
Moderating Effect of a Cross-Level Social Distancing Policy on the Disparity of COVID-19 Transmission in the United States



Abstract
:1. Introduction
2. Materials and Methods
2.1. Variables and Data Source
2.1.1. COVID-19 Infection Rate
2.1.2. Social Distancing Policy
2.1.3. Social Vulnerability Index (SVI)
2.2. Statistical Analysis
2.3. Geographically Weighted Regression (GWR)
2.4. Hierarchical Linear Model (HLM)
3. Results
3.1. SVI and COVID-19 Infection Rate
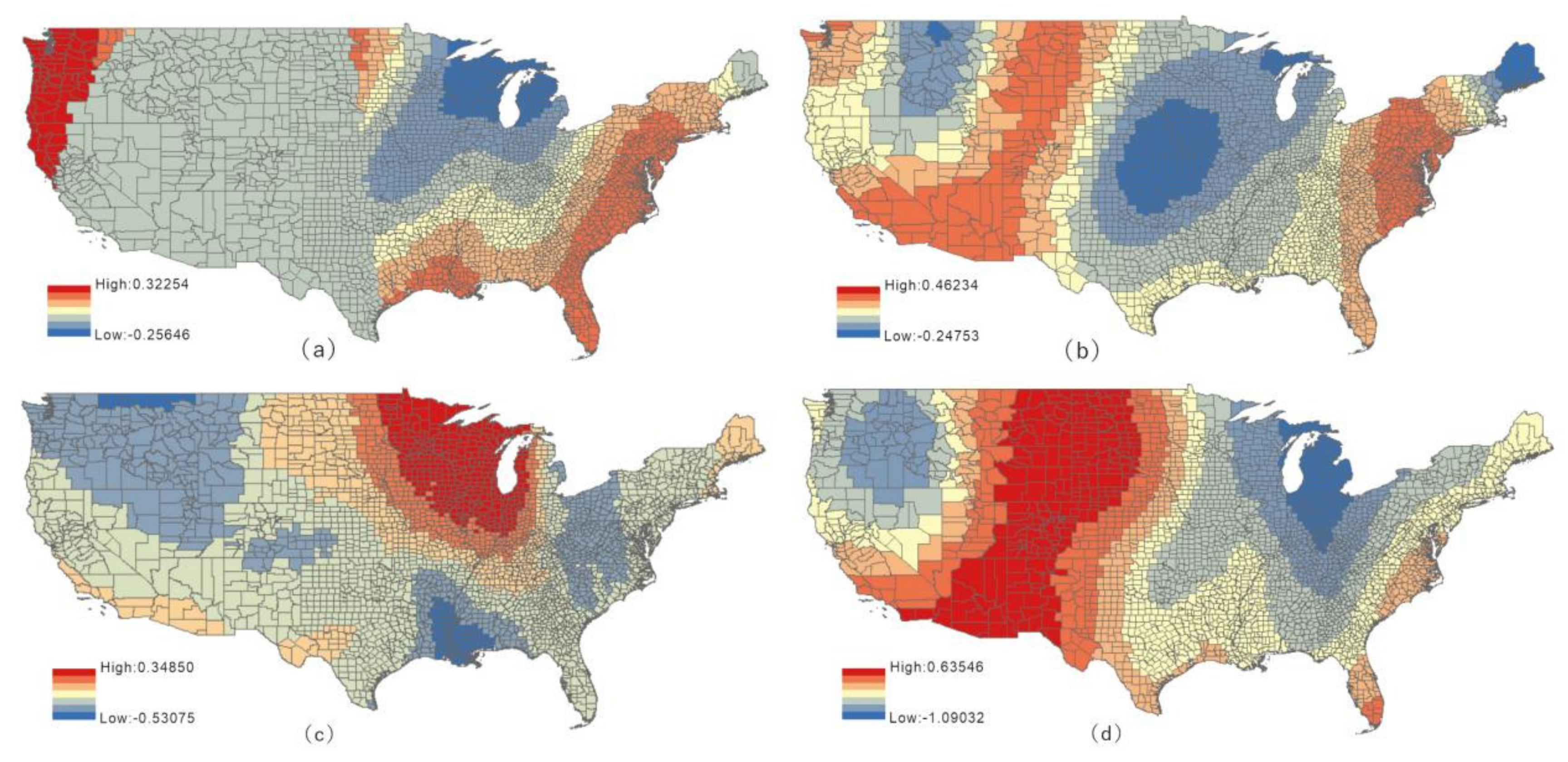
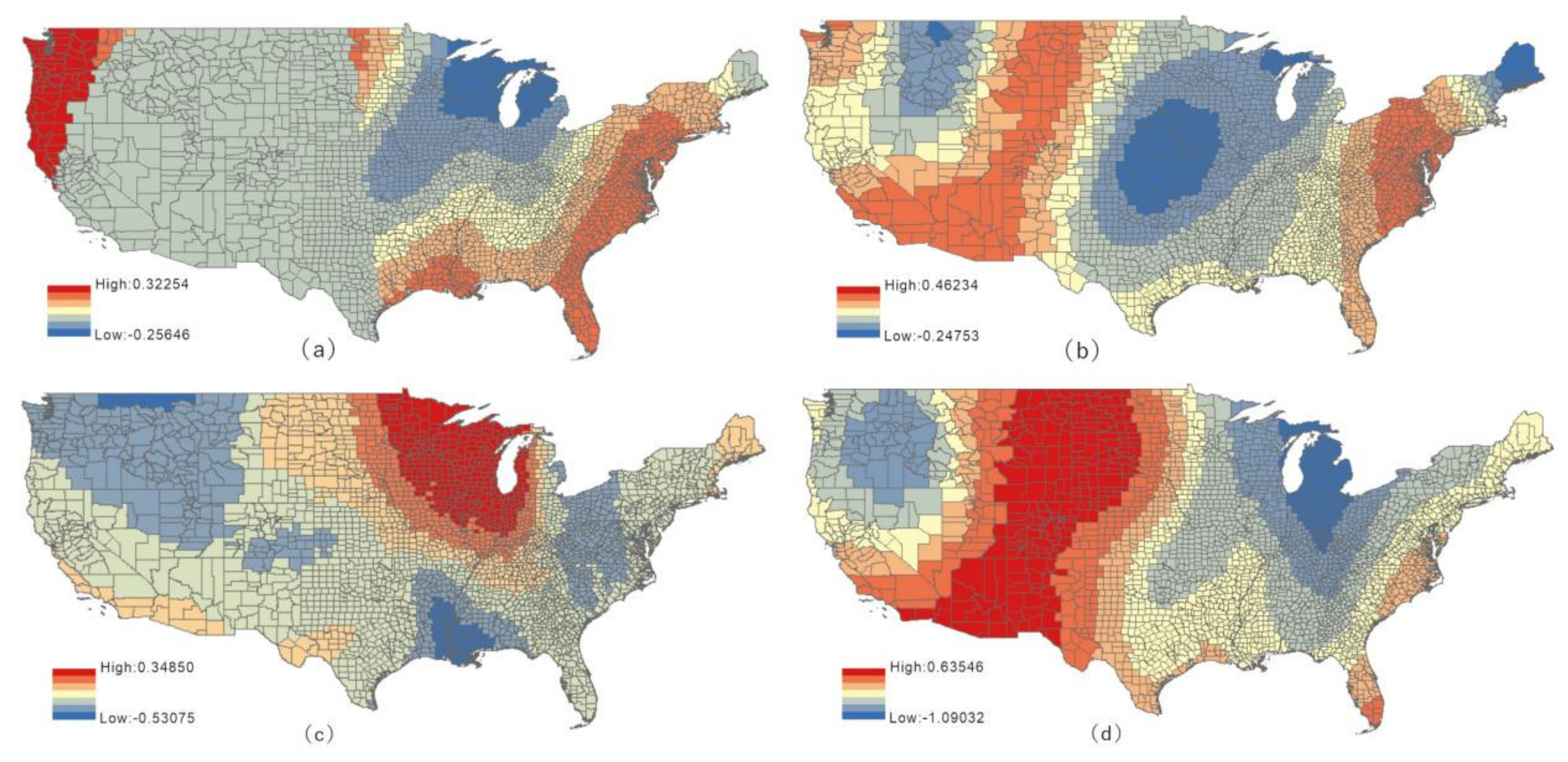
3.2. GWR Results of the SVI Subindex and COVID-19 Infection Rate
3.3. HLM
3.3.1. Null Model
3.3.2. Full Model
