
Older Adults’ and Professionals’ Attitudes Towards Stair-Fall Prevention Interventions

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Survey
2.2. Focus Groups
3. Results
3.1. Survey Results
3.2. Focus Group Results
3.2.1. Focus Group Participants
3.2.2. Attitudes Towards Stair-Fall Prevention Interventions
- 1.
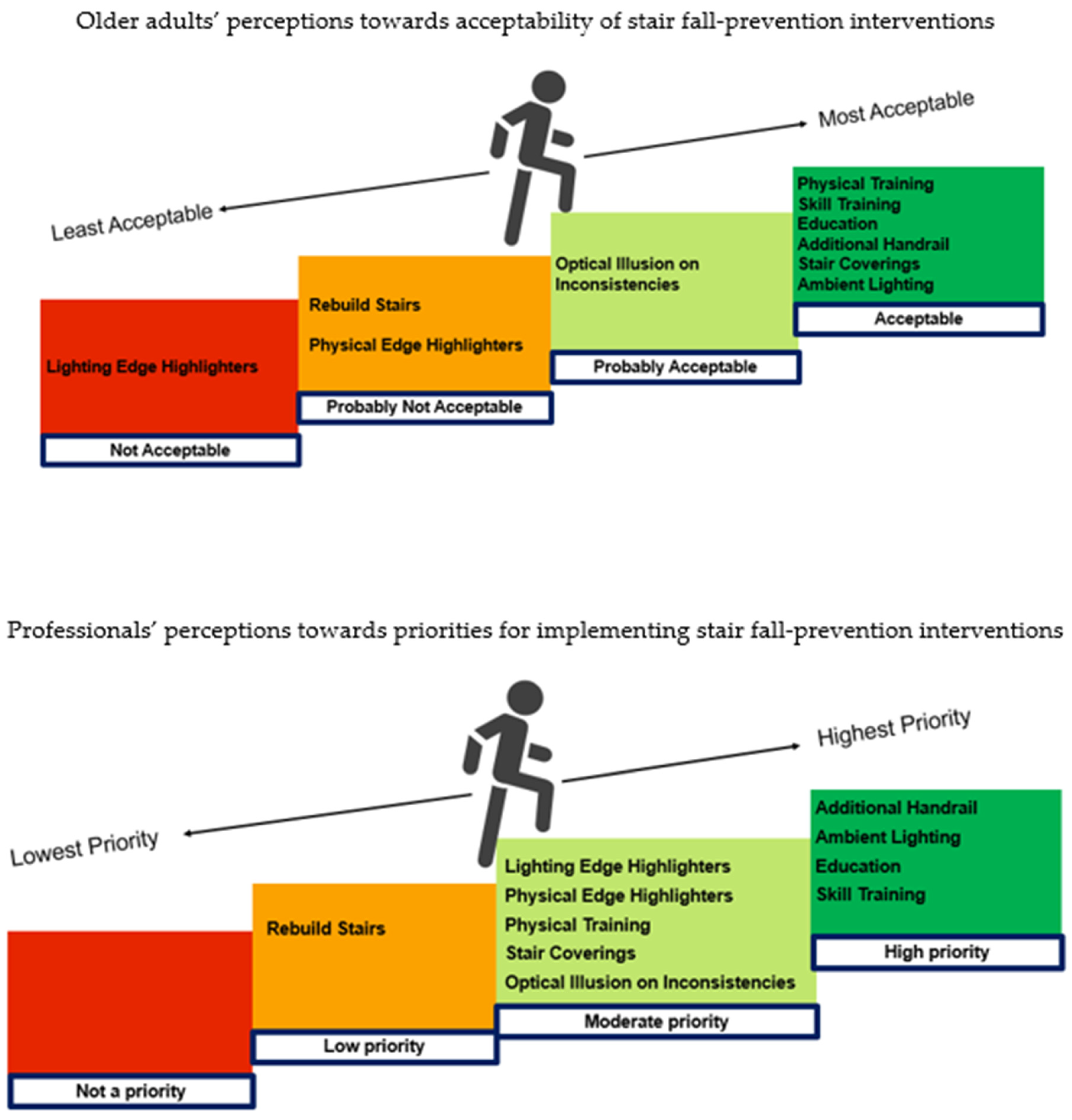
- Rebuilding stairs: All older adult participants identified practical concerns as a barrier to rebuilding stairs; P8 stated, “Apart from the cost for many older people, the sheer upheaval and working out how you find the responsible tradesmen to do the job properly are problems”; including space constraints; P2 stated, “In terraced houses the space is very confined, so you’re not going to be able to make a longer or wider staircase”. For older adults living with others or renting, having independent decision-making power or control to make significant adaptions at home was identified as a barrier. Overall, there was low acceptability of rebuilding stairs as an intervention with consensus from older adults that “the negatives would outweigh the positives” (P3), unless it was essential. Participants suggested that safe stair dimensions should be a key consideration in new build construction and consideration by older adults if moving home.
- 2.
- Additional handrail: Older adults agreed that a handrail is pivotal for stair safety, providing a sense of security and stability. “I wouldn’t go up the stairs unless I was holding onto the banister, I would never go up without holding on to something” (P4). Handrails were seen as a way of assisting with balance problems that progressively worsen with ageing and providing confidence when using stairs. Only one of the participants already had two handrails on their home staircase, but most participants acknowledged that they would feel safer using stairs if they had an extra handrail (or two). However, space constraints were raised as a key barrier to adoption: “The stairs are narrow anyway and to think of an extra handrail being put in, it would really narrow the staircase and that would feel more unsafe than it not being there” (P6). Conversely, one participant stressed that, if a staircase is wide, holding onto handrails on both sides may not be possible. Participants also expressed differing preferences for handrail shape, with some preferring traditional contoured handrails for aesthetic reasons and others desiring a shape that provides additional grip. The lack of independent decision-making power was raised as a barrier. P6 highlighted: “A lot of this is assuming […..] you have complete control over those decisions. Whereas you might live in a multi-generational household with different needs”. Older adults held concerns about stigmatisation: “that means I’m admitting I’m getting older, I’m getting more vulnerable. If new houses were built with two rails and it gradually became standard, it would help to overcome the perception that two rails means old and disabled. So I think I would start with trying to make it fashionable” (P8). Overall group consensus indicated that an additional handrail is an acceptable intervention to older adults.
