
Differences in the Glenohumeral Joint before and after Unilateral Breast Cancer Surgery: Motion Capture Analysis

 ,
,  ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Anthropometric Data of the Patients
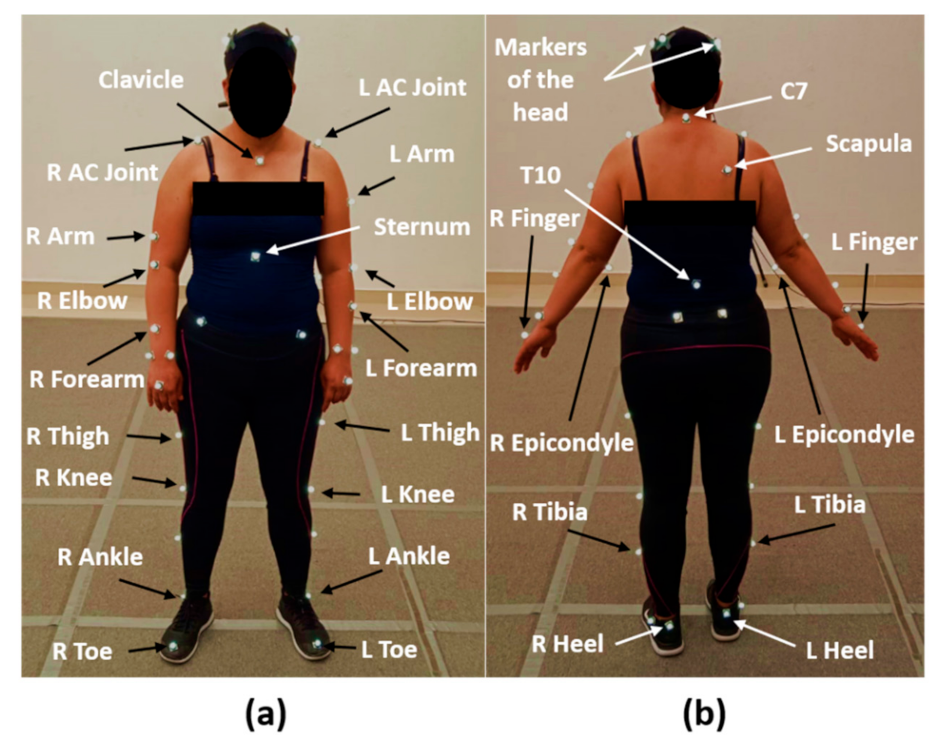
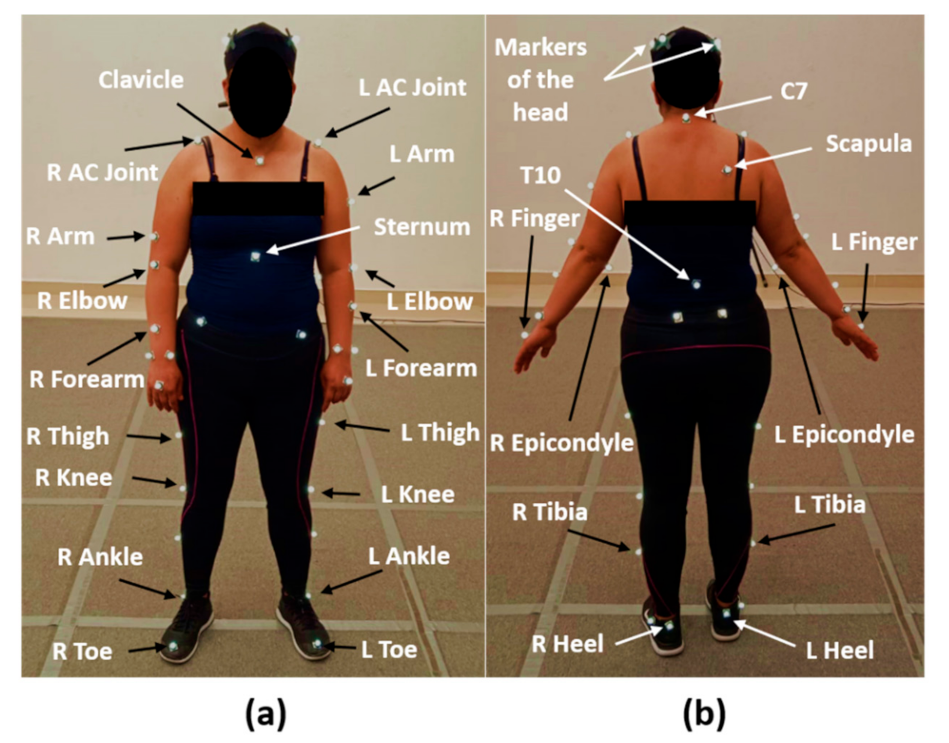
2.2. Experimental Protocol
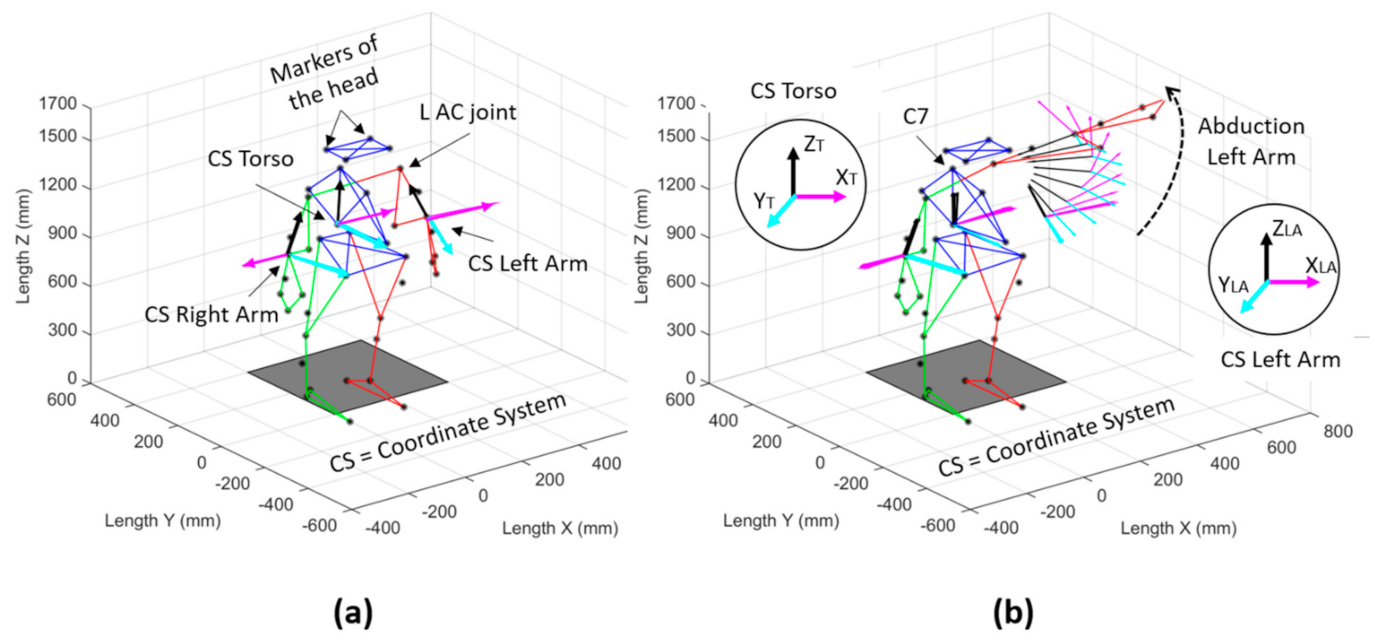
2.3. Data Processing
2.4. Statistical Analysis
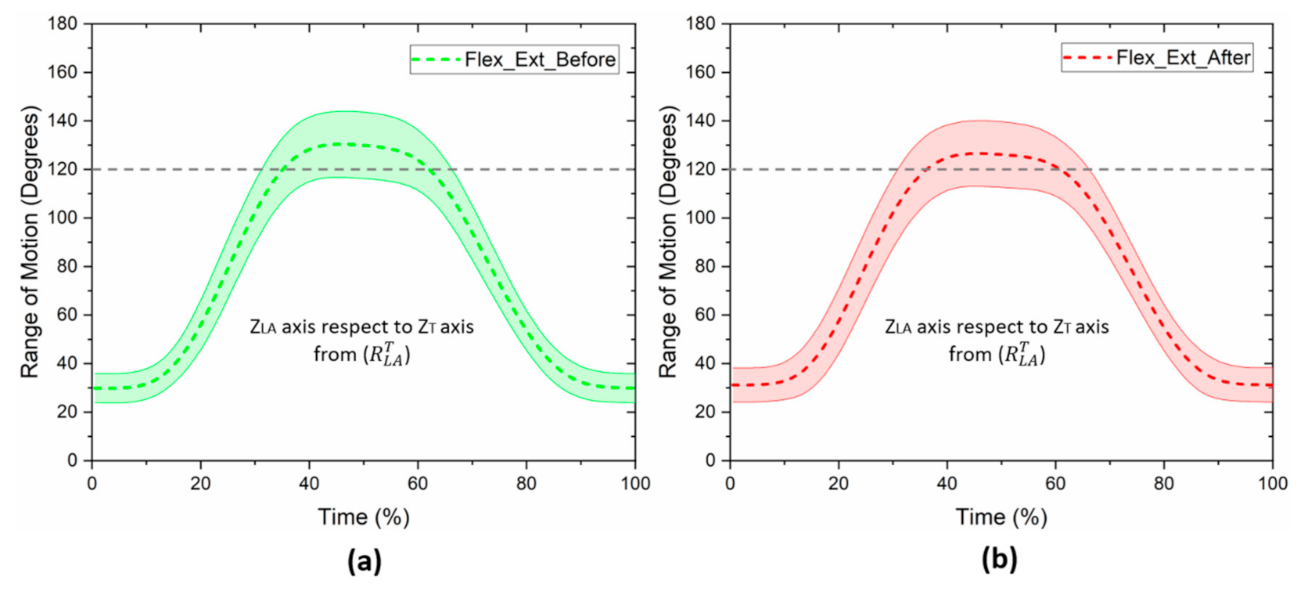
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Cancer Society. Breast Cancer Facts and Figures 2019–2020; American Cancer Society, Inc.: Atlanta, GA, USA, 2019. [Google Scholar]
- Feng, Y.; Spezia, M.; Huang, S.; Yuan, C.; Zeng, Z.; Zhang, L.; Ji, X.; Liu, W.; Huang, B.; Luo, W.; et al. Breast cancer development and progression: Risk factors, cancer stem cells, signaling pathways, genomics, and molecular pathogenesis. Genes Dis. 2018, 5, 77–106. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Mohar-Betancourt, A.; Reynoso-Noverón, N.; Armas-Texta, D.; Gutiérrez-Delgado, C.; Torres-Domínguez, J.A. Cancer Trends in Mexico: Essential Data for the Creation and Follow-Up of Public Policies. J. Glob. Oncol. 2017, 3, 740–748. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. Global Cancer Statistics 2020: Mexico. In Cancer Today; The Global Cancer ObServatory: Lyon, France, 2021; p. 2. [Google Scholar]
- Dey, B.; Kumar, A. A review article on breast Cancer. IjpprHuman 2018, 11, 284–298. [Google Scholar]
- Chrischilles, E.A.; Riley, D.; Letuchy, E.; Koehler, L.A.; Neuner, J.; Jernigan, C.; Gryzlak, B.; Segal, N.; McDowell, B.; Smith, B.; et al. Upper extremity disability and quality of life after breast cancer treatment in the Greater Plains Collaborative clinical research network. Breast Cancer Res. Treat. 2019, 175, 675–689. [Google Scholar] [CrossRef] [Green Version]
- Smoot, B.; Wampler, M.; Topp, K.S. Breast Cancer Treatments and Complications: Implications for Rehabilitation. Rehabil. Oncol. 2009, 27, 16–26. [Google Scholar] [CrossRef]
