
A Study of Climate-Sensitive Diseases in Climate-Stressed Areas of Bangladesh

 , , ,
, , ,  , ,
, ,
Abstract
1. Introduction
2. Methods
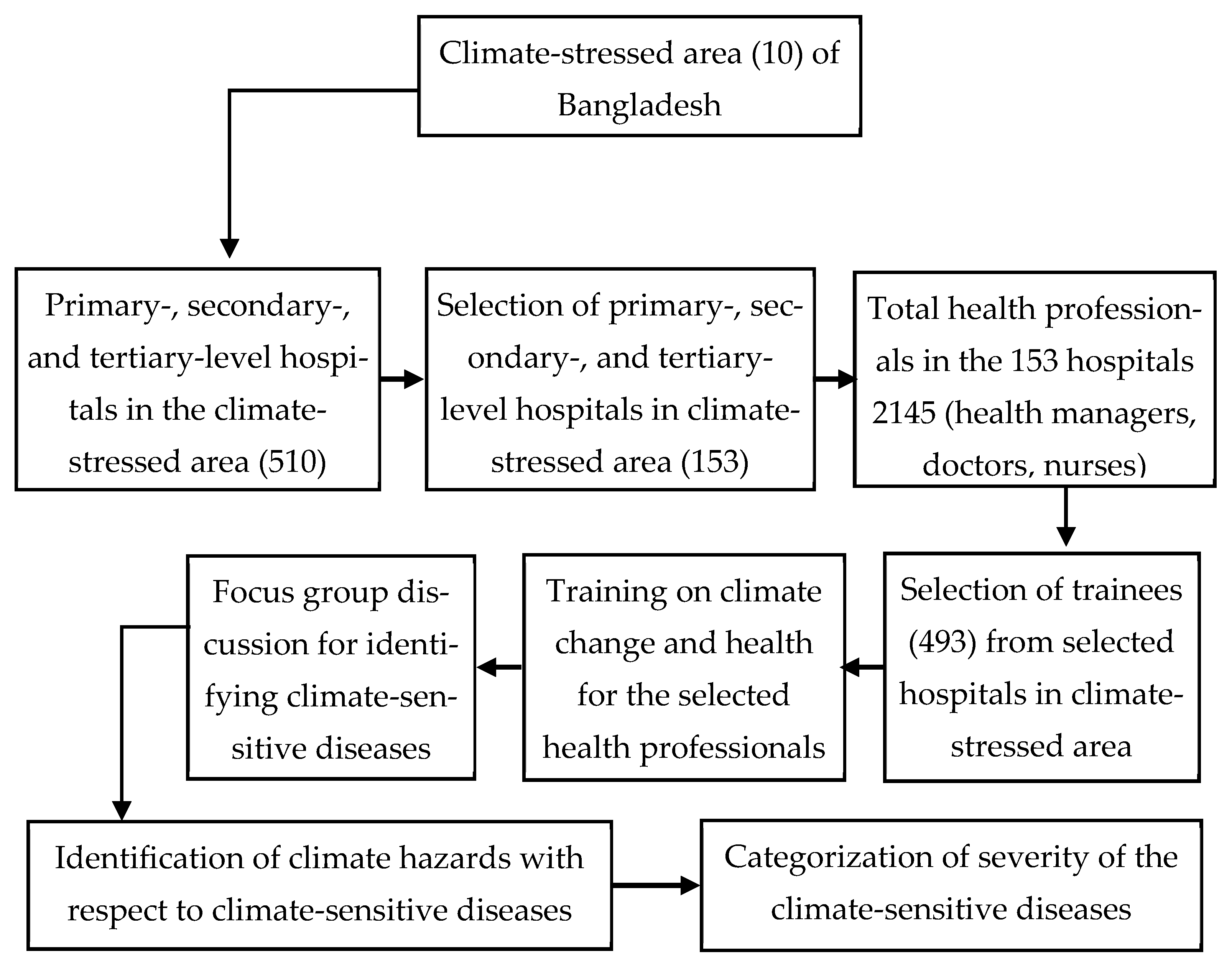
2.1. Study Design
2.2. Method, Tools, and Sample Type and Size
2.3. Training of Participating Health Professionals
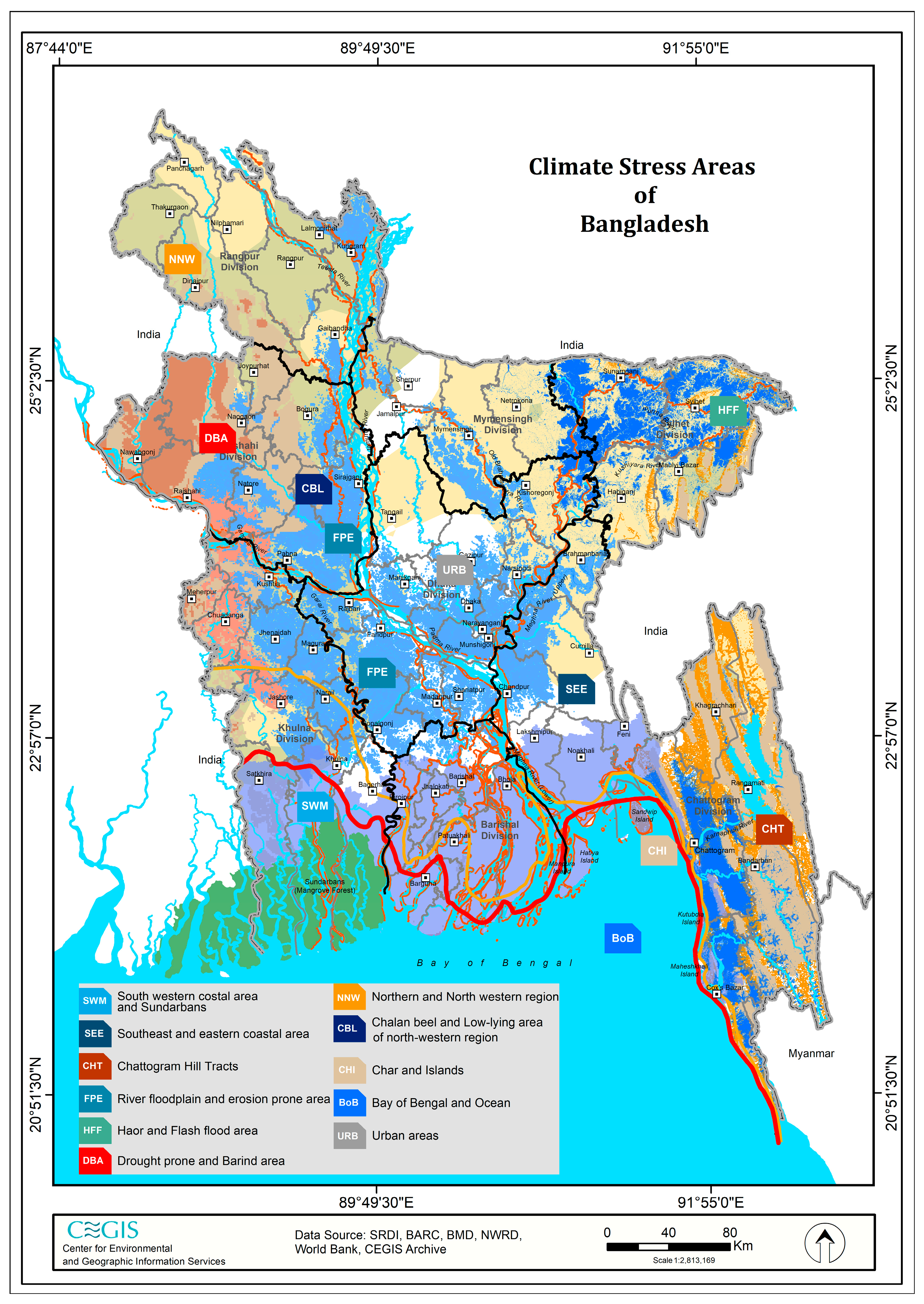
2.4. Sampling Sites
2.5. Data Collection and Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Bianco, G.; Espinoza-Chávez, R.M.; Ashigbie, P.G.; Junio, H.; Borhani, C.; Miles-Richardson, S.; Spector, J. Projected Impact of Climate Change on Human Health in Low- and Middle-income countries: A Systematic Review. BMJ Glob. Health 2024, 8, e015550. [Google Scholar] [CrossRef] [PubMed]
- The World Bank Group. Climate Risk Country Profile: Bangladesh; The World Bank Group: Washington, DC, USA, 2021; Available online: https://climateknowledgeportal.worldbank.org/sites/default/files/country-profiles/15502-WB_Bangladesh%20Country%20Profile-WEB.pdf (accessed on 14 May 2025).
