
Effect of Serial Home-Based Exercise Immediately after Latissimus Dorsi Reconstruction in Patients with Breast Cancer

Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Breast Reconstruction Using Latissimus Dorsi Flap
2.3. Serial Home-Based Exercise Program
2.4. Functional Assessments
2.4.1. Active Range of Motion in the Shoulder Joint
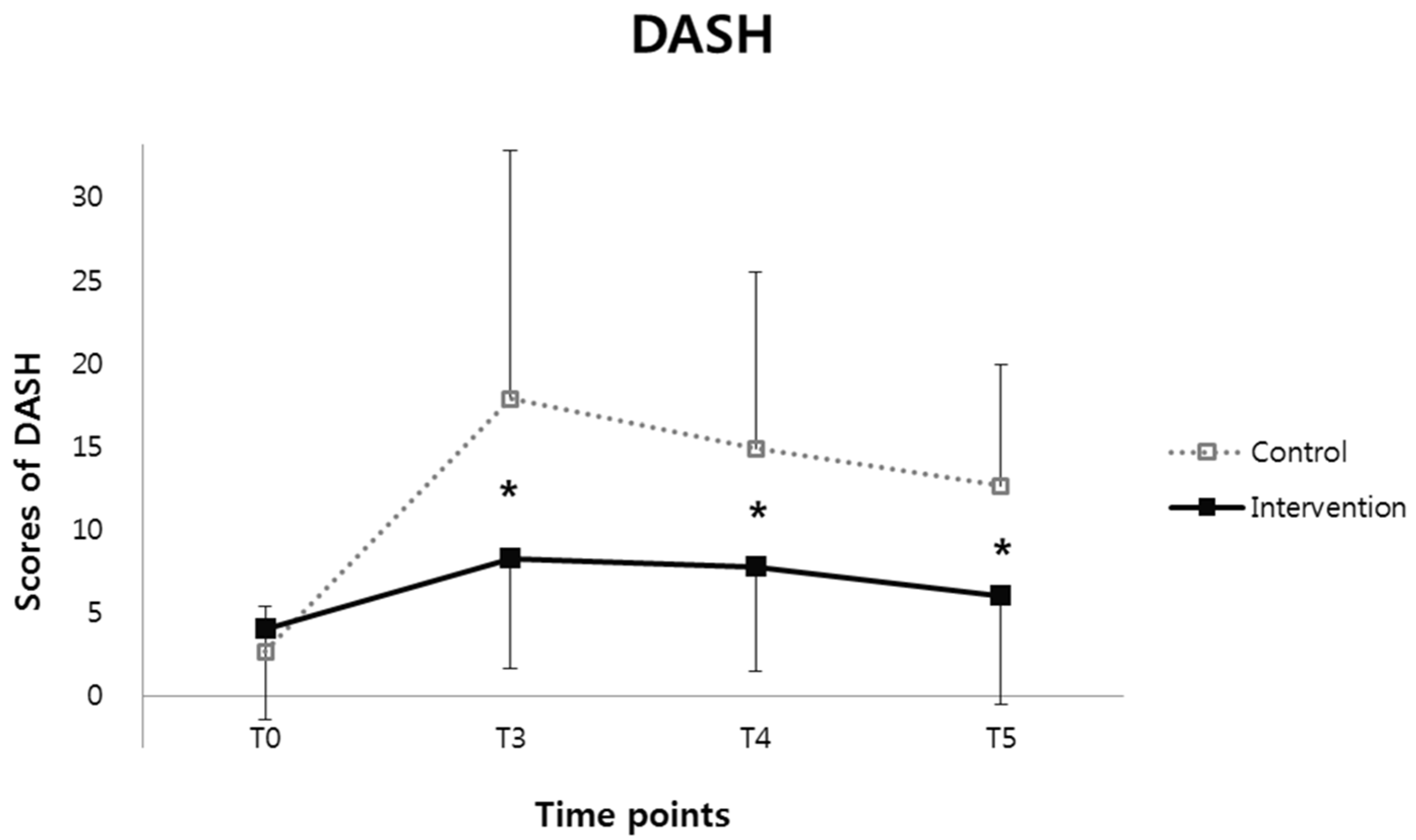
2.4.2. Disability of the Upper Extremity
2.4.3. Quality of Life Using the 36-Item Short-Form Health Survey
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Ghazal, S.; Fallowfield, L.; Blamey, R. Comparison of psychological aspects and patient satisfaction following breast conserving surgery, simple mastectomy and breast reconstruction. Eur. J. Cancer 2000, 36, 1938–1943. [Google Scholar] [CrossRef]
- Chang, D.W.; Youssef, A.; Cha, S.; Reece, G.P. Autologous breast reconstruction with the extended latissimus dorsi flap. Plast. Reconstr. Surg. 2002, 110, 751–759; discussion 760. [Google Scholar] [CrossRef] [PubMed]
- Steffenssen, M.C.; Kristiansen, A.-L.H.; Damsgaard, T.E. A systematic review and meta-analysis of functional shoulder impairment after latissimus dorsi breast reconstruction. Ann. Plast. Surg. 2019, 82, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.L. Functional morbidity following latissimus dorsi flap breast reconstruction. J. Adv. Pract. Oncol. 2014, 5, 181. [Google Scholar] [PubMed]
- Blackburn, N.E.; Mc Veigh, J.G.; Mc Caughan, E.; Wilson, I.M. The musculoskeletal consequences of breast reconstruction using the latissimus dorsi muscle for women following mastectomy for breast cancer: A critical review. Eur. J. Cancer Care (Engl.) 2018, 27, e12664. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Huh, J.S.; Min, Y.-S.; Kim, H.J.; Park, H.Y.; Jung, T.-D. Physical and functional ability recovery patterns and quality of life after immediate autologous latissimus dorsi breast reconstruction: A 1-year prospective observational study. Plast. Reconstr. Surg. 2015, 136, 1146–1154. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, R.R.; do Nascimento, S.L.; Derchain, S.F.; Sarian, L.O. Immediate breast reconstruction with a latissimus dorsi flap has no detrimental effects on shoulder motion or postsurgical complications up to 1 year after surgery. Plast. Reconstr. Surg. 2013, 131, 673e–680e. [Google Scholar] [CrossRef] [PubMed]