- Kaur, N.; Kumar, A.; Saxena, A.K.; Gupta, A.; Grover, R.K. Postmastectomy Chronic Pain in Breast Cancer Survivors: An Exploratory Study on Prevalence, Characteristics, Risk Factors, and Impact on Quality of Life. Indian J. Surg. 2017, 80, 592–598. [Google Scholar] [CrossRef]
- Zou, L.; Liu, F.-H.; Shen, P.-P.; Hu, Y.; Liu, X.-Q.; Xu, Y.-Y.; Pen, Q.-L.; Wang, B.; Zhu, Y.-Q.; Tian, Y. The incidence and risk factors of related lymphedema for breast cancer survivors post-operation: A 2-year follow-up prospective cohort study. Breast Cancer 2018, 25, 309–314. [Google Scholar] [CrossRef]
- Rafn, B.S.; Hung, S.; Hoens, A.M.; McNeely, M.L.; Singh, C.A.; Kwan, W.; Dingee, C.; McKevitt, E.C.; Kuusk, U.; Pao, J.; et al. Prospective surveillance and targeted physiotherapy for arm morbidity after breast cancer surgery: A pilot randomized controlled trial. Clin. Rehabil. 2018, 32, 811–826. [Google Scholar] [CrossRef]
- Crosbie, J.; Kilbreath, S.L.; Dylke, E.; Refshauge, K.M.; Nicholson, L.L.; Beith, J.M.; Spillane, A.J.; White, K. Effects of Mastectomy on Shoulder and Spinal Kinematics During Bilateral Upper-Limb Movement. Phys. Ther. 2010, 90, 679–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribeiro, I.; Camargo, P.; Alburquerque-Sendín, F.; Ferrari, A.V.; Arrais, C.L.; Salvini, T.F. Three-dimensional scapular kinematics, shoulder outcome measures and quality of life following treatment for breast cancer—A case control study. Musculoskelet. Sci. Pract. 2019, 40, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Brookham, R.L.; Cudlip, A.C.; Dickerson, C.R. Examining upper limb kinematics and dysfunction of breast cancer survivors in functional dynamic tasks. Clin. Biomech. 2018, 55, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Lang, A.E.; Dickerson, C.R.; Kim, S.Y.; Stobart, J.; Milosavljevic, S. Impingement pain affects kinematics of breast cancer survivors in work-related functional tasks. Clin. Biomech. 2019, 70, 223–230. [Google Scholar] [CrossRef]
- Lu, T.-W.; Chang, C.-F. Biomechanics of human movement and its clinical applications. Kaohsiung J. Med Sci. 2012, 28, S13–S25. [Google Scholar] [CrossRef]
