

An Inventory of South African Medicinal Plants Used in the Management of Sexually Transmitted and Related Opportunistic Infections: An Appraisal and Some Scientific Evidence (1990–2020)


Abstract
1. Introduction
1.1. Sexually Transmitted Infections: Historical Context and Treatments Used
1.1.1. Western Context (Focus on Gonorrhoea)
1.1.2. African Context
1.1.3. Relationship between Sexually Transmitted Infections and HIV-AIDS
2. Results and Discussions
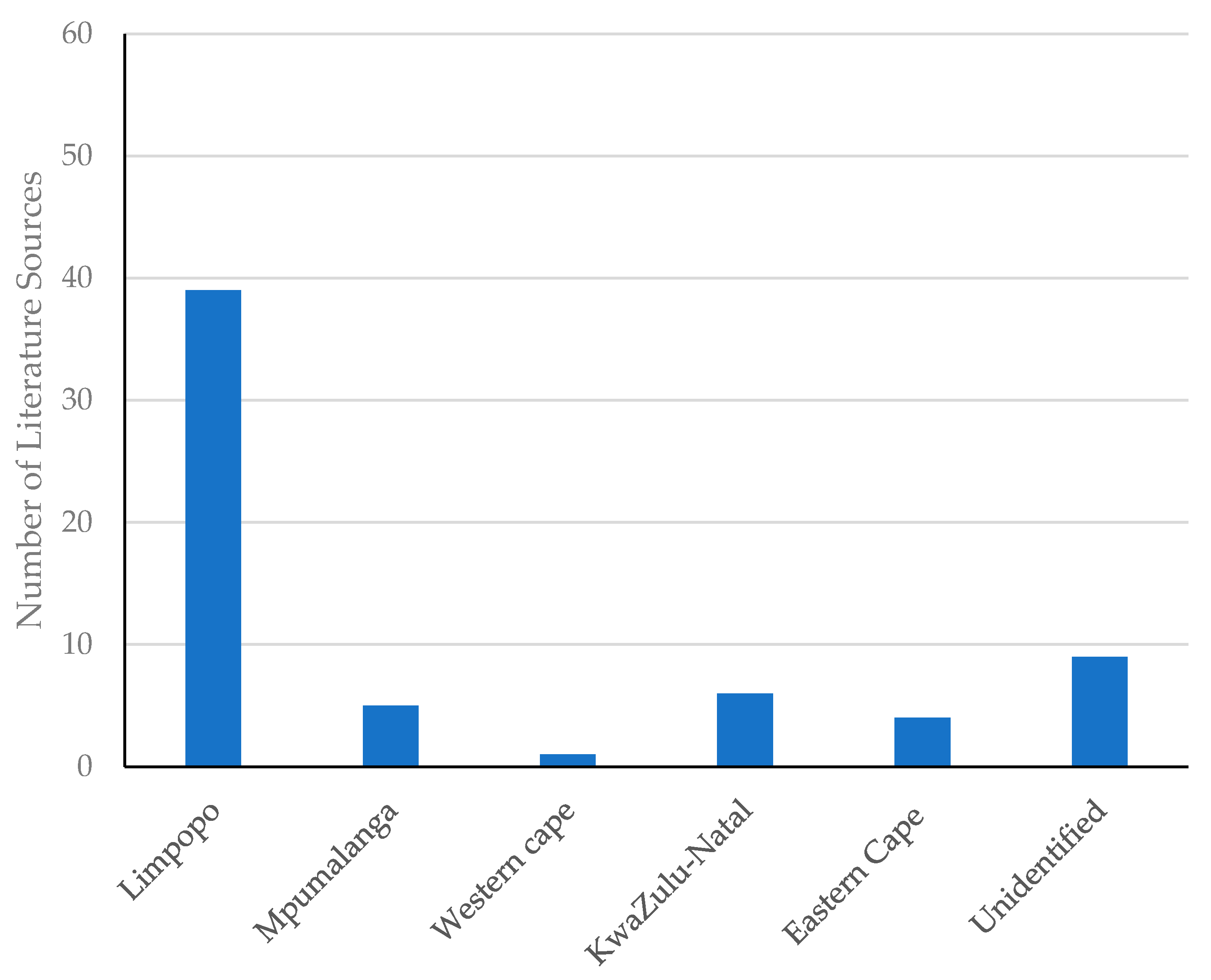
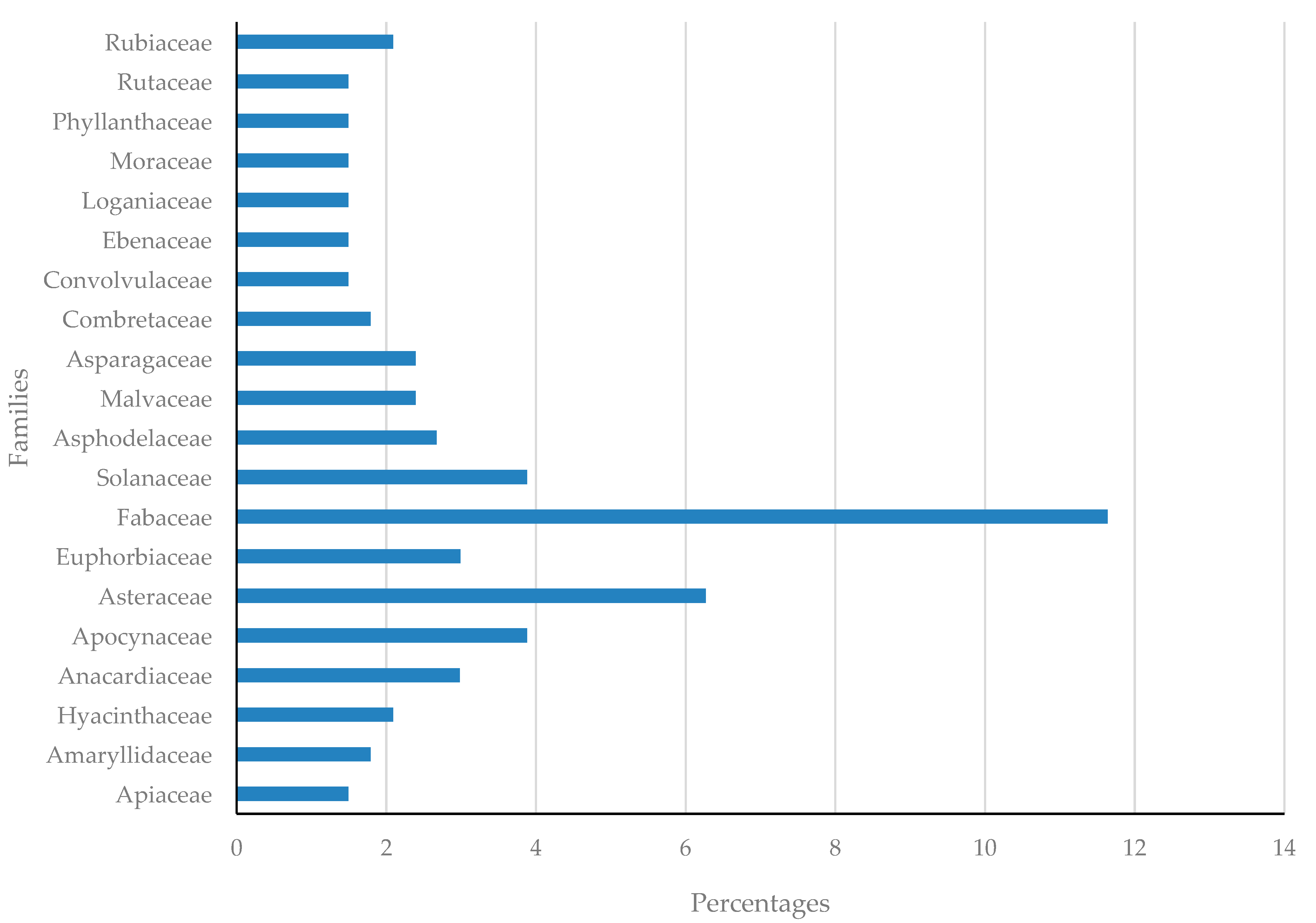
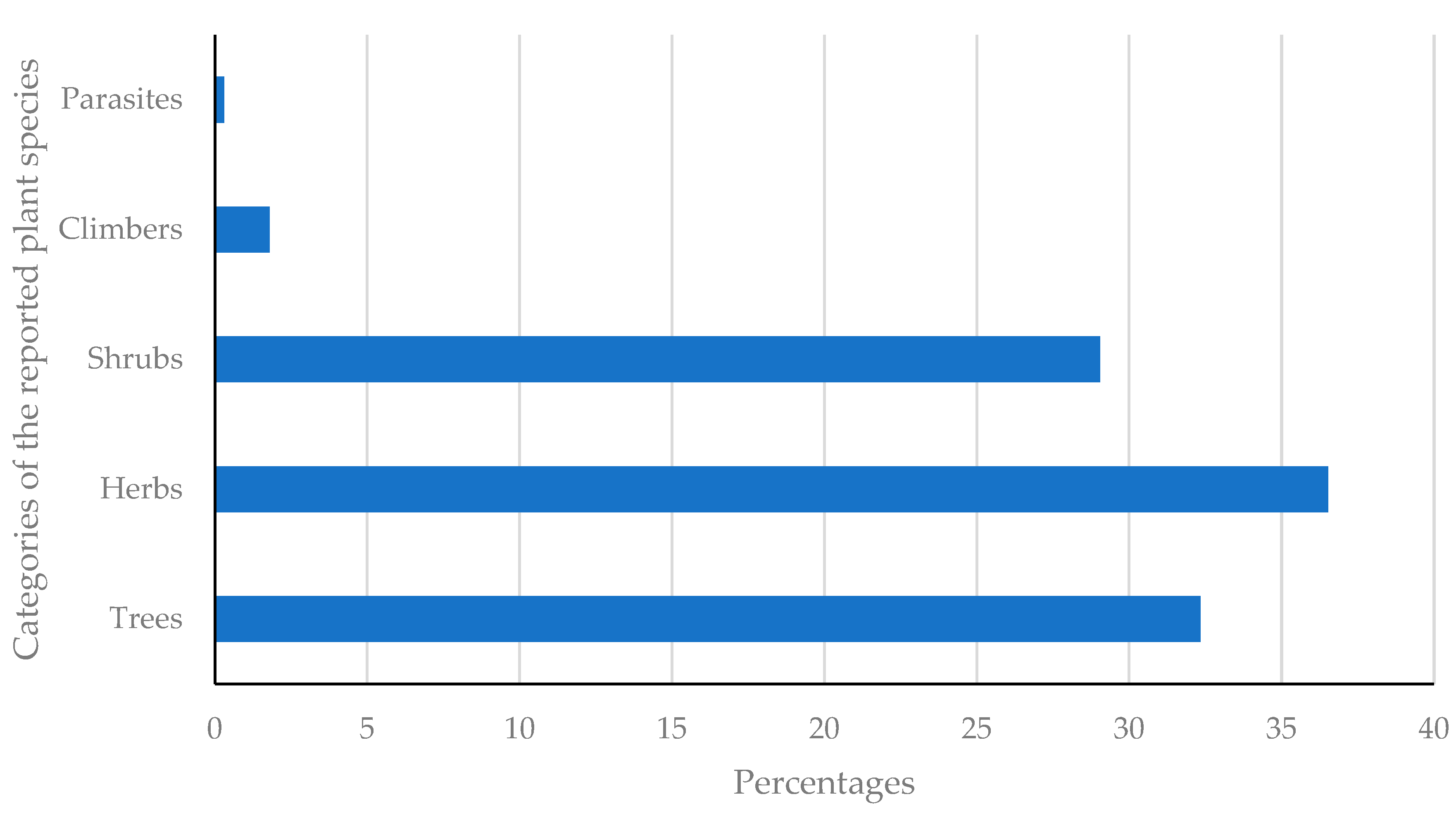
2.1. Diversity of Plant Species Used to Treat Sexually Transmitted and Related Infections
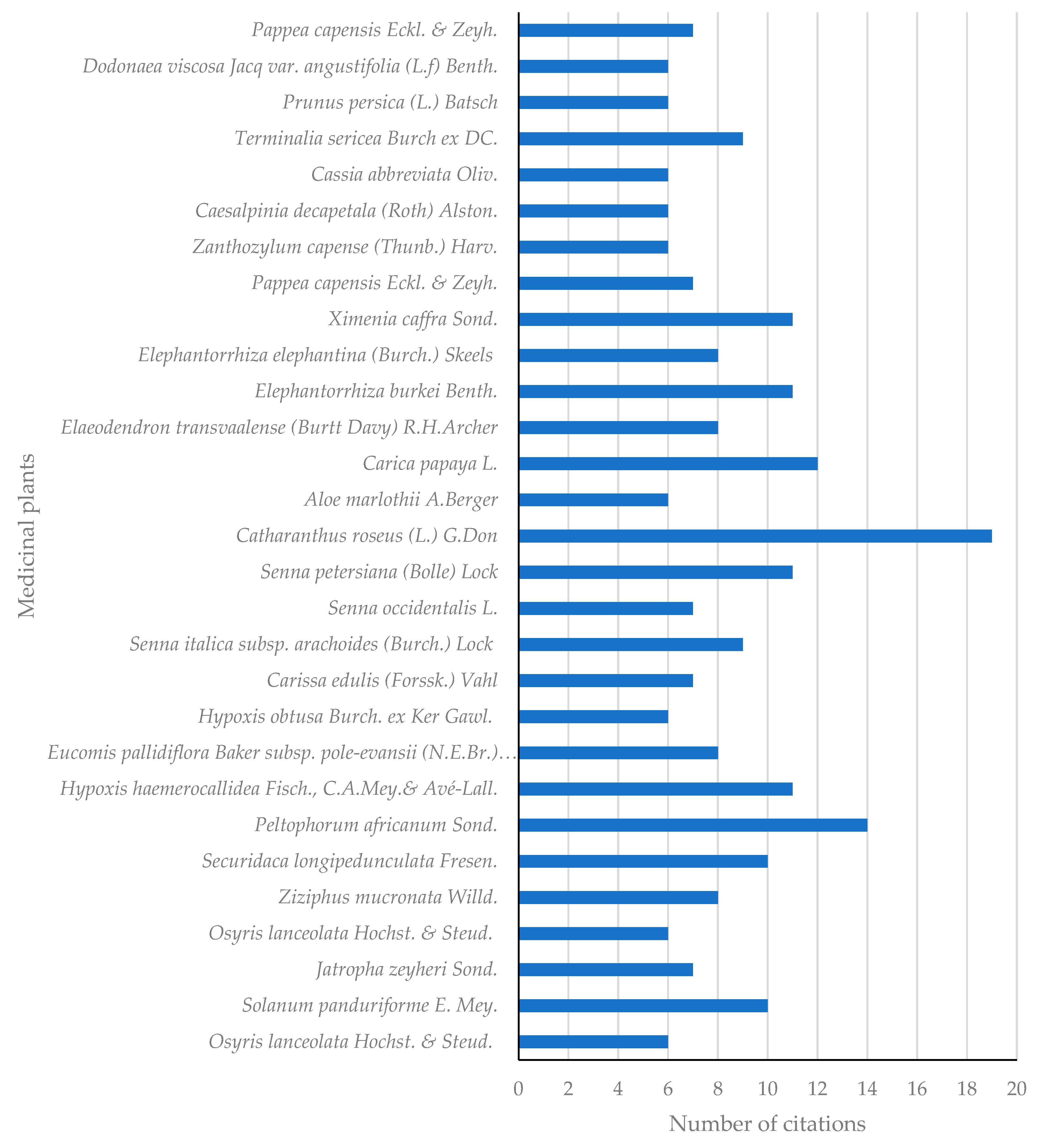
2.2. Citations of Plants Used to Treat STIs and Related Infections