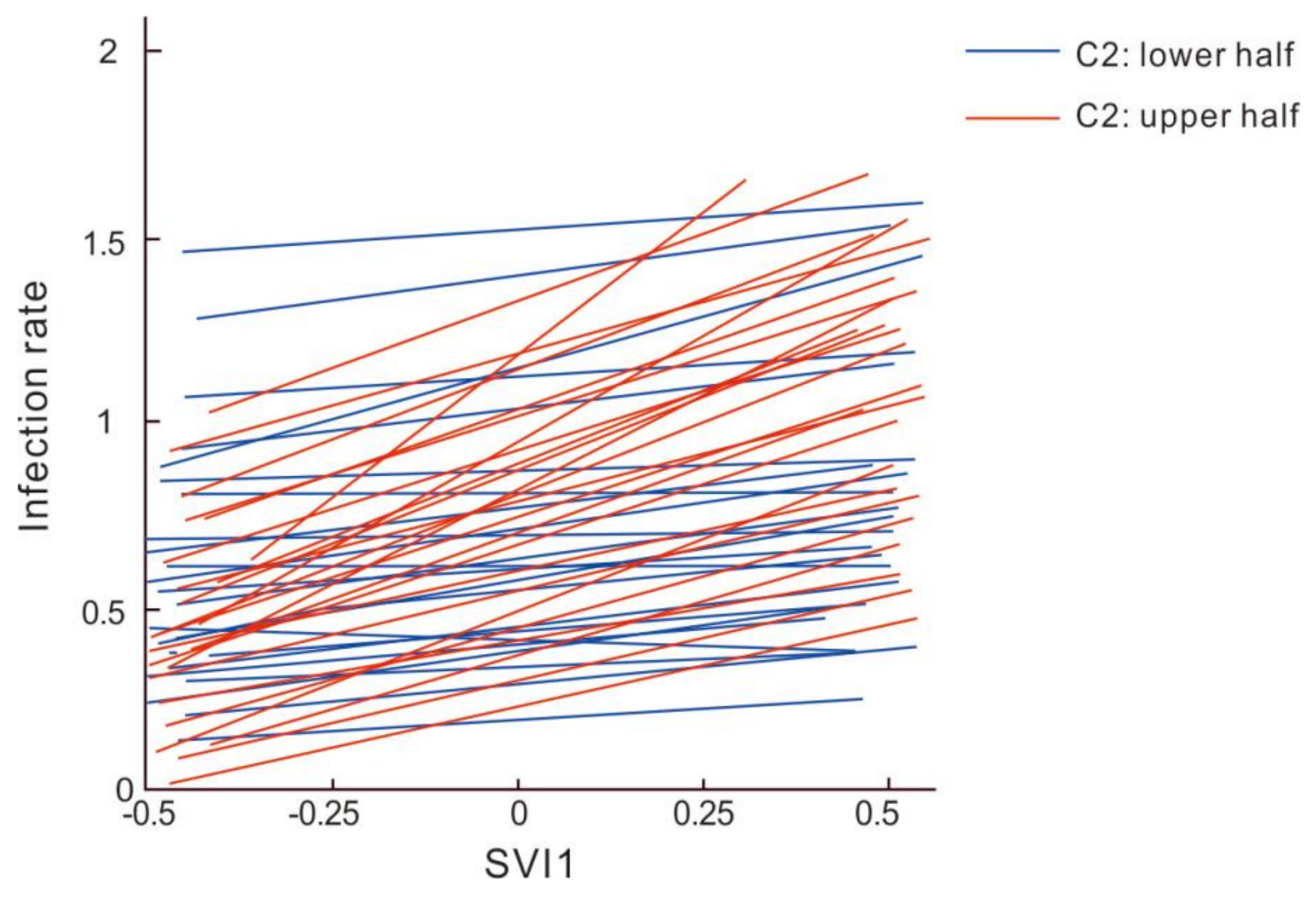
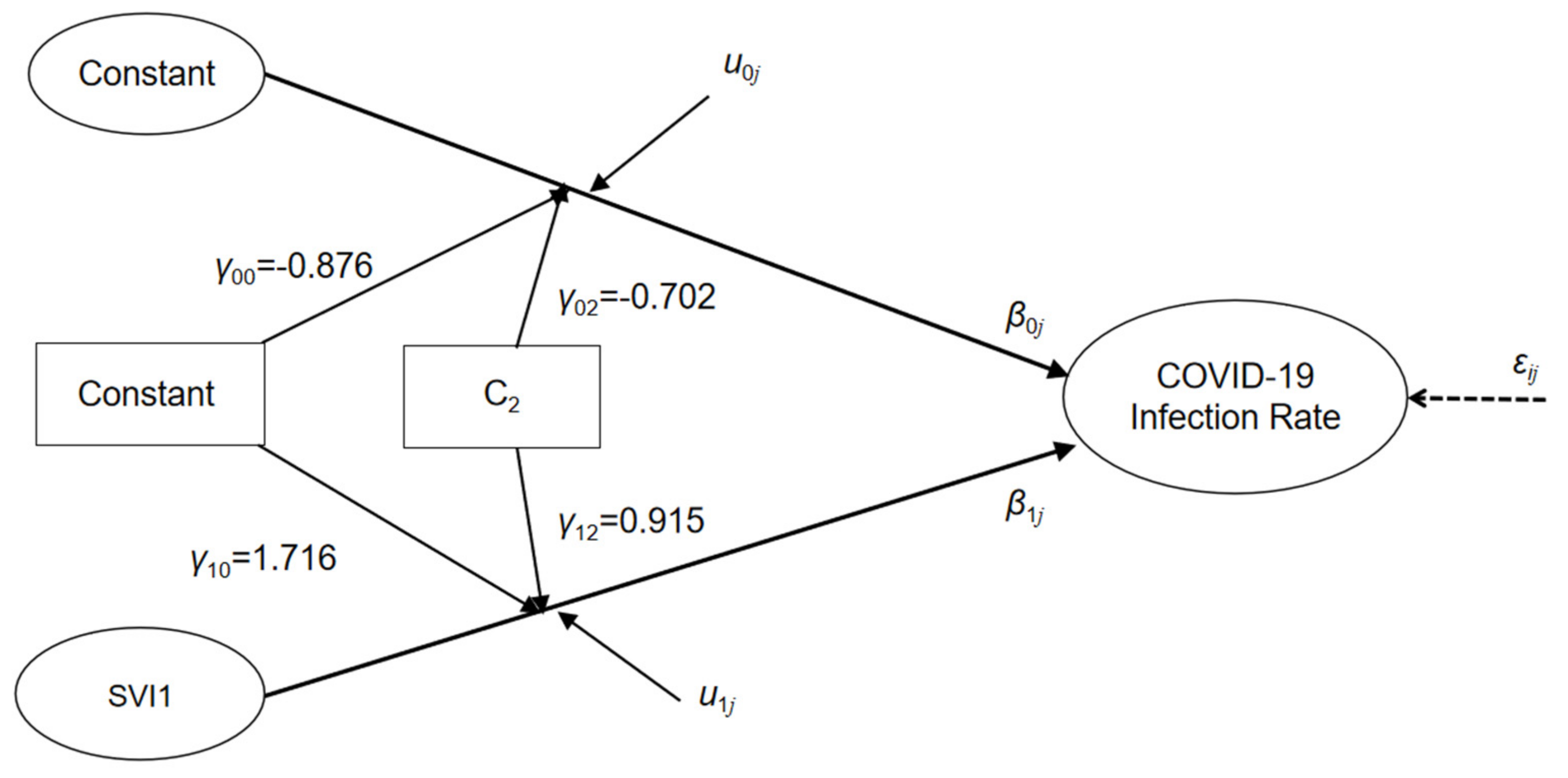
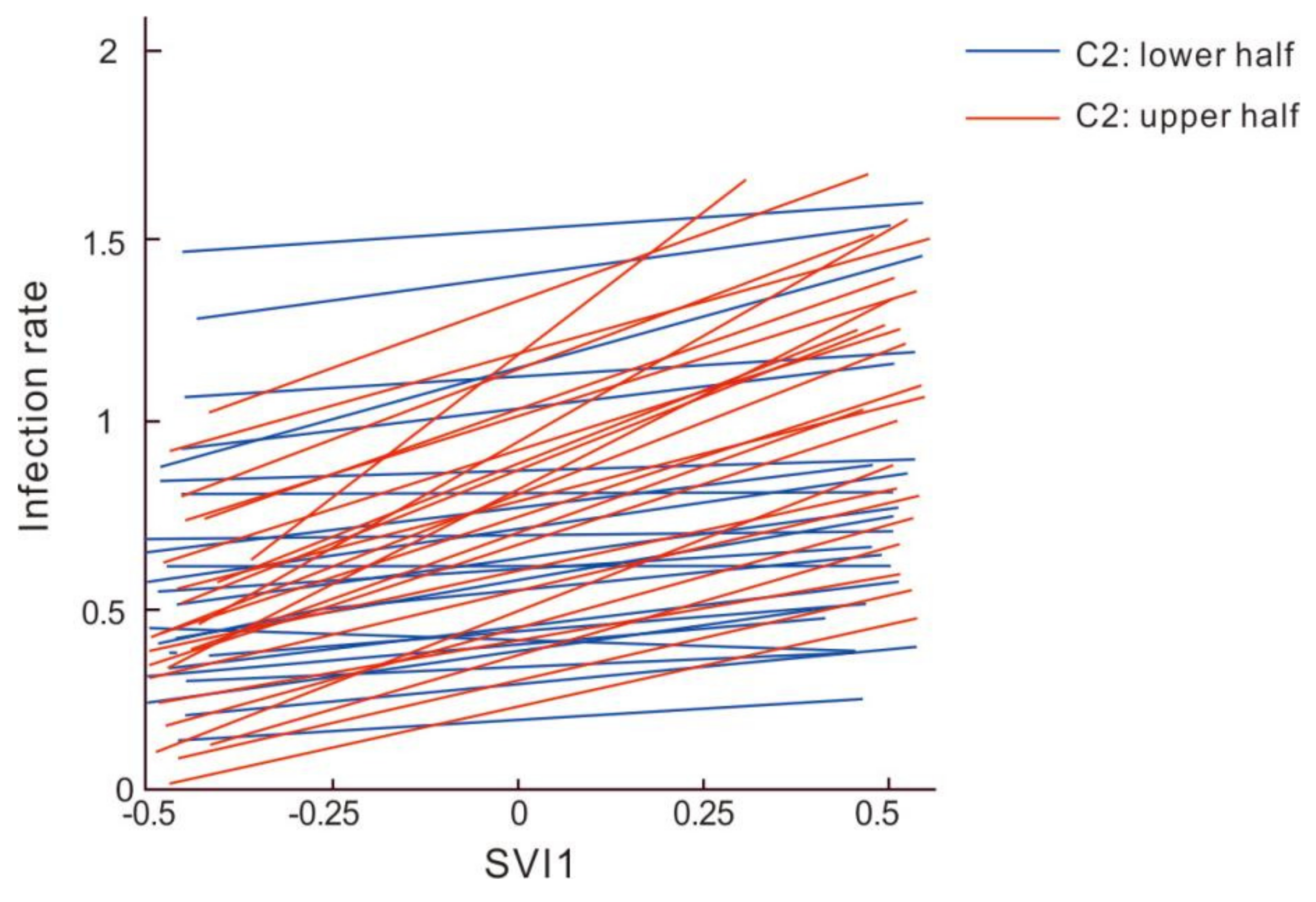
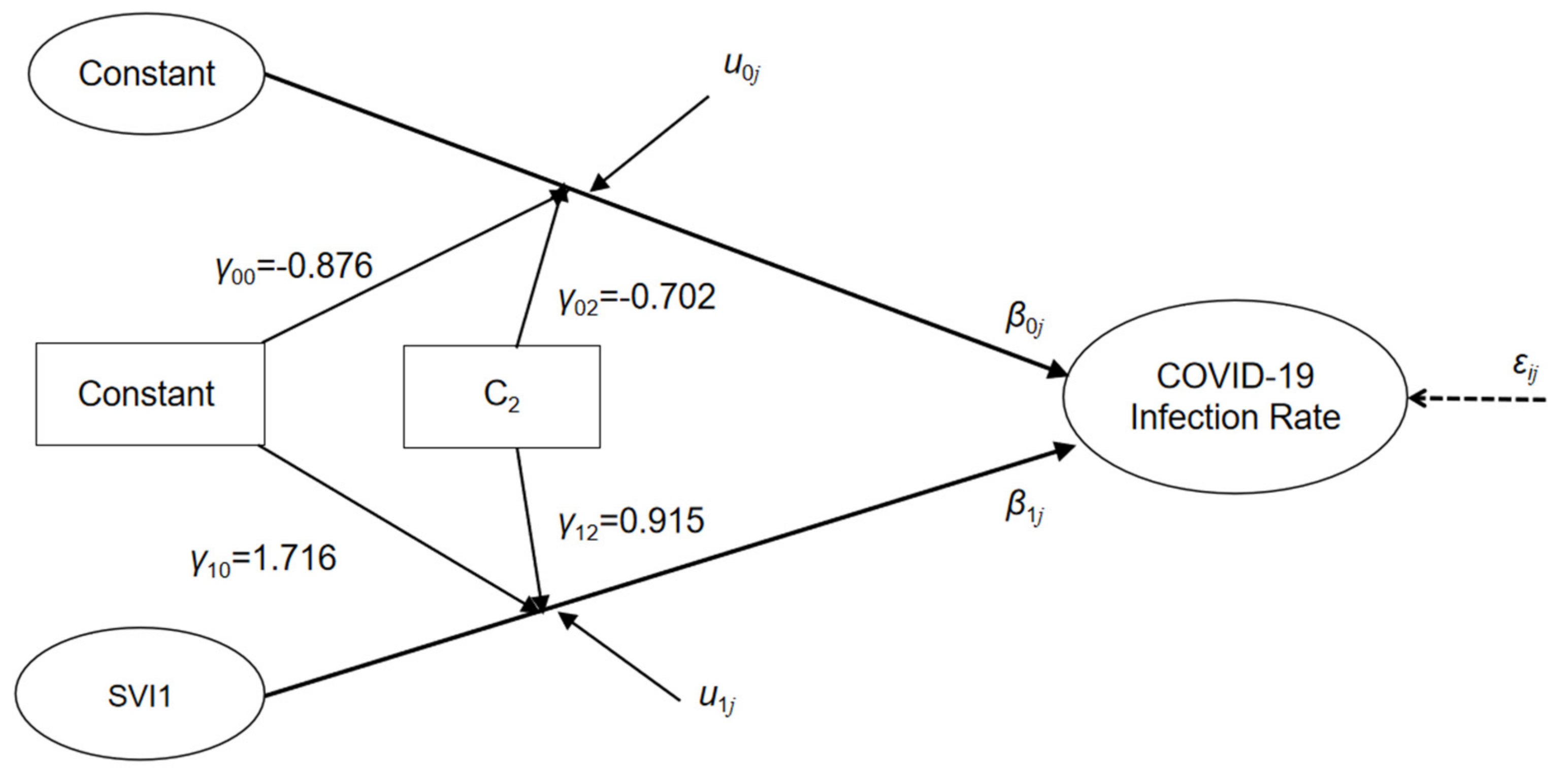
3.3.3. Cross-Level Interaction of Independent Variables
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Askitas, N.; Tatsiramos, K.; Verheyden, B. Estimating worldwide effects of non-pharmaceutical interventions on COVID-19 incidence and population mobility patterns using a multiple-event study. Sci. Rep. 2021, 11, 1972. [Google Scholar] [CrossRef] [PubMed]
- Duan, W.; Fan, Z.; Zhang, P.; Guo, G.; Qiu, X. Mathematical and computational approaches to epidemic modeling: A comprehensive review. Front. Comput. Sci. 2015, 9, 806–826. [Google Scholar] [CrossRef] [PubMed]
