
Important Preliminary Insights for Designing Successful Communication between a Robotic Learning Assistant and Children with Autism Spectrum Disorder in Germany


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
1.1. Challenges for Children with Autism and Their Caregivers
1.2. Using (New) Technologies to Support Children with Autism
1.3. Requirements for Social Robots to Be Used for Children with Autism
1.4. AI-Equipped Robotic Learning Assistant for Children with Autism Spectrum Disorder
1.5. Research Questions
2. Materials and Methods
2.1. Sample
2.1.1. Parent Interviews
2.1.2. Therapist Interviews
2.2. Procedure
3. Results
3.1. Current Therapeutic Situation
3.2. Therapeutic Learning Areas
3.3. Challenges and Deficits
3.4. Disruptive vs. Beneficial Learning Factors
3.5. Usage of (New) Technologies
3.6. Usage of a Robotic Learning Assistant in ASD Therapy
3.6.1. Perceived Benefits and Concerns
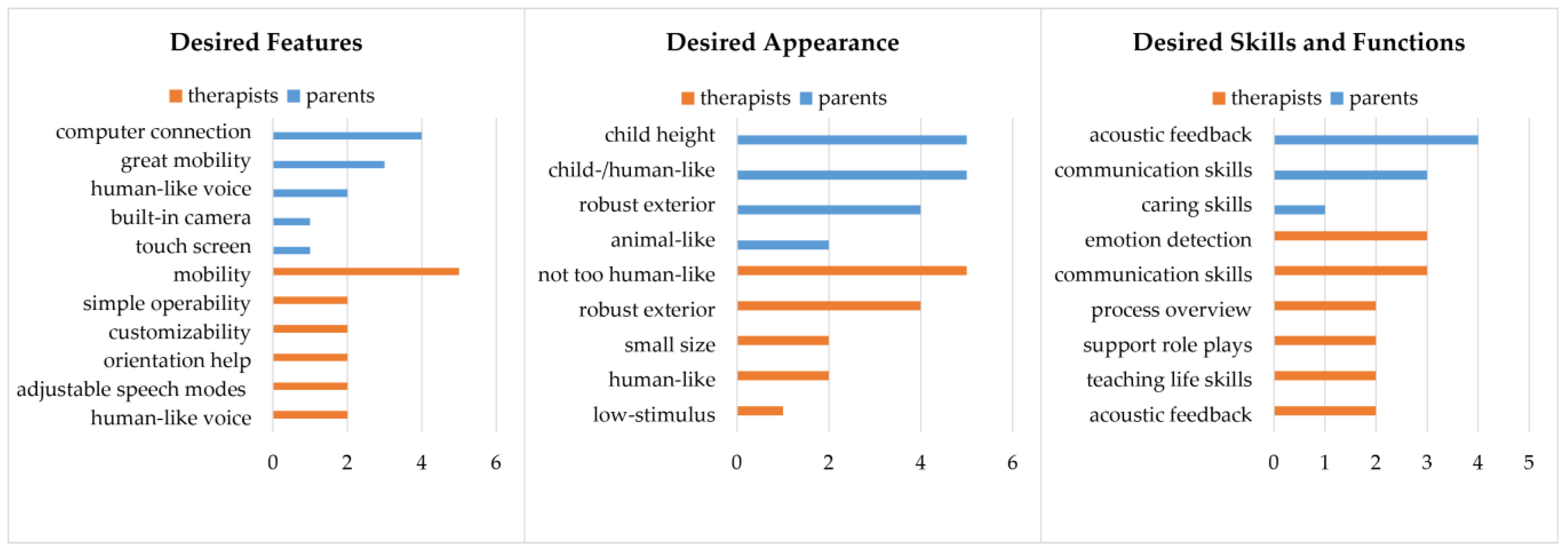
3.6.2. Desired Features, Appearance, and Functions
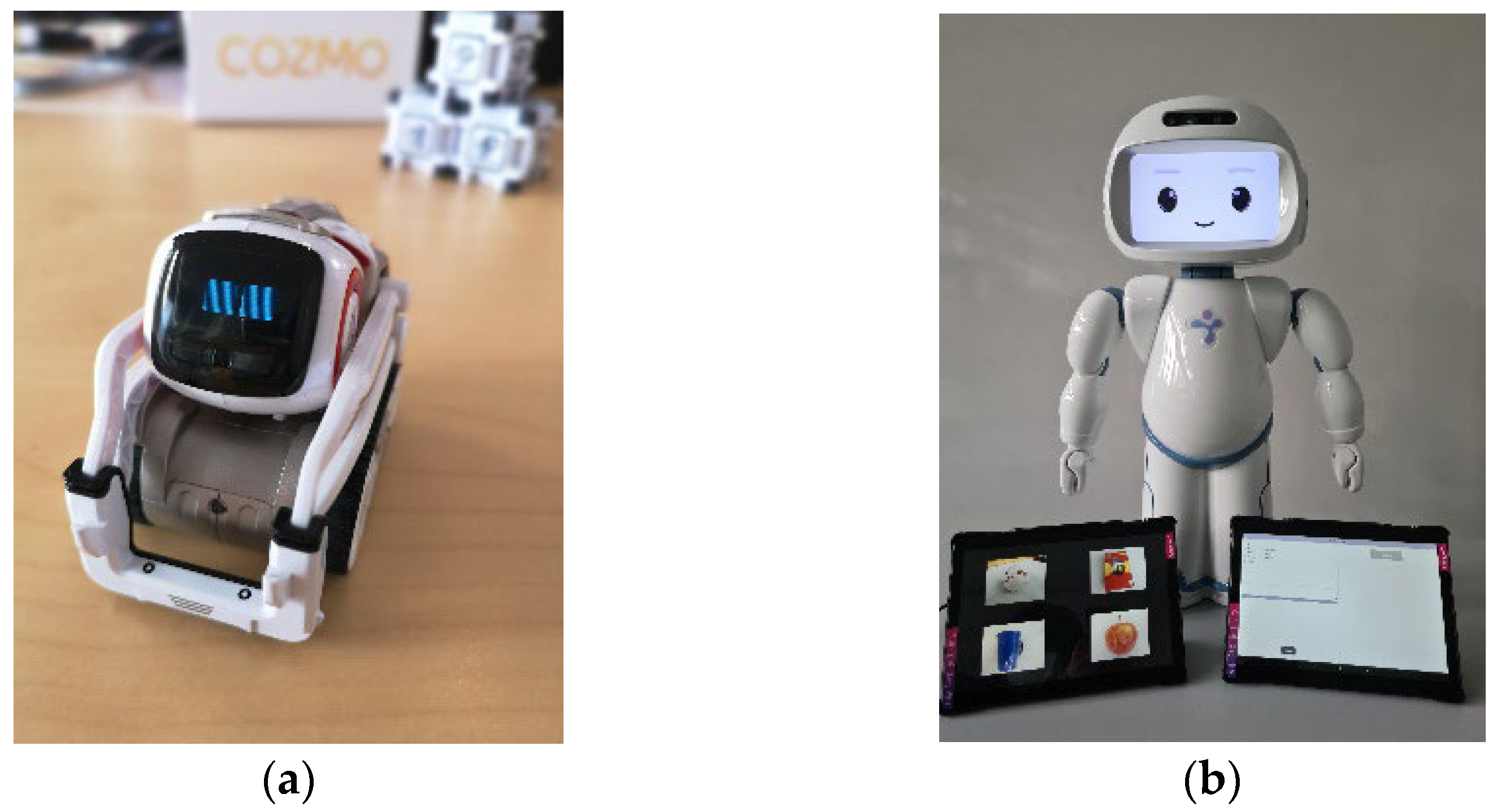
3.6.3. Perceived Benefits and Concerns Regarding Cozmo and QTrobot as Robotic Learning Assistants
4. Discussion
4.1. Limitations and Future Research
4.2. Outlook: Detecting Engagement in Children with Autism
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Interview Guide Parents
Appendix A.1. Introduction
Appendix A.2. Sociodemographic Data and Consent for Audio Recording
Appendix A.3. Warm-Up Questions/General Conditions
- Which psychotherapeutic treatment measures have you used for your child to treat the autism spectrum disorder so far?
- Outpatient/at home?
- Form/s of therapy: ABA/ABT, others?
- How long did the treatment last in total or for how long is it already going?
- At what intervals did/do the therapy sessions take place?
- How long did you have to wait for your treatment to begin?
- How did you bridge the gap until the start of treatment?
- Self-help services? Online information platforms? Unspecified therapy forms (e.g., Occupational therapy, special needs education, alternative medicine approaches)?
- In which situations would you have wished for more help?
Appendix A.4. Individual Learning Goals
- What learning deficits have you observed in your child?
- Can you name which (disturbing) emotions occur especially in specific learning situations (e.g., anger, frustration, etc.)?
- Can you name the most important (learning) goals for your child?
- In which situations/with which tasks in everyday life does your child particularly need a lot of attention and support from you/family members?
- In which situations do you encounter the greatest limitations in supporting your child?
- In which everyday situations would you wish for more support?