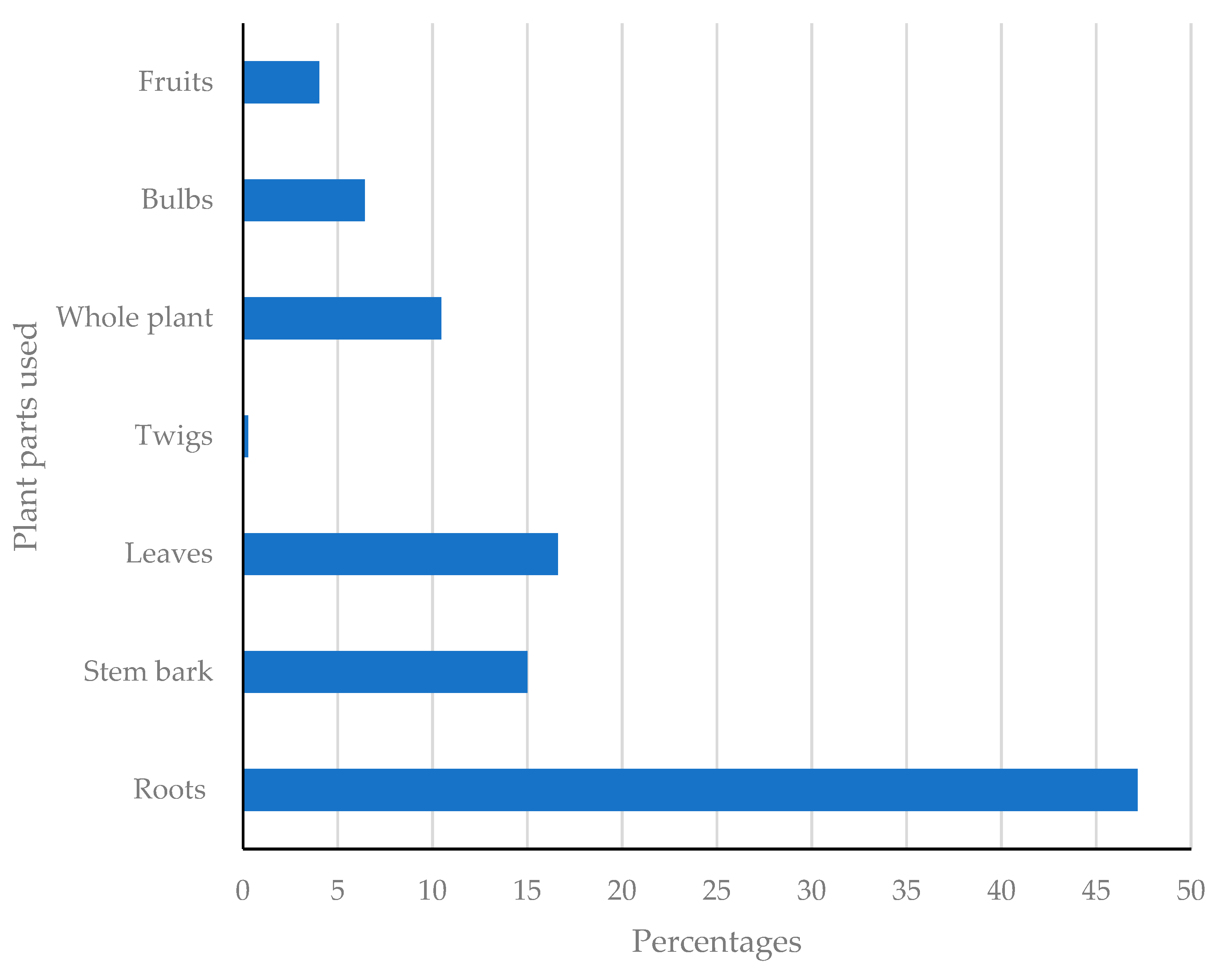
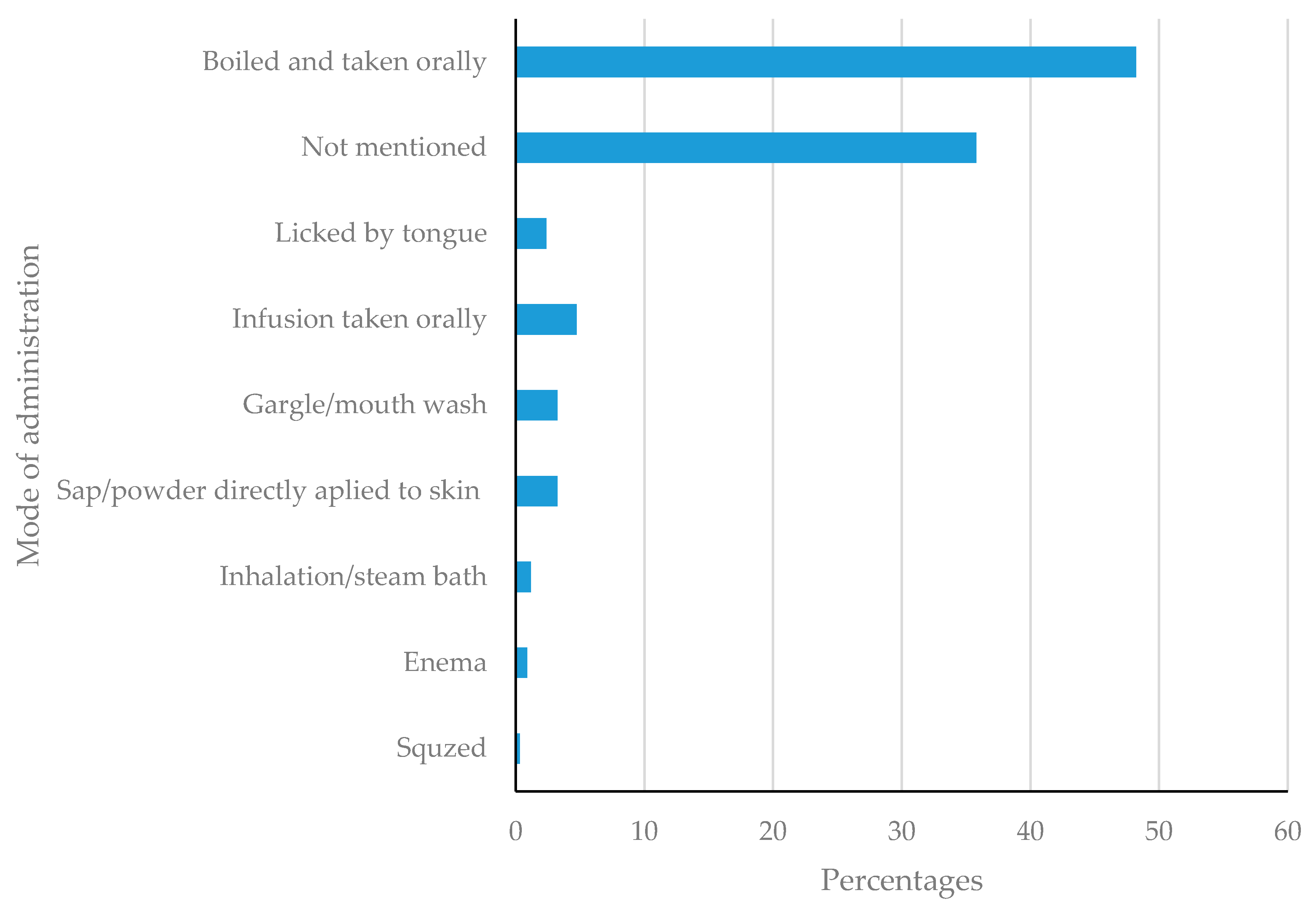
2.3. Mode of Administration and Plant Parts Used to Treat STIs and Related Infections
2.4. Relevance and Some Scientific Evidence of South African Medicinal Plants Used to Treat STIs and Related Infections
2.4.1. In Vitro Antimicrobial Activity
2.4.2. In Vitro Antiviral Activity
2.4.3. Toxicity and Clinical Trials
2.5. Plant-Based Mixtures and Products Used in Treating Sexually Transmitted and Related Infections
3. Materials and Methods
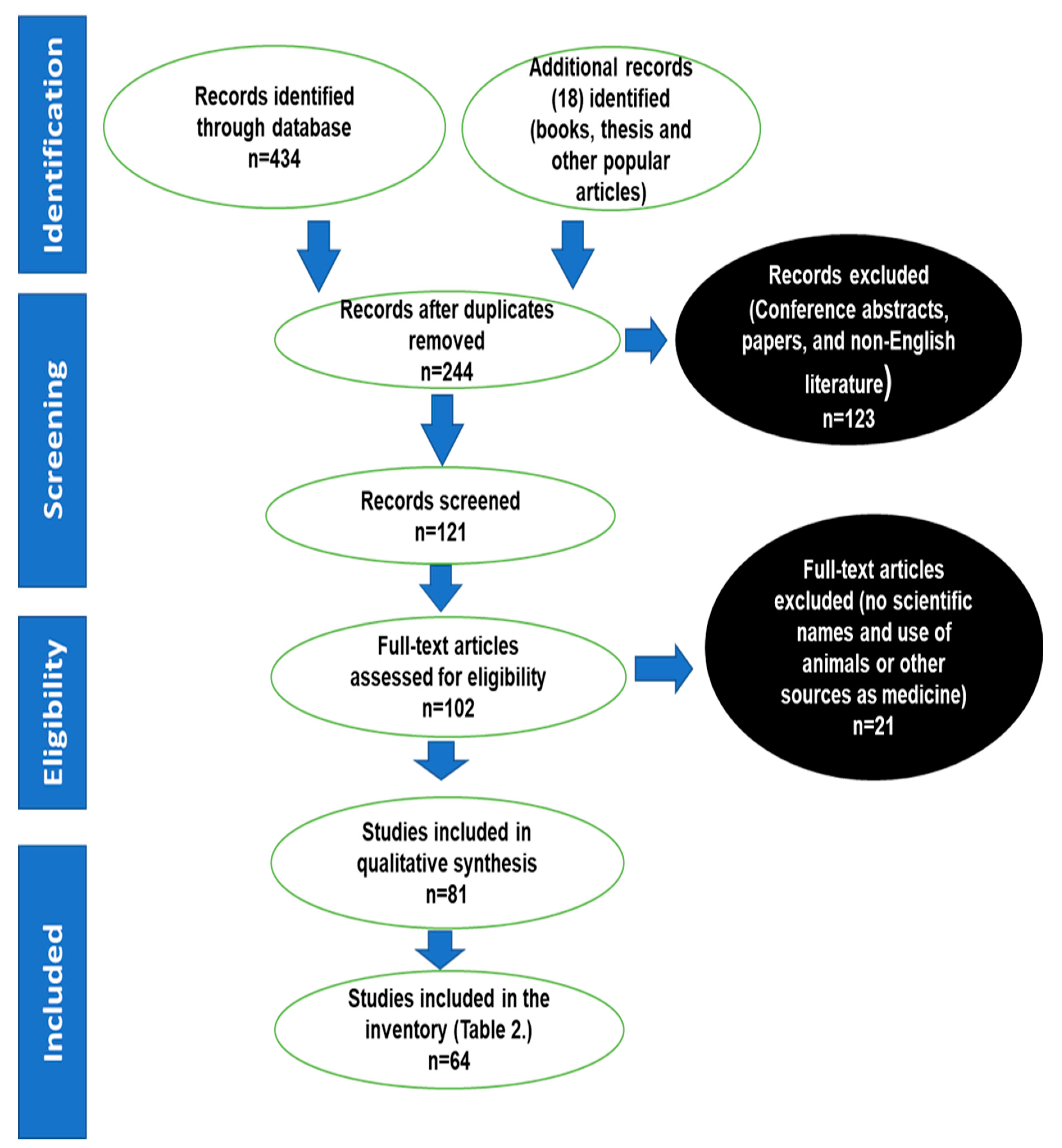
3.1. Strategy for Literature Search
3.2. Data Mining
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnson, L.F.; Dorrington, R.E.; Bradshaw, D.; Coetzee, D.J. The effect of syndromic management interventions on the prevalence of sexually transmitted infections in South Africa. Sex. Reprod. Healthc. 2011, 2, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Ventola, C.L. The antibiotic resistance crisis Part I: Causes and threats. Pharm. Ther. 2015, 40, 277–283. [Google Scholar]
- WHO, World Health Organisation STD Statistics Worldwide. Global Prevalence and Incidence of Selected Curable Sexually Transmitted Infections, Overview and Estimates. 2001. Available online: https://apps.who.int/iris/handle/10665/66818 (accessed on 12 June 2020).
- World Health Organization. Statistics about Sexually Transmitted Diseases; The World Health Report; WHO: Geneva, Switzerland, 2004. Available online: https://www.who.int/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis) (accessed on 12 June 2020).
