The Contribution of the Humanities and Social Sciences to Pharmacy Education: Literature Review and Perspectives

 ,
, {kind=link}
Abstract
1. Introduction
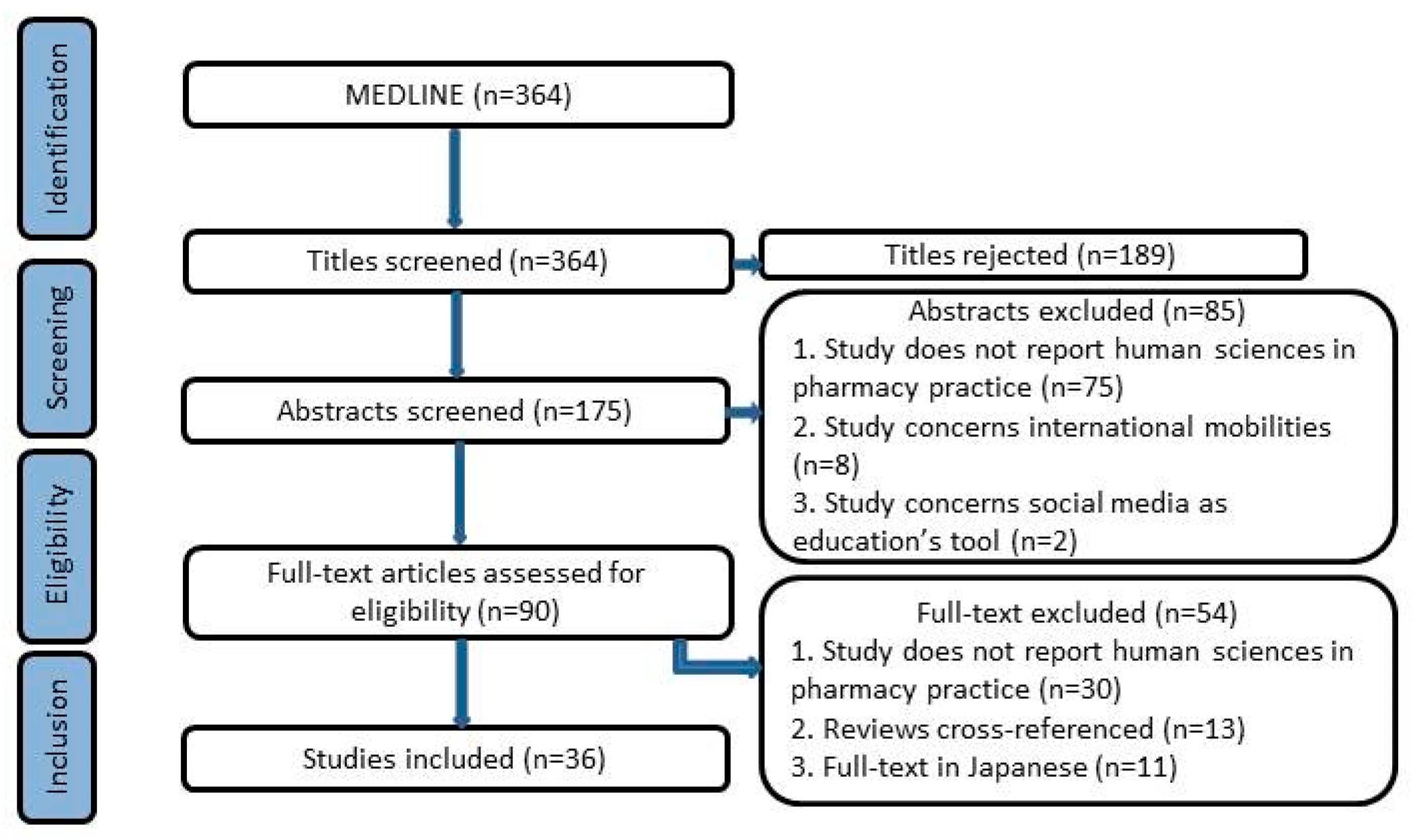
2. Materials and Methods
OR “pharmacies” [MeSH Terms] OR “pharmacies” [All Fields]) OR “social sciences”
[MeSH Major Topic])) OR “humanities” [MeSH Major Topic]) AND “education,
pharmacy” [MeSH Major Topic] AND (“2009/01/01” [PDAT] : “2019/05/01” [PDAT])
3. Results
3.1. Strategic Evolution of the Pharmacist Profession
3.1.1. Evolution of the Pharmacist Profession and Initial Training of Practitioners
3.1.2. Evolution of the Profession and Global Disparities
3.2. Relationship Skills Towards the Patient
3.2.1. Cultural and Emotional Competencies
3.2.2. Professionalism
3.3. Interprofessional Collaborations and Integration of a Multidisciplinary Team
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Study Characteristics
| Article | Year of Publication | Type of Publication | Country | Sub-Theme |
| Main topic: Strategic evolution of the pharmacist profession | ||||
| Hassali MA, et al. Social pharmacy as a field of study: the needs and challenges in global pharmacy education. [10] | 2011 | Commentary | Malaysia | Global disparities in public health |
| Law MG, et al. Addressing the global need for public health clinical pharmacists through student pharmacist education: a focus on developing nations. [12] | 2017 | Commentary | USA | Global disparities in public health |
| Palaian S, et al. Initiation of social pharmacy research in Nepal: our experiences. [11] | 2011 | Commentary | Nepal | Global disparities in public health |
| Bush AA, et al. Identifying Shared Values for School-Affiliated Student Organizations. [18] | 2017 | Empirical study | USA | Adapting training to change |
| King AE, et al. A Required Online Course with a Public Health Focus for Third Professional Year Pharmacy Students. [16] | 2015 | Empirical study | USA | Adapting training to change |
| Offiong CY, et al. The role of colleges and schools of pharmacy in the advent of Healthy People 2020. [9] | 2010 | Commentary | USA | Adapting training to change |
| Teagarden JR. Well connected: pharmacy education and the humanities. [17] | 2013 | Commentary | USA | Adapting training to change |
| Youmans S, et al. Clinical pharmacy to meet the health needs of Tanzanians: education reform through partnership across continents (2008–2011). [13] | 2012 | Commentary | Tanzania | Adapting training to change |
| American College of Clinical Pharmacy, et al. Cultural competency in health care and its implications for pharmacy part 3A: emphasis on pharmacy education, curriculums, and future directions. [15] | 2013 | Commentary | USA | Global disparities and adapting training to change |
| Nunes-da-Cunha I, et al. A Comparison of Patient-Centered Care in Pharmacy Curricula in the United States and Europe. [14] | 2016 | Empirical study | Europe/USA | Global disparities and adapting training to change |
| David PM, et al. [The evolution of pharmaceutical practice within the context of changing health territories: How can social sciences contribute to pharmaceutical education?]. [8] | 2010 | Commentary | France | Pharmacist and public health |