- Button, J.; Scott, J.; Taghizadeh, R.; Weiler-Mithoff, E.; Hart, A.M. Shoulder function following autologous latissimus dorsi breast reconstruction. A prospective three year observational study comparing quilting and non-quilting donor site techniques. J. Plast. Reconstr. Aesthetic Surg. 2010, 63, 1505–1512. [Google Scholar] [CrossRef] [PubMed]
- Glassey, N.; Perks, G.B.; McCulley, S.J. A prospective assessment of shoulder morbidity and recovery time scales following latissimus dorsi breast reconstruction. Plast. Reconstr. Surg. 2008, 122, 1334–1340. [Google Scholar] [CrossRef]
- Cifu, D.X. Braddom’s Physical Medicine and Rehabilitation—5th Edition; Elsevier: Singapore, 2015; Volume I. [Google Scholar]
- Lee, J.-Y.; Lim, J.-Y.; Oh, J.H.; Ko, Y.-M. Cross-cultural adaptation and clinical evaluation of a Korean version of the disabilities of arm, shoulder, and hand outcome questionnaire (K-DASH). J. Shoulder Elb. Surg. 2008, 17, 570–574. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Han, C.-W.; Lee, E.-J.; Iwaya, T.; Kataoka, H.; Kohzuki, M. Development of the Korean version of Short-Form 36-Item Health Survey: Health related QOL of healthy elderly people and elderly patients in Korea. Tohoku J. Exp. Med. 2004, 203, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Spear, S.L.; Hess, C.L. A review of the biomechanical and functional changes in the shoulder following transfer of the latissimus dorsi muscles. Plast. Reconstr. Surg. 2005, 115, 2070–2073. [Google Scholar] [CrossRef] [PubMed]
- Forthomme, B.; Heymans, O.; Jacquemin, D.; Klinkenberg, S.; Hoffmann, S.; Grandjean, F.-X.; Crielaard, J.-M.; Croisier, J.-L. Shoulder function after latissimus dorsi transfer in breast reconstruction. Clin. Physiol. Funct. Imaging 2010, 30, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Garusi, C.; Manconi, A.; Lanni, G.; Lomeo, G.; Loschi, P.; Simoncini, M.; Santoro, L.; Rietjens, M.; Petit, J. Shoulder function after breast reconstruction with the latissimus dorsi flap: A prospective cohort study–Combining DASH score and objective evaluation. Breast 2016, 27, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Burgess, C.; Cornelius, V.; Love, S.; Graham, J.; Richards, M.; Ramirez, A. Depression and anxiety in women with early breast cancer: Five year observational cohort study. BMJ 2005, 330, 702. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Control Group (N = 35) | Intervention Group (N = 45) | p Value | |
