Efficacy of an Objective Structured Clinical Examination Training Approach for Training Pharmacy Students in Diabetes Mellitus Counseling: A Randomized Controlled Trial

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Operational Definitions
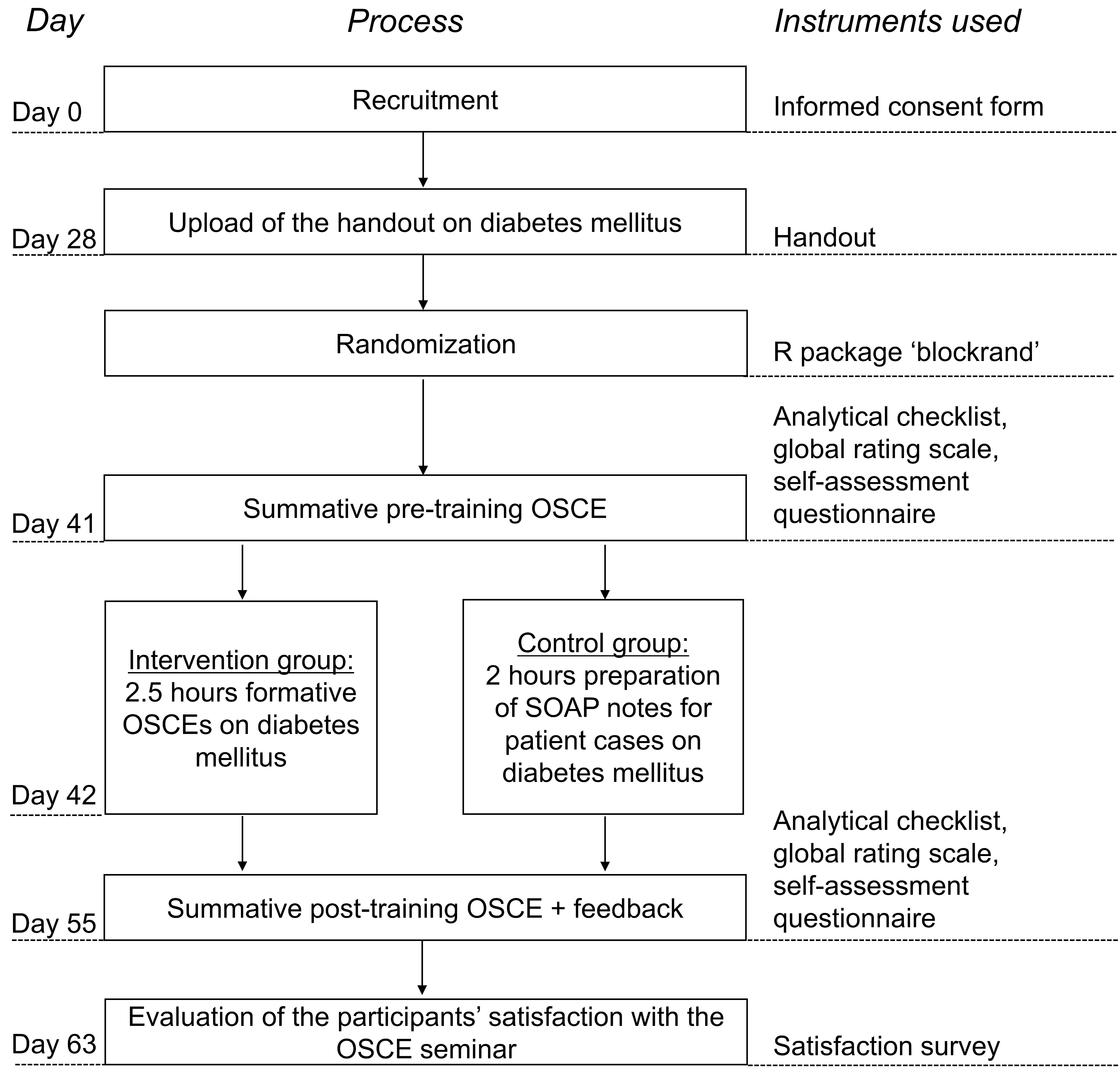
2.2. Participants and Study Design
2.3. Seminar Procedure
2.4. Instruments
2.4.1. Handout
2.4.2. OSCE Cases
2.4.3. Scoring Instruments
2.4.4. Multiple-Choice Test on Diabetes Mellitus
2.4.5. Self-Assessment Questionnaire
2.4.6. Participants’ Satisfaction Survey
2.4.7. Preparation Questionnaire
2.5. Summative OSCEs
2.6. Training for the Intervention Group
2.7. Training for the Control Group
2.8. Statistical Methods
3. Results
3.1. Participants
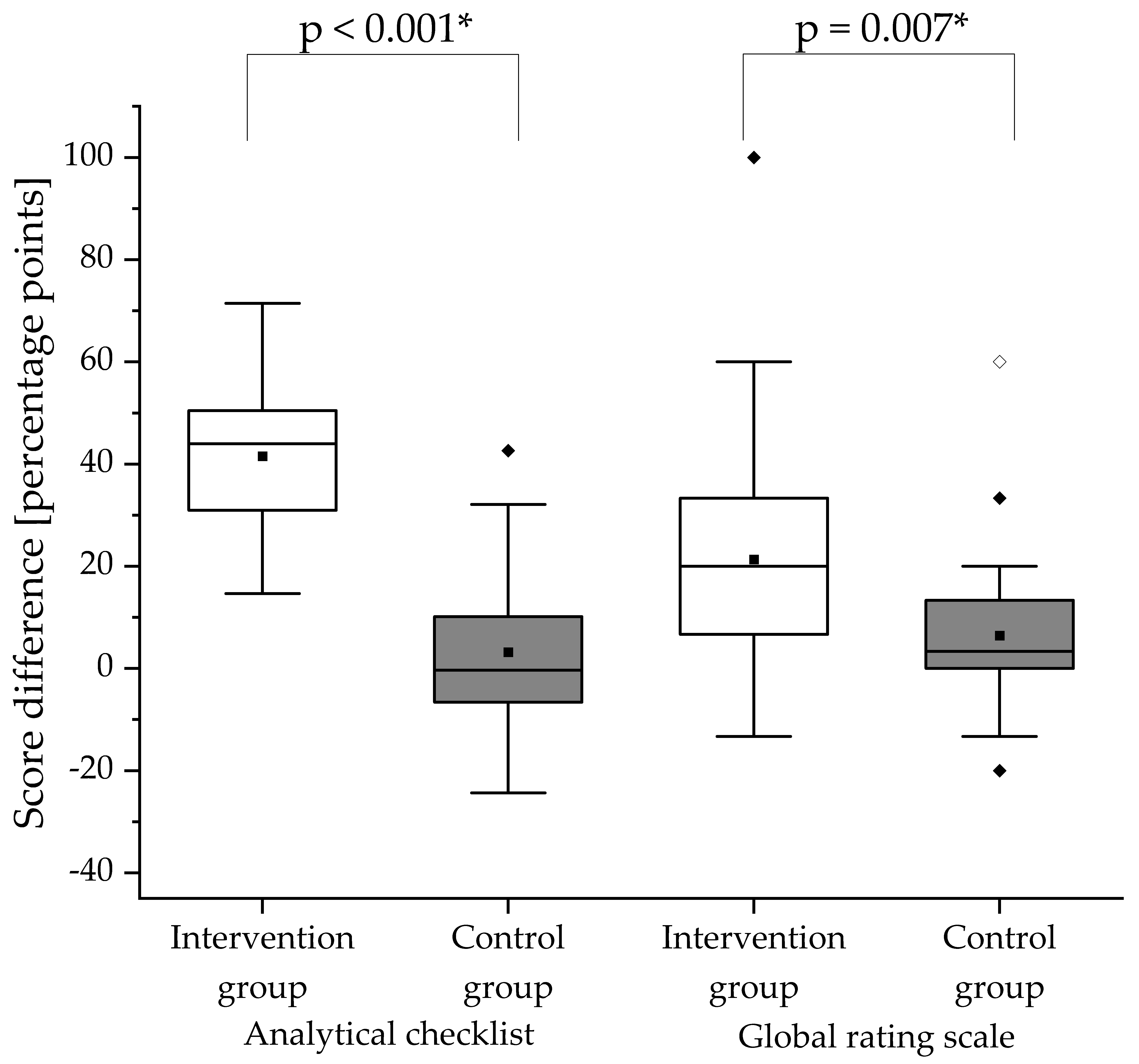
3.2. Analytical Checklists for OSCEs
3.3. Global Rating Scale
3.4. Multiple-Choice Test on Diabetes Mellitus
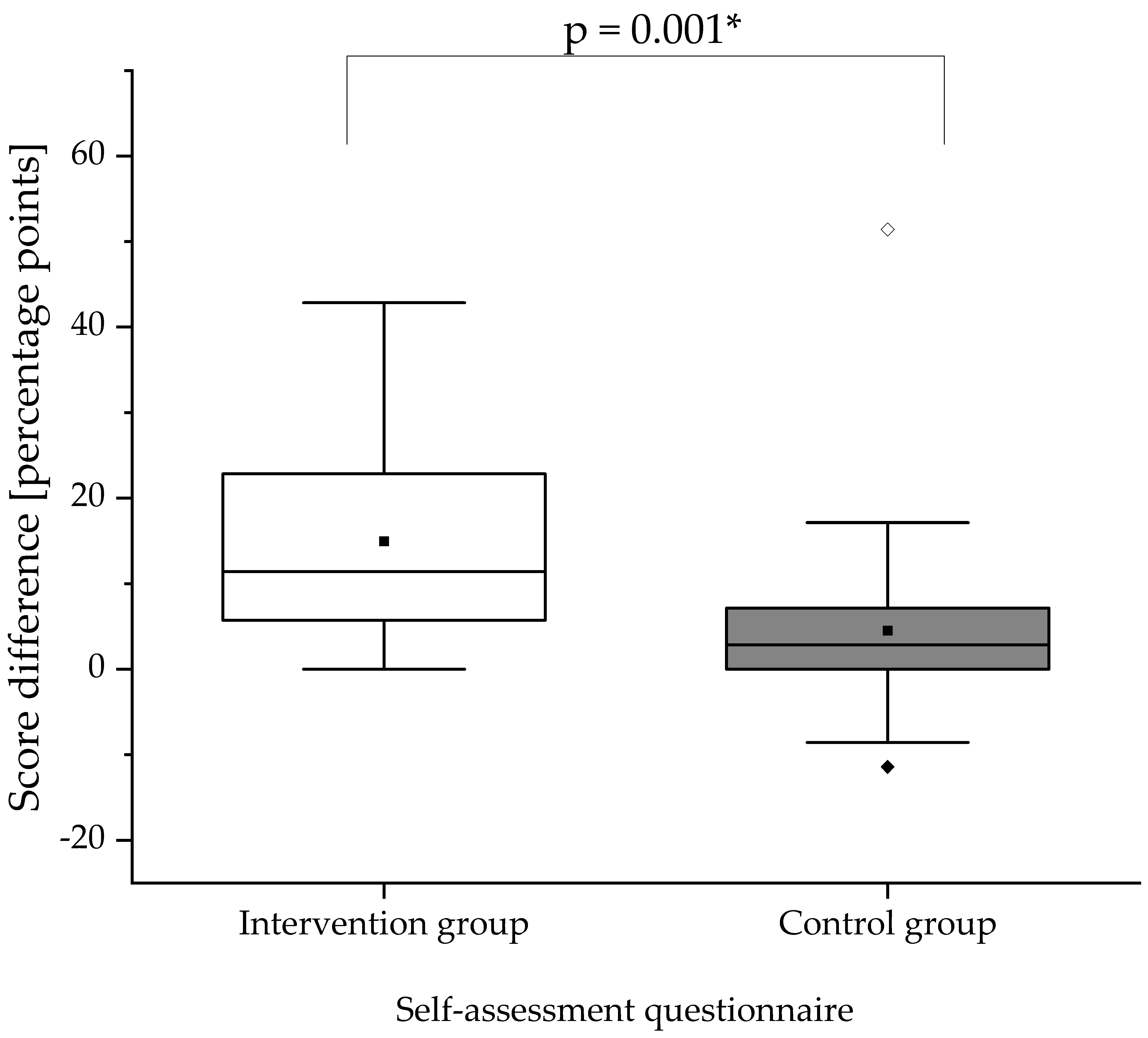