- Rashid, M.B.; Sultana, A.; Hassan, S.M.Q.; Kuya, E.; Parding, K.; Hygen, H.O. Changing Climate of Bangladesh—METreport, 04/2024. In Proceedings of the EMS Annual Meeting 2024, Barcelona, Spain, 1–6 September 2024; Available online: https://live6.bmd.gov.bd/file/2024/02/27/pdf/162368.pdf (accessed on 14 May 2025).
- Masum, J.H. Climatic Hazards in Bangladesh: A Literature Review; Coastal Development Partnership (CDP): Dhaka, Bangladesh, 2019; ISBN 978-984-34-7002-4. [Google Scholar]
- O’Leary, L.; Dasgupta, S.; Robinson, E.J.Z. Impacts of Climate Change on Health in Bangladesh: Policy Brief; Grantham Research Institute on Climate Change and the Environment and the Centre for Climate Change Economics and Policy, University of Leeds: Leeds, UK, 2023; Available online: https://www.lse.ac.uk/granthaminstitute/wp-content/uploads/2023/10/Impacts-of-climate-change-on-health-in-Bangladesh-Policy-brief.pdf (accessed on 14 May 2025).
- World Health Organization. United Nations Framework Convention on Climate Change: Climate and Health Country Profile—2015; World Health Organization: Geneva, Switzerland, 2015; Available online: https://cdn.who.int/media/docs/default-source/searo/wsh-och-searo/ban-c-h-profile.pdf?sfvrsn=8b172763_2 (accessed on 20 May 2025).
- Ministry of Environment, Forest and Climate Change, Government of the People’s Republic of Bangladesh. Summary Report: National Adaptation Plan of Bangladesh (2023–2050); Ministry of Environment, Forest and Climate Change, Government of the People’s Republic of Bangladesh: Dhaka, Bangladesh, 2022; Available online: https://www.undp.org/bangladesh/publications/national-adaptation-plan-bangladesh-2023-2050 (accessed on 20 May 2025).