- Carnevale, A.; Longo, U.G.; Schena, E.; Massaroni, C.; Presti, D.L.; Berton, A.; Candela, V.; Denaro, V. Wearable systems for shoulder kinematics assessment: A systematic review. BMC Musculoskelet. Disord. 2019, 20, 546. [Google Scholar] [CrossRef]
- García González, S.B. Análisis biomecánico de alteraciones en cintura escapular posterior al tratamiento fisioterapéutico en pacientes mastectomizadas. Bachelor’s Thesis, UNAM, Escuela Nacional de Estudios Superiores, Unidad León, México, 2019. [Google Scholar]
- Min, J.; Kim, J.; Yeon, S.; Ryu, J.; Min, J.; Park, S.; Kim, S.; Jeon, J. Change in Shoulder Function in the Early Recovery Phase after Breast Cancer Surgery: A Prospective Observational Study. J. Clin. Med. 2021, 10, 3416. [Google Scholar] [CrossRef]
- Flores, A.M.; Dwyer, K. Shoulder Impairment Before Breast Cancer Surgery. J. Women’s Health Phys. Ther. 2014, 38, 118–124. [Google Scholar] [CrossRef] [Green Version]
- Borstad, J.D.; Szucs, K.A. Three-dimensional scapula kinematics and shoulder function examined before and after surgical treatment for breast cancer. Hum. Mov. Sci. 2011, 31, 408–418. [Google Scholar] [CrossRef]
- De Groef, A.; Van Kampen, M.; Dieltjens, E.; Christiaens, M.-R.; Neven, P.; Geraerts, I.; Devoogdt, N. Effectiveness of Postoperative Physical Therapy for Upper-Limb Impairments After Breast Cancer Treatment: A Systematic Review. Arch. Phys. Med. Rehabil. 2015, 96, 1140–1153. [Google Scholar] [CrossRef]
- Lahart, I.M.; Metsios, G.S.; Nevill, A.M.; Carmichael, A.R. Physical activity for women with breast cancer after adjuvant therapy. Cochrane Database Syst. Rev. 2014, 1, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Fretta, T.D.B.; Boing, L.; Leite, B.; Vieira, M.D.C.S.; Moratelli, J.; Klen, J.A.; Campeiz, E.; Machado, Z.; Guimarães, A.C.D.A. Funcionalidade do Membro Superior após a Cirurgia do Câncer de Mama em Sobreviventes do Sul do Brasil: Estudo de Corte Transversal. Rev. Bras. Cancerol. 2021, 67, e021168. [Google Scholar] [CrossRef]