- Tshikalange, T.E.; Meyer, J.J.M.; Hussein, A.A. Antimicrobial activity, toxicity, and isolation of a bioactive compound from plants used to treat sexually transmitted diseases. J. Ethnopharmacol. 2005, 96, 515–519. [Google Scholar] [CrossRef] [PubMed]
- Ndubani, P.; Höjer, B. Traditional healers and the treatment of sexually transmitted illnesses in rural Zambia. J. Ethnopharmacol. 1999, 67, 15–25. [Google Scholar] [CrossRef]
- Kambizi, L.; Afolayan, A.J. An ethnobotanical study of plants used for the treatment of sexually transmitted diseases (njovhera) in Guruwe District, Zimbabwe. J. Ethnopharmacol. 2001, 77, 5–9. [Google Scholar] [CrossRef]
- Gbadamosi, I.T.; Egunyomi, A. Ethnobotanical survey of plants used for the treatment and management of sexually transmitted infections in Ibadan, Nigeria. Ethnobot. Res. Appl. 2014, 12, 659–669. [Google Scholar] [CrossRef]
- Gail, H.; Tarryn, B.; Oluwaseyi, A.; Denver, D.; Oluchi, M.; Charlotte, V.K.; Joop, D.J.; Diana, G. An ethnobotanical survey of medicinal plants used by traditional health practitioners to manage HIV and its related opportunistic infections in Mpoza, Eastern Cape Province, South Africa. J. Ethnopharmacol. 2015, 171, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Chinsembu, K.C. Ethnobotanical study of medicinal flora utilized by traditional healers in the management of sexually transmitted infections in Sesheke District, Western Province, Zambia. Braz. J. Pharmacog. 2016, 26, 268–274. [Google Scholar] [CrossRef]
- Chinsembu, K.C. Ethnobotanical study of plants used in the management of HIV-AIDS-related diseases in Livingstone, Southern Province, Zambia. Evidence-Based Compl. Alt. Med. 2016, 2016, 4238625. [Google Scholar] [CrossRef]
- Chinsembu, K.C.; Syakalima, M.; Semenya, S.S. Ethnomedicinal plants used by traditional healers in the management of HIV-AIDS opportunistic diseases in Lusaka, Zambia. S. Afr. J. Bot. 2019, 122, 369–384. [Google Scholar] [CrossRef]
- Runyoro, D.K.B.; Ngassapa, O.D.; Matee, M.I.N.; Joseph, C.C.; Moshi, M.J. Medicinal plants used by Tanzanian traditional healers in the management of Candida infections. J. Ethnopharmacol. 2006, 106, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Lamorde, M.; Tabuti, J.R.S.; Obua, C.; Kukunda-Byobona, C.; Lanyero, H.; Byakika-Kibwika, P.; Sbosa, G.S.; Lubega, A.; Ogwal-Okeng, J.; Ryan, M.; et al. Medicinal plants used by traditional medicine practitioners for the treatment of HIV-AIDS and related conditions in Uganda. J. Ethnopharmacol. 2010, 130, 43–53. [Google Scholar] [CrossRef]
- Anywar, G.; Kakudidi, E.; Byamukama, R.; Mukonzo, J.; Schubert, A.; Oryem-Origa, H. Indigenous traditional knowledge of medicinal plants used by herbalists in treating opportunistic infections among people living with HIV/AIDS in Uganda. J. Ethnopharmacol. 2020, 246, 112205. [Google Scholar] [CrossRef] [PubMed]
- Otang, W.F.; Grierson, D.S.; Ndip, R.N. Ethnobotanical survey of medicinal plants used in the management of opportunistic fungal infections in HIV-AIDS patients in the Amathole District of the Eastern Cape Province, South Africa. J. Med. Plants Res. 2012, 6, 2071–20180. [Google Scholar]
- Mugisha, M.K.; Asiimwe, S.; Namutebi, A.; Borg-Karlson, A.-K.; Kakudidi, E.K. Ethnobotanical study of indigenous knowledge on medicinal and nutritious plants used to manage opportunistic infections associated with HIV-AIDS in western Uganda. J. Ethnopharmacol. 2010, 155, 194–202. [Google Scholar] [CrossRef]
- Tshikalange, T.E. The Traditional Use of Medicinal Plants to Treat Sexually Transmitted Diseases. Master’s Thesis, University of Pretoria, Pretoria, South Africa, 2002. [Google Scholar]
- Mongalo, N.I.; Makhafola, T.J. Ethnobotanical Knowledge of the Lay People of Blouberg Area (Pedi Tribe), Limpopo Province, South Africa. J. Ethnobiol. Ethnomed. 2018, 14, 46. [Google Scholar] [CrossRef]
- Pham-Kanter, G.B.T.; Steinberg, M.H.; Ballard, R.C. Sexually transmitted diseases in South Africa. Genitourin. Med. 1996, 2, 160–171. [Google Scholar] [CrossRef]
- Austin, M.N.; Beigi, R.H.; Meyn, L.A.; Hillier, S.L. Microbiologic response to treatment of bacterial vaginosis with topical clindamycin or metronidazole. J. Clin. Microbiol. 2005, 43, 4492–4497. [Google Scholar] [CrossRef]
- Jose, P.P.; Vivekanandan, V.; Sobhanakumari, K. Gonorhoea: Historical outlook. J. Skin Sex. Trans. Dis. 2020, 2, 110–114. [Google Scholar]
- Tan, S.Y.; Tatsumura, Y. Alexander Fleming (1881–1955): Discoverer of penicillin P. Singap. Med. J. 2015, 56, 366–367. [Google Scholar] [CrossRef]
- Theuretzbacher, U. Global antimicrobial resistance in gram-negative pathogens and clinical needs. Curr. Opin. Microbiol. 2017, 39, 106–112. [Google Scholar] [CrossRef]
- Chandra, H.; Bishnoi, P.; Yadav, A.; Patni, B.; Mishra, A.P.; Nautiyal, A.R. Antimicrobial resistance, and the alternative resources with special emphasis on plant-based antimicrobials—A review. Plants 2017, 6, 16. [Google Scholar] [CrossRef]
- Tadesse, B.T.; Ashley, E.A.; Ongarello, S.; Havumaki, J.; Wijegoonewardena, M.; González, I.J.; Dittrich, S. Antimicrobial resistance in Africa: A systematic review. BMC Infect. Dis. 2017, 17, 616. [Google Scholar] [CrossRef]
- Gurib-Fakim, A. Medicinal plants: Traditions of yesterday and drugs of tomorrow. Mol. Asp. Med. 2006, 27, 1–93. [Google Scholar] [CrossRef]
- Nthulane, N.P.; Mosebi, S.; Tshikalange, T.E.; Nyila, M.A.; Mankga, L.T. Antimicrobial and anti-inflammatory activities of selected medicinal plants against pathogens causing sexually transmitted infections. Herb. Med. 2020, 92, 130–137. [Google Scholar] [CrossRef]
- Magee, A.R.; Van Wyk, A.-E.; Van Vuuren, S.F. Ethnobotany, and antimicrobial activity of sieketroos. S. Afr. J. Bot. 2007, 77, 159–162. [Google Scholar] [CrossRef]
- Hiraral, K. Indian family businesses in Natal, 1870–1950. Natalia 2008, 38, 27–37. [Google Scholar]
- Williams, V.L.; Wojtasika, E.M.; Byrne, M.J. A chronicle of alien medicinal plants used as traditional medicine in South Africa, and their status as invasive species. S. Afr. J. Bot. 2021, 143, 63–72. [Google Scholar] [CrossRef]
- Dufaur, L.; Matin, N. Important opportunistic infections in HIV. Medicine 2018, 46, 352–355. [Google Scholar] [CrossRef]
- Rebbapragada, A.; Kaul, R. More than their sum in your parts: The mechanisms that underpin the mutually advantageous relationship between HIV and sexually transmitted infections. Drug Discov. Today Disease Mechan. 2007, 4, 237–246. [Google Scholar] [CrossRef]
- McMichael, A.J.; Borrow, P.; Tomaras, G.D.; Goonetilleke, N.; Haynes, B.F. The immune response during acute HIV-1 infection: Clues for vaccine development. Nat. Rev. Immunol. 2010, 10, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Kaur, R.; Dhakad, M.S.; Goyal, R.; Bhalla, P.; Dewan, R. Spectrum of opportunistic fungal infections in HIV/AIDS patients in tertiary care hospital in India. Can. J. Infect. Dis. Med. Microbiol. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Vega, L.E.; Espinoza, L.R. Human Immunodeficiency Virus infection (HIV)-associated rheumatic manifestations in the pre- and post-HAART eras. Clin. Rheumatol. 2020, 39, 2515–2522. [Google Scholar] [CrossRef] [PubMed]
- Hutchings, A.; Scott, H.; Lewis, G.; Cunningham, A.B. Zulu Medicinal Plants: An Inventory; University of Natal Press: Pietermaritzburg, South Africa, 1996. [Google Scholar]
- Buwa, L.V.; Van Staden, J. Antibacterial and antifungal activity of traditional medicinal plants used against venereal diseases in South Africa. J. Ethnopharmacol. 2006, 103, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Buwa, L.V. Biological Activity of Traditional Medicinal Plants Used against Venereal Diseases in South Africa. Ph.D. Thesis, University of KwaZulu-Natal, Pietermaritzburg, South Africa, 2006. [Google Scholar]
- Chauke, M.A.; Shai, L.J.; Mogale, M.A.; Tshisikhawe, M.P.; Mokgotho, M.P. Medicinal plant use of villagers in the Mopani district, Limpopo province, South Africa. Afr. J. Trad. Compl. Alt. Med. 2015, 12, 9–26. [Google Scholar] [CrossRef]
- Corrigan, B.M.; Van Wyk, B.-E.; Geldenhuys, C.J.; Jardine, J.M. Ethnobotanical plant uses in the KwaNibela Peninsula, St. Lucia, South Africa. S. Afr. J. Bot. 2011, 77, 346–359. [Google Scholar] [CrossRef]