- Shamsuddoha, M.; Jabed, M.A.; Islam, M.S.; Sultana, N.; Imran, A.; Rabbi, S.N.A.; Jenat, T.U.; Shams, S.; Sharif, M.M. Impacts of climate change-induced natural hazards on women and their human rights implications: A study in the southwest coast of Bangladesh. J. Migr. Health 2024, 9, 100221. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.R.; Tareq, S.M.; Rahman, S.H. Effects of Climate Variables on Kala-azar Prevalence at Major Affected Districts in Bangladesh. J. Environ. Sci. Nat. Resour. 2013, 6, 79–87. [Google Scholar] [CrossRef]
- Mutsuddy, P.; Sanya, T.J.; Shamsuzzaman, A.K.M.; Kaisar, S.M.G.; Khan, M.N.A. Dengue Situation in Bangladesh: An Epidemiological Shift in terms of Morbidity and Mortality. Can. J. Infect. Dis. Med. Microbiol. 2019, 2019, 3516284. [Google Scholar] [CrossRef] [PubMed]
- Kabir, I.; Dhimal, M.; Müller, R.; Banik, S.; Haque, U. The 2017 Dhaka chikungunya outbreak. Lancet Infect. Dis. 2017, 17, 1118. [Google Scholar] [CrossRef] [PubMed]
- Ehsanur, P. An Analysis of the Impacts of Temperature on Diarrheal Disease in Bangladesh. Int. J. Soc. Sci. Econ. Res. 2017, 2, 5040–5049. [Google Scholar]
- Checkley, W.; Epstein, L.D.; Gilman, R.H.; Figueroa, D.; Cama, R.I.; Patz, J.A.; Black, R.E. Effects of EI Niño and ambient temperature on hospital admissions for diarrhoeal diseases in Peruvian children. Lancet 2000, 355, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Moon, M.P. Food and health security impact of climate change in Bangladesh: A Review. J. Water Clim. Change 2023, 14, 3484–3495. [Google Scholar] [CrossRef]
- Hayes, K.; Blashki, G.; Wiseman, J.; Burke, S.; Reifels, L. Climate Change and Mental Health: Risks, Impacts and Priority Ac-tions. Int. J. Ment. Health Syst. 2018, 12, 28. [Google Scholar] [CrossRef] [PubMed]
- Chinyere, U.; Val, E. Qualitative Research. IDOSR J. Comput. Appl. Sci. 2023, 8, 20–35. Available online: https://www.researchgate.net/publication/367221023 (accessed on 22 May 2025).
- Ismail, G.; Taliep, N. The Delphi Method. In Handbook of Social Sciences and Global Public Health; Liamputtong, P., Ed.; Springer: Cham, Switzerland, 2023. [Google Scholar] [CrossRef]
- Huq, S.; Khan, M.; Islam, A.S.; Mirza, A.B. Climate Change Impacts in Bangladesh: What Climate Change Means for a Country and Its People. 2024. Available online: https://www.icccad.net/wp-content/uploads/2024/02/Bangladesh_Final_Covers_26-Jan-2024_ONLINE_compressed.pdf#:~:text=Even%20with%20ambitious%20climate%20action%20(RCP2.%206)%2C,century%2C%20increasing%20flooding%20in%20low%2D%20lying%20Bangladesh (accessed on 22 May 2025).
- Hasan, M.K.; Younos, T.B.; Chowdhury, R.I.; Masud, K.B.; González, P.A.; Castro-Delgado, R. Cold wave induced mortalities in Bangladesh: Spatiotemporal Analysis of 20 Years’ Data, 2000–2019. Nat. Hazards Res. 2024, 4, 604–615. [Google Scholar] [CrossRef]
- Mirsaeidi, M.; Motahari, H.; Taghizadeh, K.M.; Sharifi, A.; Campos, M.; Schraufnagel, D.E. Climate Change and Respiratory Infections. Ann. Am. Thorac. Soc. 2016, 13, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Miah, M.; Ullah, S.; Siddique, M. Heat Waves in Bangladesh: Understanding the Threats and Finding Solutions. Asia Pac. J. Energy Environ. 2022, 9, 89–98. [Google Scholar] [CrossRef]