- Śliwiński, M.; Wąż, P.; Zaręba, W.; Hansdorfer-Korzon, R. Motor Control Evaluation as a Significant Component in Upper Limb Function Assessment in Female Breast Cancer Patients after Mastectomy. Healthcare 2021, 9, 973. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klassen, O.; Schmidt, M.E.; Ulrich, C.M.; Schneeweiss, A.; Potthoff, K.; Steindorf, K.; Wiskemann, J. Muscle strength in breast cancer patients receiving different treatment regimes. J. Cachexia Sarcopenia Muscle 2016, 8, 305–316. [Google Scholar] [CrossRef]
- Testa, A.; Iannace, C.; Di Libero, L.; Caracciolo, F. Strengths of early physical rehabilitation programs in surgical breast cancer patients: Results of a randomized control study. BMC Proc. 2013, 7, O5. [Google Scholar] [CrossRef] [Green Version]
- Neto, C.; Pezarat, P.; Oliveira, R. Effects of Breast Cancer Treatment on Shoulder Function: What to Expect and How to Treat? Int. J. Phys. Ther. Rehabil. 2018, 4, 1–4. [Google Scholar] [CrossRef]
- Kilbreath, S.L.; Refshauge, K.; Beith, J.; Ward, L.; Lee, M.; Simpson, J.M.; Hansen, R. Upper limb progressive resistance training and stretching exercises following surgery for early breast cancer: A randomized controlled trial. Breast Cancer Res. Treat. 2012, 133, 667–676. [Google Scholar] [CrossRef]
- Volaklis, K.A.; Halle, M.; Tokmakidis, S.P. Exercise in the prevention and rehabilitation of breast cancer. Wien. Klin. Wochenschr. 2013, 125, 297–301. [Google Scholar] [CrossRef]
- Cheville, A.L.; Tchou, J. Barriers to rehabilitation following surgery for primary breast cancer. J. Surg. Oncol. 2007, 95, 409–418. [Google Scholar] [CrossRef]
- Lee, C.H.; Chung, S.Y.; Kim, W.Y.; Yang, S.N. Effect of breast cancer surgery on chest tightness and upper limb dysfunction. Medicine 2019, 98, e15524. [Google Scholar] [CrossRef] [PubMed]
- Shamley, D.; Aguirrebeña, I.L.; Oskrochi, R.; Srinaganathan, R. Shoulder morbidity after treatment for breast cancer is bilateral and greater after mastectomy. Acta Oncol. 2012, 51, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Balak, F.; Roelen, C.A.M.; Koopmans, P.C.; Berge, E.E.T.; Groothoff, J.W. Return to Work After Early-stage Breast Cancer: A Cohort Study into the Effects of Treatment and Cancer-related Symptoms. J. Occup. Rehabil. 