| Momas I. [Public health and the pharmacist: a challenge of importance regarding training]. [7] | 2009 | Commentary | France | Pharmacist and public health |
| Main topic: Relationship skills towards the patient | ||||
| Saw PS, et al. A practical approach toward teaching ethics to community pharmacists. [32] | 2018 | Empirical study | Malaysia | Ethic |
| Cooper LA, et al. Pharmacy students’ perceptions of cultural competence encounters during practice experiences. [24] | 2014 | Empirical study | USA | Cultural competences |
| Echeverri M, et al. Racial Dynamics and Cultural Competence Training in Medical and Pharmacy Education. [25] | 2017 | Empirical study | USA | Cultural competences |
| Galal S, et al. Development and assessment of social and emotional competence through simulated patient consultations. [21] | 2012 | Empirical study | USA | Cultural competences |
| Godwin JN Jr. An enhanced appreciation of cultural competency: Applying knowledge at home and abroad. [19] | 2017 | Commentary | USA | Cultural competences |
| Jacob B, et al. First-year Student Pharmacists’ Spirituality and Perceptions Regarding the Role of Spirituality in Pharmacy Education. [26] | 2017 | Empirical study | USA | Cultural competences |
| Okoro ON, et al. Clinical cultural competency and knowledge of health disparities among pharmacy students. [22] | 2012 | Empirical study | USA | Cultural competences |
| Poirier TI, et al. A cultural competency course for pharmacy students. [20] | 2009 | Empirical study | USA | Cultural competences |
| Sales I, et al. A comparison of educational interventions to enhance cultural competency in pharmacy students. [23] | 2013 | Empirical study | USA | Cultural competences |
| Chen AM, et al. Impact of a health literacy assignment on student pharmacist learning. [30] | 2013 | Empirical study | USA | Cultural competences and professionalism |
| Terry C, et al. The Emerging Issue of Digital Empathy. [31] | 2016 | Commentary | USA | Cultural competences and professionalism |
| Zimmermann M. Integrating medical humanities into a pharmaceutical care seminar on dementia. [29] | 2013 | Empirical study | Germany | Cultural competences and professionalism |
| Horton ER, et al. A Novel Structured Format for Engaging Pharmacy Students in Bioethics Discussions. [33] | 2014 | Empirical study | USA | Ethic and professionalism |
| Smith MG, et al. Early Introduction to Professional and Ethical Dilemmas in a Pharmaceutical Care Laboratory Course. [34] | 2015 | Empirical study | USA | Ethic and professionalism |
| Mesquita AR, et al. Developing communication skills in pharmacy: a systematic review of the use of simulated patient methods. [27] | 2010 | Review article | Brazil | Professionalism |
| Mylrea MF, et al. Professionalization in Pharmacy Education as a Matter of Identity. [28] | 2015 | Commentary | Australia | Professionalism |
| Main topic: Interprofessional collaborations and integration of a multidisciplinary team | ||||