3.5. Self-Assessment Questionnaire
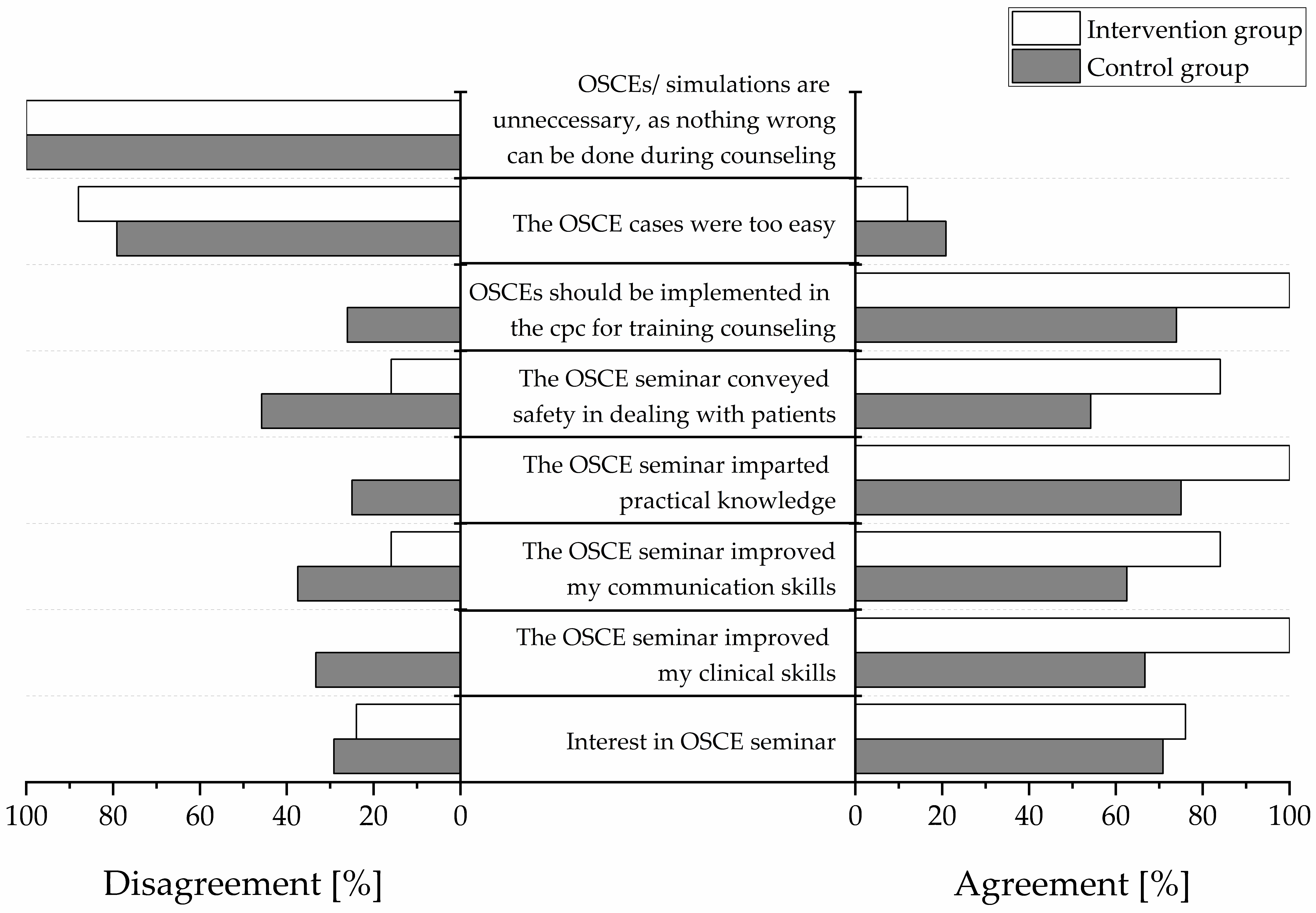
3.6. Participants’ Satisfaction
3.7. Preparation Questionnaire
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OSCE Case | Short Case Description | Number of Items in the Case |
|---|---|---|
| Summative pre-training OSCE | ||
| Case 1 | Implementation of metformin treatment
| 22 |
| Case 2 | Initiation of dapagliflozin treatment
| 27 |
| Case 3 | Implementation of sitagliptin treatment
| 22 |
| Case 4 | Initiation of acarbose treatment
| 24 |
| Case 5 | Implementation of glibenclamide treatment
| 23 |
| Case 6 | Initiation of insulin glargine treatment
| 26 |
| Summative post-training OSCE | ||
| Case 7 | Initiation of sitagliptin treatment
| 27 |
| Case 8 | Implementation of acarbose treatment
| 24 |
| Case 9 | Initiation of glibenclamide treatment
| 25 |
| Case 10 | Implementation of insulin lispro treatment
| 25 |