- Karasmanaki, E.; Tsantopoulos, G. Impacts of social distancing during COVID-19 pandemic on the daily life of forestry students. Child. Youth Serv. Rev. 2021, 120, 105781. [Google Scholar] [CrossRef] [PubMed]
- Yomoda, K.; Kurita, S. Influence of social distancing during the COVID-19 pandemic on physical activity in children: A scoping review of the literature. J. Exerc. Sci. Fit. 2021, 19, 195–203. [Google Scholar] [CrossRef]
- Zhang, C.H.; Schwartz, G.G. Spatial Disparities in Coronavirus Incidence and Mortality in the United States: An Ecological Analysis as of May 2020. J. Rural Health 2020, 36, 433–445. [Google Scholar] [CrossRef]
- Iyanda, A.E.; Boakye, K.A.; Lu, Y.M.; Oppong, J.R.; Hipp, J.R. Racial/Ethnic Heterogeneity and Rural-Urban Disparity of COVID-19 Case Fatality Ratio in the USA: A Negative Binomial and GIS-Based Analysis. J. Racial Ethn. Health Disparities 2021, 9, 708–721. [Google Scholar] [CrossRef]
- Griffith, D.; Li, B. Spatial-temporal modeling of initial COVID-19 diffusion: The cases of the Chinese Mainland and Conterminous United States. Geo-Spat. Inf. Sci. 2021, 24, 340–362. [Google Scholar] [CrossRef]
- Yang, C.W.; Sha, D.X.; Liu, Q.; Li, Y.; Lan, H.; Guan, W.W.; Hu, T.; Li, Z.; Zhang, Z.; Thompson, J.H.; et al. Taking the pulse of COVID-19: A spatiotemporal perspective. Int. J. Digit. Earth 2020, 13, 1186–1211. [Google Scholar] [CrossRef]
- Roy, S.; Ghosh, P. Factors affecting COVID-19 infected and death rates inform lockdown-related policymaking. PLoS ONE 2020, 15, e0241165. [Google Scholar] [CrossRef]
- Liu, J.T.; Zhou, J.; Yao, J.X.; Zhang, X.X.; Li, L.Y.; Xu, X.C.; He, X.; Wang, B.; Fu, S.; Niu, T.; et al. Impact of meteorological factors on the COVID-19 transmission: A multi-city study in China. Sci. Total Environ. 2020, 726, 138513. [Google Scholar] [CrossRef]
- CDC/ATSDR Social Vulnerability Index. Available online: https://www.atsdr.cdc.gov/placeandhealth/svi/ (accessed on 22 February 2022).