- 3.
- Ambient Lighting: All older adult participants agreed that adequate levels of light on stairs were important for safety. They felt this was particularly required to illuminate obstacles, especially for those with pets. A key barrier to modifying existing lighting was not understanding what type of lighting would be optimal. P8 stated, “If you are in a lighting shop you can see millions of different light fittings, but knowing what would be really good to get from the stair safety point of view is another matter”. A further barrier identified was that older adults may require assistance to move light fittings, which would add to the cost of making the change. The need for guidance on the most appropriate type and positioning of lighting, as well as where to access such guidance, were identified as facilitators to the adoption of this intervention. Group consensus was that ambient lighting is an acceptable intervention for older adults.
- 4.
- Changing stair coverings: Older adults were not aware that patterned stair coverings were a fall risk before the research team presented details of the intervention to them. P7 stated, “I think changing the stair covering is probably only going to be something that you would do if you have had a fall, because you wouldn’t actually think about it prior to that”. In addition to a lack of awareness, barriers to adoption raised by older adults included the economic cost and disruption of fitting new stair coverings. Once older adults were aware of the risk and the intervention, they suggested that everyone should be encouraged to consider the risk posed by stair décor upon the selection and purchase of a new stair covering or carpet. Education and awareness raising were highlighted as facilitators to adoption, which could be supported by carpet manufacturers and suppliers. Group consensus suggests that changing stair coverings to plain décor would be an acceptable intervention to older adults.
- 5.
- Optical illusions on inconsistent steps: Older adult participants were unaware that inconsistencies in step dimensions may exist in home staircases and can present a significant fall risk. Barriers to adoption expressed by older adults related to doubts about efficacy (not understanding how it works), concern about impact on individuals with vision problems (if it would increase trip risk), and practical concerns about the ability to apply an optical illusion on carpeted stairs. However, participants expressed willingness to consider the intervention even if it results in aesthetic variance to the staircase. Suggested facilitators to adoption included the ability to adapt the intervention to be used on carpet stairs in keeping with personal home décor preferences and seeing a practical demonstration of the illusion in a real-life environment to help end-users better understand its efficacy. Group consensus suggests that an optical illusion would probably be an acceptable intervention for older adults.
- 6.
- Physical edge highlighters: Older adults showed a lack of understanding of the intervention and expressed concern about efficacy, aesthetic preferences, and applicability on carpeted stairs. Some participants were concerned that the intervention would cause distraction: “I don’t know whether that would make me clumsier somehow because of looking at the highlighters. I’d be thinking ‘am I getting them right’, as opposed to forgetting about it and just automatically walking upstairs” (P7). Ensuring edge highlighters are designed to be flush to the step surface was suggested as a facilitator to adoption. A dislike of the aesthetic appearance was identified as a barrier and played a significant role in determining acceptability to older adults. Some participants indicated that they would consider edge highlighters if they could be seamlessly integrated within a carpeted surface or if the design could be ‘modernised’ to be in keeping with home decor. However, not all participants agreed: “Whatever surface it’s on, I don’t think it would work for me” (P3), “I just don’t think it would be accepted by many people” (P4). Group consensus suggested that physical edge highlighters would probably not be acceptable as an intervention in older adults’ homes.
- 7.
- Lighting edge highlighters: Older adults were sceptical regarding the efficacy of lighting edge highlighters on home stairs, underpinned by confusion as to how they differed from ambient lighting. On being presented with an image of the intervention by the researchers, participants expressed dissatisfaction: “That’s thrown me somehow. I don’t know, I don’t like the visual look” (P7). Older adults were concerned that lighting edge highlighters could cause visual distractions and diversion of attention: “When you first described it, I thought that would be a really good idea. But seeing it like that image, no, you’ll be looking down at it” (P3). Some participants could see the benefits of lighting to highlight step edges, but individual preferences for the positioning and brightness of lighting varied. A practical demonstration of the intervention in a home setting to increase understanding was identified as a facilitator to adoption. Participants concluded that lighting edge highlighters were not acceptable as a stair safety intervention that older adults would adopt in their homes and preferred to improve ambient lighting.
- 8.
- Physical Training: Older adult participants agreed that physical training could be beneficial to prevent stair falls, particularly to address balance problems. Older adults identified the need for personalised exercise prescription depending on health status, recognising that some older adults may be limited in their ability to engage in exercise, while others may consider it unnecessary or already engage in regular physical activity (e.g., walking, cycling, and gardening). P5 stressed, “For me that’s totally boring. I would never do it because I do other things, I keep fit and I eat healthily”. Participants highlighted facilities and supervision as facilitators: P8 stated: “who’s going to be supervising it and how you access it. For example, is it a good instructor who will tell you what you’re doing wrong, or one that just does an exercise and lets you follow them? I prefer having somebody who will actually give you some guidance”. Preferences for the mode of delivery (e.g., group-based in person or individual home-based) differed between genders. Female participants preferred the in-person group activity, offering social interaction and motivation to engage, while male participants preferred individual home-based exercise programmes, because they perceived that “Men are not group people. Even in gyms or classes, 99% are women. Fellas tend to stay on their own. I don’t know why” (P2). Group consensus suggests that physical training would be an acceptable intervention for older adults.
- 9.
- Education: Older adult participants were in agreement with P7: “I think it’s [education about stair safety] good for everybody because otherwise, until it happens, you don’t really think about it”. Older adults suggested that educational programmes should be proactive in highlighting potential stair safety issues before serious falls occur. As a facilitator to adoption, there was consensus that educational interventions would be more acceptable to older adults if signposted or delivered by professionals in the health sector. The main barrier to adoption was related to differing preferences for the mode of delivery. Female participants indicated a preference for group activities, with one stating the following: “One of the problems with things like leaflets or emails is that it doesn’t promote a conversation…[but] somebody coming and giving you a talk is it actually promotes a conversation. Using community groups you can start conversations” (P8). In contrast, male participants were less inclined to join group-based interventions and preferred accessing information individually and/or remotely (e.g., online resources, phone app). Having a range of delivery options was expressed as a facilitator to adoption. Group consensus suggests that education is an acceptable intervention for older adults and that education on stair falls should be expanded to the general public to raise wider awareness and promote social encouragement for older adults.