- Would you wish for more material on a specific category of exercises? If yes, on which ones?
Appendix A.5. Therapy Sessions
- How does a therapy session usually take place? Do you recognize a certain structure?
- Are there certain overarching themes that are discussed intensively? If yes, which ones?
- What do you experience as particularly helpful within the therapy sessions? Any specific exercises? A certain therapist’s attitude?
- Is there something that you miss within the therapy sessions/something, that is difficult/something that you would like to be different? If yes, what?
- Are you and/or your child preparing for a therapy session? If yes, in what way?
- How do you and your child organize the time after the therapy session?
- Do you follow up on a therapy session? If yes, in what way?
- Do you use progress monitoring sheets?
- How do you and your child experience the amount of time you spent for the therapy sessions? (just right, too high, too low)
- How much time do you usually spend during one week on activities that are part of the therapy? [in hours]
- How do you manage to integrate them into your everyday life?
Appendix A.6. Homework
- Are there any exercises from the therapy that you can do at home on your own–without the help of your therapist? If yes, which ones?
- Are there any exercises that your child does independently without the help of you or the therapist? If yes, which ones?
- How do you experience the tasks carried out independently? Are there sometimes difficulties in the execution? If yes, which ones?
- Is there anything you would wish for concerning the implementation of exercises in the home setting? What would help you to use the exercises more often or more successful in everyday life at home?
- In which everyday situations would you wish for more help in carrying them out?
Appendix A.7. Technology—Status Quo
- Have you and your child ever used technological devices or media within the therapy (e.g., in the context of performing certain exercises)? If yes, which devices or media did you use? How did you experience it? Rather positive or negative?
- What is your general opinion on the use of modern technologies (e.g., a robot, an online platform) in the context of psychotherapy?
- Are there aspects of the use of modern technologies within psychotherapy that you see critically or that you are concerned about?
Appendix A.8. Acceptance Platform
- Can you name specific situations in which you could have used quick, easy access to information or learning units?
- How important is it to you that information material on the causes of ASD is easily available?
- Would that have helped you shortly after the diagnosis?
- How did you inform yourself at the time?
- Would you like to have more information specifically about ABA?
- How important is the easy availability of scientific information material on exercises for specific learning objectives for you?
- Do you already make use of online materials? If yes, which ones/where?
- What do you like most about these?
- What do you like less about these?
- What are you missing?
- What do you expect from an online learning platform?
- Do you feel technically confident enough to use an online platform?
- Would you store personal data [data about your child] on an online platform?
- Would you prefer a freely accessible platform or a website with a user login? Why/Why not?
- In your opinion, would it make sense to offer the online platform and the materials available on it in several languages?
- If yes, which languages would you suggest?
- In your opinion, should both the learning materials (for children) and the platform (for children/parents) or just one of each be available in multiple languages?
Appendix A.9. Interaction Child/Platform
- In addition to the material that you could use with your child, would you also wish for interactive content for your child? (e.g., videos with questions, self-tests, etc.)
- If yes, what interactive content would you be particularly interested in?
- In general, is your child interested in technology?
- Do you think your child can independently use interactive video materials on the PC? If no, why not?
- In your opinion, what forms of positive reinforcement would be most useful (video sequences, games, etc.)?
- What potential problems do you anticipate in your child’s use of an online platform?
Appendix A.10. Acceptance Robots
- The project aims to develop a robot that uses artificial intelligence to recognize the emotions of autistic children. We will consult you as experts to find out when and where such a robot would be most useful to you and your child.
- What is your general attitude towards robots
- What is your general attitude towards artificial intelligence?
- Assuming that all data is stored following data protection regulations, e.g., with your therapist, and is not passed on. Would you agree to your child’s voice and video data being collected by the robot to improve emotion recognition? Why/Why not?
- If not, would you consider a robot that only stores this data on your personal computer?
- Do you think your child would accept a robot as a companion?
- What would be necessary to achieve that?
- Do you think your child would prefer a more human (childlike) looking robot?
- Assuming your child achieves good progress regarding his learning goals within the therapy sessions using the robot. Would you also buy a robot to use at home?
- Do you see any possibilities for financing such a robot, privately or through associations or institutes, etc.? Or how much money could you imagine investing here?
- How big should the robot ideally be?
- Do you think the robot should be mobile or is it enough if it can be placed in the room (e.g., children’s room)?
- In which spatial environments do you think you would use the robot? Outdoors/in a domestic context?
- Should it be shockproof or waterproof?
- Do you own a computer? If yes, which kind of computer?
- Would you also use the robot if it only worked in interaction with a PC?