- Zhou, L.; He, C.; Kim, H.; Honda, Y.L.W.; Hashizume, M.; Chen, R.; Kan, H. The Burden of Heat-Related Stroke Mortality under Climate Change Scenarios in 22 East Asian Cities. Environ. Int. 2022, 170, 107602. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.M.; Wang, H.W.; Chang, F.W.; Liu, Y.P.; Chiu, F.H.; Lin, Y.C.; Cheng, K.C.; Hsu, R.J. The Effects of Climate Factors on Scabies: A 14-Year Population-Based Study in Taiwan. Parasite 2016, 23, 54. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.J.; Khant, N.A.; Kim, H.; Namkoong, S. Impact of Climate Change on Waterborne Diseases: Directions towards Sustainability. Water 2023, 15, 1298. [Google Scholar] [CrossRef]
- Chowdhury, F.R.; Ibrahim, Q.S.U.; Bari, M.S.; Alam, M.M.J.; Dunachie, S.J.; Rodriguez-Morales, A.J.; Patwary, M.I. The Association between Temperature, Rainfall and Humidity with Common Climate-Sensitive Infectious Diseases in Bangladesh. PLoS ONE 2020, 15, e0232285. [Google Scholar] [CrossRef] [PubMed]
- Luby, S.P.; Rahman, M.; Arnold, B.F.; Unicomb, L.; Ashraf, S.; Winch, P.J.; Stewart, C.P.; Begum, F.; Hussain, F.; Benjamin-Chung, J.; et al. Effects of Water Quality, Sanitation, Handwashing, and Nutritional Interventions on Diarrhoea and Child Growth in Rural Bangladesh: A Cluster Randomised Controlled Trial. Lancet Glob. Health 2018, 6, e302–e315. [Google Scholar] [CrossRef] [PubMed]
- Gullón, P.; Varela, C.; Martínez, E.V.; Barroso, D.G. Association between Meteorological Factors and Hepatitis A in Spain 2010–2014. Environ. Int. 2017, 102, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Lipp, E.K.; Huq, A.; Colwell, R.R. Effects of Global Climate on Infectious Disease: The Cholera Model. Clin. Microbiol. Rev. 2002, 15, 757–770. [Google Scholar] [CrossRef] [PubMed]
- Shamsuddin, S. Rainfall Variability and Changes in Bangladesh during the last Fifty Years. In Rainfall: Behavior Forecasting and Distribution; National Center for Meteorology: Jeddah, Saudi Arabia, 2012; pp. 23–44. Available online: https://www.researchgate.net/publication/286565576 (accessed on 20 May 2025).
- Balato, N.; Megna, M.; Ayala, F.; Balato, A.; Napolitano, M.; Patruno, C. Effects of Climate Changes on Skin Diseases. Expert Rev. Anti Infect. Ther. 2014, 12, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Aditi, G.; Wendemagegn, E.; Louise, K.A.; Sarah, J.C. The Effects of Climate Change on Fungal Diseases with Cutaneous Manifestations: A Report from the International Society of Dermatology Climate Change Committee. J. Clim. Change Health 2022, 6, 100156. [Google Scholar] [CrossRef]
- Dewan, A.M.; Corner, R.; Hashizume, M.; Ongee, E.T. Typhoid Fever and Its Association with Environmental Factors in the Dhaka Metropolitan Area of Bangladesh: A Spatial and Time-Series Approach. PLoS Negl. Trop. Dis. 2013, 7, e1998. [Google Scholar] [CrossRef] [PubMed]
- Islam, S.; Haque, C.E.; Hossain, S.; Hanesiak, J. Climate Variability, Dengue Vector Abundance and Dengue Fever Cases in Dhaka, Bangladesh: A Time-Series Study. Atmosphere 2021, 12, 905. [Google Scholar] [CrossRef]
- Khan, J.R.; Awan, N.; Archie, R.J.; Sultana, N.; Muurlink, O. The Association between Drinking Water Salinity and Hyper-tension in Coastal Bangladesh. Glob. Health J. 2020, 4, 153–158. [Google Scholar] [CrossRef]
- Mishu, M.P.; Rabbani, M.M.G.; Vereeken, S.; Martin-Kerry, J.; Chowdhury, T.F.; Wahab, A.; Mashreky, S.R.; Huque, R.; Friend, R. Exploring the Association between Mental Health and Extreme Weather Events Related to Climate Change: A Scoping review. Lancet 2024, 404, S28. [Google Scholar] [CrossRef]
