risk factors and preventions of breast cancer. Int. J. Biol. Sci. 2017, 13, 1387–1397. [Google Scholar] [CrossRef] [PubMed]
- Singletary, S.E. Rating the risk factors for breast cancer. Ann. Surg. 2003, 237, 474–482. [Google Scholar] [CrossRef]
- Howell, A.; Anderson, A.S.; Clarke, R.B. Risk determination and prevention of breast cancer. Breast Cancer Res. 2014, 16, 446. [Google Scholar] [CrossRef]
- Anothaisintawee, T.; Wiratkapun, C.; Lerdsitthichai, P. Risk factors of breast cancer: A systematic review and meta-analysis. Asia Pac. J. Public Health 2013, 25, 368–387. [Google Scholar] [CrossRef] [PubMed]
- Ozsoy, A.; Barca, N.; Dolek, B.A. The relationship between breast cancer and risk factors: A single-center study. Eur. J. Breast Health 2017, 13, 145–149. [Google Scholar] [CrossRef]
- McTiernan, A. Behavioral risk factors in breast cancer: Can risk be modified? Oncologist 2003, 8, 326–334. [Google Scholar] [CrossRef]
- Patterson, R.E.; Cadmus, L.A.; Emond, J.A.; Pierce, J.P. Physical activity, diet, adiposity and female breast cancer prognosis: A review of the epidemiologic literature. Maturitas 2010, 66, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Demark-Wahnefried, W. Can lifestyle modification increase survival in women diagnosed with breast cancer? J. Nutr. 2002, 132, 3504S–3507S. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.R.; Sherman, M.E.; Rimm, D.L. Differences in risk factors for breast cancer molecular subtypes in a population-based study. Cancer Epidemiol. Biomark Prev. 2007, 16, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Anderson, W.F.; Rosenberg, P.S.; Prat, A.; Perou, C.M.; Sherman, M.E. How many etiological subtypes of breast cancer: Two, three, four, or more? J. Natl. Cancer Inst. 2014, 106, dju165. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.; Ma, J.; Zou, Z.; Jemal, A. Cancer statistics. CA Cancer. J. Clin. 2014, 64, 9–29. [Google Scholar] [CrossRef]
- Nystrom, L.; Andersson, I.; Bjurstam, N.; Frisell, J.; Nordenskjold, B.; Rutqvist, L.E. Long-term effects of mammography screening: Updated overview of the Swedish randomised trials. Lancet 2002, 359, 909–919. [Google Scholar] [CrossRef]
- Leach, M.O.; Boggis, C.R.; Dixon, A.K.; Easton, D.F.; Eeles, R.A.; Evans, D.G.; Gilbert, F.J.; Griebsch, I.; Hoff, R.J.; Kessar, P.; et al. Screening with magnetic resonance imaging and mammography of a UK population at high familial risk of breast cancer: A prospective multicentre cohort study (MARIBS). Lancet 2005, 365, 1769–1778. [Google Scholar]
- Kriege, M.; Brekelmans, C.T.; Boetes, C.; Besnard, P.E.; Zonderland, H.M.; Obdeijn, I.M.; Manoliu, R.A.; Kok, T.; Peterse, H.; Madeleine, M.A.; et al. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N. Engl. J. Med. 2004, 351, 427–437. [Google Scholar] [CrossRef]
- Le-Petross, H.T.; Whitman, G.J.; Atchley, D.P.; Yuan, Y.; Gutierrez-Barrera, A.; Hortobagyi, G.N.; Litton, J.K.; Arun, B.K. Effectiveness of alternating mammography and magnetic resonance imaging for screening women with deleterious BRCA mutations at high risk of breast cancer. Cancer 2011, 117, 3900–3907. [Google Scholar] [CrossRef]
- Saslow, D.; Boetes, C.; Burke, W.; Harms, S.; Leach, M.O.; Lehman, C.D.; Morris, E.; Pisano, E.; Schnall, M.; Sener, S.; et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J. Clin. 2007, 57, 75–89. [Google Scholar] [CrossRef]
- A Guide for Countries Joining the m-Health Program. Available online: https://www.who.int/nmh/events/2012/mhealth_guide.pdf (accessed on 7 July 2020).