|---|---|---|---|
| Age, years, mean ± SD | 43.6 ± 5.9 | 46.0 ± 6.0 | 0.077 |
| Breast cancer | |||
| Tumor location, N (%) | 0.222 | ||
| Right | 18 (51.4) | 17 (37.8) | |
| Left | 17 (48.6) | 28 (62.2) | |
| Tumor type, N (%) | 0.225 | ||
| DCIS | 6 (17.1) | 15 (33.3) | |
| ILC | 1 (2.9) | 2 (4.5) | |
| IDC | 28 (80.0) | 28 (62.2) | |
| Cancer stage, N (%) | 0.521 | ||
| Stage 0 | 3 (8.6) | 7 (15.6) | |
| Stage I | 14 (40.0) | 19 (42.2) | |
| Stage II | 17 (48.6) | 19 (42.2) | |
| Stage III | 1 (2.8) | 0 (0.0) | |
| Lymph node dissection, N (%) | 0.050 | ||
| SLNB | 24 (68.6) | 39 (86.7) | |
| ALND | 11 (31.4) | 6 (13.3) | |
| Adjuvant chemotherapy, N (%) | 27 (77.1) | 27 (60.0) | 0.104 |
| Adjuvant radiotherapy, N (%) | 15 (42.9) | 28 (62.2) | 0.085 |
| Adjuvant hormone therapy, N (%) | 0.604 | ||
| Tamoxifen | 27 (77.1) | 36 (80.0) | |
| Letrozole | 5 (14.3) | 3 (6.7) |
| Control Group | Intervention Group | p Value | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T3 | T4 | T5 | T0 | T1 | T2 | T3 | T4 | T5 | ||
| Flexion | 179.0 ± 2.4 | 141.7 ± 22.7 | 162.2 ± 13.7 | 171.3 ± 7.2 | 177.7 ± 3.4 | 177.4 ± 5.6 | 178.3 ± 9.0 | 156.3 ± 22.2 | 170.9 ± 12.7 † | 175.2 ± 10.3 | 175.0 ± 14.4 | 179.2 ± 2.2 | 0.043 * |
| Abduction | 178.8 ± 2.8 | 142.4 ± 28.4 | 164.3 ± 18.3 | 172.9 ± 8.1 | 177.9 ± 3.3 | 179.2 ± 2.3 | 179.3 ± 3.3 | 150.5 ± 34.9 | 170.0 ± 16.0 | 176.4 ± 12.9 | 175.5 ± 14.8 | 179.4 ± 2.4 | 0.160 |
| Internal Rotation | 82.6 ± 9.7 | 75.5 ± 13.1 | 76.4 ± 12.2 | 80.9 ± 8.2 | 82.7 ± 8.7 | 83.8 ± 9.1 | 87.6 ± 9.0 | 76.5 ± 15.8 | 88.6 ± 6.4 † | 86.1 ± 13.0 | 84.3 ± 13.6 | 89.8 ± 0.9 † | 0.038 * |
| External Rotation | 81.7 ± 8.5 | 74.3 ± 12.7 | 76.6 ± 10.8 | 77.7 ± 10.6 | 79.0 ± 12.2 | 80.8 ± 11.7 | 86.2 ± 5.8 | 76.0 ± 15.1 | 89.8 ± 1.5 † | 89.7 ± 1.7 † | 89.5 ± 2.3 † | 88.0 ± 5.9 | 0.047 * |
| Control Group | Intervention Group | F | p Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T3 | T4 | T5 | T0 | T3 | T4 | T5 | |||
| DASH | 2.7 ± 2.7 | 17.8 ± 14.9 | 14.8 ± 10.6 | 12.6 ± 7.3 | 4.0 ± 5.5 | 8.2 ± 6.6 † | 7.7 ± 6.3 | 6.0 ± 6.5 † | 5.809 | 0.005 * |
| Control Group | Intervention Group | F | p Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T3 | T4 | T5 | T0 | T3 | T4 | T5 | |||
| PF | 91.5 ± 15.4 | 84.1 ± 17.4 | 83.8 ± 13.7 | 85.5 ± 14.2 | 91.2 ± 15.1 | 83.2 ± 16.9 | 80.3 ± 18.6 | 86.9 ± 15.5 | 1.769 | 0.174 |