- De Beer, J.J.J.; Van Wyk, A.-E. An ethnobotanical survey of the Agter-Hantam, Northern Cape Province, South Africa. S. Afr. J. Bot. 2011, 77, 741–751. [Google Scholar] [CrossRef]
- De Wet, H.; Nzama, V.N.; Van Vuuren, S.F. Medicinal plants used for the treatment of sexually transmitted infections by lay people in Northern Maputaland, KwaZulu-Natal Province, South Africa. S. Afr. J. Bot. 2012, 78, 12–20. [Google Scholar] [CrossRef]
- Erasmus, L.J.C.; Potgieter, M.J.; Semenya, S.S.; Lennox, S.J. Phytomedicine versus Gonorrhoea: The Bapedi experience. Afr. J. Tradit. Complement Alt. Med. 2012, 9, 591–598. [Google Scholar] [CrossRef]
- Erasmus, L.J.C.; Potgieter, M.J.; Semenya, S.S. Erectile dysfunction: Definition and materia medica of Bapedi traditional healers in Limpopo Province, South Africa. J. Med. Plants Res. 2015, 9, 71–77. [Google Scholar]
- Fadipe, V.O.; Mongalo, N.I.; Opoku, A.R. In Vitro evaluation of the comprehensive antimicrobial and antioxidant properties of Curtisia dentata (Burm.f) C.A. Sm: Toxicological effect on the Human Embryonic Kidney (HEK293) and Human Hepatocellular carcinoma (HepG2) cell lines. Exp. Clin. Scie. J. 2015, 14, 971–983. [Google Scholar]
- Fadipe, V.O.; Mongalo, N.I.; Opoku, A.R.; Dikhoba, P.M.; Makhafola, T.J. Isolation of anti-mycobacterial compounds from Curtisia dentata (Burm.f.) C.A.Sm Curtisiaceae. BMC Compl. Alt. Med. 2017, 17, 306. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, L.; Van Rensburg, C.E.J.; Hoosen, A.A.; Steenkamp, V. In vitro activity medicinal plants of the Venda region, South Africa, against Trichomonas vaginalis. S. Afr. J. Epidemiol. Infect. 2008, 23, 26–28. [Google Scholar]
- Mabogo, D.E.N. The Ethnobotany of the VhaVenda. Master’s Thesis, University of Pretoria, Pretoria, South Africa, 1990. [Google Scholar]
- Maema, L.P.; Potgieter, M.J.; Samie, A. Ethnobotanical survey of invasive alien plant species used in the treatment of sexually transmitted infections in Waterberg District, South Africa. S. Afr. J. Bot. 2019, 122, 391–400. [Google Scholar] [CrossRef]
- Maema, L.P.; Potgieter, M.J.; Samie, A. Data set on preliminary phytochemical analysis and antioxidant activity of selected invasive alien plant species used in the treatment of sexually transmitted infections in Waterberg District, South Africa. Data Brief 2019, 25, 104281. [Google Scholar] [CrossRef] [PubMed]
- Magwede, K. A Quantitative Survey of the Traditional Plant Use of VhaVenda, Limpopo Province, South Africa. Ph.D. Thesis, University of Johannesburg, Johannesburg, South Africa, 2018. [Google Scholar]
- Mahwasane, S.T.; Middleton, L.; Boaduo, N. An ethnobotanical survey of indigenous knowledge on medicinal plants used by the traditional healers of the Lwamondo area, Limpopo Province, South Africa. S. Afr. J. Bot. 2013, 88, 69–75. [Google Scholar] [CrossRef]
- Maposa, S.; Afolayan, A.J.; Otunola, G.A. Evaluation of the antimicrobial properties of Vachellia karroo Hayne Banfi and Galasso pods used traditionally for the treatment of venereal diseases. Int. J. Pharmacol. 2019, 15, 772–776. [Google Scholar] [CrossRef]
- Maroyi, A.; Mosina, G.K.E. Medicinal plants and traditional practices in peri-urban domestic gardens of the Limpopo Province, South Africa. Indian J. Trad. Knowl. 2014, 13, 665–672. [Google Scholar]
- Masevhe, N.A.; McGaw, L.J.; Eloff, J.N. The traditional use of plants to manage candidiasis and related infections in Venda, South Africa. J. Ethnopharmacol. 2015, 168, 364–372. [Google Scholar] [CrossRef]
- Masevhe, N.A. Isolation and Characterization of Antifungal Compounds from Clerodendron Glabrum var Glabrum (Verbenaceae) Used Traditionally to Treat Candidiasis in Venda, South Africa. Ph.D. Thesis, University of Pretoria, Pretoria, South Africa, 2013. [Google Scholar]
- Mathibela, K.M.; Potgieter, M.J.; Tshikalange, T.E. Medicinal plants used to manage sexually transmitted infections by Bapedi traditional health practitioners in the Blouberg area, South Africa. S. Afr. J. Bot. 2019, 122, 385–390. [Google Scholar] [CrossRef]
- Mbambala, S.G.; Tshisikhawe, M.P.; Masevhe, N.A. Invasive alien plants used in the treatment of HIV-AIDS-related symptoms by traditional healers of Vhembe Municipality, Limpopo Province, South Africa. Afr. J. Trad. Compl. Alt. Med. 2017, 14, 80–88. [Google Scholar] [CrossRef]
- Mbanjwa, S.G. A Quantitative Ethnobotanical Survey of the Ixopo Area of KwaZulu-Natal, South Africa. Master’s Thesis, University of Johannesburg, Johannesburg, South Africa, 2020. [Google Scholar]
- Mhlongo, L.S.; Van Wyk, B.-E. Zulu medicinal ethnobotany: New records from the Amandawe area of KwaZulu-Natal, South Africa. S. Afr. J. Bot. 2019, 122, 266–290. [Google Scholar] [CrossRef]
- Moeng, T.E. An Investigation into the Trade of Medicinal Plants by Muthi Shops and Street Vendors in the Limpopo Province, South Africa. Master’s Thesis, University of Limpopo, Sovenga, Polokwane, South Africa, 2010. [Google Scholar]
- Mhlongo, L.S. The Medicinal Ethnobotany of the Amandawe Area in KwaCele, KwaZulu-Natal, South Africa. Master’s Thesis, University of Johannesburg, Johannesburg, South Africa, 2019. [Google Scholar]
- Mogale, M.M.P.; Raimondo, D.C.; Van Wyk, B.-E. The Ethnobotany of Central Sekhukhuneland, South Africa. S. Afr. J. Bot. 2019, 122, 90–119. [Google Scholar] [CrossRef]
- Mongalo, N.I. Antibacterial Activities of Selected Medicinal Plants Used to Treat Sexually Transmitted Infections in Blouberg area, Limpopo Province. Master’s Thesis, University of Zululand, Richards Bay, South Africa, 2013. [Google Scholar]
- Mongalo, N.I.; McGaw, L.J.; Finnie, J.F.; Van Staden, J. Pharmacological properties of extracts from six South African medicinal plants used to treat sexually transmitted infections (STIs) and related infections. S. Afr. J. Bot. 2017, 112, 290–295. [Google Scholar] [CrossRef]
- Mulaudzi, R.B.; Ndhlala, A.R.; Kulkarni, M.G.; Finnie, J.F.; Van Staden, J. Antimicrobial properties and phenolic contents of medicinal plants used by the Venda people for conditions related to venereal diseases. J. Ethnopharmacol. 2011, 135, 330–337. [Google Scholar] [CrossRef]
- Mulaudzi, R.B.; Ndhlala, A.R.; Kulkarni, M.G.; Finnie, J.F.; Van Staden, J. Anti-inflammatory and mutagenic evaluation of medicinal plants used by Venda people against venereal and related infections. J. Ethnopharmacol. 2013, 146, 173–179. [Google Scholar] [CrossRef]
- Mulaudzi, R.B. Pharmacological Evaluation of Medicinal Plants Used by Venda People against Venereal and Related Diseases. Ph.D. Thesis, University of KwaZulu-Natal, Pietermaritzburg, South Africa, 2012. [Google Scholar]
- Mulaudzi, R.B.; Ndhlala, A.R.; Van Staden, J. Ethnopharmacological evaluation of a traditional herbal remedy used to treat gonorrhoea in Limpopo province, South Africa. S. Afr. J. Bot. 2015, 97, 117–122. [Google Scholar] [CrossRef]
- Naidoo, D.; Van Vuuren, S.F.; Van Zyl, R.L.; De Wet, H. Plants traditionally used individually and in combination to treat sexually transmitted infections in northern Maputaland, South Africa: Antimicrobial activity and cytotoxicity. J. Ethnopharmacol. 2013, 149, 656–667. [Google Scholar] [CrossRef]
- Rankoana, S.A. The Use of Indigenous Knowledge for Primary Health Care among the Northern Sotho in the Limpopo Province. Ph.D. Thesis, University of Limpopo, Turfloop Campus, Polokwane, South Africa, 2012. [Google Scholar]
- Rasekgala, M.T. The Ethnoecological Assessment of Cassia abbreviata Oliv. at Matsa village, Limpopo Province, South Africa. Master’s Thesis, University of Venda, Thohoyandou, South Africa, 2017. [Google Scholar]
- Rasethe, M.T.; Semenya, S.S.; Maroyi, A. Medicinal plants traded in informal herbal medicine markets of the Limpopo Province. Evid. Based Compl. Alt. Med. 2019, 2019. [Google Scholar] [CrossRef]
- Samie, A.; Tambani, T.; Harshfield, E.; Green, E.; Ramalivhana, J.N.; Bessong, P.O. Antifungal activities of selected Venda medicinal plants against Candida albicans, Candida krusei and Cryptococcus neoformans isolated from South African AIDS patients. Afr. J. Biotechnol. 2010, 9, 2965–2976. [Google Scholar]
- Semenya, S.S.; Potgieter, M.J. Catharanthus roseus (L.) G. Don.: Extraordinary Bapedi medicinal herb for gonorrhoea. J. Med. Plants Res. 2013, 7, 1434–1438. [Google Scholar]
