
One Cup of Coffee a Day Modulates the Relationship between Metabolic Syndrome and Eating Fast: A Cross-Sectional Study


Abstract
1. Background
2. Methods
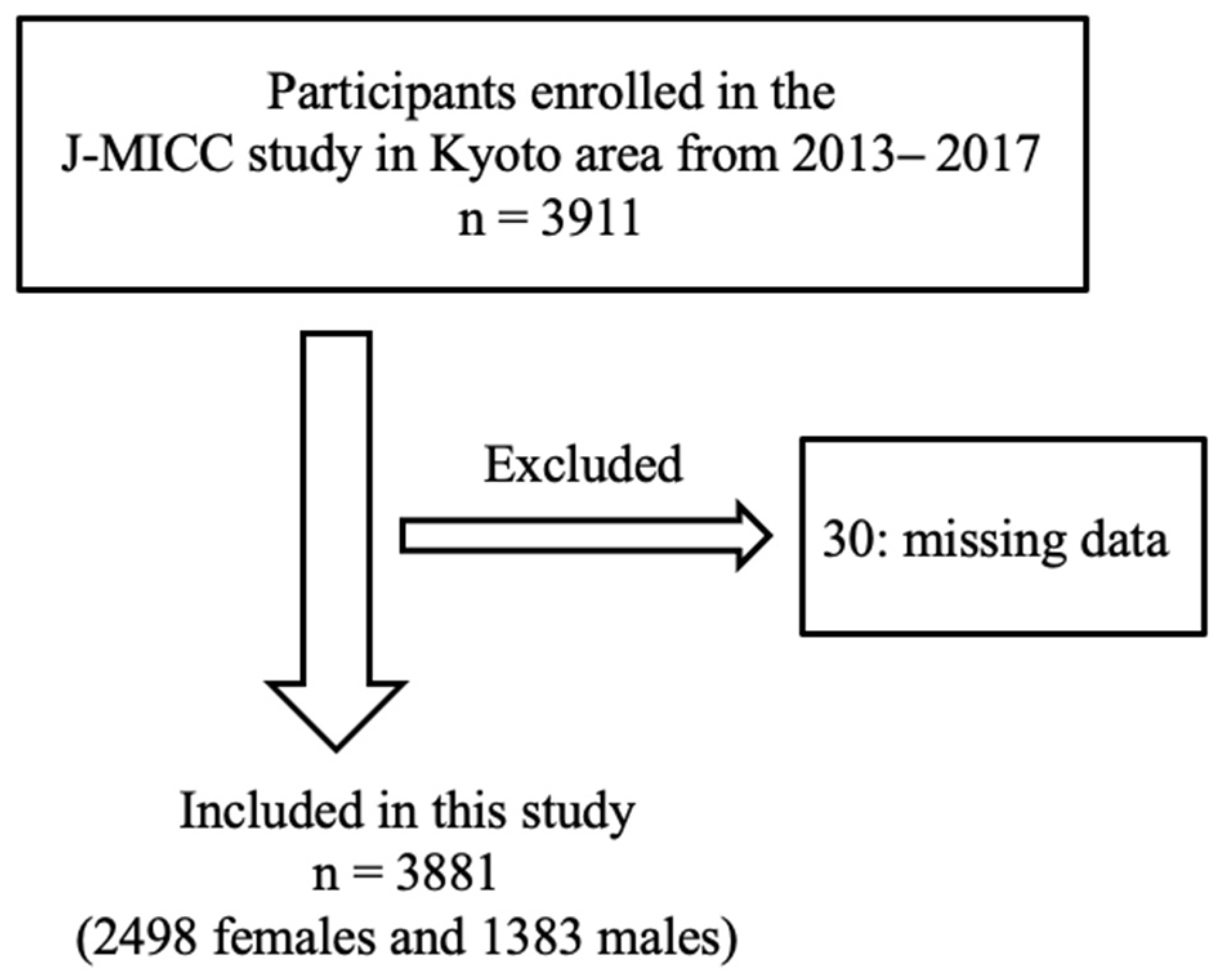
2.1. Study Population and Design
2.2. Data Collection and Measurements
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Esposito, K.; Chiodini, P.; Colao, A.; Lenzi, A.; Giugliano, D. Metabolic syndrome and risk of cancer: A systematic review and meta-analysis. Diabetes Care 2012, 35, 2402–2411. [Google Scholar] [CrossRef]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef]
- Yuan, S.Q.; Liu, Y.M.; Liang, W.; Li, F.F.; Zeng, Y.; Liu, Y.Y.; Huang, S.Z.; He, Q.Y.; Quach, B.; Jiao, J.; et al. Association Between Eating Speed and Metabolic Syndrome: A Systematic Review and Meta-Analysis. Front. Nutr. 2021, 8, 700936. [Google Scholar] [CrossRef]
- Hurst, Y.; Fukuda, H. Effects of changes in eating speed on obesity in patients with diabetes: A secondary analysis of longitudinal health check-up data. BMJ Open 2018, 8, e019589. [Google Scholar] [CrossRef] [PubMed]
- Nagahama, S.; Kurotani, K.; Pham, N.M.; Nanri, A.; Kuwahara, K.; Dan, M.; Nishiwaki, Y.; Mizoue, T. Self-reported eating rate and metabolic syndrome in Japanese people: Cross-sectional study. BMJ Open 2014, 4, e005241. [Google Scholar] [CrossRef]
- World Cancer Research Fund International. Diet, Activity and Cancer. Available online: https://worldpopulationreview.com/country-rankings/coffee-consumption-by-country (accessed on 28 February 2024).
- Shang, F.; Li, X.; Jiang, X. Coffee consumption and risk of the metabolic syndrome: A meta-analysis. Diabetes Metab. 2016, 42, 80–87. [Google Scholar] [CrossRef]
- Naveed, M.; Hejazi, V.; Abbas, M.; Kamboh, A.A.; Khan, G.J.; Shumzaid, M.; Ahmad, F.; Babazadeh, D.; FangFang, X.; Modarresi-Ghazani, F.; et al. Chlorogenic acid (CGA): A pharmacological review and call for further research. Biomed. Pharmacother. 2018, 97, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Tajik, N.; Tajik, M.; Mack, I.; Enck, P. The potential effects of chlorogenic acid, the main phenolic components in coffee, on health: A comprehensive review of the literature. Eur. J. Nutr. 2017, 56, 2215–2244. [Google Scholar] [CrossRef] [PubMed]