| Case 11 | Initiation of metformin treatment
| 25 |
| Case 12 | Implementation of glimepiride treatment
| 23 |
Appendix B
| Patient Case | Short Case Description |
|---|---|
| Case 1 | Implementation of pre-mixed insulin
|
| Case 2 | Initiation of pioglitazone and implementation of glibenclamide
|
| Case 3 | Implementation of insulin lispro and insulin detemir
|
| Case 4 | Implementation of dapagliflozin and metformin
|
| Case 5 | Implementation of sitagliptin
|
Appendix C
| Group | Summative Pre-Training Score in % | Summative Post-Training Score in % | Score Difference in Percentage Points | p-Value 1 | |||
|---|---|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | ||
| Analytical checklist | |||||||
| Intervention | 27.16 (12.75) | 33.33 (18.18) | 68.67 (14.55) | 69.57 (27.33) | 41.52 (14.63) | 43.98 (19.54) | p < 0.001 |
| Control | 31.61 (8.69) | 32.58 (13.16) | 34.76 (17.64) | 30.03 (20.92) | 3.16 (14.87) | −0.33 (16.73) | |
| Global rating scale | |||||||
| Intervention | 54.13 (18.69) | 60 (20) | 75.47 (13.84) | 80 (13.33) | 21.33 (24.42) | 20 (26.67) | p = 0.007 |
| Control | 62.22 (19.72) | 63.33 (20) | 68.61 (14.77) | 70 (16.67) | 6.39 (17.19) | 3.33 (13.33) | |
| Self-assessment questionnaire | |||||||
| Intervention | 48.69 (9.20) | 48.57 (14.29) | 63.66 (11.47) | 62.86 (17.14) | 14.97 (12.38) | 11.43 (17.14) | p = 0.001 |
| Control | 43.81 (12.93) | 42.86 (22.86) | 48.33 (14.95) | 47.14 (24.29) | 4.52 (12.03) | 2.86 (7.14) | |
References
- World Health Organization (WHO). Joint FIP/WHO Guidelines on Good Pharmacy Practice: Standards for Quality of Pharmacy Services; WHO Technical Report Series, No. 961; World Health Organization: Geneva, Switzerland, 2011; Available online: https://www.who.int/medicines/areas/quality_safety/quality_assurance/FIPWHOGuidelinesGoodPharmacyPracticeTRS961Annex8.pdf (accessed on 20 November 2020).