- Mirzabaev, A.; Kerr, R.B.; Hasegawa, T.; Pradhan, P.; Wreford, A.; von der Pahlen, M.C.T.; Gurney-Smith, H. Severe Climate Change Risks to Food Security and Nutrition. Clim. Risk Manag. 2023, 39, 100473. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Sl. No. | Climate-Stressed Area | BoB | CBL | CHI | CHT | DBA | FPE | HFF | NNW | SEE | SWM | Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Number of districts | 1 | 2 | 2 | 3 | 1 | 3 | 2 | 1 | 3 | 3 | 21 | |
| 2 | Number of upazilas | 7 | 13 | 13 | 19 | 11 | 21 | 17 | 13 | 19 | 23 | 156 | |
| 3 | Number of selected HCFs | 7 | 13 | 13 | 19 | 10 | 21 | 16 | 13 | 18 | 23 | 153 | |
| 4 | Total public health professionals in the selected HCFs | UH&FPOs | 7 | 13 | 14 | 25 | 11 | 19 | 21 | 13 | 19 | 22 | 162 |
| Doctors | 46 | 183 | 182 | 164 | 81 | 170 | 152 | 228 | 298 | 187 | 1691 | ||
| Nurses | 23 | 23 | 12 | 39 | 32 | 36 | 20 | 45 | 36 | 34 | 292 | ||
| Total | 76 | 219 | 208 | 228 | 124 | 225 | 193 | 286 | 353 | 243 | 2145 | ||
| 5 | Selected health professionals in the selected HCFs | UH&FPOs | 7 | 9 | 12 | 19 | 7 | 17 | 16 | 12 | 17 | 20 | 136 |
| Doctors | 8 | 17 | 14 | 22 | 21 | 31 | 25 | 16 | 25 | 23 | 202 | ||
| Nurses | 6 | 16 | 11 | 19 | 11 | 30 | 16 | 12 | 15 | 19 | 155 | ||
| Total | 21 | 42 | 37 | 60 | 39 | 78 | 57 | 40 | 57 | 62 | 493 | ||
| No | Most Severe Climate Stress Disease Name | Outbreak/Prevalence Period/Season | Reason/Caused By | South-Western Coastal Area and Sundarbans | Southeast and Eastern Coastal Area | Chattogram Hill Tracts | Rivers, Floodplains, and Erosion-Prone Areas | Haor and Flash Flood Areas | Drought-Prone and Barind Areas | Northern Northwestern Region | Chalan Beel and Low-Lying Areas of Northwestern Region | Chars and Islands | Bay of Bengal and Ocean |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SWM | SEE | CHT | FPE | HFF | DBA | NNW | CBL | CHI | BOB | ||||
| 1 | Pneumonia/RTI/ARI | Winter | Cold, respiratory droplets, air pollution | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 |
| 2 | Scabies | Summer | Contaminated water, temperature rise | 3 | 3 | 3 | 3 | 3 | |||||
| 3 | Heat stroke | Summer | Heat wave | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |||
| 4 | Cholera | Summer, rainy | Contaminated water | 2 | 2 | 2 | 2 | 2 | |||||
| 5 | Diarrhea | Summer, rainy | Contaminated water | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 |
| 6 | AWD | Summer, rainy | Flash flood, heavy rainfall | 5 | 5 | 5 | |||||||
| 7 | Hepatitis | Summer, rainy | Contaminated water and poor sanitation | 1 | 1 | 1 | 1 | 1 | |||||
| 8 | Skin diseases including tinea | Rainy | Contaminated water, insects | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | ||
| 9 | Typhoid | Rainy | Contaminated food and water | 3 | 3 | 3 | 3 | 3 | 3 | 3 | |||
| 10 | Dengue | Rainy | Vector borne (mosquitoes) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |||
| 11 | Malnutrition | All season | Protein and energy deficiency | 5 | 5 | ||||||||
| 12 | Mental health | All season | Heat wave, extreme cold | 1 | 1 | 1 | 1 | ||||||
| 13 | NCD, e.g., hypertension | All season | Salinity of water | 3 | |||||||||
| Severe | Moderate to Severe | Moderate | Mild to Moderate | Mild | |||||||||
| 5 | 4 | 3 | 2 | 1 | |||||||||