- Tanihara, S.; Imatoh, T.; Miyazaki, M.; Babazono, A.; Momose, Y.; Baba, M.; Uryu, Y.; Une, H. Retrospective longitudinal study on the relationship between 8-year weight change and current eating speed. Appetite 2011, 57, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Yamane, M.; Ekuni, D.; Mizutani, S.; Kataoka, K.; Sakumoto-Kataoka, M.; Kawabata, Y.; Omori, C.; Azuma, T.; Tomofuji, T.; Iwasaki, Y.; et al. Relationships between eating quickly and weight gain in Japanese university students: A longitudinal study. Obesity 2014, 22, 2262–2266. [Google Scholar] [CrossRef] [PubMed]
- Verhoeven, A.A.; Adriaanse, M.A.; Evers, C.; de Ridder, D.T. The power of habits: Unhealthy snacking behaviour is primarily predicted by habit strength. Br. J. Health Psychol. 2012, 17, 758–770. [Google Scholar] [CrossRef]
- Wakai, K.; Hamajima, N.; Okada, R.; Naito, M.; Morita, E.; Hishida, A.; Kawai, S.; Nishio, K.; Yin, G.; Asai, Y.; et al. Profile of Participants and Genotype Distributions of 108 Polymorphisms in a Cross-Sectional Study of Associations of Genotypes with Lifestyle and Clinical Factors: A Project in the Japan Multi-Institutional Collaborative Cohort (J-MICC) Study. J. Epidemiol. 2011, 21, 223–235. [Google Scholar] [CrossRef]
- Haraguchi, N.; Koyama, T.; Kuriyama, N.; Ozaki, E.; Matsui, D.; Watanabe, I.; Uehara, R.; Watanabe, Y. Assessment of anthropometric indices other than BMI to evaluate arterial stiffness. Hypertens. Res. 2019, 42, 1599–1605. [Google Scholar] [CrossRef]
- Tokudome, Y.; Goto, C.; Imaeda, N.; Hasegawa, T.; Kato, R.; Hirose, K.; Tajima, K.; Tokudome, S. Relative validity of a short food frequency questionnaire for assessing nutrient intake versus three-day weighed diet records in middle-aged Japanese. J. Epidemiol. 2005, 15, 135–145. [Google Scholar] [CrossRef]
- Imaeda, N.; Goto, C.; Tokudome, Y.; Hirose, K.; Tajima, K.; Tokudome, S. Reproducibility of a short food frequency questionnaire for Japanese general population. J. Epidemiol. 2007, 17, 100–107. [Google Scholar] [CrossRef]
- Goto, C.; Tokudome, Y.; Imaeda, N.; Takekuma, K.; Kuriki, K.; Igarashi, F.; Ikeda, M.; Tokudome, S. Validation study of fatty acid consumption assessed with a short food frequency questionnaire against plasma concentration in middle-aged Japanese people. Scand. J. Food Nutr. 2006, 50, 77–82. [Google Scholar] [CrossRef]
- Tokudome, S.; Goto, C.; Imaeda, N.; Tokudome, Y.; Ikeda, M.; Maki, S. Development of a data-based short food frequency questionnaire for assessing nutrient intake by middle-aged Japanese. Asian Pac. J. Cancer Prev. 2004, 5, 40–43. [Google Scholar]
