Effectiveness of an Advanced Clinical Decision Support System on Clinical Decision-Making Skills in a Call Center Medication Therapy Management Pharmacy Setting: A Pilot Study





Abstract
1. Introduction
2. Materials and Methods
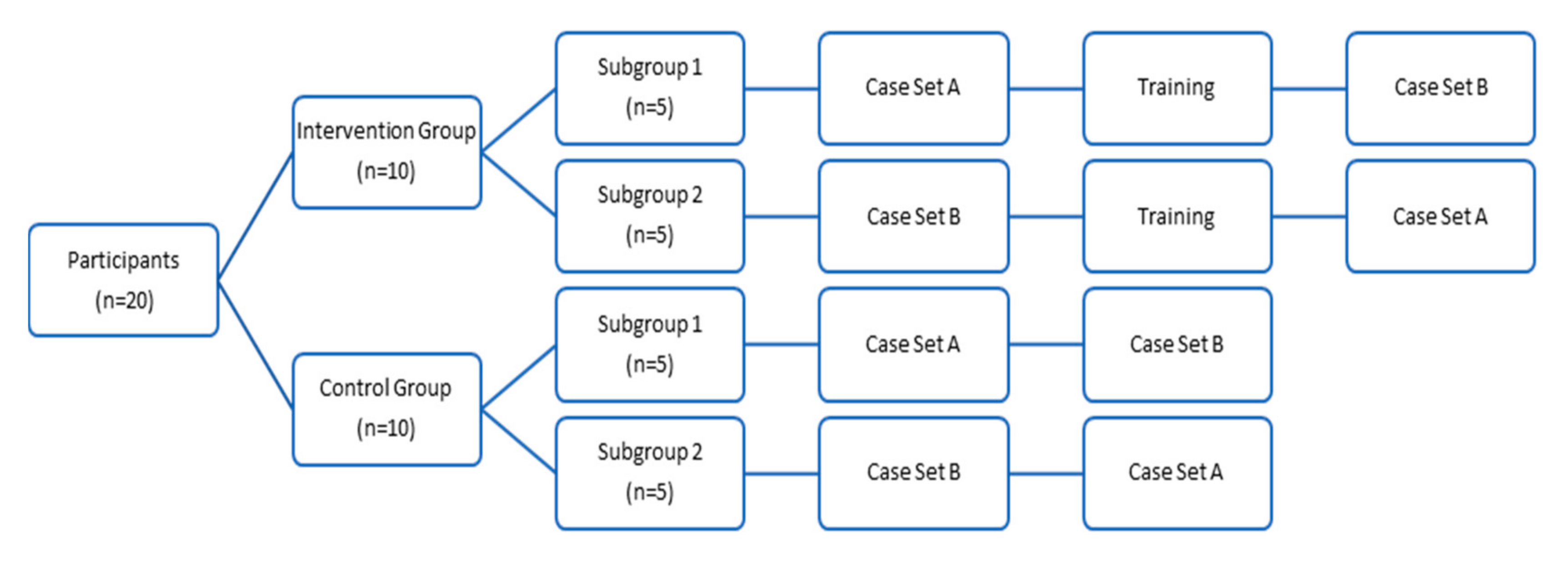
2.1. Study Design
2.2. Study Participants and Site
2.3. Study Recruitment and Enrollment
2.4. Clinical Skills Assessment
2.5. Intervention
2.6. Data Collection
2.6.1. Intervention Group
2.6.2. Control Group
2.7. Data Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A: Clinical Assessment Case Set A
- 1.
- Your patient is a 76 y/o Male with NKDA. SCr 0.98, Height 6′1”, Weight 251 lb. Past medical history includes: coronary artery disease, anxiety disorder, gout, hyperlipidemia, insomnia, low testosterone, sleep apnea, vitamin D deficiency.
- He is taking:Allopurinol 300 mg 2 tabs PO qAMAspirin 325 mg PO qAMBupropion XL 150 mg PO qAMClopidogrel 75 mg PO qAMEscitalopram 20 mg PO qAMMetoprolol Tartrate 25 mg PO BIDOmega 3 (strength unknown) 1 PO BIDOxycodone-Acetaminophen 5–325 mg PO q4h prnRosuvastatin 40 mg PO qAMZolpidem 10 mg PO qHS
- □
- Recommendation to change medication
- □
- Recommendation to decrease medication dose
- □
- Recommendation to increase medication dose
- □
- Recommendation to change medication timing of administration
- □
- Recommendation to start medication
- □
- Recommendation to discontinue medication
- □
- Recommendation to start monitoring
- 2.