Appendix A.10.1. QTrobot
- What is your first impression of the robot?
- Can you imagine this kind of robot as a support within the therapy/in the interaction with your child? If no, why not?
- Can you imagine using this type of robot alone, without the support of your therapist? If no, why not?
- Do you think your child would treat the robot carefully during the interaction?
- Do you think your child would accept this robot as a companion? If no, why not?
Appendix A.10.2. Cozmo
- What is your first impression of the robot?
- Can you imagine this kind of robot as a support within the therapy/in the interaction with your child? If no, why not?
- Can you imagine using this type of robot alone, without the support of your therapist? If no, why not?
- Do you think your child would treat the robot carefully during the interaction?
- Do you think your child would accept this robot as a companion? If no, why not?
Appendix A.10.3. Acceptance Robot (Conclusion)
- Which of the two robots could you rather imagine using together with your child?
- Positive aspects robot 1 (QTrobot)/robot 2 (Cozmo)
Appendix A.11. Closing
- Is there anything else that you feel is important and would like to share with us that has not yet been addressed? Thank you very much for your participation!
Appendix B. Interview Guide Therapists
Appendix B.1. Introduction
Appendix B.2. Sociodemographic Data and Consent for Audio Recording
Appendix B.3. Warm-Up Questions/General Conditions
- How did you start with ASD therapy?
- How long have you been working at/for your institute/employer?
- How long have you been working as a therapist?
- How long have you been working with ASD patients?
Appendix B.4. Psychotherapy
- What is a typical working day like in your institution?
- What percentage of the work is related to the direct or indirect treatment of ASD patients?
- What are the general conditions of a typical treatment of ASD patients in your institution? Outpatient/in the home environment?
- Types of treatment: ABA, TEACCH, DIR/Floortime, others?
- Average length of treatment (per session & total length)?
- How are your treatment rooms designed?
- In general, how does a typical treatment of ASD patients take place in your institution?
- What are the modules/components of the form of therapy you use?
- What tools do you use during a therapy session?
- How much time do you have for each patient? How much time do you have in between patients?
- What is the percentage of patients for whom you use autism-specific behavioral therapy?
- How do you decide whether autism-specific behavioral therapy is appropriate for the patient?
- How do you organize aftercare? Are there special structures for aftercare?
- In which way and at which point in time (at which intervals) and with which instruments do you record the patient’s condition?
- Do you use progress monitoring forms? If yes, in which form (digital, on paper)?
Appendix B.5. Opportunities
- Which parts of a therapy session are challenging for you?
- Are there any problems that occur frequently during a therapy session?
- Administrative/organizational problems?
- Content related problems?
- How do you fix these problems? How do manage to continue despite the problems?
- With what do your patients seem to have most problems?
- How do you fix these problems? How do manage to continue despite the problems?
- On which subjects would you like to have more information that are easily accessible?
- When and how would you obtain this information?
- What form would be most suitable for you (e.g., videos, work instructions/material, literature)?
Appendix B.6. Patients
- How old are the patients you provide treatment for (on average)?
- How many families with a migration background do you supervise?
- In which languages do you mainly communicate with your patients and their relatives?
- Are there any specifics in dealing with patients or their relatives who have a migration background?
- Language barriers? Other challenges?
Appendix B.7. Technology Status-Quo
- What is your general opinion on the use of modern technologies in psychotherapy?
- Are there any aspects that you see critically concerning the use of modern technologies within psychotherapy or that you are concerned about?
- Do you have experience with the use of technical tools in psychotherapy?
- Experiences with online tools/(therapy) robots/e-learning?
Appendix B.8. Acceptance Platform
- Do you already make use of online materials?
- If yes, which ones?
- What do you particularly like about them? What do you like less about them?
- What are you missing?
- What do you expect from the therapy assistance through the online platform?
- How do you imagine the use of the online platform in different therapy situations?
- Do you have the impression that your patients are generally interested in technology?
- Do you think your patients could–with your guidance–use interactive video materials on the computer on their own? If no, why not?
- What potential problems do you anticipate in your patients’ interaction with an online platform?
- In your opinion, would it make sense to offer the online platform and the materials available on it in several languages?
- If yes, which languages would you suggest for it?
- In your opinion, should both the learning materials (for children) and the platform (for children/parents) or only one of both be available in multiple languages?
Appendix B.9. Acceptance Robots
- Imagine that a robot could support patients in their daily lives. What characteristics would you give the robot or what would you like it to have?
- What do you expect from the therapy assistance provided by the robot?
- Do you think the robot should be mobile or is it enough if it can be placed in the room (e.g., children’s room)?