- Semenya, S.; Potgieter, M.; Tshisikhawe, M.; Shava, S.; Maroyi, A. Medicinal utilisation of exotic plants by Bapedi traditional healers to treat human ailments in Limpopo Province, South Africa. J. Ethnopharmacol. 2012, 144, 646–655. [Google Scholar] [CrossRef] [PubMed]
- Semenya, S.S.; Potgieter, M.J.; Erasmus, L.J.C. Exotic and indigenous problem plants species used by the Bapedi to treat sexually transmitted infections in Limpopo Province, South Africa. Afr. Health Scie. 2013, 13, 320–326. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Semenya, S.S.; Potgieter, M.J.; Erasmus, L.J.C. Indigenous plant species used by Bapedi healers to treat sexually transmitted infections: Their distribution, harvesting, conservation and threats. S. Afr. J. Bot. 2013, 87, 66–75. [Google Scholar] [CrossRef]
- Semenya, S.S.; Maroyi, A.; Potgieter, M.J.; Erasmus, L.J.C. Herbal medicines used by Bapedi traditional healers to treat reproductive ailments in the Limpopo Province, South Africa. Afr. J. Trad. Compl Alt. Med. 2013, 10, 331–339. [Google Scholar] [CrossRef]
- Semenya, S.S.; Potgieter, M.J.; Tshisikhawe, M.P. Use, conservation, and present availability status of ethnomedicinal plants of Matebele-village in the Limpopo Province, South Africa. Afr. J. Biotechnol. 2013, 12, 2392–2405. [Google Scholar]
- Semenya, S.S.; Potgieter, M.J.; Erasmus, L.J. Bapedi phytomedicine and their use in the treatment of sexually transmitted infections in Limpopo Province, South Africa. Afr. J. Pharm. Pharmacol. 2013, 7, 250–262. [Google Scholar] [CrossRef]
- Shai, L.J.; Chauke, M.A.; Magano, S.R.; Mogale, A.M.; Eloff, J.N. Antibacterial activity of sixteen plant species from Phalaborwa, Limpopo Province, South Africa. J. Med. Plants Res. 2013, 7, 1899–1906. [Google Scholar]
- Shai, K.N.; Ncama, K.; Ndhlovu, P.T. An exploratory study on the diverse uses and benefits of locally sourced fruit species in three villages of Mpumalanga Province, South Africa. Foods 2020, 9, 1581. [Google Scholar] [CrossRef]
- Tlakula, P.K. Ethnobotanical Survey and Conservation of Medicinal Plants Used by Local People Thulamela Municipality, Limpopo Province. Master’s Thesis, University of Pretoria, Pretoria, South Africa, 2016. [Google Scholar]
- Tshikalange, T.E.; Mamba, P.; Adebayo, S.A. Antimicrobial, antioxidant, and cytotoxicity studies of medicinal plants used in the treatment of sexually transmitted infections. Int. J. Pharmacog. Phytochem Res. 2016, 8, 1891–1895. [Google Scholar]
- Tshikalange, T.E.; Mophuting, B.C.; Mahore, J.; Winterboer, S.; Lall, N. An Ethnobotanical Study of Medicinal Plants Used in Villages under Jongilanga Tribal council, Mpumalanga, South Africa. Afr. J. Tradit. Complement. Altern. Med. 2016, 13, 83–89. [Google Scholar] [CrossRef]
- Van Vuuren, S.F.; Naidoo, D. An antimicrobial investigation of plants used traditionally in southern Africa to treat sexually transmitted infections. J. Ethnopharmacol. 2010, 130, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Van Wyk, B.-E.; Van Oudtshoorn, B.; Gericke, N. Medicinal Plants of South Africa, 1st ed.; Fourth Impression; Briza Publications: Pretoria, South Africa, 2005. [Google Scholar]
- Van Wyk, B.-E.; Van Oudtshoorn, B.; Gericke, N. Medicinal Plants of South Africa, 1st ed.; Second Impression; Briza Publications: Pretoria, South Africa, 2013. [Google Scholar]
- Van Wyk, B.-E.; De Wet, H.; Van Heerden, F.R. A review of Khoisan and Cape Dutch medical ethnobotany. J. Ethnopharmacol. 2008, 119, 331–341. [Google Scholar] [CrossRef]
- Van Wyk, B.-E.; de Wet, H.; Van Heerden, F.R. An ethnobotanical survey of medicinal plants in the south-eastern Karoo, South Africa. S. Afr. J. Bot. 2008, 74, 696–704. [Google Scholar] [CrossRef]
- Van Wyk, B.-E. A broad review of commercially important southern African medicinal plants. J. Ethnopharmacol. 2011, 119, 342–355. [Google Scholar] [CrossRef] [PubMed]
- Venter, F.; Venter, J.-A. Making the Most of Indigenous Trees, 2nd ed.; Fourth Impression; Briza Publications: Pretoria, South Africa, 2009. [Google Scholar]
- Thring, T.S.A.; Weitz, F.M. Medicinal plant use in the Bredasdorp/Elim region of the Southern Overberg in the Western Cape Province of South Africa. J. Ethnopharmacol. 2006, 103, 261–275. [Google Scholar] [CrossRef]
- Van Wyk, B.E. A family-level floristic inventory and analysis of medicinal plants used in traditional African medicine. J. Ethnopharmacol. 2020, 249, 112351. [Google Scholar] [CrossRef]
- Amen, Y.M.; Marzouk, A.M.; Zaghloul, M.G.; Afifi, M.S. The genus Machaerium (Fabaceae): Taxonomy, phytochemistry, traditional uses and biological activities. Nat. Prod. Res. 2015, 29, 1388–1405. [Google Scholar] [CrossRef]
- Macêdo, N.S.; Silveira, Z.S.; Bezerra, A.H.; Costa, J.; Coutinho, H.; Romano, B.; Capasso, R.; Cunha, F.; da Silva, M.V. Caesalpinia ferrea C. Mart. (Fabaceae) Phytochemistry, Ethnobotany, and Bioactivities: A Review. Molecules 2020, 25, 3831. [Google Scholar] [CrossRef]
- Aremu, A.O.; Pendota, S. Medicinal plants for mitigating pain and inflammatory-related conditions: An appraisal of ethnobotanical uses and patterns in South Africa. Front. Pharmacol. 2021, 12, 75858. [Google Scholar] [CrossRef]
- Klopper, R.R.; Hamer, M.; Steenkamp, Y.; Smith, G.; Crouch, N.R. Richest of the rich: South Africa’s biodiversity treasure trove. Quest 2010, 6, 20–23. [Google Scholar]
- Mongalo, N.I. Peltophorum africanum Sond [Mosetlha]: A review of its ethnomedicinal uses, toxicology, phytochemistry and pharmacological activities. J. Med. Plants Res. 2013, 7, 3484–3491. [Google Scholar]
- Mazimba, O. Pharmacology and phytochemistry studies in Peltophorum africanum. Bull. Fac. Pharm. Cairo Univ. 2014, 52, 145–153. [Google Scholar] [CrossRef]
- Balogun, F.O.; Ashafa, A.O. A review of plants used in South African traditional medicine for the management and treatment of hypertension. Planta Med. 2019, 85, 312–334. [Google Scholar] [CrossRef]
- Van Vuuren, S.F.; Frank, L. Review: Southern African medicinal plants used as blood purifiers. J. Ethnopharmacol. 2020, 249, 112434. [Google Scholar] [CrossRef] [PubMed]
- DeNegre, A.A.; Ndeffo Mbah, M.L.; Myers, K.; Fefferman, N.H. Emergence of antibiotic resistance in immunocompromised host populations: A case study of emerging antibiotic resistant tuberculosis in AIDS patients. PLoS ONE 2019, 14, e0212969. [Google Scholar] [CrossRef] [PubMed]
- Matowa, P.R.; Gundidza, M.; Gwanzura, L. A survey of ethnomedicinal plants used to treat cancer by traditional medicine practitioners in Zimbabwe. BMC Complement Med. Ther. 2020, 20, 278. [Google Scholar] [CrossRef]
- Rashid, S.; Ahmad, M.; Zafar, M.; Sultana, S.; Ayub, M.; Khan, M.A.; Yaseen, G. Ethnobotanical survey of medicinally important shrubs and trees of Himalayan region of Azad Jammu and Kashmir, Pakistan. J. Ethnopharmacol. 2015, 166, 340–351. [Google Scholar] [CrossRef]
- Tugume, P.; Kakudidi, E.K.; Buyinza, M.; Namaalwa, J.; Kamatenesi, M.; Mucunguzi, P.; Kalema, J. Ethnobotanical survey of medicinal plant species used by communities around Mabira Central Forest Reserve, Uganda. J. Ethnobiol. Ethnomed. 2016, 12, 5. [Google Scholar] [CrossRef]
- Desai, N.C.; Maheta, A.S.; Rajpara, K.M.; Joshi, V.V.; Vaghani, H.V.; Satodiya, H.M. Green synthesis of novel quinoline based imidazole derivatives and evaluation of their antimicrobial activity. J. Saudi Chem. Soc. 2014, 18, 963–971. [Google Scholar] [CrossRef]
- Martini, N.D.; Katerere, D.R.P.; Eloff, J.N. Seven bioactive flavonoids isolated from Combretum erythrophyllum (Combretaceae). S. Afr. J. Bot. 2004, 70, 310–312. [Google Scholar] [CrossRef]
- Bussmann, R.W.; Malca-García, G.; Glenn, A.; Sharon, D.; Chait, G.; Díaz, D.; Pourmand, K.; Jonat, B.; Somogy, S.; Guardado, G.; et al. Minimum inhibitory concentrations of medicinal plants used in Northern Peru as antibacterial remedies. J. Ethnopharmacol. 2010, 132, 101–108. [Google Scholar] [CrossRef]
- Mongalo, N.I. Isolation, and Characterization of Bioactive Compounds from Six South African Medicinal Plants Used in the Treatment of Sexually Transmitted and Related Infections. Ph.D. Thesis, University of KwaZulu-Natal, Pietermaritzburg, South Africa.