- Imaeda, N.; Goto, C.; Sasakabe, T.; Mikami, H.; Oze, I.; Hosono, A.; Naito, M.; Miyagawa, N.; Ozaki, E.; Ikezaki, H.; et al. Reproducibility and validity of food group intake in a short food frequency questionnaire for the middle-aged Japanese population. Environ. Health Prev. Med. 2021, 26, 28. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Hara, M.; Higaki, Y.; Taguchi, N.; Shinchi, K.; Morita, E.; Naito, M.; Hamajima, N.; Takashima, N.; Suzuki, S.; Nakamura, A.; et al. Effect of the PPARG2 Pro12Ala polymorphism and clinical risk factors for diabetes mellitus on HbA1c in the Japanese general population. J. Epidemiol. 2012, 22, 523–531. [Google Scholar] [CrossRef]
- Hara, M.; Hachiya, T.; Sutoh, Y.; Matsuo, K.; Nishida, Y.; Shimanoe, C.; Tanaka, K.; Shimizu, A.; Ohnaka, K.; Kawaguchi, T.; et al. Genomewide Association Study of Leisure-Time Exercise Behavior in Japanese Adults. Med. Sci. Sport. Exerc. 2018, 50, 2433–2441. [Google Scholar] [CrossRef]
- Yamagishi, K.; Iso, H. The criteria for metabolic syndrome and the national health screening and education system in Japan. Epidemiol. Health 2017, 39, e2017003. [Google Scholar] [CrossRef]
- Baspinar, B.; Eskici, G.; Ozcelik, A.O. How coffee affects metabolic syndrome and its components. Food Funct. 2017, 8, 2089–2101. [Google Scholar] [CrossRef]
- Kim, H.J.; Cho, S.; Jacobs, D.R., Jr.; Park, K. Instant coffee consumption may be associated with higher risk of metabolic syndrome in Korean adults. Diabetes Res. Clin. Pract. 2014, 106, 145–153. [Google Scholar] [CrossRef]
- Otsuka, R.; Tamakoshi, K.; Yatsuya, H.; Murata, C.; Sekiya, A.; Wada, K.; Zhang, H.M.; Matsushita, K.; Sugiura, K.; Takefuji, S.; et al. Eating fast leads to obesity: Findings based on self-administered questionnaires among middle-aged Japanese men and women. J. Epidemiol. 2006, 16, 117–124. [Google Scholar] [CrossRef]
- Otsuka, R.; Tamakoshi, K.; Yatsuya, H.; Wada, K.; Matsushita, K.; OuYang, P.; Hotta, Y.; Takefuji, S.; Mitsuhashi, H.; Sugiura, K.; et al. Eating fast leads to insulin resistance: Findings in middle-aged Japanese men and women. Prev. Med. 2008, 46, 154–159. [Google Scholar] [CrossRef]
- Sakurai, M.; Nakamura, K.; Miura, K.; Takamura, T.; Yoshita, K.; Nagasawa, S.Y.; Morikawa, Y.; Ishizaki, M.; Kido, T.; Naruse, Y.; et al. Self-reported speed of eating and 7-year risk of type 2 diabetes mellitus in middle-aged Japanese men. Metabolism 2012, 61, 1566–1571. [Google Scholar] [CrossRef]
- Zhu, B.; Haruyama, Y.; Muto, T.; Yamazaki, T. Association between eating speed and metabolic syndrome in a three-year population-based cohort study. J. Epidemiol. 2015, 25, 332–336. [Google Scholar] [CrossRef]