- In your opinion, what are the advantages and disadvantages of a static or mobile robot?
- In which spatial environments would you imagine to use the robot? Outside, domestic environment?
- Do you think your patients would accept a robot as a companion?
- What would be important for that?
- Do you think your patients would prefer a more human (childlike) looking robot?
Appendix B.9.1. QTrobot
- What is your first impression of the robot?
- Can you imagine using this kind of robot for therapy purposes? If yes–how do you imagine the use of the robot in different therapy situations? If no, why not?
- How often do you imagine using the robot as a tool in the therapy sessions?
- Do you think your patients would be careful in interaction with the robot?
- Do you think your patients would accept this robot as a companion? If no, why not?
Appendix B.9.2. Cozmo
- What is your first impression of the robot?
- Can you imagine using this kind of robot for therapy purposes? If yes, how do you imagine the use of the robot in different therapy situations? If no, why not?
- How often do you imagine to use the robot as a tool in the therapy sessions?
- Do you think your patients would be careful in interaction with the robot?
- Do you think your patients would accept this robot as a companion? If no, why not?
Appendix B.9.3. Acceptance Robot (Conclusion)
- Which of the two robots could you rather imagine working with?
- Positive aspects Robot 1 (QTrobot)/Robot 2 (Cozmo)
- Negative Aspects Robot 1 (QTrobot)/Robot 2 (Cozmo)
Appendix B.10. Part 10: Closing
References
- Swaggart, B.L.; Gagnon, E.; Bock, S.J.; Earles, T.L.; Quinn, C.; Myles, B.S.; Simpson, R.L. Using social stories to teach social and behavioral skills to children with autism. Focus Autistic Behav. 1995, 10, 1–16. [Google Scholar] [CrossRef]
- Wing, L. Social behavioral and cognitive characteristics: An epidemiological approach. In Autism; Rutter, M., Schopler, E., Eds.; Springer: Boston, MA, USA, 1978; pp. 27–45. ISBN 978-1-4684-0789-1. [Google Scholar]
- Habermann, L.; Kißler, C. Das autistische Spektrum aus Wissenschaftlicher, Therapeutischer und Autistischer Perspektive [The Autistic Spectrum from Scientific, Therapeutical, and Autistic Perspective]; Springer: Wiesbaden, Germany, 2022; ISBN 978-3-658-37601-7. [Google Scholar]
- Bölte, S. Symptomatik und Klassifikation [Symptoms and classification]. In Autismus. Spektrum, Ursachen, Diagnostik, Intervention, Perspektiven. [Autism. Spectrum, Causes, Diagnosis, Interventions, Perspectives]; Bölte, S., Ed.; Hans Huber: Göttingen, Germany, 2009; pp. 31–45. [Google Scholar]
- Dziobek, I.; Rogers, K.; Fleck, S.; Bahnemann, M.; Heekeren, H.R.; Wolf, O.T.; Convit, A. Dissociation of cognitive and emotional empathy in adults with Asperger syndrome using the Multifaceted Empathy Test (MET). J. Autism Dev. Disord. 2008, 38, 464–473. [Google Scholar] [CrossRef] [PubMed]
- Krasny, L.; Williams, B.J.; Provencal, S.; Ozonoff, S. Social skills interventions for the autism spectrum: Essential ingredients and a model curriculum. Child Adolesc. Psychiatr. Clin. North Am. 2003, 12, 107–122. [Google Scholar] [CrossRef]
- Sallows, G.O.; Graupner, T.D. Intensive Behavioral Treatment for Children With Autism: Four-Year Outcome and Predictors. Am. J. Ment. Retard. 2005, 110, 417–438. [Google Scholar] [CrossRef]
- Peca, A.; Coeckelbergh, M.; Simut, R.; Costescu, C.; Pintea, S.; David, D.; Vanderborght, B. Robot enhanced therapy for children with autism disorders: Measuring ethical a cceptability. IEEE Technol. Soc. Mag. 2016, 35, 54–66. [Google Scholar] [CrossRef]
- Crowe, B.H.A.; Salt, A.T. Autism: The management and support of children and young people on the autism spectrum (NICE Clinical Guideline 170). Arch. Dis. Child. Educ. Pract. 2015, 100, 20–23. [Google Scholar] [CrossRef]
- Freitag, C.M. Autism Spectrum Disorders in Childhood, Adolescence and Adulthood, Part 2: Therapy: Interdisciplinary S3 Guideline of the DGKJP and the DGPPN as well as the Participating Professional Societies, Professional Associations and Patient Organisations. Available online: https://www.awmf.org/leitlinien/detail/ll/028-047.html (accessed on 19 August 2022).