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action; Sabaté, E., Ed.; World Health Organization: Geneva, Switzerland, 2003; Available online: https://www.who.int/chp/knowledge/publications/adherence_report/en/ (accessed on 20 November 2020).
- Kehrer, J.P.; Eberhart, G.; Wing, M.; Horon, K. Pharmacy’s role in a modern health continuum. Can. Pharm. J. 2013, 146, 321–324. [Google Scholar] [CrossRef]
- Bates, I.; John, C.; Bruno, A.; Fu, P.; Aliabadi, S. An analysis of the global pharmacy workforce capacity. Hum. Resour. Health 2016, 14, 61. [Google Scholar] [CrossRef]
- Korf, C.; Bauer, E. Apotheken-Wirtschaftsbericht 2017—Ein erfolgreiches Jahr mit Risiken und Nebenwirkungen. Pharm. Ztg. 2017, 162, 20–35. [Google Scholar]
- National Association of Pharmacy Regulatory Authorities. National Statistics|NAPRA. Available online: https://napra.ca/national-statistics (accessed on 20 November 2020).
- Krass, I.; Schieback, P.; Dhippayom, T. Adherence to diabetes medication: A systematic review. Diabet. Med. 2015, 32, 725–737. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. IDF Diabetes Atlas 9th Edition 2019. Available online: https://www.diabetesatlas.org/upload/resources/2019/IDF_Atlas_9th_Edition_2019.pdf (accessed on 20 November 2020).
- Ho, P.M.; Rumsfeld, J.S.; Masoudi, F.A.; McClure, D.L.; Plomondon, M.E.; Steiner, J.F.; Magid, D.J. Effect of Medication Nonadherence on Hospitalization and Mortality Among Patients With Diabetes Mellitus. Arch. Intern. Med. 2006, 166, 1836–1841. [Google Scholar] [CrossRef] [PubMed]
- Egede, L.E.; Gebregziabher, M.; Dismuke, C.E.; Lynch, C.P.; Axon, R.N.; Zhao, Y.; Mauldin, P.D. Medication Nonadherence in Diabetes: Longitudinal effects on costs and potential cost savings from improvement. Diabetes Care 2012, 35, 2533–2539. [Google Scholar] [CrossRef]
- Egede, L.E.; Gebregziabher, M.; Echols, C.; Lynch, C.P. Longitudinal effects of medication nonadherence on glycemic control. Ann. Pharmacother. 2014, 48, 562–570. [Google Scholar] [CrossRef] [PubMed]
- Krass, I.; Armour, C.L.; Mitchell, B.; Brillant, M.; Dienaar, R.; Hughes, J.; Lau, P.; Peterson, G.; Stewart, K.; Taylor, S.; et al. The Pharmacy Diabetes Care Program: Assessment of a community pharmacy diabetes service model in Australia. Diabet. Med. 2007, 24, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Obarcanin, E.; Krüger, M.; Müller, P.; Nemitz, V.; Schwender, H.; Hasanbegovic, S.; Kalajdzisalihovic, S.; Läer, S. Pharmaceutical care of adolescents with diabetes mellitus type 1: The DIADEMA study, a randomized controlled trial. Int. J. Clin. Pharm. 2015, 37, 790–798. [Google Scholar] [CrossRef] [PubMed]
- Tanzi, M.G. Counseling to enhance medication adherence. PharmacyToday 2012, 18, 29. [Google Scholar] [CrossRef]
- Pathickal, S.; Patel, R.; Swaby, S. The Importance of Counseling and Its Impact on Medication Adherence. Available online: https://rhochistj.org/RhoChiPost/importance-counseling-impact-medication-adherence/ (accessed on 20 November 2020).