2008, 18, 267–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saini, S.K.; Prakash, K.; Pugazhendi, S. Effectiveness of yoga on quality of life of breast cancer patients undergoing chemotherapy: A randomized clinical controlled study. Indian J. Palliat. Care 2020, 26, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-J.; Chan, Y.-N.; Jheng, Y.-W.; Wu, C.-J.; Lin, M.-W.; Tseng, L.-M.; Tsai, Y.-F.; Liu, L.-C. Chemotherapy-induced peripheral neuropathy in newly diagnosed breast cancer survivors treated with taxane: A prospective longitudinal study. Support. Care Cancer 2020, 29, 2959–2971. [Google Scholar] [CrossRef]
- Binotto, M.; Reinert, T.; Werutsky, G.; Zaffaroni, F.; Schwartsmann, G. Health-related quality of life before and during chemotherapy in patients with early-stage breast cancer. Ecancermedicalscience 2020, 14, 1007. [Google Scholar] [CrossRef] [Green Version]
- Reynoso-Noverón, N.; Villarreal-Garza, C.; Soto-Perez-De-Celis, E.; Arce-Salinas, C.; Matus-Santos, J.; Ramírez-Ugalde, M.T.; Alvarado-Miranda, A.; Cabrera-Galeana, P.; Meneses-García, A.; Lara-Medina, F.; et al. Clinical and Epidemiological Profile of Breast Cancer in Mexico: Results of the Seguro Popular. J. Glob. Oncol. 2017, 3, 757–764. [Google Scholar] [CrossRef]
- Maffuz-Aziz, A.; Labastida-Almendaro, S.; Espejo-Fonseca, A.; Rodriguez-Cuevas, S. Clinical and pathological features of breast cancer in a population of Mexico. Cirugía Y Cir. 2017, 85, 201–207. [Google Scholar] [CrossRef] [Green Version]
- Bertehelli Cardona, I.; Ángeles Casas, M.; Mejía Miranda, N.; Ángeles, J.M. Obesity in women with breast cancer at a general hospital in Hidalgo, Mexico. Atención Fam. 2017, 25, 3–6. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Anthropometric Data | Measurement Mean ± Std | Clinical Data | Measurement n (%) |
|---|---|---|---|
| Age (years) | 46.7 ± 8.2 | Stage cancer I and II | 8 (53.3%) |
| Body weight (kg) | 68.4 ± 7.2 | Stage cancer III | 7 (46.7%) |
| Height (cm) | 156.9 ± 5.1 | Chemotherapy (yes) | 8 (53.3%) |
| Body mass index BMI (kg/m2) | 27.8 ± 3.1 | Axillary lymph node dissection (yes) | 11 (73.3%) |
| Range of Motion (Degrees) | Patients with Chemotherapy Treatment (n = 8) | Patients without Chemotherapy Treatment (n = 7) | p-Value |