- Wong, C.; Odom, S.L.; Hume, K.A.; Cox, A.W.; Fettig, A.; Kucharczyk, S.; Brock, M.E.; Plavnick, J.B.; Fleury, V.P.; Schultz, T.R. Evidence-based practices for children, youth, and young adults with Autism Spectrum Disorder: A comprehensive review. J. Autism Dev. Disord. 2015, 45, 1951–1966. [Google Scholar] [CrossRef]
- Weinmann, S.; Schwarzbach, C.; Begemann, M.; Roll, S.; Vauth, C.; Willich, S.N.; Greiner, W. Behavioural and skill-based early interventions in children with autism spectrum disorders. GMS Health Technol. Assess. 2009, 5, Doc10. [Google Scholar] [CrossRef]
- Donnellan, A.M.; Kilman, B.A. Behavioral approaches to social skill development in autism. In Social Behavior in Autism; Schopler, E., Mesibov, G.B., Eds.; Springer: Boston, MA, USA, 1986; pp. 213–236. ISBN 978-1-4899-2244-1. [Google Scholar]
- Herbrecht, E.; Poustka, F.; Birnkammer, S.; Duketis, E.; Schlitt, S.; Schmötzer, G.; Bölte, S. Pilot evaluation of the Frankfurt Social Skills Training for children and adolescents with autism spectrum disorder. Eur. Child Adolesc. Psychiatry 2009, 18, 327–335. [Google Scholar] [CrossRef]
- Corsello, C.M. Early intervention in autism. Infants Young Child 2005, 18, 74–85. [Google Scholar] [CrossRef]
- Smith, T. Outcome of early intervention for children with autism. Clin. Psychol. Sci. Pract. 1999, 6, 33–49. [Google Scholar] [CrossRef]
- Kendall, T.; Megnin-Viggars, O.; Gould, N.; Taylor, C.; Burt, L.R.; Baird, G. Management of autism in children and young people: Summary of NICE and SCIE guidance. BMJ 2013, 347, f4865. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Reichow, B.; Hume, K.; Barton, E.E.; Boyd, B.A. Early intensive behavioral intervention (EIBI) for young children with autism spectrum disorders (ASD). Cochrane Database Syst. Rev. 2018, 5, CD009260. [Google Scholar] [CrossRef] [PubMed]
- Rabsahl, A.K. Aktive Elternrolle bei der Therapie von Autismus-Spektrum-Störungen: Belastungen nehmen, Kompetenzen Fördern; Springer Spektrum: Wiesbaden, Germany, 2016; ISBN 9783658110307. [Google Scholar]
- Murray, M.J. Attention-Deficit/Hyperactivity Disorder in the context of Autism Spectrum Disorders. Curr. Psychiatry Rep. 2010, 12, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Conn, K.; Sarkar, N.; Stone, W. Physiology-based affect recognition for computer-assisted intervention of children with Autism Spectrum Disorder. Int. J. Hum. Comput. Stud. 2008, 66, 662–677. [Google Scholar] [CrossRef]
- Bachmann, C.; Hoffmann, F. Autismus-Spektrum-Störungen in Deutschland: Diagnoseprävalenz, Versorgung und zeitliche Trends [Autism Spectrum Disorders in Germany: Diagnosis prevalence, treatment, and time trends]. In Versorgungs-Report 2015/2016 Schwerpunkt: Kinder und Jugendliche; Klauber, J., Günster, C., Gerste, B., Robra, B.-P., Schmacke, N., Eds.; Schattauer: Stuttgart, Germany, 2016; pp. 167–184. [Google Scholar]
- Röttgers, H.R.; Rentmeister, K. Alltagsorientiertes Lernen von Menschen mit Autismus, 1. ed.; Kohlhammer: Stuttgart, Germany, 2020; ISBN 9783170330252. [Google Scholar]
- Venkatesh, S.; Greenhill, S.; Phung, D.; Adams, B.; Duong, T. Pervasive multimedia for autism intervention. Pervasive Mob. Comput. 2012, 8, 863–882. [Google Scholar] [CrossRef]
- Johnston, K.J.; Wen, H.; Joynt Maddox, K.E. Lack of access to specialists associated with mortality and preventable hospitalizations of rural medicare beneficiaries. Health Aff. 2019, 38, 1993–2002. [Google Scholar] [CrossRef]
- Rieger, M.O.; Wang, M.; Massloch, M.; Reinhardt, D. Opinions on technology: A cultural divide between East Asia and Germany? Rev. Behav. Econ. 2021, 8, 73–110. [Google Scholar] [CrossRef]