- Rowe, M.; Frantz, J.; Bozalek, V. The role of blended learning in the clinical education of healthcare students: A systematic review. Med. Teach. 2012, 34, e216–e221. [Google Scholar] [CrossRef] [PubMed]
- Harden, R.M. What is an OSCE? Med. Teach. 1988, 10, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Chisnall, B.; Vince, T.; Hall, S.; Tribe, R. Evaluation of outcomes of a formative objective structured clinical examination for second-year UK medical students. Int. J. Med. Educ. 2015, 6, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Rong Ho, C.; Ming Lin, C. A Short Commentary about Benefits and Drawbacks of Osces in the Nursing Education. J. Nurs. Care 2016, 5. [Google Scholar] [CrossRef]
- Alkhateeb, N.E.; Al-Dabbagh, A.; Ibrahim, M.; Al-Tawil, N.G. Effect of a Formative Objective Structured Clinical Examination on the Clinical Performance of Undergraduate Medical Students in a Summative Examination: A Randomized Controlled Trial. Indian Pediatr. 2019, 56, 745–748. [Google Scholar] [CrossRef]
- Brazeau, C.; Boyd, L.; Crosson, J. Changing an Existing OSCE to a Teaching Tool: The Making of a Teaching OSCE. Acad. Med. 2002, 77, 932. [Google Scholar] [CrossRef]
- Farahani, I.; Laeer, S.; Farahani, S.; Schwender, H.; Laven, A. Blended learning: Improving the diabetes mellitus counseling skills of German pharmacy students. Curr. Pharm. Teach. Learn. 2020, 12, 963–974. [Google Scholar] [CrossRef]
- Sulaiman, N.D.; Shorbagi, S.I.; Abdalla, N.Y.; Daghistani, M.T.; Mahmoud, I.E.; Al-Moslih, A.M. Group OSCE (GOSCE) as a formative clinical assessment tool for pre-clerkship medical students at the University of Sharjah. J. Taibah Univ. Med. Sci. 2018, 13, 409–414. [Google Scholar] [CrossRef]
- Lien, H.-H.; Hsu, S.-F.; Chen, S.-C.; Yeh, J.-H. Can teaching hospitals use serial formative OSCEs to improve student performance? BMC Res. Notes 2016, 9, 464. [Google Scholar] [CrossRef]
- Gums, T.H.; Kleppinger, E.L.; Urick, B.Y. Outcomes of Individualized Formative Assessments in a Pharmacy Skills Laboratory. Am. J. Pharm. Educ. 2014, 78, 166. [Google Scholar] [CrossRef]
- Young, I.; Montgomery, K.; Kearns, P.; Hayward, S.; Mellanby, E. The benefits of a peer-assisted mock OSCE. Clin. Teach. 2014, 11, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.L.; Dankoski, M.E. Objective structured clinical exams: A critical review. Fam. Med. 2008, 40, 574–578. [Google Scholar] [PubMed]
- Elliot, D.L.; Fields, S.A.; Keenen, T.L.; Jaffe, A.C.; Toffler, W.L. Use of a group objective structured clinical examination with first-year medical students. Acad. Med. 1994, 69, 990–992. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.B.; Madrazo, L.; Khan, U.; Thangarasa, T.; McConnell, M.; Khamisa, K. A student-initiated objective structured clinical examination as a sustainable cost-effective learning experience. Med. Educ. Online 2018, 23, 1440111. [Google Scholar] [CrossRef] [PubMed]
- Konopasek, L.; Kelly, K.V.; Bylund, C.L.; Wenderoth, S.; Storey-Johnson, C. The Group Objective Structured Clinical Experience: Building communication skills in the clinical reasoning context. Patient Educ. Couns. 2014, 96, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Biran, L.A. Self-assessment and learning through GOSCE (group objective structured clinical examination). Med. Educ. 1991, 25, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Cole, J.D.; Ruble, M.J.; Donnelly, J.; Groves, B. Peer-assisted Learning: Clinical Skills Training for Pharmacy Students. Am. J. Pharm. Educ. 2018, 82, 6511. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environmental for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Bundesärztekammer (BÄK); Kassenärztliche Bundesvereinigung (KBV); Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften. Nationale Versorgungsleitlinie Therapie des Typ-2-Diabetes—Langfassung. 1. Auflage. Version 4. Available online: www.dm-therapie.versorgungsleitlinien.de (accessed on 20 November 2020).
- Deutsche Diabetes Gesellschaft. S3-Leitlinie Therapie des Typ-1-Diabetes. 2. Auflage. Available online: www.awmf.org/leitlinien/detail/ll/057-013.html (accessed on 20 November 2020).