- Your patient (age and gender unknown) has the following labs: Mg 2.0, K 4.4. Allergic to penicillin. Past medical history includes: atrial flutter with rapid ventricular response, coronary artery disease status post stent, deep vein thrombosis, hypertension, hypothyroidism.
- They are taking:Lisinopril 10 mg PO qAMLoratadine 10 mg PO qAMLevothyroxine 88 mcg PO qAMMetoprolol ER 50 mg PO qAMWarfarin 2.5 mg PO qAMSertraline 25 mg PO qAMVenlafaxine ER 150 mg PO qAMVitamin D 1000 international units PO qAMPantoprazole 40 mg PO qAMAtorvastatin 40 mg PO qAMClopidogrel 75 mg PO qAMFerrous sulfate 325 mg PO qAMPotassium chloride 20 meq PO qAMAmiodarone 400 mg PO BIDDigoxin 125 mcg PO qAM
- □
- Recommendation to change medication
- □
- Recommendation to decrease medication dose
- □
- Recommendation to increase medication dose
- □
- Recommendation to change medication timing of administration
- □
- Recommendation to start medication
- □
- Recommendation to discontinue medication
- □
- Recommendation to start monitoring
- 3.
- Your patient is a 73 y/o female that is allergic to alprazolam. Labs = Mg 2.0, K 4.4. Past medical history includes: Trigeminal neuralgia, major depressive disorder, chronic obstructive pulmonary disease (stage 3) with multiple hospital admissions, history of SIADH.
- She is taking:Aspirin 81 mg PO qAMCalcichew PO qAMLisinopril 20 mg PO qAMCarbamazepine 200 mg PO qAMTerazosin 4 mg PO qAMZolpidem 10 mg PO qHS prnMirtazapine 30 mg PO qHS + 7.5 mg PO qHS prnFamotidine 20 mg PO BIDSenna 8.6 mg PO BIDAmlodipine 10 mg PO qAMPregabalin 75 mg PO BIDAlbuterol Inhale 2 puffs PO 5 times daily +4 puffs q4h prnTiotropium Respimat 2 puffs PO daily
- □
- Recommendation to change medication
- □
- Recommendation to decrease medication dose
- □
- Recommendation to increase medication dose
- □
- Recommendation to change medication timing of administration
- □
- Recommendation to start medication
- □
- Recommendation to discontinue medication
- □
- Recommendation to start monitoring
Appendix B: Clinical Assessment Case Set B
- 1.
- Your patient is an 82-year-old male that is allergic to dye. His Scr is 1.1, Height 5’2”, 190 lb. Past medical history includes: STEMI 2016, chronic stable angina, chronic low back pain, BPH, GERD, hypothyroidism.
- He is taking:Acetaminophen 500 mg PO TIDAspirin 81 mg PO qAMAtorvastatin 40 mg PO qHSCalcium carbonate 600 mg PO BIDCholecalciferol 1000 unit PO qAMClopidogrel 75 mg tablet PO qAMDocusate sodium 100 mg PO qAMEsomeprazole 40 mg PO qAMFamotidine 10 mg PO qAMFerrous sulfate 325 mg PO BIDFinasteride 5 mg PO qAMIsosorbide mononitrate ER 30 mg PO qAMLevothyroxine 112 mcg PO qAMMetoprolol tartrate 25 mg PO BIDOxycodone-acetaminophen 7.5 mg/325 mg PO TID prnPolyethylene glycol 3350 17 g/dose PO qAMTamsulosin 0.4 mg PO qAM
- □
- Recommendation to change medication
- □
- Recommendation to decrease medication dose
- □
- Recommendation to increase medication dose
- □
- Recommendation to change medication timing of administration
- □
- Recommendation to start medication
- □
- Recommendation to discontinue medication
- □
- Recommendation to start monitoring
- 2.
- Your patient is a 63 y/o female with NKDA. No recent labs. Her past medical history includes: hypertension, hyperlipidemia, diabetes mellitus, peripheral neuropathy, essential tremor, depression, anxiety, history cardiovascular accident, carotid stenosis, irritable bowel syndrome, history of falls.