- Dasgupta, S.; Bowen, V.B.; Leidner, A.; Fletcher, K.; Musial, T.; Rose, C.; Cha, A.; Kang, G.; Dirlikov, E.; Pevzner, E.; et al. Association Between Social Vulnerability and a County’s Risk for Becoming a COVID-19 Hotspot—United States, June 1–July 25, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1535–1541. [Google Scholar] [CrossRef] [PubMed]
- Gaynor, T.S.; Wilson, M.E. Social Vulnerability and Equity: The Disproportionate Impact of COVID-19. Public Adm. Rev. 2020, 80, 832–838. [Google Scholar] [CrossRef]
- Hathaway, E.D. American Indian and Alaska Native People: Social Vulnerability and COVID-19. J. Rural Health 2021, 37, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Karmakar, M.; Lantz, P.M.; Tipirneni, R. Association of Social and Demographic Factors With COVID-19 Incidence and Death Rates in the US. JAMA Netw. Open 2021, 4, e2036462. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.Y.; Li, Z.Q.; Mathews, M.C.; Praharaj, S.; Karna, B.; Solis, P. The spatial association of social vulnerability with COVID-19 prevalence in the contiguous United States. Int. J. Environ. Health Res. 2020, 1–8. [Google Scholar] [CrossRef]
- LeRose, J.J.; Merlo, C.; Duong, P.; Harden, K.; Rush, R.; Artzberger, A.; Sidhu, N.; Sandhu, A.; Chopra, T. The role of the social vulnerability index in personal protective equipment shortages, number of cases, and associated mortality during the coronavirus disease 2019 (COVID-19) pandemic in Michigan skilled nursing facilities. Infect. Cont. Hosp. Ep. 2021, 42, 877–880. [Google Scholar] [CrossRef]
- Karaye, I.M.; Horney, J.A. The Impact of Social Vulnerability on COVID-19 in the US: An Analysis of Spatially Varying Relationships. Am. J. Prev. Med. 2020, 59, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Khazanchi, R.; Beiter, E.R.; Gondi, S.; Beckman, A.L.; Bilinski, A.; Ganguli, I. County-Level Association of Social Vulnerability with COVID-19 Cases and Deaths in the USA. J. Gen. Intern. Med. 2020, 35, 2784–2787. [Google Scholar] [CrossRef]
- Bilal, U.; Tabb, L.P.; Barber, S.; Roux, A.V.D. Spatial Inequities in COVID-19 Testing, Positivity, Confirmed Cases, and Mortality in 3 US Cities An Ecological Study. Ann. Intern. Med. 2021, 174, 936–944. [Google Scholar]
- Kim, S.J.; Bostwick, W. Social Vulnerability and Racial Inequality in COVID-19 Deaths in Chicago. Health Educ. Behav. 2020, 47, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Xie, K.; Liang, B.; Dulebenets, M.A.; Mei, Y. The Impact of Risk Perception on Social Distancing during the COVID-19 Pandemic in China. Int. J. Environ. Res. Public Health 2020, 17, 6256. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Zou, H.; Xie, K.; Dulebenets, M.A. An Assessment of Social Distancing Obedience Behavior during the COVID-19 Post-Epidemic Period in China: A Cross-Sectional Survey. Sustainability 2021, 13, 8091. [Google Scholar] [CrossRef]
- Khorram-Manesh, A.; Dulebenets, M.A.; Goniewicz, K. Implementing Public Health Strategies-The Need for Educational Initiatives: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 5888. [Google Scholar] [CrossRef] [PubMed]
- Courtemanche, C.; Garuccio, J.; Le, A.; Pinkston, J.; Yelowitz, A. Strong Social Distancing Measures In The United States Reduced The COVID-19 Growth Rate. Health Aff. 2020, 39, 1237–1246. [Google Scholar] [CrossRef]
- Kaufman, B.G.; Whitaker, R.; Mahendraratnam, N.; Hurewitz, S.; Yi, J.; Smith, V.A.; McClellan, M. State variation in effects of state social distancing policies on COVID-19 cases. BMC Public Health 2021, 21, 1239. [Google Scholar] [CrossRef]
- Jia, J.S.S.; Lu, X.; Yuan, Y.; Xu, G.; Jia, J.M.; Christakis, N.A. Population flow drives spatio-temporal distribution of COVID-19 in China. Nature 2020, 582, 389–394. [Google Scholar] [CrossRef]
- Badr, H.S.; Du, H.; Marshall, M.; Dong, E.; Squire, M.M.; Gardner, L.M. Association between mobility patterns and COVID-19 transmission in the USA: A mathematical modelling study. Lancet Infect. Dis. 2020, 20, 1247–1254. [Google Scholar] [CrossRef]
- Lasry, A.; Kidder, D.; Hast, M.; Poovey, J.; Sunshine, G.; Winglee, K.; Zviedrite, N.; Ahmed, F.; Ethier, K.A.; CDC Public Health Law Program; et al. Timing of Community Mitigation and Changes in Reported COVID-19 and Community Mobility—Four US Metropolitan Areas, February 26–April 1, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 451–457. [Google Scholar] [CrossRef] [Green Version]
- Hou, X.; Gao, S.; Li, Q.; Kang, Y.; Chen, N.; Chen, K.; Rao, J.; Ellenberg, J.S.; Patz, J.A. Intracounty modeling of COVID-19 infection with human mobility: Assessing spatial heterogeneity with business traffic, age, and race. Proc. Natl. Acad. Sci. USA 2021, 118, e2020524118. [Google Scholar] [CrossRef]