- Maruyama, K.; Sato, S.; Ohira, T.; Maeda, K.; Noda, H.; Kubota, Y.; Nishimura, S.; Kitamura, A.; Kiyama, M.; Okada, T.; et al. The joint impact on being overweight of self reported behaviours of eating quickly and eating until full: Cross sectional survey. BMJ 2008, 337, a2002. [Google Scholar] [CrossRef]
- Hsieh, S.D.; Muto, T.; Murase, T.; Tsuji, H.; Arase, Y. Eating until feeling full and rapid eating both increase metabolic risk factors in Japanese men and women. Public Health Nutr. 2011, 14, 1266–1269. [Google Scholar] [CrossRef][Green Version]
- Lee, A.; Lim, W.; Kim, S.; Khil, H.; Cheon, E.; An, S.; Hong, S.; Lee, D.H.; Kang, S.S.; Oh, H.; et al. Coffee Intake and Obesity: A Meta-Analysis. Nutrients 2019, 11, 1274. [Google Scholar] [CrossRef]
- Pauwels, E.K.J.; Volterrani, D. Coffee Consumption and Cancer Risk: An Assessment of the Health Implications Based on Recent Knowledge. Med. Princ. Pract. 2021, 30, 401–411. [Google Scholar] [CrossRef]
- Jiménez, S.L.; Díaz-Lara, J.; Pareja-Galeano, H.; Del Coso, J. Caffeinated Drinks and Physical Performance in Sport: A Systematic Review. Nutrients 2021, 13, 2944. [Google Scholar] [CrossRef]
- Harpaz, E.; Tamir, S.; Weinstein, A.; Weinstein, Y. The effect of caffeine on energy balance. J. Basic Clin. Physiol. Pharmacol. 2017, 28, 1–10. [Google Scholar] [CrossRef]
- Ding, M.; Bhupathiraju, S.N.; Chen, M.; van Dam, R.M.; Hu, F.B. Caffeinated and decaffeinated coffee consumption and risk of type 2 diabetes: A systematic review and a dose-response meta-analysis. Diabetes Care 2014, 37, 569–586. [Google Scholar] [CrossRef]
- Huxley, R.; Lee, C.M.; Barzi, F.; Timmermeister, L.; Czernichow, S.; Perkovic, V.; Grobbee, D.E.; Batty, D.; Woodward, M. Coffee, decaffeinated coffee, and tea consumption in relation to incident type 2 diabetes mellitus: A systematic review with meta-analysis. Arch. Intern. Med. 2009, 169, 2053–2063. [Google Scholar] [CrossRef]
- Thom, E. The effect of chlorogenic acid enriched coffee on glucose absorption in healthy volunteers and its effect on body mass when used long-term in overweight and obese people. J. Int. Med. Res. 2007, 35, 900–908. [Google Scholar] [CrossRef]
- Ramli, N.N.S.; Alkhaldy, A.A.; Mhd Jalil, A.M. Effects of Caffeinated and Decaffeinated Coffee Consumption on Metabolic Syndrome Parameters: A Systematic Review and Meta-Analysis of Data from Randomised Controlled Trials. Medicina 2021, 57, 957. [Google Scholar] [CrossRef]


{kind=link}
| Eating Speed | ||||||||
|---|---|---|---|---|---|---|---|---|