- 10.
- Skill Training: Older adult participants generally agreed that skill training on the safe use of home stairs would be helpful because “I had a fall on stairs […..] but I know I could have done something to avoid it” (P6). Gaining access to skill training and motivating older adults, particularly non-fallers, were barriers to adoption. “People who have had falls will be more motivated probably. But practically I don’t know how you’d get it across to the general public” (P8). Participants suggested that skill training could be delivered in a class-like setting, such as at a fitness centre or a community centre. Consensus was that skill training is considered an acceptable intervention for older adults.
3.2.3. Summary of Focus Group Results
4. Discussion
4.1. Barriers
4.2. Facilitators
4.3. Intervention Acceptability and Priority
4.4. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Copy of Older Adult Survey Questions
- 1.
- What is your age?
- 2.
- What is your gender?
- 3.
- What is your ethnic group?
- 4.
- How is your overall health in general?
- 5.
- Do you have any conditions or illnesses that affect you in any of the following areas? Select any that apply
- 6.
- How would you describe your activity status?
- 7.
- What type of property do you live in?
- 8.
- Do you own or rent your current home?
- 9.
- Are you currently living alone?
- 10.
- Please indicate the extent that you agree or disagree with the statements in the table below:
| Strongly disagree | Disagree | Agree | Strongly agree | Undecided | |
| ‘Falling on stairs is a concern for older adults’ | ◻ | ◻ | ◻ | ◻ | ◻ |
| ‘Stair falls are common for older adults’ | ◻ | ◻ | ◻ | ◻ | ◻ |
| ‘Stair falls in older adults are preventable’ | ◻ | ◻ | ◻ | ◻ | ◻ |
- 11.
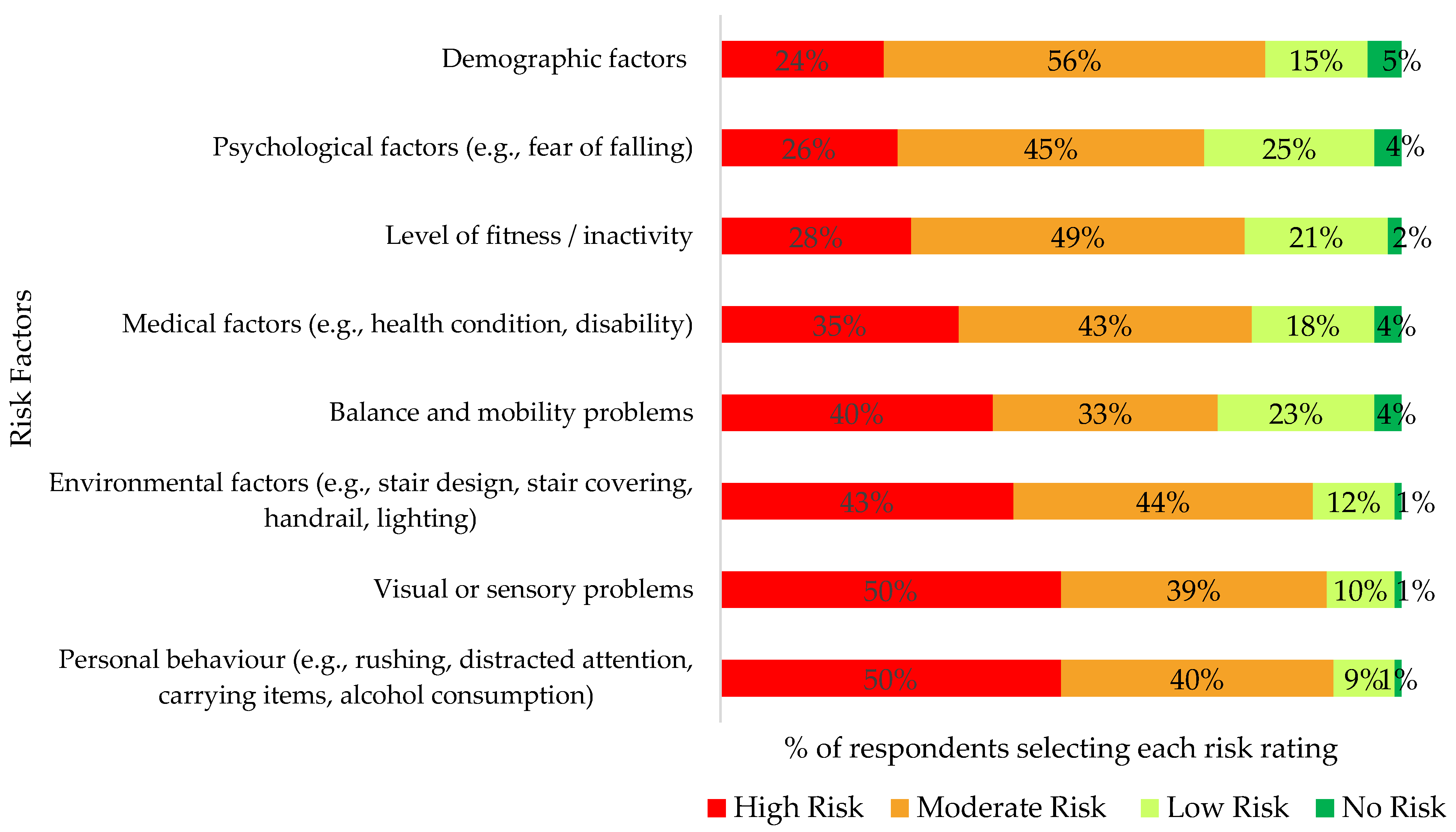
- Rate the extent that you think each of the factors in the table below are a risk factor for stair falls:
| No risk | Low risk | Moderate risk | High risk | |
| Medical factors (e.g., healthcondition, disability, impact of medication) | ◻ | ◻ | ◻ | ◻ |
| Balance and mobility problems | ◻ | ◻ | ◻ | ◻ |
| Visual or sensory problems | ◻ | ◻ | ◻ | ◻ |
| Level of fitness/inactivity | ◻ | ◻ | ◻ | ◻ |
| Psychological factors (e.g., anxiety, fear of falling) | ◻ | ◻ | ◻ | ◻ |
| Environmental factors (e.g., stair design, stair covering, presence of handrail, lighting, obstacles) | ◻ | ◻ | ◻ | ◻ |
| Personal behaviour (e.g., rushed movement, distracted attention, carrying items, alcohol consumption) | ◻ | ◻ | ◻ | ◻ |
| Demographic factors (e.g., living alone) | ◻ | ◻ | ◻ | ◻ |
- 12.