|---|---|---|---|
| Flexion–extension Mean ± std | 92.0 ± 8.5 | 113.5 ± 11.3 | 0.001 * |
| Abduction–adduction Median (Q1–Q3) | 101.2 (70.7–103.7) | 114.8 (103.3–126.7) | 0.015 ** |
| Group | Movement | Before (Degrees) | After (Degrees) | p-Value |
|---|---|---|---|---|
| 1 | Flexion–extension Mean ± std | 113.5 ± 11.3 | 107.3 ± 15.4 | 0.384 * |
| 2 | Flexion–extension Mean ± std | 92.0 ± 8.5 | 84.7 ± 11.3 | 0.243 * |
| 1 | Abduction–adduction Median (Q1–Q3) | 114.8 (103.3–126.7) | 108.4 (94.3–117.4) | 0.233 ** |
| 2 | Abduction–adduction Median (Q1–Q3) | 101.2 (77.8–103.7) | 87.6 (68.3–99.8) | 0.176 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-González, S.B.; Huerta-Franco, M.R.; Miguel-Andrés, I.; de Jesús Mayagoitia-Vázquez, J.; León-Rodríguez, M.; Barrera-Beltrán, K.; Espinoza-Macías, G. Differences in the Glenohumeral Joint before and after Unilateral Breast Cancer Surgery: Motion Capture Analysis. Healthcare 2022, 10, 707. https://doi.org/10.3390/healthcare10040707
García-González SB, Huerta-Franco MR, Miguel-Andrés I, de Jesús Mayagoitia-Vázquez J, León-Rodríguez M, Barrera-Beltrán K, Espinoza-Macías G. Differences in the Glenohumeral Joint before and after Unilateral Breast Cancer Surgery: Motion Capture Analysis. Healthcare. 2022; 10(4):707. https://doi.org/10.3390/healthcare10040707
Chicago/Turabian StyleGarcía-González, Silvia Beatríz, María Raquel Huerta-Franco, Israel Miguel-Andrés, José de Jesús Mayagoitia-Vázquez, Miguel León-Rodríguez, Karla Barrera-Beltrán, and Gilberto Espinoza-Macías. 2022. "Differences in the Glenohumeral Joint before and after Unilateral Breast Cancer Surgery: Motion Capture Analysis" Healthcare 10, no. 4: 707. https://doi.org/10.3390/healthcare10040707
APA StyleGarcía-González, S. B., Huerta-Franco, M. R., Miguel-Andrés, I., de Jesús Mayagoitia-Vázquez, J., León-Rodríguez, M., Barrera-Beltrán, K., & Espinoza-Macías, G. (2022). Differences in the Glenohumeral Joint before and after Unilateral Breast Cancer Surgery: Motion Capture Analysis. Healthcare, 10(4), 707. https://doi.org/10.3390/healthcare10040707