- Mongalo, N.I.; McGaw, L.J.; Finnie, J.F.; Van Staden, J. Isolation, and characterization of antimicrobial and anti-inflammatory activity triterpenoids from the acetone extract of Grewia flava DC. (Malvaceae). S. Afr. J. Bot. 2022, 149, 87–95. [Google Scholar] [CrossRef]
- Okoye, E.I.; Mbah, F. Effects of crude solvent extracts of flower and stalk of male Carica papaya (paw paw) on ten pathogenic bacteria. Pharm. Chem. J. 2016, 4, 186–191. [Google Scholar]
- Mamabolo, M.P.; Muganza1, F.M.; Olivier, M.T.; Olaokun, O.O.; Nemutavhanani, L.D. Evaluation of antigonorrhea activity and cytotoxicity of Helichrysum caespititium (DC) Harv. whole plant extracts. Biol. Med. 2018, 10, 1000422. [Google Scholar] [CrossRef]
- Seleteng-Kose, S.; Moteetee, A.; Van Vuuren, S. Medicinal plants used for the treatment of sexually transmitted infections in the Maseru District, Lesotho: Antimicrobial validation, phytochemical and cytotoxicity studies. S. Afr. J. Bot. 2019, 122, 457–466. [Google Scholar] [CrossRef]
- Kambizi, L.; Afolayan, A.J. Extracts from Aloe ferox and Withania somnifera inhibit Candida albicans and Neisseria gonorrhea. Afr. J. Biotech. 2008, 7, 12–15. [Google Scholar]
- Mills, E.; Cooper, C.; Seely, D.; Kanfer, I. African herbal medicines in the treatment of HIV: Hypoxis and Sutherlandia. An overview of evidence and pharmacology. Nutr. J. 2005, 4, 19. [Google Scholar] [CrossRef]
- Fasinu, P.S.; Gutmann, H.; Schiller, H.; Bouic, P.J.; Rosenkranz, B. The potential of Hypoxis hemerocallidea for herb-drug interaction. Pharm. Biol. 2013, 51, 1499–1507. [Google Scholar] [CrossRef]
- Prinsloo, G.; Marokane, C.K.; Street, R.A. Anti-HIV activity of southern African plants: Current developments, phytochemistry and future research. J. Ethnopharmacol. 2018, 21, 133–155. [Google Scholar]
- Theo, A.; Masebe, T.; Suzuki, Y.; Kikuchi, H.; Wada, S.; Obi, C.L.; Bessong, P.O.; Usuzawa, M.; Oshima, Y.; Hattori, T. Peltophorum africanum, A traditional medicinal plant, contains an anti-HIV-1 constituent, betulinic acid. Tohoku J. Exp. Med. 2009, 217, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Khlebnicova, T.S.; Piven, Y.A.; Lakhvich, F.A.; Sorokina, I.V.; Frolova, T.S.; Baev, D.S.; Tolstikova, T.G. Betulinic Acid-Azaprostanoid Hybrids: Synthesis and Pharmacological Evaluation as Anti-inflammatory Agents. Antiinflamm. Antiallergy Agents Med. Chem. 2020, 19, 254–267. [Google Scholar] [CrossRef] [PubMed]
- Bessong, P.O.; Obi, C.L.; Andréola, M.-L.; Rojas, L.B.; Pouységu, L.; Igumbor, E.; Meyer, J.J.M.; Quideau, S.; Litvak, S. Evaluation of selected South African medicinal plants for inhibitory properties against human immunodeficiency virus type 1 reverse transcriptase and integrase. J. Ethnopharmacol. 2005, 99, 83–91. [Google Scholar] [PubMed]
- Mahomed, I.M.; Ojewole, J.A. Hypoglycemic effect of Hypoxis hemerocallidea corm (African potato) aqueous extract in rats. Methods Find. Exp. Clin. Pharmacol. 2003, 25, 617–623. [Google Scholar] [CrossRef]
- Matyanga, C.M.J.; Morse, G.D.; Gundidza, M.; Nhachi, C.F.B. African potato (Hypoxis hemerocallidea): A systematic review of its chemistry, pharmacology and ethno medicinal properties. BMC Complement Med. Ther. 2020, 20, 182. [Google Scholar] [CrossRef]
- Lamprecht, J.H.; Freestone, M.; Bouic, P.J.D. A comparison of the survival benefit provided by putative immune modulators in the FIV (feline immunodeficiency virus) infected laboratory cat model. In Proceedings of the 13th International AIDS Conference, Durban, South Africa, 9–14 July 2000; Monduzzi Editore: Bologna, Italy, 2000; pp. 21–24. [Google Scholar]
- Albrecht, C.F.; Kruger, P.B.; Smit, B.J.; Freestone, M.; Gouws, L.; Miller, R.; Van Jaarsveld, P.P. The pharmacokinetic behaviour of hypoxoside taken orally by patients with lung cancer in a phase I trial. S. Afr. Med. J. 1995, 85, 861–865. [Google Scholar]
- Bizimenyera, S.E. The Potential Role of Antibacterial, Antioxidant and Antiparasitic Activity of Peltophorum africanum Sond. (Fabaceae) Extracts in Veterinary Medicine. Ph.D. Thesis, University of Pretoria, Pretoria, South Africa, 2007. [Google Scholar]
- Okeleye, B.I. In Vitro activity of bioactive compounds of selected South African medicinal plants on clinical isolates of Helicobacter pylori. Master’s Thesis, University of Fort Hare, Alice, South Africa, 2011. [Google Scholar]
- Parkar, H.; Aiyegoro, O.A.; Steenkamp, P.; Steenkamp, V. Extracts of Terminalia sericea enhance cell migratory activity of endothelial hybrid and fibroblast cells in vitro. Planta Med. 2017, 83, 1397–1404. [Google Scholar] [CrossRef]
- Mongalo, N.I.; McGaw, L.J.; Segapelo, T.V.; Finnie, J.F.; Van Staden, J. Ethnobotany, phytochemistry, toxicology and pharmacological properties of Terminalia sericea Burch. ex DC. (Combretaceae)—A review. J. Ethnopharmacol. 2016, 194, 789–802. [Google Scholar] [CrossRef]
- Cock, I.; Mavuso, N.; Van Vuuren, S. A review of plant-based therapies for the treatment of urinary tract infections in traditional Southern African Medicine. Evid. Based Complement Alternat. Med. 2021, 2021, 7341124. [Google Scholar] [CrossRef]
- Okaiyeto, K.; Oguntibeju, O.O. African Herbal Medicines: Adverse effects and cytotoxic potentials with different therapeutic Applications. Int. J. Environ. Res. Public Health. 2021, 18, 5988. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Steward, L.A.; PRISMA- P. Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sources | Province | Title or Focus of the Study | Citations |
|---|---|---|---|
| [5] | Limpopo | Antimicrobial activity, toxicity, and isolation of a bioactive compound from plants used to treat sexually transmitted diseases. | 6 |
| [9] | Eastern Cape | An ethnobotanical survey of medicinal plants used by traditional health practitioners to manage HIV and its related opportunistic infections in Mpoza, Eastern Cape Province, South Africa. | 17 |
| [18] | Limpopo | The traditional use of medicinal plants to treat sexually transmitted diseases. | 6 |
| [19] | Limpopo | Ethnobotanical Knowledge of the Lay People of Blouberg Area (Pedi Tribe), Limpopo Province, South Africa. | 33 |
| [29] | Eastern Cape | Ethnobotany and antimicrobial activity of sieketroos. | 3 |
| [37] | KwaZulu-Natal | Zulu Medicinal Plants: An Inventory. | 13 |
| [38] | Eastern Cape | Antibacterial and antifungal activity of traditional medicinal plants used against venereal diseases in South Africa. | 13 |
| [39] | Eastern Cape | Biological activity of traditional medicinal plants used against venereal diseases in South Africa. | 13 |
| [40] | Limpopo | Medicinal plant use of villagers in the Mopani district, Limpopo province, South Africa. | 21 |
| [41] | KwaZulu-Natal | Ethnobotanical plant uses in the KwaNibela Peninsula, St Lucia, South Africa. | 5 |
| [42] | Unidentified | An ethnobotanical survey of the Agter-Hantam, Northern Cape Province, South Africa. | 4 |
| [43] | KwaZulu-Natal | Medicinal plants used for the treatment of sexually transmitted infections by lay people in Northern Maputaland, KwaZulu-Natal Province, South Africa. | 33 |
| [44] | Limpopo | Phytomedicine versus Gonorrhoea: The Bapedi experience. | 18 |
| [45] | Limpopo | Erectile dysfunction: Definition and materia medica of Bapedi traditional healers in Limpopo Province, South Africa. | 12 |
| [46] | Mpumalanga | In Vitro evaluation of the comprehensive antimicrobial and antioxidant properties of Curtisia dentata (Burm.f) C.A. Sm: Toxicological effect on the Human Embryonic Kidney (HEK293) and Human Hepatocellular carcinoma (HepG2) cell lines. | 1 |
| [47] | Mpumalanga | Isolation of anti-mycobacterial compounds from Curtisia dentata (Burm.f.) C.A. Sm Curtisiaceae. | 1 |
| [48] | Limpopo | In vitro activity medicinal plants of the Venda region, South Africa, against Trichomonas vaginalis. | 29 |
| [49] | Limpopo | The ethnobotany of the VhaVenda. | 45 |
| [50] | Limpopo | Ethnobotanical survey of invasive alien plant species used in the treatment of sexually transmitted infections in Waterberg District, South Africa. | 14 |
| [51] | Limpopo | Data set on preliminary phytochemical analysis and antioxidant activity of selected invasive alien plant species used in the treatment of sexually transmitted infections in Waterberg District, South Africa. | 6 |
| [52] | Limpopo | A quantitative survey of the traditional plant use of VhaVenda, Limpopo Province, South Africa. | 55 |
| [53] | Limpopo | An ethnobotanical survey of indigenous knowledge on medicinal plants used by the traditional healers of the Lwamondo area, Limpopo Province, South Africa. | 5 |
| [54] | Unidentified | Evaluation of the antimicrobial properties of Vachellia karroo Hayne Banfi and Galasso pods used traditionally for the treatment of venereal diseases. | 1 |
| [55] | Limpopo | Medicinal plants and traditional practices in peri-urban domestic gardens of the Limpopo Province, South Africa. | 7 |
| [56] | Limpopo | The traditional use of plants to manage candidiasis and related infections in Venda, South Africa. | 45 |
| [57] | Limpopo | Isolation and characterization of antifungal compounds from Clerodendron glabrum var glabrum (Verbenaceae) used traditionally to treat candidiasis in Venda, South Africa. | 45 |
| [58] | Limpopo | Medicinal plants used to manage sexually transmitted infections by Bapedi traditional health practitioners in the Blouberg area, South Africa. | 17 |
| [59] | Limpopo | Invasive alien plants used in the treatment of HIV-AIDS-related symptoms by traditional healers of Vhembe Municipality, Limpopo Province, South Africa. | 38 |
| [60] | KwaZulu-Natal | A quantitative ethnobotanical survey of the Ixopo area of KwaZulu-Natal, South Africa. | 9 |
| [61] | KwaZulu-Natal | Zulu medicinal ethnobotany: new records from the Amandawe area of KwaZulu-Natal, South Africa. | 16 |
| [62] | Limpopo | An investigation into the trade of medicinal plants by muthi shops and street vendors in the Limpopo Province, South Africa. | 7 |
| [63] | KwaZulu-Natal | The medicinal ethnobotany of the Amandawe area in KwaCele, KwaZulu-Natal, South Africa. | 16 |
| [64] | Limpopo | The Ethnobotany of Central Sekhukhuneland, South Africa. | 33 |
| [65] | Limpopo | Antibacterial activities of selected medicinal plants used to treat sexually transmitted infections in Blouberg area, Limpopo Province. | 11 |