- Please indicate the extent that you agree or disagree with the statements in following questions:
| Strongly disagree | Disagree | Agree | Strongly agree | Undecided | |
| ‘I consider myself at risk of falling on stairs at home’ | ◻ | ◻ | ◻ | ◻ | ◻ |
| ‘I am fit and healthy so I don’t see myself at risk falling on stairs’ | ◻ | ◻ | ◻ | ◻ | ◻ |
- 13.
- Have you ever had a fall on stairs in your home?
- 14.
- Do you consider your stairs at home to be safe (not presenting a fall risk)?
- 15.
- Please indicate the extent that you agree or disagree with the statements in the table below:
| Strongly disagree | Disagree | Agree | Strongly Agree | Undecided | |
| ‘I consider stair fall prevention at home a priority’ | ◻ | ◻ | ◻ | ◻ | ◻ |
| ‘I am aware of what changes can be made at home to reduce the risk of stair falls’ | ◻ | ◻ | ◻ | ◻ | ◻ |
- 16.
- Would you be interested in making changes to your home environment to reduce risk of stair falls?
- 17.
- Would you be interested in engaging in behavioural changes to reduce risk of stair falls?
- 18.
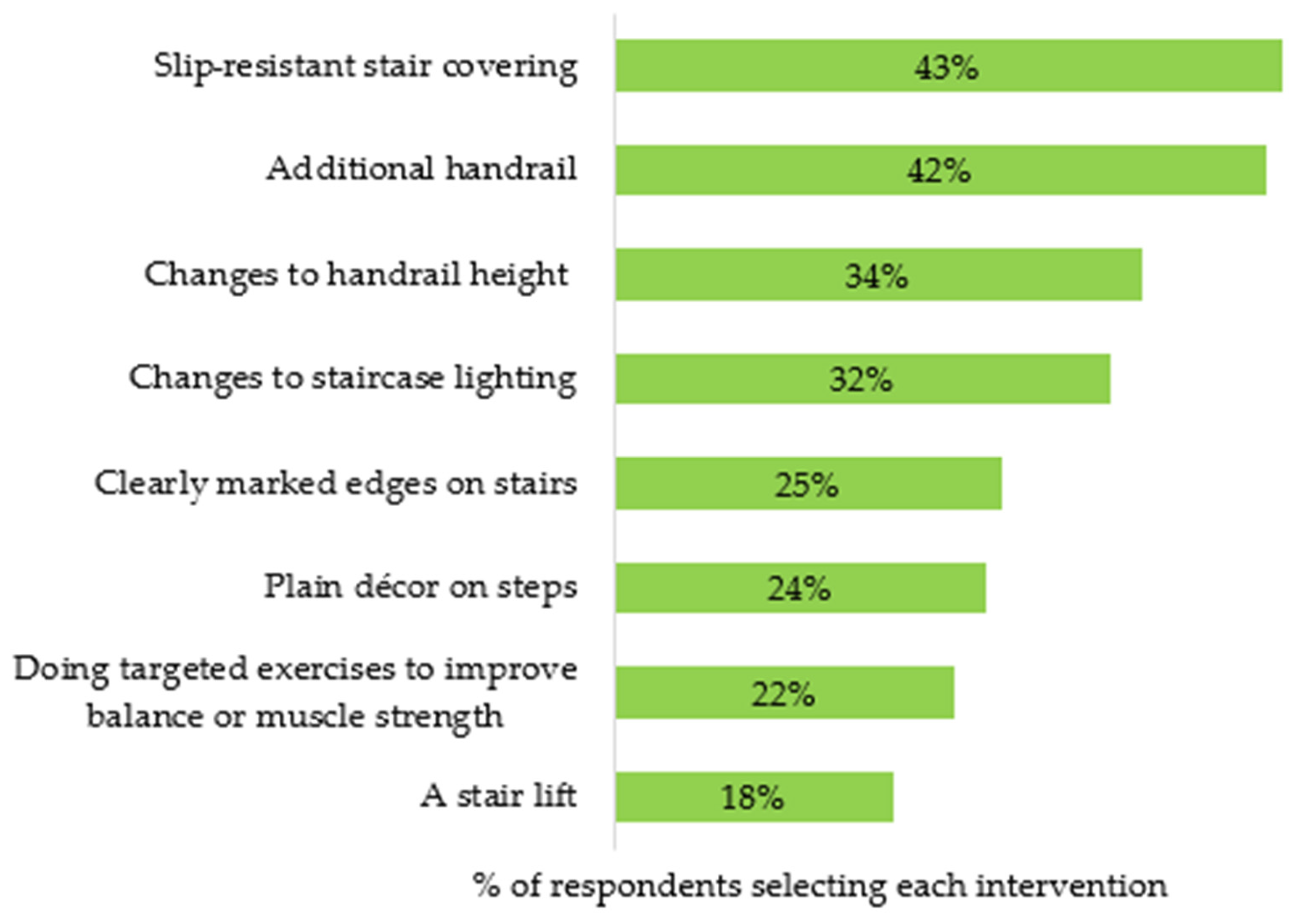
- Which of the following do you think would be good adaptions or interventions to improve hoe stair safety? Select any that apply
- 19.
- Is there anything that would encourage you to adopt interventions or adaptions that reduce risk of stair falls in your home? Select any that apply
- 20.