- Lord, C.; Cook, E.H.; Leventhal, B.L.; Amaral, D.G. Autism Spectrum Disorders. Neuron 2000, 28, 355–363. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of mental Disorders: DSM-5, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013; ISBN 0-89042-555-8. [Google Scholar]
- Pennisi, P.; Tonacci, A.; Tartarisco, G.; Billeci, L.; Ruta, L.; Gangemi, S.; Pioggia, G. Autism and social robotics: A systematic review. Autism Res. Off. J. Int. Soc. Autism Res. 2016, 9, 165–183. [Google Scholar] [CrossRef]
- Welch, K.C.; Lahiri, U.; Warren, Z.; Sarkar, N. An Approach to the Design of Socially Acceptable Robots for Children with Autism Spectrum Disorders. Int. J. Soc. Robot. 2010, 2, 391–403. [Google Scholar] [CrossRef]
- Keen, D. Engagement of children with autism in learning. Australas. J. Spec. Educ. 2009, 33, 130–140. [Google Scholar] [CrossRef]
- O’Brien, G.; Pearson, J. Autism and learning disability. Autism 2004, 8, 125–140. [Google Scholar] [CrossRef]
- Canitano, R.; Scandurra, V. Psychopharmacology in autism: An update. Prog. Neuropsychopharmacol. Biol. Psychiatry 2011, 35, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Keenan, M. Eltern als Therapeuten von Kindern mit Autismus-Spektrum-Störungen: Selbständigkeit fördern mit Applied Behaviour Analysis; Kohlhammer Verlag: Stuttgart, Germany, 2014; ISBN 9783170285743. [Google Scholar]
- Klauber, J.; Günster, C.; Gerste, B.; Robra, B.-P.; Schmacke, N. (Eds.) Versorgungs-Report 2015/2016 Schwerpunkt: Kinder und Jugendliche; Schattauer: Stuttgart, Germany, 2016. [Google Scholar]
- Lambert, M.; Bock, T.; Naber, D.; Löwe, B.; Schulte-Markwort, M.; Schäfer, I.; Gumz, A.; Degkwitz, P.; Schulte, B.; König, H.H.; et al. Die psychische Gesundheit von Kindern, Jugendlichen und jungen Erwachsenen Teil 1: Häufigkeit, Störungspersistenz, Belastungsfaktoren, Service-Inanspruchnahme und Behandlungsverzögerung mit Konsequenzen [The mental health of children, adolescents and young adults Part 1: Frequency, disorder persistence, stress factors, service use, and treatment delay with consequences]. Fortschr. Neurol. Psychiatr. 2013, 81, 614–627. [Google Scholar] [CrossRef] [PubMed]
- Wend-Erdel, M. Die Finanzierungssituation Evidenzbasierter Fördermaßnahmen für autistische Kinder; Weidler: Berlin. Germany, 2011. [Google Scholar]
- Keenan, M.; Dillenburger, K.; Röttgers, H.R.; Dounavi, K.; Jónsdóttir, S.L.; Moderato, P.; Schenk, J.J.A.M.; Virués-Ortega, J.; Roll-Pettersson, L.; Martin, N. Autism and ABA: The gulf between North America and Europe. Rev. J. Autism Dev. Disord. 2015, 2, 167–183. [Google Scholar] [CrossRef]
- Wood, L.J.; Zaraki, A.; Robins, B.; Dautenhahn, K. Developing Kaspar: A humanoid robot for children with autism. Int. J. Soc. Robot. 2021, 13, 491–508. [Google Scholar] [CrossRef] [PubMed]
- Faraj, A.; Alzahrani, S.; Almumtin, R.; Alrajhi, D.; Alshyban, S.; Alshabanah, M.; Alsmadi, M.; Almarashdeh, I. Developing and implementing an online learning platform for children with autism. Int. J. Sci. Res. Sci. Technol. 2020, 7, 176–188. [Google Scholar] [CrossRef]
- Konstantinidis, E.I.; Hitoglou-Antoniadou, M.; Luneski, A.; Bamidis, P.D.; Nikolaidou, M.M. Using affective avatars and rich multimedia content for education of children with autism. In Proceedings of the 2nd International Conference on Pervsive Technologies Related to Assistive Environments—PETRA’09, Corfu Greece, 9–13 June 2009; ACM: New York, NY, USA, 2009; pp. 1–6, ISBN 9781605584096. [Google Scholar]
- Holeva, V.; Nikopoulou, V.A.; Lytridis, C.; Bazinas, C.; Kechayas, P.; Sidiropoulos, G.; Papadopoulou, M.; Kerasidou, M.D.; Karatsioras, C.; Geronikola, N.; et al. Effectiveness of a robot-assisted psychological intervention for children with autism apectrum disorder. J. Autism Dev. Disord. 2022, 52, 1–17. [Google Scholar] [CrossRef]