- Reiser, B. Measuring the effectiveness of diagnostic markers in the presence of measurement error through the use of ROC curves. Stat. Med. 2000, 19, 2115–2129. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Frequencies (%) |
|---|---|
| Reproductive History | |
| Age at menarche | |
| ≥14 years | 155 (23.7%) |
| 14–13 years | 421 (64.3%) |
| >12–<13 years | 0 (0%) |
| <12 years | 79 (12.1%) |
| Age at first birth | |
| ≥30 years | 58 (8.9%) |
| 25–29 years | 142 (21.7%) |
| 20–24 years | 238 (36.3%) |
| <20 years | 167 (25.5%) |
| Nulliparous | 50 (7.8%) |
| Menopausal status | |
| Premenopausal | 314 (47.9%) |
| Perimenopausal | 13 (2.0%) |
| Postmenopausal | 328 (50.1%) |
| Breastfeeding | |
| ≥24 months | 285 (43.5%) |
| <24–>18 months | 0 (0%) |
| 18–12 months | 236 (36.0%) |
| <12–>6 months | 0 (0%) |
| <6 months | 83 (12.7%) |
| Never | 51 (7.8%) |
| Breast density | |
| Extremely dense | 58 (8.9%) |
| Heterogeneously dense | 334 (51.0%) |
| Almost entirely fatty | 263 (40.2%) |
| Demographic Data | |
| >1 First degree relatives | |
| Yes | 65 (9.9%) |
| No | 590 (90.1%) |
| Second degree relatives | |
| Yes | 41 (6.3%) |
| No | 614 (93.7%) |
| Hormone Replacement Therapy | |
| Yes | 17 (2.6%) |
| No | 638 (97.4%) |
| Breast biopsy | |
| Yes | 85 (13.0%) |
| No | 570 (87.0%) |
| Age | |
| >50 | 320 (48.9%) |
| ≤50 | 335 (51.1%) |
| Disease status | |
| Breast cancer cases | 318 (48.5%) |
| Without breast cancer | 337 (51.5%) |
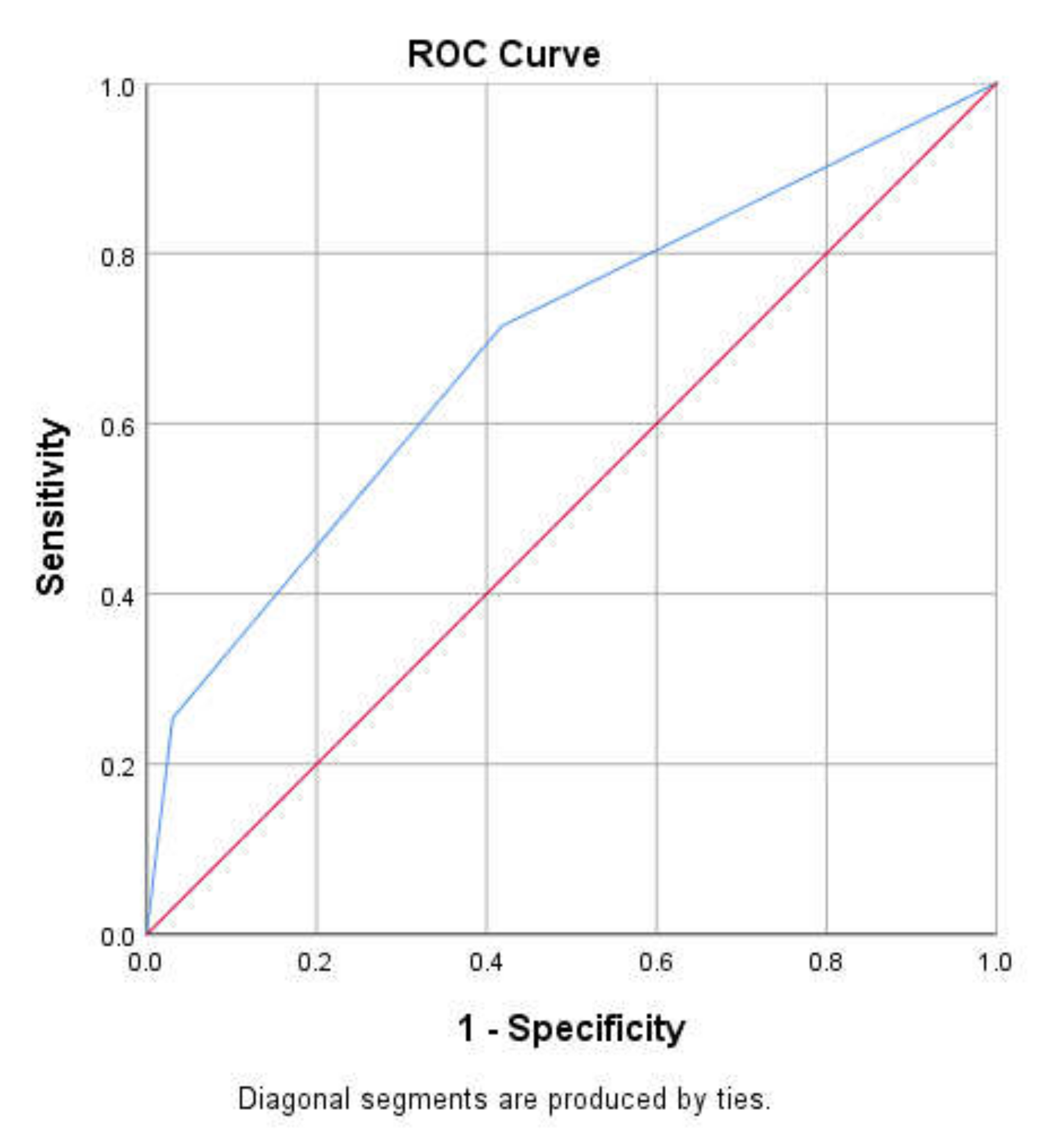