- Is there anything that stops or is delaying you from adopting interventions or adaptions that reduce risk of stair falls in your home? Select any that apply
Appendix B

{kind=link}
{kind=link}
{kind=link}
| Intervention | Category | Description of Intervention |
|---|---|---|
| Rebuilding stairs | Environment Intervention | Replacing existing staircase to meet UK building regulations specified in approved Document K (e.g., step rise, going and pitch). |
| Ambient lighting | Environment Intervention | Increasing illumination on stairs by adding more sources of ambient light, moving light fittings, and/or modifying sources of lightning. Intended to reduce fall risk by allowing a safer placement of feet on step tread (e.g., smaller foot overhang) and adequate foot clearance over step edge during stair ascent and descent. |
| Changing stair coverings (to plain décor) | Environment Intervention | Removing patterned carpets and coverings and replacing with plain, single colour step-surface decor to improve delineating step edges. Intended to reduce fall risk by allowing safer placement of feet on step tread mainly during stair descent. |
| Optical illusion on inconsistencies | Environment Intervention | Superimposing a horizontal–vertical illusion design on the riser of an inconsistently taller step within the staircase. Intended to improve foot clearance over the edge of an inconsistent step during stair ascent. |
| Edge highlighters (physical) | Environment Intervention | Superimposing along the edge of steps, physical strips, and nosings of adequate colour contrast and slip resistance. Intended to (1) improve the placement of feet with the available step tread during stair descent and (2) minimise the risk for a slip if there is a large foot overhang during stair descent. |
| Edge highlighters (lighting) | Environment Intervention | Adding appropriate lightning sources at specific places around the staircase to highlight the edge of the steps. Intended to reduce fall risk by allowing safer placement of feet on the step tread and adequate foot clearance over the step edge. |
| Additional handrail | Environment Intervention | Adding a second handrail of standards and characteristics specified in UK building regulations Document K. Intended to allow the safer placement of feet on step tread by improving balance control during stair descent. |
| Physical Training | Functional Capability Intervention | Improvement of relevant functional capabilities which deteriorate with old age, e.g., muscle strength and balance, through systematic engagement in appropriate exercise training. Intended to reduce fall risk by allowing a better controlled placement of feet on the step tread during stair ascent and descent and more successful recovery following a postural instability (e.g., grabbing onto handrails quickly and effectively following a collision with a step edge during stair ascent). |
| Education | Behavioural Intervention | Increasing awareness around factors influencing stair-fall risk and individual and socio-economic consequences of stair falls. Intended to improve safety by providing knowledge to enable end-users to implement effective and pragmatic measures to improve stair safety. |
| Skill Training | Behavioural Intervention | Improving stepping technique through training from relevant health practitioners (e.g., occupational therapists). Intended to reduce fall risk by teaching users how to move their feet on steps, taking into account individual functional limitations and actual home stairs and environmental design. Intended to improve safety by teaching tailor-made routines and practices on stairs, accounting for end-user circumstances. |
References
- Montero-Odasso, M.; van der Velde, N.; Martin, F.C.; Petrovic, M.; Tan, M.P.; Ryg, J.; Aguilar-Navarro, S.; Alexander, N.B.; Becker, C.; Blain, H.; et al. Task Force on Global Guidelines for Falls in Older Adults. World guidelines for falls prevention and management for older adults: A global initiative. Age Ageing 2022, 51, afac205. [Google Scholar] [CrossRef]
- WHO (World Health Organization). Falls. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/falls (accessed on 2 June 2023).
- Child, S.; Goodwin, V.; Garside, R.; Jones-Hughes, T.; Boddy, K.; Stein, K. Factors influencing the implementation of fall-prevention programmes: A systematic review and synthesis of qualitative studies. Implement. Sci. 2012, 14, 91. [Google Scholar] [CrossRef] [PubMed]
- OHID (Office for Health Improvement and Disparities). Falls: Applying All Our Health. 2022. Available online: https://www.gov.uk/government/publications/falls-applying-all-our-health/falls-applying-all-our-health (accessed on 10 May 2023).
- Age UK. Falls in Later Life: A Huge Concern for Older People. 2019. Available online: https://www.ageuk.org.uk/latest-press/articles/2019/may/falls-in-later-life-a-huge-concern-for-older-people/ (accessed on 18 August 2022).
- NICE (National Institute for Health and Care Excellence). Falls in Older People: Assessing Risk and Prevention (CG161); ISBN 978-1-4731-0132-6. 2013. Available online: https://www.nice.org.uk/guidance/cg161 (accessed on 12 November 2022).
- Smith, M.L.; Ory, M.G. Multi-directional nature of falls among older adults: A rationale for prevention and management. Front. Public Health 2023, 11, 1117863. [Google Scholar] [CrossRef] [PubMed]
- Stevens, J.A.; Sleet, D.A.; Rubenstein, L.Z. The Influence of Older Adults’ Beliefs and Attitudes on Adopting Fall Prevention Behaviors. Am. J. Lifestyle Med. 2017, 12, 324–330. [Google Scholar] [CrossRef]
- WHO (World Health Organization). WHO Global Report on Falls Prevention in Older Age. 2007. Available online: https://www.who.int/publications/i/item/9789241563536 (accessed on 2 June 2023).
- Local Government Association. Meeting the Home Adaptation Needs of Older People; Local Government Association: London, UK, 2020. [Google Scholar]
- Mulliner, E.; Riley, M.; Maliene, V. Older People’s Preferences for Housing and Environment Characteristics. Sustainability 2020, 12, 5723. [Google Scholar] [CrossRef]
- Jacobs, J.V. A review of stairway falls and stair negotiation: Lessons learned and future needs to reduce injury. Gait Posture 2016, 49, 159–167. [Google Scholar] [CrossRef]
- Oh-Park, M.; Wang, C.; Verghese, J. Stair negotiation time in community-dwelling older adults: Normative values and association with functional decline. Arch. Phys. Med. Rehabil. 2011, 92, 2006–2011. [Google Scholar] [CrossRef]
- Tural, E.; Lu, D.; Cole, D.A. Factors predicting older Adults’ attitudes toward and intentions to use stair mobility assistive designs at home Author links open overlay panel. Prev. Med. Rep. 2020, 18, 101082. [Google Scholar] [CrossRef]
- Startzell, J.K.; Owens, D.A.; Mulfinger, L.M.; Cavanagh, P.R. Stair negotiation in older people: A review. J. Am. Geriatr. Soc. 2000, 48, 567–580. [Google Scholar] [CrossRef]
- RoSPA (Royal Society for the Prevention of Accidents). Home Safety Position Statements. 2018. Available online: https://www.ageuk.org.uk/bp-assets/globalassets/lambeth/aukl-news-section-pictures/royal-society-for-the-prevention-of-accidents---home-safety-position-statements.pdf (accessed on 30 May 2025).