| Branch-Mays GL, et al. An Interprofessional Education and Collaborative Practice Model for Dentistry and Pharmacy. [42] | 2017 | Empirical study | USA | In professional practice |
| El-Awaisi A, et al. A comprehensive systematic review of pharmacy perspectives on interprofessional education and collaborative practice. [35] | 2018 | Review article | Qatar | In professional practice |
| LaRochelle JM, et al. Racial Differences in Communication Apprehension and Interprofessional Socialization in Fourth-Year Doctor of Pharmacy Students. [39] | 2016 | Empirical study | USA | In professional practice |
| El-Awaisi A, et al. Interprofessional education in the Arabic-speaking Middle East: Perspectives of pharmacy academics. [41] | 2016 | Empirical study | Arabic-speaking Middle East | Disparities |
| Anderson E, et al. Interprofessional learning on polypharmacy. [40] | 2016 | Empirical study | Royaume-Uni | Right for the training |
| Gilligan C, et al. Recommendations from recent graduates in medicine, nursing and pharmacy on improving interprofessional education in university programs: a qualitative study. [38] | 2014 | Empirical study | Australia TasmaniaNew Zealand | Right for the training |
| Goldstone LW, et al. An interprofessional psychiatric advanced pharmacy practice experience. [36] | 2013 | Empirical study | USA | Right for the training |
| Pittenger AL, et al. An interprofessional diabetes experience to improve pharmacy and nursing students’ competency in collaborative practice. [37] | 2013 | Empirical study | USA | Right for the training |
References
- Dindial, S.; Fung, C.; Arya, V. A Call for Greater Policy Emphasis and Public Health Applications in Pharmacy Education. Am. J. Pharm. Educ. 2012, 76. [Google Scholar] [CrossRef] [PubMed]
- Lichtveld, M.Y.; Cioffi, J.P.; Baker, E.L.; Bailey, S.B.; Gebbie, K.; Henderson, J.V.; Weiss, S.M.; Kurz, R.S.; Margolis, S.; Miner, K.; et al. Partnership for Front-Line Success. J. Public Heal. Manag. Pr. 2001, 7, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Golodner, L.; A Zellmer, W. A Consumer Advocate’s Perspective on Pharmacist Competencies and Pharmacy Education. Am. J. Pharm. Educ. 2013, 77, 48. [Google Scholar] [CrossRef]
- Poirier, T.I.; Stamper-Carr, C. A Call for a New Ism in Pharmacy. Am. J. Pharm. Educ. 2018, 82, 6441. [Google Scholar] [CrossRef] [PubMed]
- Levac, D.; Colquhoun, H.; A Nixon, S. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Heal. Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Momas, I. Public health and the pharmacist: A challenge of importance regarding training. Ann. Pharm. Françaises 2009, 67, 25–31. [Google Scholar] [CrossRef] [PubMed]
- David, P.-M.; Locher, F. The evolution of pharmaceutical practice within the context of changing health territories: How can social sciences contribute to pharmaceutical education? Ann. Pharm. Françaises 2010, 68, 205–211. [Google Scholar] [CrossRef]
- Offiong, C.Y.; Oji, V.U.; Bunyan, W.; Lewis, J.A.; Moore, C.; Olusanya, O.A. The Role of Colleges and Schools of Pharmacy in the Advent of Healthy People 2020. Am. J. Pharm. Educ. 2011, 75, 56. [Google Scholar] [CrossRef]