| Slow | Normal | Fast | p-Value | |||||
| Mean/n | SD/% | Mean/n | SD/% | Mean/n | SD/% | |||
| All | n = 523 | n = 1963 | n = 1395 | |||||
| Sex (female), n [%] | 350 | [66.9] | 1303 | [66.4] | 845 | [60.6] | 0.001 | |
| Age (years), mean [SD] | 57.9 | [10.2] | 58.0 | [9.9] | 56.5 a* | [9.8] | <0.001 | |
| METs (h/day), mean [SD] | 14.2 | [10.3] | 14.8 | [10.4] | 14.4 | [10.7] | 0.225 | |
| Smokers, n [%] | ||||||||
| Current | 44 | [8.4] | 181 | [9.2] | 127 | [9.1] | 0.049 | |
| Former | 115 | [22.0] | 434 | [22.1] | 367 | [26.3] | ||
| Never | 364 | [69.6] | 1348 | [68.7] | 901 | [64.6] | ||
| Current drinkers, n [%] | ||||||||
| Current | 315 | [60.2] | 1143 | [58.2] | 830 | [59.5] | 0.542 | |
| Former | 5 | [1.0] | 30 | [1.5] | 26 | [1.9] | ||
| Never | 203 | [38.8] | 791 | [40.3] | 539 | [38.6] | ||
| Coffee (drip, filter, or instant) ≥ 1 cup/day, n [%] | 336 | [64.2] | 1312 | [66.8] | 981 | [70.3] | 0.019 | |
| Coffee (canned, plastic bottle, or carton) ≥ 1 cup/day, n [%] | 39 | [7.5] | 157 | [8.0] | 127 | [9.1] | 0.387 | |
| Ischemic heart disease, n [%] | 3 | [0.6] | 18 | [0.9] | 3 | [0.2] | 0.038 | |
| Stroke, n [%] | 11 | [2.1] | 32 | [1.6] | 21 | [1.5] | 0.655 | |
| BMI (kg/m2), mean [SD] | 21.5 | [3.2] | 22.0 b** | [3.1] | 22.9 b** | [3.3] | <0.001 | |
| Waist circumference (cm), mean [SD] | 79.1 | [9.1] | 80.2 a* | [9.1] | 82.3 b** | [9.4] | <0.001 | |
| Systolic blood pressure (mmHg), mean [SD] | 128 | [19.8] | 129 | [19.1] | 130 | [19.3] | 0.249 | |
| Diastolic blood pressure (mmHg), mean [SD] | 77.6 | [11.2] | 79.4 b** | [11.2] | 79.9 b** | [11.6] | 0.001 | |
| Triglyceride (mg/dL), mean [SD] | 91.5 | [59.1] | 100.0 | [76.0] | 104 b** | [71.6] | <0.001 | |
| HDL-cholesterol (mg/dL), mean [SD] | 72.8 | [16.6] | 70.6 b** | [17.5] | 69.1 b** | [17.3] | <0.001 | |
| LDL-cholesterol (mg/dL), mean [SD] | 122 | [30.8] | 126 a* | [30.4] | 126 | [30.9] | 0.040 | |
| Glucose (mg/dL), mean [SD] | 90.8 | [16.4] | 90.2 | [13.5] | 91.0 | [15.6] | 0.752 | |
| Hemoglobin A1c (%), mean [SD] | 5.6 | [0.5] | 5.6 | [0.4] | 5.6 | [0.5] | 0.516 | |
| Energy (kcal/day), mean [SD] | 1607 | [317] | 1586 | [348] | 1627 | [377] | 0.010 | |
| Metabolic syndrome, n [%] | 64 | [12.2] | 280 | [14.3] | 251 | [18.0] | 0.001 | |
| Female | n = 350 | n = 1303 | n = 845 | |||||
| Age (years), mean [SD] | 57.2 | [10.2] | 57.2 | [9.8] | 56.3 | [9.8] | 0.117 | |
| METs (h/day), mean [SD] | 14.6 | [10.4] | 15.0 | [10.3] | 14.8 | [10.1] | 0.646 | |
| Smokers, n [%] | ||||||||