| Cut-Off Value | Sensitivity | Specificity |
|---|---|---|
| 0.5–1.0 | 71.4% | 41.7% |
| Risk Status | Suggestions/Advice | Outcome |
|---|---|---|
| High-risk (>1 FDR and ≥50 years) | Regular monitoring, early detection and preventive interventions | Reduced mortality |
| Moderate-risk (>1 FDR or ≥50 years) | Further screening to access risk | Prevention of occurrence |
| Low-risk (No FDR, <50 years) | Primary care | Awareness and prevention |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Danladi, C.D.; Serakinci, N. Risk Prediction Model Development for Late On-Set Breast Cancer Screening in Low- and Middle-Income Societies: A Model Study for North Cyprus. Healthcare 2020, 8, 213. https://doi.org/10.3390/healthcare8030213
Danladi CD, Serakinci N. Risk Prediction Model Development for Late On-Set Breast Cancer Screening in Low- and Middle-Income Societies: A Model Study for North Cyprus. Healthcare. 2020; 8(3):213. https://doi.org/10.3390/healthcare8030213
Chicago/Turabian StyleDanladi, Ceasar Dubor, and Nedime Serakinci. 2020. "Risk Prediction Model Development for Late On-Set Breast Cancer Screening in Low- and Middle-Income Societies: A Model Study for North Cyprus" Healthcare 8, no. 3: 213. https://doi.org/10.3390/healthcare8030213
APA StyleDanladi, C. D., & Serakinci, N. (2020). Risk Prediction Model Development for Late On-Set Breast Cancer Screening in Low- and Middle-Income Societies: A Model Study for North Cyprus. Healthcare, 8(3), 213. https://doi.org/10.3390/healthcare8030213