- Hassali, M.A.; Shafie, A.A.; Al-Haddad, M.S.; Abduelkarem, A.; Ibrahim, M.I.; Palaian, S.; Abrika, O.S.S. Social pharmacy as a field of study: The needs and challenges in global pharmacy education. Res. Soc. Adm. Pharm. 2011, 7, 415–420. [Google Scholar] [CrossRef]
- Palaian, S.; Poudel, A.; Alam, K.; Ibrahim, M.I.M.; Mishra, P. Initiation of social pharmacy research in Nepal: Our experiences. Int. J. Clin. Pharm. 2011, 33, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Law, M.G.; Maposa, P.; Steeb, D.R.; Duncan, G.J. Addressing the global need for public health clinical pharmacists through student pharmacist education: A focus on developing nations. Int. J. Clin. Pharm. 2017, 39, 1141–1144. [Google Scholar] [CrossRef] [PubMed]
- Youmans, S.; Ngassapa, O.; Chambuso, M. Clinical pharmacy to meet the health needs of Tanzanians: Education reform through partnership across continents (2008–2011). J. Public Heal. Policy 2012, 33, S110–S125. [Google Scholar] [CrossRef]
- Nunes-Da-Cunha, I.; Arguello, B.; Martinez, F.M.; Fernandez-Llimos, F. A Comparison of Patient-Centered Care in Pharmacy Curricula in the United States and Europe. Am. J. Pharm. Educ. 2016, 80, 83. [Google Scholar] [CrossRef] [PubMed]
- American College of Clinical Pharmacy; O’Connell, M.B.; De Bittner, M.R.; Poirier, T.I.; Karaoui, L.R.; Echeverri, M.; Chen, A.M.H.; Lee, S.-Y.; Vyas, D.; O’Neil, C.K.; et al. Cultural Competency in Health Care and Its Implications for Pharmacy Part 3A: Emphasis on Pharmacy Education, Curriculums, and Future Directions. Pharm. J. Hum. Pharm. Drug 2013, 33, e347–e367. [Google Scholar] [CrossRef]
- King, A.E.; Egras, A.M. A Required Online Course with a Public Health Focus for Third Professional Year Pharmacy Students. Am. J. Pharm. Educ. 2015, 79, 68. [Google Scholar] [CrossRef]
- Teagarden, J.R. Well Connected: Pharmacy Education and the Humanities. J. Med. Hum. 2013, 34, 477–480. [Google Scholar] [CrossRef]
- Bush, A.A.; Buhlinger, K.M.; McLaughlin, J.E. Identifying Shared Values for School-Affiliated Student Organizations. Am. J. Pharm. Educ. 2017, 81, 6076. [Google Scholar] [CrossRef]
- Godwin, J.N. An enhanced appreciation of cultural competency: Applying knowledge at home and abroad. J. Am. Pharm. Assoc. 2017, 57, 293–294. [Google Scholar] [CrossRef][Green Version]
- Poirier, T.I.; Butler, L.M.; Devraj, R.; Gupchup, G.V.; Santanello, C.; Lynch, J.C. A Cultural Competency Course for Pharmacy Students. Am. J. Pharm. Educ. 2009, 73, 81. [Google Scholar] [CrossRef]
- Galal, S.M.; Carr-Lopez, S.; Seal, C.R.; Scott, A.N.; Lopez, C. Development and Assessment of Social and Emotional Competence Through Simulated Patient Consultations. Am. J. Pharm. Educ. 2012, 76. [Google Scholar] [CrossRef] [PubMed]
- Okoro, O.N.; Odedina, F.T.; Reams, R.R.; Smith, W.T. Clinical Cultural Competency and Knowledge of Health Disparities Among Pharmacy Students. Am. J. Pharm. Educ. 2012, 76. [Google Scholar] [CrossRef] [PubMed]
- Sales, I.; Jonkman, L.; Connor, S.; Hall, D. A Comparison of Educational Interventions to Enhance Cultural Competency in Pharmacy Students. Am. J. Pharm. Educ. 2013, 77, 76. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.-A.; Vellurattil, R.P.; Quiñones-Boex, A. Pharmacy Students’ Perceptions of Cultural Competence Encounters During Practice Experiences. Am. J. Pharm. Educ. 2014, 78. [Google Scholar] [CrossRef] [PubMed]