| RP | 67.4 ± 39.5 | 48.9 ± 45.3 | 58.3 ± 37.4 | 76.3 ± 36.8 | 81.7 ± 30.8 | 61.8 ± 38.6 † | 62.5 ± 39.7 † | 75.0 ± 33.3 | 3.064 | 0.032 * |
| BP | 78.2 ± 18.0 | 77.3 ± 16.1 | 75.8 ± 16.4 | 82.3 ± 15.3 | 83.1 ± 15.3 | 72.6 ± 13.6 | 74.3 ± 19.3 | 81.9 ± 18.3 | 0.653 | 0.583 |
| GH | 59.6 ± 22.8 | 68.6 ± 13.2 | 61.5 ± 19.3 | 63.7 ± 21.3 | 62.1 ± 15.5 | 50.2 ± 22.5 | 56.6 ± 18.4 | 64.0 ± 18.2 | 0.136 | 0.938 |
| PCS | 50.6 ± 8.0 | 46.9 ± 8.3 | 46.8 ± 7.6 | 48.9 ± 6.6 | 51.9 ± 6.3 | 46.6 ± 6.1 | 46.1 ± 8.0 | 49.8 ± 7.1 | 0.516 | 0.672 |
| VT | 55.2 ± 18.6 | 57.7 ± 21.9 | 55.7 ± 16.0 | 61.8 ± 18.6 | 53.1 ± 18.1 | 62.8 ± 16.2 † | 56.1 ± 15.9 | 60.2 ± 17.6 | 3.128 | 0.029 * |
| SF | 81.5 ± 22.9 | 80.7 ± 18.8 | 77.4 ± 21.1 | 84.9 ± 18.9 | 88.3 ± 18.2 | 82.0 ± 16.9 | 79.3 ± 16.8 | 90.7 ± 16.1 | 0.204 | 0.894 |
| RE | 69.6 ± 41.3 | 62.1 ± 45.2 | 69.8 ± 37.9 | 78.9 ± 38.8 | 77.0 ± 34.7 | 65.7 ± 43.0 | 64.0 ± 41.3 | 75.3 ± 35.3 | 1.209 | 0.311 |
| MH | 60.2 ± 17.8 | 63.6 ± 19.3 | 68.4 ± 16.4 | 74.3 ± 17.6 | 64.0 ± 20.3 | 72.6 ± 15.9 † | 68.8 ± 15.2 | 71.1 ± 17.6 | 2.927 | 0.049 * |
| MCS | 39.8 ± 11.1 | 41.4 ± 11.4 | 42.9 ± 10.3 | 46.3 ± 10.8 | 41.9 ± 11.3 | 44.8 ± 10.1 | 42.8 ± 8.2 | 45.4 ± 9.6 | 1.150 | 0.333 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, E.; Lee, J.S.; Park, H.Y.; Yang, J.D.; Jung, T.-D. Effect of Serial Home-Based Exercise Immediately after Latissimus Dorsi Reconstruction in Patients with Breast Cancer. Healthcare 2022, 10, 1760. https://doi.org/10.3390/healthcare10091760
Park E, Lee JS, Park HY, Yang JD, Jung T-D. Effect of Serial Home-Based Exercise Immediately after Latissimus Dorsi Reconstruction in Patients with Breast Cancer. Healthcare. 2022; 10(9):1760. https://doi.org/10.3390/healthcare10091760
Chicago/Turabian StylePark, Eunhee, Joon Seok Lee, Ho Yong Park, Jung Dug Yang, and Tae-Du Jung. 2022. "Effect of Serial Home-Based Exercise Immediately after Latissimus Dorsi Reconstruction in Patients with Breast Cancer" Healthcare 10, no. 9: 1760. https://doi.org/10.3390/healthcare10091760
APA StylePark, E., Lee, J. S., Park, H. Y., Yang, J. D., & Jung, T.-D. (2022). Effect of Serial Home-Based Exercise Immediately after Latissimus Dorsi Reconstruction in Patients with Breast Cancer. Healthcare, 10(9), 1760. https://doi.org/10.3390/healthcare10091760