- HM Government. Approved Document K: Protection from Falling, Collision and Impact; Ministry of Housing, Communities and Local Government: London, UK, 2013. [Google Scholar]
- Home Builders Federation. Housing Horizons: Examining UK Housing Stock in an International Context. 2023. Available online: https://www.hbf.co.uk/news/housing-horizons/ (accessed on 28 April 2025).
- Di Giulio, I.; Reeves, N.D.; Roys, M.; Buckley, J.G.; Jones, D.A.; Gavin, J.P.; Baltzopoulos, V.; Maganaris, C.N. Stair Gait in Older Adults Worsens with Smaller Step Treads and When Transitioning Between Level and Stair Walking. Front. Sports Act. Living 2020, 2, 63. [Google Scholar] [CrossRef]
- Francksen, N.C.; Ackermans, T.M.A.; Holzer, D.; Ebner, S.A.; Maganaris, C.N.; Hollands, M.A.; Karamanidis, K.; Roys, M.; O’Brien, T.D. Negotiating stairs with an inconsistent riser: Implications for stepping safety. Appl. Ergon. 2020, 87, 103131. [Google Scholar] [CrossRef] [PubMed]
- Thomas, N.M.; Skervin, T.; Foster, R.J.; O’Brien, T.D.; Carpenter, M.G.; Maganaris, C.N.; Baltzopoulos, V.; Lees, C.; Hollands, M.A. Optimal lighting levels for stair safety: Influence of lightbulb type and brightness on confidence, dynamic balance and stepping characteristics. Exp. Gerontol. 2020, 132, 110839. [Google Scholar] [CrossRef] [PubMed]
- Thomas, N.M.; Skervin, T.; Foster, R.J.; Parr, J.V.; Carpenter, M.G.; O’Brien, T.D.; Maganaris, C.N.; Baltzopoulos, V.; Lees, C.; Hollands, M.A. Influence of step-surface visual properties on confidence, anxiety, dynamic stability, and gaze behaviour in young and older adults. Hum. Mov. Sci. 2021, 77, 102774. [Google Scholar] [CrossRef] [PubMed]
- Gavin, J.P.; Reeves, N.D.; Jones, D.A.; Roys, M.; Buckley, J.G.; Baltzopoulos, V.; Maganaris, C.N. Combined Resistance and Stretching Exercise Training Benefits Stair Descent Biomechanics in Older Adults. Front. Physiol. 2019, 10, 873. [Google Scholar] [CrossRef]
- Reeves, N.D.; Spanjaard, M.; Mohagheghi, A.A.; Baltzopoulos, V.; Maganaris, C.N. Influence of light handrail use on the biomechanics of stair negotiation in old age. Gait Posture 2008, 28, 327–336. [Google Scholar] [CrossRef]
- King, S.L.; Underdown, T.; Reeves, N.D.; Baltzopoulos, V.; Maganaris, C.N. Alternate stair descent strategies for reducing joint moment demands in older individuals. J. Biomech. 2018, 78, 126–133. [Google Scholar] [CrossRef]
- Zietz, D.; Hollands, M. Gaze behavior of young and older adults during stair walking. J. Mot. Behav. 2009, 41, 357–365. [Google Scholar] [CrossRef]
- Clemson, L.; Mackenzie, L.; Roberts, C.; Poulos, R.; Tan, A.; Lovarini, M.; Sherrington, C.; Simpson, J.M.; Willis, K.; Lam, M.; et al. Integrated solutions for sustainable fall prevention in primary care, the iSOLVE project: A type 2 hybrid effectiveness-implementation design. Implement. Sci. 2017, 12, 12. [Google Scholar] [CrossRef]
- Vincenzo, J.L.; Patton, S.K.; Lefler, L.L.; McElfish, P.A.; Wei, J.; Curran, G.M. A qualitative study of older adults’ facilitators, barriers, and cues to action to engage in falls prevention using health belief model constructs. Arch. Gerontol. Geriatr. 2022, 99, 104610. [Google Scholar] [CrossRef]
- Day, L.; Donaldson, A.; Thompson, C.; Thomas, M. Integrating proven falls prevention interventions into government programs. Aust. N. Z. J. Public Health 2014, 38, 122–127. [Google Scholar] [CrossRef]
- van Rhyn, B.; Barwick, A. Health Practitioners’ Perceptions of Falls and Fall Prevention in Older People: A Metasynthesis. Qual. Health Res. 2019, 29, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Bunn, F.; Dickinson, A.; Barnett-page, E.; Mcinnes, E.; Horton, K. A systematic review of older people’s perceptions of facilitators and barriers to participation in falls-prevention interventions. Ageing Soc. 2008, 28, 449–472. [Google Scholar] [CrossRef]
- McMahon, S.; Talley, K.M.; Wyman, J.F. Older people’s perspectives on fall risk and fall prevention programs: A literature review. Int. J. Older People Nurs. 2011, 6, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Prochorskaite, A.; Couch, C.; Malys, N.; Maliene, V. Housing Stakeholder Preferences for the “Soft” Features of Sustainable and Healthy Housing Design in the UK. Int. J. Environ. Res. Public Health 2016, 13, 111. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, A.; Horton, K.; Machen, I.; Bunn, F.; Cove, J.; Jain, D.; Maddex, T. The role of health professionals in promoting the uptake of fall prevention interventions: A qualitative study of older people’s views. Age Ageing 2011, 40, 724–730. [Google Scholar] [CrossRef]
- Francis-Coad, J.; Watts, T.; Etherton-Beer, C.; Panes, G.; Griffiths, H.; Anderson, M.; Williams, T.; Griffiths, B.; Nobre, D.; Hill, A.M. Evaluation of older people’s knowledge, awareness, motivation and perceptions about falls and falls prevention in residential aged care homes: A tale of two cities. Ageing Soc. 2019, 39, 2541–2559. [Google Scholar] [CrossRef]
- Kruse, R.L.; Moore, C.M.; Tofle, R.B.; LeMaster, J.W.; Aud, M.; Hicks, L.L.; Mehr, D.R. Older Adults’ Attitudes Toward Home Modifications for Fall Prevention. J. Hous. Elder. 2010, 24, 110–129. [Google Scholar] [CrossRef]
- McInnes, E.; Askie, L. Evidence review on older people’s views and experiences of falls prevention strategies. Worldviews Evid. Based Nurse 2004, 1, 20–37. [Google Scholar] [CrossRef]