- Messner, W.; Payson, S.E. Variation in COVID-19 outbreaks at the US state and county levels. Public Health 2020, 187, 15–18. [Google Scholar] [CrossRef]
- Sun, F.; Matthews, S.A.; Yang, T.-C.; Hu, M.-H. A spatial analysis of the COVID-19 period prevalence in US counties through June 28, 2020: Where geography matters? Ann. Epidemiol. 2020, 52, 54–59.e1. [Google Scholar] [CrossRef] [PubMed]
- Thomas, L.J.; Huang, P.; Yin, F.; Luo, X.I.; Almquist, Z.W.; Hipp, J.R.; Butts, C.T. Spatial heterogeneity can lead to substantial local variations in COVID-19 timing and severity. Proc. Natl. Acad. Sci. USA 2020, 117, 24180–24187. [Google Scholar] [CrossRef] [PubMed]
- Villeneuve, P.J.; Goldberg, M.S. Methodological Considerations for Epidemiological Studies of Air Pollution and the SARS and COVID-19 Coronavirus Outbreaks. Environ. Health Perspect. 2020, 128, 095001. [Google Scholar] [CrossRef] [PubMed]
- Probst, T.M.; Lee, H.J.; Bazzoli, A. Economic Stressors and the Enactment of CDC-Recommended COVID-19 Prevention Behaviors: The Impact of State-Level Context. J. Appl. Psychol. 2020, 105, 1397–1407. [Google Scholar] [CrossRef] [PubMed]
- McNeish, D.; Kelley, K. Fixed Effects Models Versus Mixed Effects Models for Clustered Data: Reviewing the Approaches, Disentangling the Differences, and Making Recommendations. Psychol. Methods 2019, 24, 20–35. [Google Scholar] [CrossRef]
- Cunningham, G.B.; Nite, C. Demographics, politics, and health factors predict mask wearing during the COVID-19 pandemic: A cross-sectional study. BMC Public Health 2021, 21, 1403. [Google Scholar] [CrossRef] [PubMed]
- Scarpone, C.; Brinkmann, S.T.; Grosse, T.; Sonnenwald, D.; Fuchs, M.; Walker, B.B. A multimethod approach for county-scale geospatial analysis of emerging infectious diseases: A cross-sectional case study of COVID-19 incidence in Germany. Int. J. Health Geogr. 2020, 19, 32. [Google Scholar] [CrossRef]
- Smith, M.D.; Wesselbaum, D. COVID-19, Food Insecurity, and Migration. J. Nutr. 2020, 150, 2855–2858. [Google Scholar] [CrossRef]
- Diez-Roux, A.V. Bringing context back into epidemiology: Variables and fallacies in multilevel analysis. Am. J. Public Health 1998, 88, 216–222. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Zyphur, M.J.; Preacher, K.J. Testing Multilevel Mediation Using Hierarchical Linear Models Problems and Solutions. Organ. Res. Methods 2009, 12, 695–719. [Google Scholar] [CrossRef] [Green Version]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Oxford COVID-19 Government Response Tracker. Available online: https://covidtracker.bsg.ox.ac.uk/ (accessed on 22 February 2022).
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav 2021, 5, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, B.E.; Gregory, E.W.; Hallisey, E.J.; Heitgerd, J.L.; Lewis, B. A Social Vulnerability Index for Disaster Management. J. Homel. Secur. Emerg. Manag. 2011, 8, 3. [Google Scholar] [CrossRef]
- Tobler, W. On the first law of geography: A reply. Ann. Assoc. Am. Geogr. 2004, 94, 304–310. [Google Scholar] [CrossRef]
- Brunsdon, C.; Fotheringham, A.S.; Charlton, M.E. Geographically weighted regression: A method for exploring spatial nonstationarity. Geogr. Anal. 1996, 28, 281–298. [Google Scholar] [CrossRef]
- Blalock, H.M. Contextual-Effects Models: Theoretical and Methodological Issues. Annu. Rev. Sociol. 1984, 10, 353–372. [Google Scholar] [CrossRef]
- Duncan, C.; Jones, K.; Moon, G. Health-related behaviour in context: A multilevel modelling approach. Soc. Sci. Med. 1996, 42, 817–830. [Google Scholar] [CrossRef]
- Zhang, Y.J.; Jin, Y.L.; Zhu, T.T. The health effects of individual characteristics and environmental factors in China: Evidence from the hierarchical linear model. J. Clean. Prod. 2018, 194, 554–563. [Google Scholar] [CrossRef]
- Luo, W.; Azen, R. Determining Predictor Importance in Hierarchical Linear Models Using Dominance Analysis. J. Educ. Behav. Stat. 2013, 38, 3–31. [Google Scholar] [CrossRef]
- Gibbons, J.; Schiaffino, M.K. Determining the spatial heterogeneity underlying racial and ethnic differences in timely mammography screening. Int. J. Health Geogr. 2016, 15, 39. [Google Scholar] [CrossRef] [Green Version]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations—uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Castro, S.L. Data analytic methods for the analysis of multilevel questions—A comparison of intraclass correlation coefficients, r(wg(j)), hierarchical linear modeling, within- and between-analysis, and random group resampling. Leadersh. Q. 2002, 13, 69–93. [Google Scholar] [CrossRef]