- Laven, A.; Deters, M.A.; Rose, O.; Schwender, H.; Smaranda, A.; Waltering, I.; Laeer, S. PharmAdhere: Training German community pharmacists with Objective Structured Clinical Examinations. Int. J. Clin. Pharm. 2018, 40, 1317–1327. [Google Scholar] [CrossRef]
- Microsoft Corporation. Microsoft Excel 2019 (for Windows); Microsoft Corporation: Redmond, WA, USA, 2019. [Google Scholar]
- OriginLab Corporation. OriginPro 2019; OriginLab Corporation: Northampton, MA, USA, 2019. [Google Scholar]
- Payne, N.J.; Bradley, E.B.; Heald, E.B.; Maughan, K.L.; Michaelsen, V.E.; Wang, X.-Q.; Corbett, E.C. Sharpening the eye of the OSCE with critical action analysis. Acad. Med. 2008, 83, 900–905. [Google Scholar] [CrossRef]
- Sandilands, D.D.; Gotzmann, A.; Roy, M.; Zumbo, B.D.; de Champlain, A. Weighting checklist items and station components on a large-scale OSCE: Is it worth the effort? Med. Teach. 2014, 36, 585–590. [Google Scholar] [CrossRef]
- Harden, R.M.; Lilley, P.; Patricio, M. The Definitive Guide to the OSCE: The Objective Structured Clinical Examination as a Performance Assessment; Elsevier: London, UK, 2016; ISBN 0702055492. [Google Scholar]
- McClimens, A.; Ibbotson, R.; Kenyon, C.; McLean, S.; Soltani, H. Confidence and performance in objective structured clinical examination. Br. J. Midwifery 2012, 20, 746–751. [Google Scholar] [CrossRef]
- Bevan, J.; Russell, B.; Marshall, B. A new approach to OSCE preparation—PrOSCEs. BMC Med. Educ. 2019, 19, 126. [Google Scholar] [CrossRef] [PubMed]
- Soni, M.R. A Comparative Study to assess the Opinion and Level of Satisfaction of the Student Nurses regarding Objective Structured Clinical Examination (OSCE) and Traditional Method of Clinical Skills Assessment related to Antenatal Examination. Int. J. Nurs. Midwifery Res. 2017, 4, 9–12. [Google Scholar] [CrossRef]




| Intervention Group (n = 25) | Control Group (n = 24) | |
|---|---|---|
| Age in years | ||
| Mean (SD) | 26.20 (± 6.14) | 24.96 (± 5.80) |
| Median | 25 | 23.5 |
| Range (minimum to maximum) | 21–49 | 20–50 |
| Gender | ||
| Female, n (%) | 18 (72) | 16 (66.67) |
| Male, n (%) | 7 (28) | 8 (33.33) |
| Experience | ||
| Additional education as pharmaceutical technician assistant Yes, n (%) | 5 (20) | 1 (4.17) |
| Currently or formerly working in a community pharmacy (counseling patients) Yes, n (%) | 2 (8) | 6 (25) |
| Group | Summative Pre-Training OSCE Score in % | Summative Post-Training OSCE Score in % | Score Difference in Percentage Points | |||
|---|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | |
| Section 1 Greeting | ||||||
| Intervention | 4 (11.06) | 0 (0) | 88 (18.95) | 100 (33.33) | 84 (19.53) | 100 (33.33) |
| Control | 5.56 (12.69) | 0 (0) | 13.89 (19.45) | 0 (33.33) | 8.33 (20.26) | 0 (16.67) |
| Section 2 Medical history | ||||||
| Intervention | 37.26 (14.60) | 40 (14.29) | 72.34 (25.83) | 80 (42.86) | 35.09 (28.79) | 37.14 (40) |
| Control | 47.74 (16.80) | 42.86 (20) | 53.10 (16.74) | 57.14 (20) | 5.36 (16.19) | 2.86 (20) |
| Section 3.1/3.2 Information on the drug (Initiation/Implementation) | ||||||
| Intervention | 33.42 (26.31) | 33.33 (37.5) | 71.90 (24.30) | 75 (30.36) | 38.48 (36.28) | 44.64 (35.71) |
| Control | 38.84 (17.73) | 35.42 (26.79) | 35.49 (31.41) | 35.42 (53.57) | −3.35 (33.53) | −7.44 (43.81) |
| Section 3.3 Prevention | ||||||
| Intervention | 27.2 (28.21) | 20 (40) | 51.2 (22.42) | 60 (20) | 24 (34.64) | 20 (60) |
| Control | 14.17 (19.98) | 0 (40) | 25 (23.77) | 20 (40) | 10.83 (30.63) | 0 (50) |
| Section 4 Goal setting | ||||||
| Intervention | 12 (33.17) | 0 (0) | 32 (47.61) | 0 (100) | 20 (40.82) | 0 (0) |
| Control | 16.67 (38.07) | 0 (0) | 16.67 (38.07) | 0 (0) | −8.88 × 1016 (58.98) | 0 (0) |
| Section 5 Patient involvement | ||||||
| Intervention | 46 (49.83) | 0 (100) | 74 (35.71) | 100 (50) | 28 (72.28) | 50 (100) |
| Control | 50 (51.08) | 50 (100) | 50 (46.63) | 50 (100) | −7.03 × 1016 (46.63) | 0 (0) |
| Section 6 Risk-Communication | ||||||
| Intervention | 4 (20) | 0 (0) | 64 (48.99) | 100 (100) | 60 (50) | 100 (100) |
| Control | 0 (0) | 0 (0) | 20.83 (41.49) | 0 (0) | 20.83 (41.49) | 0 (0) |
| Group | Summative Pre-Training OSCE Score in % | Summative Post-Training OSCE Score in % | Score Difference in Percentage Points | |||
|---|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | |
| Verbal communication skills | ||||||
| Intervention | 51.2 (23.15) | 60 (20) | 77.6 (15.62) | 80 (20) | 26.4 (25.64) | 20 (20) |
| Control | 63.33 (24.79) | 60 (30) | 68.33 (16.59) | 60 (20) | 4.8 (21.04) | 0 (20) |
| Non-verbal communication skills | ||||||
| Intervention | 57.6 (17.63) | 60 (0) | 76 (15.28) | 80 (20) | 18.4 (26.41) | 20 (40) |
| Control | 64.17 (18.63) | 60 (20) | 70.83 (16.66) | 70 (20) | 6.4 (18) | 0 (20) |
| Patient-centered communication skills | ||||||
| Intervention | 53.6 (24.98) | 60 (40) | 72.8 (19.04) | 80 (20) | 19.2 (29.71) | 20 (40) |
| Control | 59.17 (23.94) | 60 (40) | 66.67 (20.99) | 60 (20) | 7.2 (27.01) | 0 (20) |
| First Multiple-Choice Test on Diabetes | Second Multiple-Choice Test on Diabetes | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Score achieved in points | 0 | 1 | 2 | 3 | 4 | 0 | 1 | 2 | 3 | 4 |
| Proportion of the intervention group in % | 0 | 0 | 0 | 8 | 92 | 0 | 16 | 4 | 32.00 | 48.00 |
| Proportion of the control group in % | 0 | 0 | 0 | 16.67 | 83.33 | 0 | 4.17 | 8.33 | 33.33 | 54.17 |
| Group | Free-Text Item | Themes 1 |
|---|---|---|
| Intervention group | I particularly liked the following at the OSCE seminar: | • the practical exercise of counseling (simulation) and the practical training intervention |
| • the practical relevance | ||
| • the checklist as a good guide | ||
| I would change the following: | • time schedules for the OSCEs | |
| • checklist or OSCEs were not realistic | ||
| • all students should have the possibility to complete the OSCE training intervention | ||
| Control group | I particularly liked the following at the OSCE seminar: | • the practical exercise of counseling (simulation) |
| • the practical relevance | ||
| • feedback | ||
| I would change the following: | • the intervention group was better trained for the counseling was trained better, while preparing SOAP notes in the control group did not prepare for patient counseling | |
| • provision of guidance document (checklist) | ||
| • several topics should be covered |
| Intervention Group N 1 = 25 | Control Group N 1 = 24 | |||
|---|---|---|---|---|
| First Summative OSCE | Second Summative OSCE | First Summative OSCE | Second Summative OSCE | |
| Preparation of themselves | N = 25 | N = 25 | N = 24 | N = 24 |
| Yes | 92.00% | 84.00% | 91.67% | 50% |
| No | 8.00% | 8.00% | 8.33% | 29.17% |
| n.a. | 0.00% | 8.00% | 0% | 20.83% |
| Duration of preparation | N = 23 | N = 21 | N = 22 | N = 12 |
| ≤30 min | 26.09% | 61.90% | 45.45% | 66.67% |
| >30 min–≤1 h | 30.43% | 19.05% | 22.73% | 16.67% |
| >1 h–≤2 h | 30.43% | 19.05% | 13.64% | 16.67% |
| >2 h–≤3 h | 13.04% | 0.00% | 18.18% | 0.00% |
| >3 h | 0.00% | 0.00% | 0.00% | 0.00% |
| Tool used for the preparation | N = 23 | N = 21 | N = 22 | N = 12 |
| Handout | 100.00% | 66.67% | 100% | 83.33% |
| Textbooks | 4.35% | 4.76% | 0.00% | 0.00% |
| Internet | 8.70% | 0.00% | 9.09% | 8.33% |
| Own notes for other seminars | 4.35% | 0.00% | 9.09% | 0.00% |
| Notes from training | - | 71.43% | - | 16.67% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farahani, I.; Farahani, S.; Deters, M.A.; Schwender, H.; Laeer, S. Efficacy of an Objective Structured Clinical Examination Training Approach for Training Pharmacy Students in Diabetes Mellitus Counseling: A Randomized Controlled Trial. Pharmacy 2020, 8, 229. https://doi.org/10.3390/pharmacy8040229
Farahani I, Farahani S, Deters MA, Schwender H, Laeer S. Efficacy of an Objective Structured Clinical Examination Training Approach for Training Pharmacy Students in Diabetes Mellitus Counseling: A Randomized Controlled Trial. Pharmacy. 2020; 8(4):229. https://doi.org/10.3390/pharmacy8040229
Chicago/Turabian StyleFarahani, Imaneh, Samieh Farahani, Maira A. Deters, Holger Schwender, and Stephanie Laeer. 2020. "Efficacy of an Objective Structured Clinical Examination Training Approach for Training Pharmacy Students in Diabetes Mellitus Counseling: A Randomized Controlled Trial" Pharmacy 8, no. 4: 229. https://doi.org/10.3390/pharmacy8040229
APA StyleFarahani, I., Farahani, S., Deters, M. A., Schwender, H., & Laeer, S. (2020). Efficacy of an Objective Structured Clinical Examination Training Approach for Training Pharmacy Students in Diabetes Mellitus Counseling: A Randomized Controlled Trial. Pharmacy, 8(4), 229. https://doi.org/10.3390/pharmacy8040229