- Yardley, L.; Donovan-Hall, M.; Francis, K.; Todd, C. Older People’s Views of Falls-Prevention Interventions in Six European Countries. Gerontologist 2006, 46, 650–660. [Google Scholar] [CrossRef]
- Creswell, J. Research Design: Qualitative, Quantitative and Mixed Methods Approaches; SAGE Publications: London, UK, 2015. [Google Scholar]
- Morgan, D.L. Successful Focus Groups: Advancing the State of the Art; SAGE Publications: Thousand Oaks, CA, USA, 2013. [Google Scholar] [CrossRef]
- Curry, L.A.; Nembhard, I.M.; Bradley, E.H. Qualitative and Mixed Methods Provide Unique Contributions to Outcomes Research. Circulation 2009, 119, 1442–1452. [Google Scholar] [CrossRef]
- Thelu, M.; Webster, B.; Jones, K.; Orrell, M. A cross sectional survey on UK older adult’s attitudes to ageing, dementia and positive psychology attributes. BMC Geriatr. 2022, 22, 837. [Google Scholar] [CrossRef] [PubMed]
- Turner, A.; Nowson, C.; Worsley, A.; Devine, A.; Dyer, S.; Grimes, C. Knowledge, Attitudes, and Behaviours Concerning the Mediterranean Diet Among Older Adults in Australia. J. Community Health 2023, 48, 951–962. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, Y.; Suzuki, M.; Hata, Y.; Sakaki, T. Negative attitudes of healthy older adults toward unhealthy older adults: Focus on the subjective health. Arch. Gerontol. Geriatr. 2023, 105, 104850. [Google Scholar] [CrossRef] [PubMed]
- Kung, C.S.J.; Steptoe, A. Changes in Internet use patterns among older adults in England from before to after the outbreak of the COVID-19 pandemic. Sci. Rep. 2023, 13, 3932. [Google Scholar] [CrossRef]
- Age UK. The State of Health and Care of Older People in England 2024; Age UK: London, UK, 2024; Available online: https://www.ageuk.org.uk/siteassets/documents/reports-and-publications/reports-and-briefings/health--wellbeing/state-of-health-and-care/state_of_health_and_social_care_24.pdf (accessed on 29 April 2025).
- Yount, J. Strength in Numbers: A Community Education Program to Prevent Falls in Older Adults. Home Healthc. Now 2016, 34, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Pillay, J.; Gaudet, L.A.; Saba, S.; Vandermeer, B.; Ashiq, A.R.; Wingert, A.; Hartling, L. Falls prevention interventions for community-dwelling older adults: Systematic review and meta-analysis of benefits, harms, and patient values and preferences. Syst. Rev. 2024, 13, 289. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Thematic Analysis: A Practical Guide; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2021; ISBN 9781473953246. [Google Scholar]
- Horne, M.; Speed, S.; Skelton, D.; Todd, C. What do community-dwelling Caucasian and South Asian 60–70 year olds think about exercise for fall prevention? Age Ageing 2009, 38, 68–73. [Google Scholar] [CrossRef]
- Nyman, S.R.; Yardley, L. Usability and acceptability of a website that provides tailored advice on falls prevention activities for older people. Health Inform. J. 2009, 15, 27–39. [Google Scholar] [CrossRef]
- Bailey, C.; Aitken, D.; Wilson, G.; Hodgson, P.; Douglas, B.; Docking, R. “What? That’s for Old People, that.” Home Adaptations, Ageing and Stigmatisation: A Qualitative Inquiry. Int. J. Environ. Res. Public Health 2019, 16, 4989. [Google Scholar] [CrossRef]
- Nyman, S.R.; Victor, C.R. Older people’s participation in and engagement with falls prevention interventions in community settings: An augment to the cochrane systematic review. Age Ageing 2011, 41, 16–23. [Google Scholar] [CrossRef]
- Dorresteijn, T.A.C.; Rixt Zijlstra, G.A.; Van Eijs, Y.J.J.; Vlaeyen, J.W.S.; Kempen, G. Older people’s preferences regarding programme formats for managing concerns about falls. Age Ageing 2012, 41, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Khong, L.; Bulsara, C.; Hill, K.D.; Hill, A.-M. How older adults would like falls prevention information delivered: Fresh insights from a World Café forum. Ageing Soc. 2017, 37, 1179–1196. [Google Scholar] [CrossRef]
- Gumber, L.; Timmons, S.; Coupland, C.; Gladman, J.; Iliffe, S.; Kendrick, D.; Lafond, N.; Logan, P.; Masud, T.; Skelton, D.; et al. ‘It is designed for everybody to find their own level and to improve themselves’; views of older people and instructors of the Falls Management Exercise (FaME) programme. Age Ageing 2022, 51, afac023. [Google Scholar] [CrossRef] [PubMed]
- Kiami, S.; Sky, R.; Goodgold, S. Facilitators and barriers to enrolling in falls prevention programming among community dwelling older adults. Arch. Gerontol. Geriatr. 2019, 82, 106–113. [Google Scholar] [CrossRef]
- Gordon, N.P.; Hornbrook, M.C. Differences in Access to and Preferences for Using Patient Portals and Other eHealth Technologies Based on Race, Ethnicity, and Age: A Database and Survey Study of Seniors in a Large Health Plan. J. Med. Internet Res. 2016, 18, 50. [Google Scholar] [CrossRef]
- Carande-Kulis, V.; Stevens, J.A.; Florence, C.S.; Beattie, B.L.; Arias, I. A cost–benefit analysis of three older adult fall prevention interventions. J. Saf. Res. 2015, 52, 65–70. [Google Scholar] [CrossRef]
- Carnemolla, P.; Bridge, C. A scoping review of home modification interventions—Mapping the evidence base. Indoor Built Environ. 2018, 29, 299–310. [Google Scholar] [CrossRef]
- Powell, J.; McIntosh, S.; Bird, E.; Ige, J.; Garrett, H.; Roys, M. The Role of Home Adaptations in Improving Later Life; Centre for Ageing Better: London, UK, 2017. [Google Scholar]