| A “severe” hospital visit was labelled as critical in terms of symptoms, which may cause significant impairment of daily activities and require thorough medical treatment while having a risk of complications or long-term health effects. | A “moderate to severe” hospital visits was denoted as needing intensive medication with medical consultancy to prevent complications. | A “moderate” severity of hospital visit was labelled as a disease with symptoms that may affect daily routine and need medical consultancy and some medication. | A “mild to moderate” severity hospital visit was defined as patients possibly needing to take primary medication to avoid the deterioration of their health condition. | A “mild” severity hospital visit was defined as patients with symptoms of a disease that are manageable, do not require immediate medication, and may improve over time even without medical consultancy or medication. | |||||||||
| No | National Level Severity Index of Hospital Visits of CSD = ∑ (Weightage of CSD)/Number of Areas (0–5) | Climate Stressed Area Wise Severity Index of Hospital Visits of CSD = ∑ (Weightage of CSD)/Number of Identified Diseases (0–5) | ||
|---|---|---|---|---|
| Disease | Index | Stressed Area | Index | |
| 1 | Diarrhea | 5 | Bay of Bangla and Ocean (BoB) | 4 |
| 2 | AWD | 5 | Chars and islands (CHI) | 4 |
| 3 | Malnutrition | 5 | Chattogram Hill tracts (CHT) | 3 |
| 4 | Pneumonia/RTI/ARI | 4 | Haor and flash flood areas (HHF) | 3 |
| 5 | Scabies | 3 | Northern northwestern region (NNW) | 3 |
| 6 | Skin diseases including tinea | 3 | Southwestern coastal area and Sundarbans (SWM) | 3 |
| 7 | Typhoid | 3 | Rivers, floodplains, and erosion-prone areas (FPE) | 3 |
| 8 | NCD, e.g., hypertension | 3 | Chalan Beel and low-lying areas of north-western region (CBL) | 3 |
| 9 | Cholera | 2 | Drought-prone and Barind areas (DBA) | 3 |
| 10 | Heat stroke | 1 | Southeast and eastern coastal area (SEE) | 2 |
| 11 | Hepatitis | 1 | ||
| 12 | Dengue | 1 | ||
| 13 | Mental health | 1 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 World Health Organization; Licensee MDPI, Basel, Switzerland. This is an open access article distributed under the terms of the Creative Commons Attribution IGO License (http://creativecommons.org/licenses/by/3.0/igo/legalcode/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any reproduction of this article there should not be any suggestion that WHO or this article endorse any specific organisation or products. The use of the WHO logo is not permitted.
Share and Cite
Kabir, A.; Alam, S.; Tarin, N.J.; Sarkar, S.; Eshofonie, A.; Sarker, M.F.R.; Rahman, A.K.S.; Shirin, T. A Study of Climate-Sensitive Diseases in Climate-Stressed Areas of Bangladesh. Climate 2025, 13, 166. https://doi.org/10.3390/cli13080166
Kabir A, Alam S, Tarin NJ, Sarkar S, Eshofonie A, Sarker MFR, Rahman AKS, Shirin T. A Study of Climate-Sensitive Diseases in Climate-Stressed Areas of Bangladesh. Climate. 2025; 13(8):166. https://doi.org/10.3390/cli13080166
Chicago/Turabian StyleKabir, Ahammadul, Shahidul Alam, Nusrat Jahan Tarin, Shila Sarkar, Anthony Eshofonie, Mohammad Ferdous Rahman Sarker, Abul Kashem Shafiqur Rahman, and Tahmina Shirin. 2025. "A Study of Climate-Sensitive Diseases in Climate-Stressed Areas of Bangladesh" Climate 13, no. 8: 166. https://doi.org/10.3390/cli13080166
APA StyleKabir, A., Alam, S., Tarin, N. J., Sarkar, S., Eshofonie, A., Sarker, M. F. R., Rahman, A. K. S., & Shirin, T. (2025). A Study of Climate-Sensitive Diseases in Climate-Stressed Areas of Bangladesh. Climate, 13(8), 166. https://doi.org/10.3390/cli13080166