| Current | 16 | [4.6] | 59 | [4.5] | 28 | [3.3] | 0.042 | |
| Former | 39 | [11.1] | 125 | [9.6] | 115 | [13.6] | ||
| Never | 295 | [84.3] | 1119 | [85.9] | 702 | [83.1] | ||
| Current drinkers, n [%] | ||||||||
| Current | 178 | [50.9] | 630 | [48.0] | 430 | [50.9] | 0.754 | |
| Former | 4 | [1.1] | 16 | [1.2] | 12 | [1.4] | ||
| Never | 168 | [45.8] | 657 | [50.4] | 403 | [47.7] | ||
| Coffee (drip, filter, or instant) ≥ 1 cup/day, n [%] | 227 | [64.9] | 893 | [68.5] | 612 | [72.4] | 0.024 | |
| Coffee (canned, plastic bottle, or carton) ≥ 1 cup/day, n [%] | 19 | [5.4] | 71 | [5.4] | 38 | [4.5] | 0.597 | |
| Ischemic heart disease, n [%] | 0 | [0] | 5 | [0.4] | 0 | [0] | 0.101 | |
| Stroke, n [%] | 5 | [1.4] | 20 | [1.5] | 10 | [1.2] | 0.794 | |
| BMI (kg/m2), mean [SD] | 21.0 | [3.2] | 21.3 a* | [3.0] | 22.1 b** | [3.3] | <0.001 | |
| Waist circumference (cm), mean [SD] | 77.2 | [9.2] | 78.0 | [8.7] | 80.0 b** | [9.2] | <0.001 | |
| Systolic blood pressure (mmHg), mean [SD] | 125 | [19.4] | 126 | [18.5] | 126 | [19.7] | 0.378 | |
| Diastolic blood pressure (mmHg), mean [SD] | 75.6 | [11.0] | 77.2 a* | [10.8] | 77.6 a* | [11.3] | 0.016 | |
| Triglyceride (mg/dL), mean [SD] | 81.7 | [41.3] | 87.7 | [64.3] | 90.5 a* | [50.6] | 0.010 | |
| HDL-cholesterol (mg/dL), mean [SD] | 76.7 | [15.8] | 75.1 | [16.7] | 74.1 a* | [16.3] | 0.023 | |
| LDL-cholesterol (mg/dL), mean [SD] | 126 | [31.2] | 128 | [30.8] | 128 | [32.7] | 0.314 | |
| Glucose (mg/dL), mean [SD] | 88.8 | [14.5] | 87.9 | [11.5] | 88.4 | [12.5] | 0.986 | |
| Hemoglobin A1c (%), mean [SD] | 5.6 | [0.5] | 5.5 | [0.4] | 5.5 | [0.4] | 0.749 | |
| Energy (kcal/day), mean [SD] | 1502 | [240] | 1464 | [261] | 1482 | [287] | 0.063 | |
| Metabolic syndrome, n [%] | 21 | [6.0] | 74 | [5.7] | 70 | [8.3] | 0.053 | |
| Male | n = 173 | n = 660 | n = 550 | |||||
| Age (years), mean [SD] | 59.5 | [10.0] | 59.7 | [9.9] | 56.7 b** | [9.9] | <0.001 | |
| METs (h/day), mean [SD] | 13.4 | [10.1] | 14.2 | [10.5] | 13.8 | [11.7] | 0.361 | |
| Smokers, n [%] | ||||||||
| Current | 28 | [16.2] | 122 | [18.5] | 99 | [18.0] | 0.790 | |
| Former | 76 | [43.9] | 309 | [46.8] | 252 | [45.8] | ||
| Never | 69 | [39.9] | 229 | [34.7] | 199 | [36.2] | ||
| Current drinkers, n [%] | ||||||||
| Current | 137 | [79.2] | 512 | [77.6] | 400 | [72.7] | 0.158 | |
| Former | 1 | [0.6] | 14 | [2.1] | 14 | [2.5] | ||
| Never | 35 | [20.2] | 134 | [20.3] | 136 | [24.7] | ||
| Coffee (drip, filter, or instant) ≥ 1 cup/day, n [%] | 109 | [63] | 419 | [63.5] | 369 | [67.1] | 0.366 | |