- Hughes, K.; van Beurden, E.; Eakin, E.G.; Barnett, L.M.; Patterson, E.; Backhouse, J.; Jones, S.; Hauser, D.; Beard, J.R.; Newman, B. Older Persons’ Perception of Risk of Falling: Implications for Fall-Prevention Campaigns. Am. J. Public Health 2008, 98, 351–357. [Google Scholar] [CrossRef]
- Vaportzis, E.; Giatsi Clausen, M.; Gow, A.J. Older Adults Perceptions of Technology and Barriers to Interacting with Tablet Computers: A Focus Group Study. Front. Psychol. 2017, 8, 1687. [Google Scholar] [CrossRef]
| Question | Response Options | Percent of Respondents |
|---|---|---|
| Age | 55–59 | 21% |
| 60–64 | 27% | |
| 65–69 | 24% | |
| 70–74 | 10% | |
| 75–79 | 8% | |
| 80–84 | 7% | |
| 85–89 | 2% | |
| 90+ | 1% | |
| Gender | Male | 45% |
| Female | 55% | |
| Ethnicity | White | 81% |
| Black/African/Caribbean/Black British | 7% | |
| Asian/Asian British | 7% | |
| Mixed/Multiple Ethnic Groups | 2% | |
| Other Ethnic Group | 2% | |
| Undisclosed | 1% | |
| Living alone | Yes | 31% |
| No | 69% | |
| Property type | Detached house | 26% |
| Semi-detached | 25% | |
| Terraced house | 10% | |
| Bungalow (containing stairs) | 21% | |
| Flat/Apartment (containing/accessed via stairs) | 18% | |
| Housing tenure | Owner occupied | 80% |
| Private rented | 13% | |
| Social rented | 6% | |
| Other | 1% | |
| Previous stair fall | No | 44% |
| Yes, one fall | 32% | |
| Yes, more than one fall | 24% |
| Participant ID | Age | Gender | Ethnic Group | Stair-Fall History | Health Impairment | Living Alone | House Type |
|---|---|---|---|---|---|---|---|
| P1 | 70–74 | Male | White | Non-faller | Mobility, Dexterity | No | Semi-detached |
| P2 | 70–74 | Male | White | Non-faller | None | No | Detached |
| P3 | 75–79 | Female | White | Non-faller | Hearing | Yes | Terrace |
| P4 | 80–84 | Female | White | Non-faller | Other (not specified) | Yes | Semi-detached |
| P5 | 75–79 | Female | White | Non-faller | None | Yes | Terrace |
| P6 | 65–69 | Female | Other Ethnic Group | Faller | Hearing, Mobility | Yes | Terrace |
| P7 | 60–64 | Female | White | Faller | Vision | No | Detached |
| P8 | 70–74 | Female | White | Faller | None | Yes | Detached |
| Participant ID | Professional Role |
|---|---|
| S1 | Housing and Health and Stair Safety Consultant |
| S2 | Stair Safety Specialist |
| S3 | Housing and Falls Expert |
| S4 | Surveyor for Social Housing Provider |
| S5 | Consultant Geriatrician |
| S6 | Consultant Geriatrician, NHS |
| S7 | Lead Practitioner for Prevention of Falls (Inpatient) |
| S8 | Clinical Fall Lead and Pathway Co-ordinator (Outpatient) |
| S9 | Community Physiotherapist |
| S10 | Occupational Therapist, NHS |
| S11 | Specialist Falls Nurse, NHS |
| Intervention | Barrier Themes | Facilitator Themes | |
|---|---|---|---|
| Environment | Rebuild stairs Optical illusion Change stair coverings (plain décor) Physical edge highlighter Lighting edge highlighter | Cost | Financial assistance/funding |
| Space constraints | Guidance and advice | ||
| Disruption/rehousing | Raising awareness | ||
| Lack of decision-making power or living with others | Practical demonstrations | ||
| Not knowing where to find reliable advice/tradesmen | Research evidence | ||
| Lack of awareness of risk | Adaptable design to meet aesthetic preferences | ||
| Doubts about efficacy/Lack of understanding of intervention | Social support and encouragement | ||
| Suitability for individual health status | |||
| Aesthetics | |||
| Stigma and pride | |||
| Ambient lighting Additional handrail | Space constraints | ||
| Cost | Economical options | ||
| Lack of understanding (e.g., safest changes, accessing tradesmen) | Guidance and advice | ||
| Lack of decision-making power or living with others | Raising awareness | ||
| Stigma and pride | Social support and encouragement | ||
| Habitual behaviour | Behaviour change | ||
| Behaviour and Capability | Physical training Skill training Education | Relevance/suitability for individual health status | Tailored to individual needs and circumstances |
| Lack of awareness of risks | Raising awareness in general public | ||
| Access by and promotion of information to target audience | Trusted referrals and advice | ||
| Personal preferences for delivery style | Variety of delivery options | ||
| Motivation/maintaining engagement of end-users | Social support and encouragement | ||
| Lack of resources in health sector | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mulliner, E.; O’Brien, T.D.; Maliene, V.; Maganaris, C.N.; Mason, R. Older Adults’ and Professionals’ Attitudes Towards Stair-Fall Prevention Interventions. Healthcare 2025, 13, 1324. https://doi.org/10.3390/healthcare13111324
Mulliner E, O’Brien TD, Maliene V, Maganaris CN, Mason R. Older Adults’ and Professionals’ Attitudes Towards Stair-Fall Prevention Interventions. Healthcare. 2025; 13(11):1324. https://doi.org/10.3390/healthcare13111324
Chicago/Turabian StyleMulliner, Emma, Thomas D. O’Brien, Vida Maliene, Constantinos N. Maganaris, and Rachel Mason. 2025. "Older Adults’ and Professionals’ Attitudes Towards Stair-Fall Prevention Interventions" Healthcare 13, no. 11: 1324. https://doi.org/10.3390/healthcare13111324
APA StyleMulliner, E., O’Brien, T. D., Maliene, V., Maganaris, C. N., & Mason, R. (2025). Older Adults’ and Professionals’ Attitudes Towards Stair-Fall Prevention Interventions. Healthcare, 13(11), 1324. https://doi.org/10.3390/healthcare13111324