- Echeverri, M.; Dise, T. Racial Dynamics and Cultural Competence Training in Medical and Pharmacy Education. J. Heal. Care Poor Underserved 2017, 28, 266–278. [Google Scholar] [CrossRef]
- Jacob, B.C.; White, A.; Shogbon, A. First-year Student Pharmacists’ Spirituality and Perceptions Regarding the Role of Spirituality in Pharmacy Education. Am. J. Pharm. Educ. 2017, 81. [Google Scholar] [CrossRef]
- Mesquita, A.R.; Lyra, D.P.; Brito, G.C.; Balisa-Rocha, B.J.; Aguiar, P.M.; Neto, A.C.D.A.; Aguiar, P.M. Developing communication skills in pharmacy: A systematic review of the use of simulated patient methods. Patient Educ. Couns. 2010, 78, 143–148. [Google Scholar] [CrossRef]
- Mylrea, M.F.; Gupta, T.S.; Glass, B.D. Professionalization in Pharmacy Education as a Matter of Identity. Am. J. Pharm. Educ. 2015, 79, 142. [Google Scholar] [CrossRef]
- Zimmermann, M. Integrating Medical Humanities into a Pharmaceutical Care Seminar on Dementia. Am. J. Pharm. Educ. 2013, 77. [Google Scholar] [CrossRef]
- Chen, A.M.H.; Noureldin, M.; Plake, K.S. Impact of a health literacy assignment on student pharmacist learning. Res. Soc. Adm. Pharm. 2013, 9, 531–541. [Google Scholar] [CrossRef]
- Terry, C.; Cain, J. The Emerging Issue of Digital Empathy. Am. J. Pharm. Educ. 2016, 80, 58. [Google Scholar] [CrossRef] [PubMed]
- Saw, P.S.; Chuah, L.H.; Lee, S.W.H. A practical approach toward teaching ethics to community pharmacists. Int. J. Clin. Pharm. 2018, 40, 1131–1136. [Google Scholar] [CrossRef] [PubMed]
- Horton, E.R.; Morin, A.; Pervanas, H.C.; Mukherjee, S.M.; Belliveau, P. A Novel Structured Format for Engaging Pharmacy Students in Bioethics Discussions. Am. J. Pharm. Educ. 2014, 78, 171. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.G.; Dinkins, M.M. Early Introduction to Professional and Ethical Dilemmas in a Pharmaceutical Care Laboratory Course. Am. J. Pharm. Educ. 2015, 79, 156. [Google Scholar] [CrossRef] [PubMed]
- El-Awaisi, A.; Joseph, S.; El Hajj, M.S.; Diack, L. A comprehensive systematic review of pharmacy perspectives on interprofessional education and collaborative practice. Res. Soc. Adm. Pharm. 2018, 14. [Google Scholar] [CrossRef]
- Goldstone, L.W.; Cooley, J. An Interprofessional Psychiatric Advanced Pharmacy Practice Experience. Am. J. Pharm. Educ. 2013, 77, 129. [Google Scholar] [CrossRef]
- Pittenger, A.L.; Westberg, S.; Rowan, M.; Schweiss, S. An Interprofessional Diabetes Experience to Improve Pharmacy and Nursing Students’ Competency in Collaborative Practice. Am. J. Pharm. Educ. 2013, 77, 197. [Google Scholar] [CrossRef]
- Gilligan, C.; Outram, S.V.; Levett-Jones, T. Recommendations from recent graduates in medicine, nursing and pharmacy on improving interprofessional education in university programs: A qualitative study. BMC Med. Educ. 2014, 14, 52. [Google Scholar] [CrossRef]
- LaRochelle, J.M.; Karpinski, A.C. Racial Differences in Communication Apprehension and Interprofessional Socialization in Fourth-Year Doctor of Pharmacy Students. Am. J. Pharm. Educ. 2016, 80. [Google Scholar] [CrossRef]