- She is taking:Acetaminophen 325 mg tablet 2 PO q6h prn painAspirin 81 mg, delayed release PO qAMClopidogrel 75 mg PO qAMFluoxetine 20 mg PO qAMFolic acid 1 mg PO qAMGabapentin 300 mg PO qAMLisinopril 5 mg PO qAMLoperamide 2 mg PO daily prn, up to 2 tabs per dayMelatonin 3 mg tablet PO qHSMetformin 500 mg PO BID with mealsMirtazapine 7.5 mg PO qHS prnPantoprazole 40 mg, delayed release PO qAMPropranolol 60 mg tablet 1.5 PO BIDThiamine HCl 100 mg PO qAM
- □
- Recommendation to change medication
- □
- Recommendation to decrease medication dose
- □
- Recommendation to increase medication dose
- □
- Recommendation to change medication timing of administration
- □
- Recommendation to start medication
- □
- Recommendation to discontinue medication
- □
- Recommendation to start monitoring
- 3.
- Your patient is an 81 y/o Female, NKDA with a past medical history of anxiety, atrial fibrillation, gastroesophageal reflux disease, essential tremors, hypertension, hypothyroidism.
- She is taking:Acetaminophen 325 mg PO TIDLactobacillus 10 billion cell PO qAMDiltiazem ER 360 mg 24 h PO qAMDulera 100 mcg-5 mcg/actuation HFA aerosol inhaler 2 puffs PO BIDDuloxetine 60 mg, delayed release PO qAMLevothyroxine 88 mcg capsule PO qAMLorazepam 0.5 mg PO TIDIpratropium-albuterol 0.5 mg–3 mg (2.5 mg base)/3 mL inhaled q6h prnPantoprazole 40 mg, delayed release PO qAMPotassium chloride ER 20 mEq, extended release PO qAMQuetiapine 25 mg PO qAMTopiramate 50 mg PO qAm
- □
- Recommendation to change medication
- □
- Recommendation to decrease medication dose
- □
- Recommendation to increase medication dose
- □
- Recommendation to change medication timing of administration
- □
- Recommendation to start medication
- □
- Recommendation to discontinue medication
- □
- Recommendation to start monitoring
References
- Doan, J.; Zakrzewski-Jakubiak, H.; Roy, J.; Turgeon, J.; Tannenbaum, C. Prevalence and Risk of Potential Cytochrome P450–Mediated Drug-Drug Interactions in Older Hospitalized Patients with Polypharmacy. Ann. Pharmacother. 2013, 47, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.; Norouzi, M.; Ashouri, A.; Javadi, M.; Gholami, K.; Hadjibabaie, M. Study of Potential Drug-Drug Interactions in Prescriptions of University-Based Pharmacies. J. Pharm. Care 2014, 2, 60–65. [Google Scholar]
- Weideman, R.A.; Bernstein, I.H.; McKinney, W.P. Pharmacist recognition of potential drug interactions. Am. J. Health Syst. Pharm. 1999, 56, 1524–1529. [Google Scholar] [CrossRef] [PubMed]
- Agency for Healthcare Research and Quality. Available online: https://www.ahrq.gov/cpi/about/otherwebsites/clinical-decision-support/index.html (accessed on 9 July 2020).
- Jia, P.; Zhang, L.; Chen, J.; Zhao, P.; Zhang, M. The Effects of Clinical Decision Support Systems on Medication Safety: An Overview. PLoS ONE 2016, 11, e0167683. [Google Scholar] [CrossRef] [PubMed]
- Turgeon, J.; Michaud, V. Clinical Decision Support Systems: Great Promises for Better Management of Patients’ Drug Therapy. Expect Opin. Drug Metab. Toxicol. 2016, 12, 993–995. [Google Scholar] [CrossRef] [PubMed]
- Zakrzewski-Jakubiak, H.; Doan, J.; Lamoureux, P.; Singh, D.; Turgeon, J.; Tannenbaum, C. Detection and prevention of drug-drug interactions in the hospitalized elderly: Utility of new cytochrome p450-based software. Am. J. Geriatr. Pharmacother. 2011, 9, 461–470. [Google Scholar] [CrossRef] [PubMed]
- US Trademark Registrations. Available online: https://uspto.report/TM/88768328 (accessed on 9 July 2020).
- Survey Monkey. Available online: https://www.surveymonkey.com/ (accessed on 23 June 2020).
- Systematized Nomenclature of Medicine—Clinical Terms. Available online: http://www.snomed.org/ (accessed on 5 March 2020).