| Coffee (canned, plastic bottle, or carton) ≥ 1 cup/day, n [%] | 20 | [11.6] | 86 | [13.0] | 89 | [16.2] | 0.173 | |
| Ischemic heart disease, n [%] | 3 | [1.7] | 13 | [2.0] | 3 | [0.5] | 0.096 | |
| Stroke, n [%] | 6 | [3.5] | 12 | [1.8] | 11 | [2.0] | 0.395 | |
| BMI (kg/m2), mean [SD] | 22.7 | [2.8] | 23.3 a* | [2.9] | 24.0 b** | [3.0] | <0.001 | |
| Waist circumference (cm), mean [SD] | 83.0 | [7.6] | 84.5 | [8.2] | 85.9 b** | [8.6] | <0.001 | |
| Systolic blood pressure (mmHg), mean [SD] | 135 | [18.6] | 136 | [18.5] | 135 | [18.0] | 0.325 | |
| Diastolic blood pressure (mmHg), mean [SD] | 81.8 | [10.6] | 83.8 | [10.7] | 83.4 | [11.2] | 0.107 | |
| Triglyceride (mg/dL), mean [SD] | 111 | [81.0] | 125 | [89.9] | 125 | [86.6] | 0.083 | |
| HDL-cholesterol (mg/dL), mean [SD] | 64.8 | [15.2] | 61.6 a* | [15.6] | 61.3 a* | [15.9] | 0.010 | |
| LDL-cholesterol (mg/dL), mean [SD] | 115 | [28.6] | 122 a* | [29.1] | 124 b** | [29.7] | 0.006 | |
| Glucose (mg/dL), mean [SD] | 94.9 | [19.1] | 94.9 | [15.8] | 94.9 | [18.7] | 0.244 | |
| Hemoglobin A1c (%), mean [SD] | 5.7 | [0.6] | 5.6 | [0.5] | 5.6 | [0.6] | 0.543 | |
| Energy (kcal/day), mean [SD] | 1817 | [348] | 1828 | [372] | 1848 | [392] | 0.574 | |
| Metabolic syndrome, n [%] | 43 | [24.9] | 206 | [31.2] | 181 | [32.9] | 0.136 | |
| OR | 95% CI | p-Value | ||
|---|---|---|---|---|
| All | Coffee (filtered or instant) < 1 cup/day | Ref | ||
| Coffee (filtered or instant) ≥ 1 cup/day | 0.695 | 0.570–0.847 | <0.001 | |
| Coffee (canned, bottled or packed) < 1 cup/day | Ref | |||
| Coffee (canned, bottled or packed) ≥ 1 cup/day | 1.187 | 0.867–1.626 | 0.284 | |
| Eating speed | ||||
| Slow | Ref | |||
| Normal | 1.212 | 0.887–1.656 | 0.228 | |
| Fast | 1.689 | 1.227–2.324 | 0.001 | |
| Female | Coffee (filtered or instant) < 1 cup/day | Ref | ||
| Coffee (filtered or instant) ≥ 1 cup/day | 0.570 | 0.410–0.792 | 0.001 | |
| Coffee (canned, bottled or packed) < 1 cup/day | Ref | |||
| Coffee (canned, bottled or packed) ≥ 1 cup/day | 2.056 | 1.110–3.811 | 0.022 | |
| Eating speed | ||||
| Slow | Ref | |||
| Normal | 0.973 | 0.585–1.619 | 0.917 | |
| Fast | 1.607 | 0.960–2.691 | 0.071 | |
| Male | Coffee (filtered or instant) <1 cup/day | Ref | ||
| Coffee (filtered or instant) ≥1 cup/day | 0.784 | 0.613–1.003 | 0.053 | |
| Coffee (canned, bottled or packed) <1 cup/day | Ref | |||
| Coffee (canned, bottled or packed) ≥1 cup/day | 1.030 | 0.722–1.468 | 0.872 | |
| Eating speed | ||||
| Slow | Ref | |||