| [66] | Limpopo | Pharmacological properties of extracts from six South African medicinal plants used to treat sexually transmitted infections (STIs) and related infections. | 6 |
| [67] | Limpopo | Antimicrobial properties and phenolic contents of medicinal plants used by the Venda people for conditions related to venereal diseases. | 12 |
| [68] | Limpopo | Anti-inflammatory and mutagenic evaluation of medicinal plants used by Venda people against venereal and related infections. | 12 |
| [69] | Limpopo | Pharmacological evaluation of medicinal plants used by Venda people against venereal and related diseases. | 12 |
| [70] | Limpopo | Ethnopharmacological evaluation of a traditional herbal remedy used to treat gonorrhoea in Limpopo province, South Africa. | 8 |
| [71] | Limpopo | Plants traditionally used individually and in combination to treat sexually transmitted infections in northern Maputaland, South Africa: Antimicrobial activity and cytotoxicity. | 19 |
| [72] | Limpopo | The use of indigenous knowledge for primary health care among the Northern Sotho in the Limpopo Province. | 4 |
| [73] | Limpopo | The ethnoecological assessment of Cassia abbreviata Oliv. at Matsa village, Limpopo Province, South Africa. | 1 |
| [74] | Limpopo | Medicinal plants traded in informal herbal medicine markets of the Limpopo Province. | 20 |
| [75] | Limpopo | Antifungal activities of selected Venda medicinal plants against Candida albicans, Candida krusei and Cryptococcus neoformans isolated from South African AIDS patients. | 12 |
| [76] | Limpopo | Extraordinary Bapedi medicinal herb for gonorrhoea. | 1 |
| [77] | Limpopo | Medicinal utilisation of exotic plants by Bapedi traditional healers to treat human ailments in Limpopo Province, South Africa. | 11 |
| [78] | Limpopo | Exotic and indigenous problem plants species used by the Bapedi to treat sexually transmitted infections in Limpopo Province, South Africa. | 10 |
| [79] | Limpopo | Indigenous plant species used by Bapedi healers to treat sexually transmitted infections: Their distribution, harvesting, conservation and threats. | 37 |
| [80] | Limpopo | Herbal medicines used by Bapedi traditional healers to treat reproductive ailments in the Limpopo Province, South Africa. | 21 |
| [81] | Limpopo | Use, conservation, and present availability status of ethnomedicinal plants of Matebele-village in the Limpopo Province, South Africa. | 3 |
| [82] | Limpopo | Bapedi phytomedicine and their use in the treatment of sexually transmitted infections in Limpopo Province, South Africa. | 47 |
| [83] | Limpopo | Antibacterial activity of sixteen plant species from Phalaborwa. | 2 |
| [84] | Mpumalanga | An Exploratory study on the diverse uses and benefits of locally sourced fruit species in three villages of Mpumalanga Province, South Africa. | 3 |
| [85] | Limpopo | Ethnobotanical survey and conservation of medicinal plants used by local people Thulamela municipality, Limpopo Province. | 3 |
| [86] | Mpumalanga | Antimicrobial, antioxidant, and cytotoxicity studies of medicinal plants used in the treatment of sexually transmitted infections. | 5 |
| [87] | Mpumalanga | An Ethnobotanical Study of Medicinal Plants Used in Villages under Jongilanga Tribal council, Mpumalanga. | 9 |
| [88] | Unidentified | An antimicrobial investigation of plants used traditionally in southern Africa to treat sexually transmitted infections. | 24 |
| [89] | Unidentified | Medicinal plants of South Africa. | 16 |
| [90] | Unidentified | Medicinal plants of South Africa. | 23 |
| [91] | Unidentified | A review of Khoisan and Cape Dutch medical ethnobotany. | 1 |
| [92] | Unidentified | An ethnobotanical survey of medicinal plants in the south-eastern Karoo, South Africa. | 7 |
| [93] | Unidentified | A broad review of commercially important southern African medicinal plants. | 1 |
| [94] | Unidentified | Making the most of indigenous trees. | 7 |
| [95] | Western Cape | Medicinal plant use in the Bredasdorp/Elim region of the Southern Overberg in the Western Cape Province of South Africa. | 3 |
| Plant Species | Reported Relevant In Vitro Antimicrobial Activity | Experimental Evidence Assessment | Reference(s) |
|---|---|---|---|
| Grewia flava | The acetone extract exhibited a minimum inhibitory concentration of 0.05 mg/mL against Mycoplasma hominis. Taraxerol and lupeol (Column Chromatography; NMR Mass Spectrometry and FTIR) isolated from root acetone extract exhibited MIC value of 0.03 against Candida albicans. Aqueous fraction from acetone roots extract exhibited MIC value of 0.04 mg/mL against Staphylococcus aureus isolated from wound of HIV-AIDS patient, while lupeol exhibited MIC values of 0.01 and 0.030 against M. hominis and Cryptococcus neoformans. | Positive evidence, dose dependence | [66,112,113] |
| Carica papaya | Aqueous extract from the leaves exhibited minimum inhibitory concentrations of 0.38 and 0.50 mg/mL against Ureaplasma urealyticum and Oligella urealytica, respectively, while organic extract (1:1 methanol: dichloromethane) exhibited an MIC value of 0.25 mg/mL against Neisseria gonorhoeae. Aqueous and ethanol extracts from flowers exhibited MIC value of 0.05 mg/mL against Neisseria gonorrhoea. | Positive evidence, dose dependence | [71,114] |
| Helichrysum caespititium | Organic extract from whole plant exhibited minimum inhibitory concentrations of 0.02, 0.10 and 0.06 mg/mL against Candida albicans, Gardnerella vaginalis and Neisseria gonorrhoea, respectively. Hexane extract from whole plant exhibited an MIC value of 0.04 mg/mL against Neisseria gonorrhoea. | Positive evidence, dose dependence | [115,116] |
| Hypoxis haemerocallidea | The aqueous extract from corms exhibited MIC values of 0.25 and 0.5 mg/mL against Ureaplasma urealyticum and Neisseria gonorrhoea, respectively. | Positive evidence, dose dependence | [71] |
| Peltophorum africanum | Organic extract from the roots exhibited MIC values of 0.04, 0.25 and 0.50 mg/mL against Ureaplasma urealyticum, Neisseria gonorrhoea and Gardnerella vaginalis. | Positive evidence, dose dependence | [71] |
| Sclerocarrya birrea | Organic extract from stem bark exhibited an MIC value of 0.25 mg /mL against both Ureaplasma urealyticum and Neisseria gonorrhoea, while aqueous extract yielded MIC values of 0.25 and 0.50 mg/mL against Ureaplasma urealyticum and Neisseria gonorrhoea. | Positive evidence, dose dependence | [71] |
| Syzygium cordatum | Aqueous extract from stem bark exhibited MIC value of 0.25 mg/mL against both Ureaplasma urealyticum and Neisseria gonorrhoea, and MIC values of 0.50 and 0.75 mg/L against Candida albicans and Gardnerella vaginalis, respectively. | Positive evidence, dose dependence | [71] |
| Ximenia caffra | Aqueous extracts from roots exhibited MIC value of 0.25 against both Neisseria gonorhoeae and Ureaplasma urealyticum, while organic extract yielded MIC values of 0.50 and 0.75 mg/mL against Ureaplasma urealyticum and Oligella urealytica, respectively. | Positive evidence, dose dependence | [71] |
| Aloe ferrox | Methanol extract from leaves and Aloin (Column Chromatography, NMR and Mass Spectrometry) exhibited MIC values of 0.5 and 0.1 mg/mL against N. gonorhoeae, respectively. | Positive evidence, dose dependence | [117] |
| Ranunculus multifidus | Aqueous extract exhibited MIC value of 0.02 mg/mL against Ureaplasma urealyticum. | Positive evidence, dose dependence | [71] |
| Withania somnifera | Methanol root extract exhibited MIC value of 0.5 mg/mL against N. gonorrhoeae. | Positive evidence, dose dependence | [117] |
| Bowiea volubilis | The ethanol extract from bulbs exhibited MIC value of 3.125 mg/mL against Staphylococcus aureus. | Inconclusive evidence, dose dependence | [39,40,89] |
| Plant Species | Mixture or Possible Quantities | Therapeutic Indication | Reference |
|---|---|---|---|
| Terminalia sericea, Cassine transvaalensis, Elephantorrhiza burkei, Rauvolvia caffra and Andredera cordifolia | Equal quantities of the plants | Unidentified STIs | [17] |
| Bauhinia galpinii, Elephantorrhiza burkei and Cassia abbreviata | Equal quantities of the roots are boiled and taken orally | Impotence | [19] |
| Peltophorum africanum, Elephantorrhiza burkei, Cassia abbreviata, and three nodes of Cissus quadrangulari | Equal quantities of the plant species and three nodes of Cissus quadrangularis | Dropsy/syphilis | [19] |
| Cassia Abbreviata, Jatropha zeyheri, Cissus quadrangularis, Elephantorrhiza burkei, Peltophorum africanum, Waltheria indida, Urginea sanguinea and Harpagophythum procumbens | Equal quantities of the plant species and three nodes of Cissus quadrangularis | Dropsy/syphilis | [65] |
| Anredera cordifolia, Catharanthus roseus, Datura stramonium, Gomphocarpus fruticosus, Prunus persica, Senna italica, Senna petersiana, and Solanum panduriforme | Different plant parts | Gonorrhoea and opportunistic infections associated with HIV-AIDS | [70] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mongalo, N.I.; Raletsena, M.V. An Inventory of South African Medicinal Plants Used in the Management of Sexually Transmitted and Related Opportunistic Infections: An Appraisal and Some Scientific Evidence (1990–2020). Plants 2022, 11, 3241. https://doi.org/10.3390/plants11233241
Mongalo NI, Raletsena MV. An Inventory of South African Medicinal Plants Used in the Management of Sexually Transmitted and Related Opportunistic Infections: An Appraisal and Some Scientific Evidence (1990–2020). Plants. 2022; 11(23):3241. https://doi.org/10.3390/plants11233241
Chicago/Turabian StyleMongalo, Nkoana I., and Maropeng V. Raletsena. 2022. "An Inventory of South African Medicinal Plants Used in the Management of Sexually Transmitted and Related Opportunistic Infections: An Appraisal and Some Scientific Evidence (1990–2020)" Plants 11, no. 23: 3241. https://doi.org/10.3390/plants11233241
APA StyleMongalo, N. I., & Raletsena, M. V. (2022). An Inventory of South African Medicinal Plants Used in the Management of Sexually Transmitted and Related Opportunistic Infections: An Appraisal and Some Scientific Evidence (1990–2020). Plants, 11(23), 3241. https://doi.org/10.3390/plants11233241