- Bankes, D.; Jin, H.; Finnel, S.; Michaud, V.; Knowlton, C.; Turgeon, J.; Stein, A. Association of a Novel Medication Risk Score with Adverse Drug Events and Other Pertinent Outcomes Among Participants of the Programs of All-Inclusive Care for the Elderly. Pharmacy 2020, 8, 87. [Google Scholar] [CrossRef] [PubMed]
- Bain, K.; McGain, D.; Cicali, E.; Knowlton, C.; Michaud, V.; Turgeon, J. Precision medication: An illustrative case series guiding the clinical application of multi-drug interactions and pharmacogenomics. Clin. Case Rep. 2019, 8, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Fowler, S.; Morcos, P.N.; Cleary, Y.; Martin-Facklam, M.; Parrott, N.; Gertz, M.; Yu, L. Progress in Prediction and Interpretation of Clinically Relevant Metabolic Drug-Drug Interactions: A Minireview Illustrating Recent Developments and Current Opportunities. Curr. Pharmacol. Rep. 2017, 3, 36–49. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Intervention Group (n = 10) n (%) | Control Group (n = 10) n (%) |
|---|---|---|
| Age (years) | ||
| 20–30 | 8 (80) | 2 (20) |
| 31–40 | 1 (10) | 6 (60) |
| 41–50 | 0 | 1 (10) |
| 51–60 | 1 (10) | 1 (10) |
| Female gender | 5 (50) | 4 (40) |
| Pharmacy Practice Setting | ||
| Community Pharmacy | 6 (60) | 4 (40) |
| Hospital Pharmacy | 1 (10) | 0 |
| Ambulatory Care Pharmacy | 1 (10) | 6 (60) |
| Managed Care Pharmacy | 6 (60) | 1 (10) |
| Other | 3 (30) | 0 |
| Years of Experience as a Pharmacist | ||
| 0–3 | 7 (70) | 4 (40) |
| 4–6 | 1 (10) | 1 (10) |
| 7–10 | 0 | 4 (40) |
| 10 or more | 2 (20) | 1 (10) |
| Credentials | ||
| BPharm | 1 (10) | 1 (10) |
| PharmD | 9 (90) | 9 (90) |
| MPH | 1 (10) | 0 |
| Characteristic | Intervention Group (n = 10) n (%) | Control Group (n = 10) n (%) |
|---|---|---|
| “Did you find the clinical decision support system to be helpful?” | ||
| Strongly Agree | 10 (100) | N/A |
| “Would you recommend the decision support system to others?” | ||
| Strongly Agree | 10 (100) | N/A |
| “Would use of a clinical decision support system improve your quantity of clinical recommendations?” | ||
| Strongly Agree | 8 (80) | 6 (60) |
| Agree | 2 (20) | 4 (40) |
| “Would use of a clinical decision support system improve your quality of clinical recommendations?” | ||
| Strongly Agree | 10 (100) | 6 (60) |
| Agree | 0 | 4 (40) |
| “Would use of a clinical decision support system enable you to provide better patient care?” | ||
| Strongly Agree | 10 (100) | 5 (50) |
| Agree | 0 | 5 (50) |
| Pre-Test, Median (IQR) | Post-Test, Median (IQR) | p-Value | |
|---|---|---|---|
| Intervention group | 3.0 (3.0) | 6.5 (4.0) | 0.02 |
| Control group | 3.0 (2.0) | 3.5 (1.0) | 0.48 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bingham, J.M.; Michaud, V.; Turgeon, J.; Axon, D.R. Effectiveness of an Advanced Clinical Decision Support System on Clinical Decision-Making Skills in a Call Center Medication Therapy Management Pharmacy Setting: A Pilot Study. Pharmacy 2020, 8, 228. https://doi.org/10.3390/pharmacy8040228
Bingham JM, Michaud V, Turgeon J, Axon DR. Effectiveness of an Advanced Clinical Decision Support System on Clinical Decision-Making Skills in a Call Center Medication Therapy Management Pharmacy Setting: A Pilot Study. Pharmacy. 2020; 8(4):228. https://doi.org/10.3390/pharmacy8040228
Chicago/Turabian StyleBingham, Jennifer M., Veronique Michaud, Jacques Turgeon, and David R. Axon. 2020. "Effectiveness of an Advanced Clinical Decision Support System on Clinical Decision-Making Skills in a Call Center Medication Therapy Management Pharmacy Setting: A Pilot Study" Pharmacy 8, no. 4: 228. https://doi.org/10.3390/pharmacy8040228
APA StyleBingham, J. M., Michaud, V., Turgeon, J., & Axon, D. R. (2020). Effectiveness of an Advanced Clinical Decision Support System on Clinical Decision-Making Skills in a Call Center Medication Therapy Management Pharmacy Setting: A Pilot Study. Pharmacy, 8(4), 228. https://doi.org/10.3390/pharmacy8040228