- Dyer, O. COVID-19: Black people and other minorities are hardest hit in US. BMJ 2020, 369, m1483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, C.P.; Essien, U.R.; Pasha, S.; Gross, J.R.; Wang, S.-y.; Nunez-Smith, M. Racial and Ethnic Disparities in Population-Level COVID-19 Mortality. J. Gen. Intern. Med. 2020, 35, 3097–3099. [Google Scholar] [CrossRef] [PubMed]
- Wadhera, R.K.; Wadhera, P.; Gaba, P.; Figueroa, J.F.; Maddox, K.E.J.; Yeh, R.W.; Shen, C. Variation in COVID-19 Hospitalizations and Deaths Across New York City Boroughs. JAMA J. Am. Med. Assoc. 2020, 323, 2192–2195. [Google Scholar] [CrossRef]
- Rogers, T.N.; Rogers, C.R.; VanSant-Webb, E.; Gu, L.Y.; Yan, B.; Qeadan, F. Racial Disparities in COVID-19 Mortality Among Essential Workers in the United States. World Med. Health Policy 2020, 12, 311–327. [Google Scholar] [CrossRef]
- McCormack, G.; Avery, C.; Spitzer, A.K.-L.; Chandra, A. Economic Vulnerability of Households With Essential Workers. JAMA J. Am. Med. Assoc. 2020, 324, 388–390. [Google Scholar] [CrossRef]
- Xiong, D.; Zhang, L.; Watson, G.L.; Sundin, P.; Bufford, T.; Zoller, J.A.; Shamshoian, J.; Suchard, M.A.; Ramirez, C.M. Pseudo-likelihood based logistic regression for estimating COVID-19 infection and case fatality rates by gender, race, and age in California. Epidemics 2020, 33, 100418. [Google Scholar] [CrossRef]
- Levin, A.T.; Hanage, W.P.; Owusu-Boaitey, N.; Cochran, K.B.; Walsh, S.P.; Meyerowitz-Katz, G. Assessing the age specificity of infection fatality rates for COVID-19: Systematic review, meta-analysis, and public policy implications. Eur. J. Epidemiol. 2020, 35, 1123–1138. [Google Scholar] [CrossRef]
- Lee, S.; Zabinsky, Z.B.; Wasserheit, J.N.; Kofsky, S.M.; Liu, S. COVID-19 Pandemic Response Simulation in a Large City: Impact of Nonpharmaceutical Interventions on Reopening Society. Med. Decis. Mak. 2021, 41, 419–429. [Google Scholar] [CrossRef]
- Wellenius, G.A.; Vispute, S.; Espinosa, V.; Fabrikant, A.; Tsai, T.C.; Hennessy, J.; Dai, A.; Williams, B.; Gadepalli, K.; Boulanger, A.; et al. Impacts of social distancing policies on mobility and COVID-19 case growth in the US. Nat. Commun. 2021, 12, 3118. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | Infection Rates | |
|---|---|---|
| B | p 1 | |
| Overall social vulnerability index (SVI) | 0.36 | ** |
| Socioeconomic status subindex (SVI1) | 0.08 | |
| Household characteristics and disability subindex (SVI2) | 0.71 | *** |
| Racial/ethnic minority status and language subindex (SVI3) | 0.42 | *** |
| Housing type and transportation subindex (SVI4) | 0.34 | *** |
| Level | Variance Component | Contribution Ratio | Degree of Freedom | Chi-Square | p 1 |
|---|---|---|---|---|---|
| 2 | 0.51 | 0.67 | 50 | 2642.831 | *** |
| 1 | 0.25 | 0.33 |
| Fixed Effect | |||
|---|---|---|---|
| Parameter | Correlation Coefficient | T | p 1 |
| INTRCPT2, γ00 | −0.8757 | −8.3627 | *** |
| School closure(C1), γ01 | −0.2963 | −3.8930 | *** |
| Workplace closure(C2),γ02 | −0.7016 | −6.3153 | *** |
| Public transport closure(C3), γ03 | −0.2265 | −2.0523 | * |
| Internal movement restrictions(C4), γ04 | −0.6643 | −5.8852 | *** |
| SVI1, γ10 | 1.7160 | 10.9709 | *** |
| SVI2, γ20 | −0.6052 | −6.35301 | *** |
| SVI3, γ30 | 3.1622 | 25.4515 | *** |
| SVI4, γ40 | 1.4475 | 17.5870 | *** |
| Random Effect | |||
| Parameter | Standard Deviation | Variance Component | p |
| INTRCPT1, u0 | 0.77267 | 0.59701 | *** |
| SVI1 slope, u1 | 0.93057 | 0.86596 | *** |
| SVI2 slope, u2 | 0.49347 | 0.24352 | *** |
| SVI3 slope, u3 | 0.62611 | 0.39201 | *** |
| SVI4 slope, u4 | 0.39923 | 0.15938 | *** |
| r | 0.68458 | 0.46865 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, Z.; Li, L.; Ma, J.; Tang, Z.; Shen, H.; Zhu, H.; Wu, B. Moderating Effect of a Cross-Level Social Distancing Policy on the Disparity of COVID-19 Transmission in the United States. ISPRS Int. J. Geo-Inf. 2022, 11, 229. https://doi.org/10.3390/ijgi11040229
Luo Z, Li L, Ma J, Tang Z, Shen H, Zhu H, Wu B. Moderating Effect of a Cross-Level Social Distancing Policy on the Disparity of COVID-19 Transmission in the United States. ISPRS International Journal of Geo-Information. 2022; 11(4):229. https://doi.org/10.3390/ijgi11040229
Chicago/Turabian StyleLuo, Zhenwei, Lin Li, Jianfang Ma, Zhuo Tang, Hang Shen, Haihong Zhu, and Bin Wu. 2022. "Moderating Effect of a Cross-Level Social Distancing Policy on the Disparity of COVID-19 Transmission in the United States" ISPRS International Journal of Geo-Information 11, no. 4: 229. https://doi.org/10.3390/ijgi11040229
APA StyleLuo, Z., Li, L., Ma, J., Tang, Z., Shen, H., Zhu, H., & Wu, B. (2022). Moderating Effect of a Cross-Level Social Distancing Policy on the Disparity of COVID-19 Transmission in the United States. ISPRS International Journal of Geo-Information, 11(4), 229. https://doi.org/10.3390/ijgi11040229