- Anderson, E.; Lakhani, N. Interprofessional learning on polypharmacy. Clin. Teach. 2016, 13, 291–297. [Google Scholar] [CrossRef]
- El-Awaisi, A.; El Hajj, M.S.; Joseph, S.C.; Diack, L. Interprofessional education in the Arabic-speaking Middle East: Perspectives of pharmacy academics. J. Interprof. Care 2016, 30, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Branch-Mays, G.L.; Pittenger, A.L.; Williamson, K.; Milone, A.; Hein, E.; Thierer, T. An Interprofessional Education and Collaborative Practice Model for Dentistry and Pharmacy. J. Dent. Educ. 2017, 81, 1413–1420. [Google Scholar] [CrossRef] [PubMed]
- Nutbeam, D. Health Promotion Glossary. Heal. Promot. Int. 1998, 13, 349–364. [Google Scholar] [CrossRef]
- Der Putten, M.; Makone, A.S.; Chiriseri, E.T.; Vichit-Vadakan, N. Fostering a Paradigm Shift in the Roles of Health Promotion Education in Southeast Asia. Res. Hum. Soc. Sci. 2012, 2, 28–38. [Google Scholar]
- Barry Margaret, M.; Barbara, B.-K.; Heather, D.; Colette, D.; Richard, P.; Marielle, S.; Viv, S.; Gerard, V.d.Z.; Anna, Z. CompHP: Developing Competencies and Professional Standards for Health Promotion Capacity Building in Europe: The CompHP Project Handbook; International Union for Health Promotion and Education: Paris, French, 2012. [Google Scholar]
- Braveman, P.; Gottlieb, L. The Social Determinants of Health: It’s Time to Consider the Causes of the Causes. Public Heal. Rep. 2014, 129, 19–31. [Google Scholar] [CrossRef]
- Marmot, M.; Bell, R. Fair society, healthy lives. Public Heal. 2012, 126, S4–S10. [Google Scholar] [CrossRef]
- Wylie, A.; Leedham-Green, K. Health promotion in medical education: Lessons from a major undergraduate curriculum implementation. Educ. Prim. Care 2017, 28, 325–333. [Google Scholar] [CrossRef]
- Svensson, C.K.; Ascione, F.J.; Bauman, J.L.; Brueggemeier, R.W.; Letendre, D.E.; Roberts, J.C.; Speedie, M.K. Are We Producing Innovators and Leaders or Change Resisters and Followers? Am. J. Pharm. Educ. 2012, 76, 124. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boulliat, C.; Darlington, E.; Faure, M.-A.; Massoubre, B.; Dussart, C. The Contribution of the Humanities and Social Sciences to Pharmacy Education: Literature Review and Perspectives. Pharmacy 2020, 8, 227. https://doi.org/10.3390/pharmacy8040227
Boulliat C, Darlington E, Faure M-A, Massoubre B, Dussart C. The Contribution of the Humanities and Social Sciences to Pharmacy Education: Literature Review and Perspectives. Pharmacy. 2020; 8(4):227. https://doi.org/10.3390/pharmacy8040227
Chicago/Turabian StyleBoulliat, Caroline, Emily Darlington, Marie-Ange Faure, Bernard Massoubre, and Claude Dussart. 2020. "The Contribution of the Humanities and Social Sciences to Pharmacy Education: Literature Review and Perspectives" Pharmacy 8, no. 4: 227. https://doi.org/10.3390/pharmacy8040227
APA StyleBoulliat, C., Darlington, E., Faure, M.-A., Massoubre, B., & Dussart, C. (2020). The Contribution of the Humanities and Social Sciences to Pharmacy Education: Literature Review and Perspectives. Pharmacy, 8(4), 227. https://doi.org/10.3390/pharmacy8040227