| Normal | 1.337 | 0.930–2.038 | 0.110 | |
| Fast | 1.750 | 1.171–2.616 | 0.006 | |
| Number | Number of MetS | OR | 95% CI | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| All | Coffee (filtered or instant) < 1 cup/day | Eating speed | Slow | 163 | 24 | 0.502 | 0.296–0.851 | 0.010 |
| Normal | 534 | 117 | 0.734 | 0.525–1.028 | 0.072 | |||
| Fast | 324 | 90 | Ref | |||||
| Coffee (filtered or instant) ≥ 1 cup/day | Eating speed | Slow | 296 | 40 | 0.448 | 0.289–0.693 | <0.001 | |
| Normal | 1149 | 163 | 0.482 | 0.353–0.658 | <0.001 | |||
| Fast | 820 | 161 | 0.684 | 0.499–0.936 | 0.018 | |||
| Female | Coffee (filtered or instant) < 1 cup/day | Eating speed | Slow | 115 | 8 | 0.414 | 0.182–0.942 | 0.036 |
| Normal | 380 | 30 | 0.470 | 0.274–0.806 | 0.006 | |||
| Fast | 201 | 32 | Ref | |||||
| Coffee (filtered or instant) ≥ 1 cup/day | Eating speed | Slow | 214 | 13 | 0.360 | 0.182–0.714 | 0.003 | |
| Normal | 849 | 44 | 0.310 | 0.190–0.507 | <0.001 | |||
| Fast | 574 | 38 | 0.423 | 0.255–0.702 | 0.001 | |||
| Male | Coffee (filtered or instant) < 1 cup/day | Eating speed | Slow | 48 | 16 | 0.576 | 0.295–1.122 | 0.105 |
| Normal | 154 | 87 | 0.963 | 0.631–1.469 | 0.860 | |||
| Fast | 123 | 58 | Ref | |||||
| Coffee (filtered or instant) ≥ 1 cup/day | Eating speed | Slow | 82 | 27 | 0.527 | 0.303–0.915 | 0.023 | |
| Normal | 300 | 119 | 0.643 | 0.434–0.953 | 0.028 | |||
| Fast | 246 | 123 | 0.916 | 0.618–1.358 | 0.662 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hiramatsu, R.; Ozaki, E.; Tomida, S.; Koyama, T. One Cup of Coffee a Day Modulates the Relationship between Metabolic Syndrome and Eating Fast: A Cross-Sectional Study. Healthcare 2024, 12, 603. https://doi.org/10.3390/healthcare12060603
Hiramatsu R, Ozaki E, Tomida S, Koyama T. One Cup of Coffee a Day Modulates the Relationship between Metabolic Syndrome and Eating Fast: A Cross-Sectional Study. Healthcare. 2024; 12(6):603. https://doi.org/10.3390/healthcare12060603
Chicago/Turabian StyleHiramatsu, Reisa, Etsuko Ozaki, Satomi Tomida, and Teruhide Koyama. 2024. "One Cup of Coffee a Day Modulates the Relationship between Metabolic Syndrome and Eating Fast: A Cross-Sectional Study" Healthcare 12, no. 6: 603. https://doi.org/10.3390/healthcare12060603
APA StyleHiramatsu, R., Ozaki, E., Tomida, S., & Koyama, T. (2024). One Cup of Coffee a Day Modulates the Relationship between Metabolic Syndrome and Eating Fast: A Cross-Sectional Study. Healthcare, 12(6), 603. https://doi.org/10.3390/healthcare12060603