- Chevalier, P.; Li, J.J.; Ainger, E.; Alcorn, A.M.; Babovic, S.; Charisi, V.; Petrovic, S.; Schadenberg, B.R.; Pellicano, E.; Evers, V. Dialogue design for a robot-based face-mirroring game to engage autistic children with emotional expressions. In Social Robotics; Kheddar, A., Yoshida, E., Ge, S.S., Suzuki, K., Cabibihan, J.-J., Eyssel, F., He, H., Eds.; Springer: Cham, Switzerland, 2017; pp. 546–555. ISBN 978-3-319-70021-2. [Google Scholar]
- Ferrari, E.; Robins, B.; Dautenhahn, K. Therapeutic and educational objectives in robot assisted play for children with autism. In Proceedings of the 18th IEEE International Symposium on Robot and Human Interactive Communication—RO-MAN’09, Toyama, Japan, 27 September–2 October 2009; IEEE: Piscataway, NJ, USA, 2009; pp. 108–114. [Google Scholar]
- Kozima, H.; Nakagawa, C.; Yasuda, Y. Children–robot interaction: A pilot study in autism therapy. In Progress in Brain Research: From Action to Cognition; Von Hofsten, C., Rosander, K., Eds.; Elsevier: Amsterdam, The Netherlands, 2007; pp. 385–400. ISBN 9780444530165. [Google Scholar]
- Ricks, D.J.; Colton, M.B. Trends and considerations in robot-assisted autism therapy. In Proceedings of the 2010 IEEE International Conference on Robotics and Automation—ICRA’10, Online, 6–12 December 2020; IEEE: Piscataway, NJ, USA, 2010; pp. 4354–4359, ISBN 978-1-4244-5038-1. [Google Scholar]
- Robins, B.; Dautenhahn, K.; Boekhorst, R.T.; Billard, A. Robotic assistants in therapy and education of children with autism: Can a small humanoid robot help encourage social interaction skills? Univers. Access Inf. Soc. 2005, 4, 105–120. [Google Scholar] [CrossRef]
- Huijnen, C.A.G.J.; Lexis, M.A.S.; Jansens, R.; de Witte, L.P. Mapping robots to therapy and educational objectives for children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2016, 46, 2100–2114. [Google Scholar] [CrossRef]
- Papakostas, G.A.; Sidiropoulos, G.K.; Papadopoulou, C.I.; Vrochidou, E.; Kaburlasos, V.G.; Papadopoulou, M.T.; Holeva, V.; Nikopoulou, V.-A.; Dalivigkas, N. Social robots in special education: A systematic review. Electronics 2021, 10, 1398. [Google Scholar] [CrossRef]
- Dautenhahn, K. Socially intelligent robots: Dimensions of human-robot interaction. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 2007, 362, 679–704. [Google Scholar] [CrossRef] [PubMed]
- Cabibihan, J.-J.; Javed, H.; Ang, M.; Aljunied, S.M. Why robots? A survey on the roles and benefits of social robots in the therapy of children with autism. Int. J. Soc. Robot. 2013, 5, 593–618. [Google Scholar] [CrossRef]
- Scassellati, B. How social robots will help us to diagnose, treat, and understand autism. In Robotics Research; Thrun, S., Brooks, R., Durrant-Whyte, H., Eds.; Springer: Berlin/Heidelberg, Germany, 2007; pp. 552–563. ISBN 978-3-540-48110-2. [Google Scholar]
- Giullian, N.; Ricks, D.; Atherton, A.; Colton, M.; Goodrich, M.; Brinton, B. Detailed requirements for robots in autism therapy. In Proceedings of the 2010 IEEE International Conference on Systems, Man and Cybernetics, Istanbul, Turkey, 10–13 October 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 2595–2602. [Google Scholar]
- Scassellati, B.; Admoni, H.; Matarić, M. Robots for use in autism research. Annu. Rev. Biomed. Eng. 2012, 14, 275–294. [Google Scholar] [CrossRef]
- Van Straten, C.L.; Smeekens, I.; Barakova, E.; Glennon, J.; Buitelaar, J.; Chen, A. Effects of robots’ intonation and bodily appearance on robot-mediated communicative treatment outcomes for children with autism spectrum disorder. Pers. Ubiquitous Comput. 2018, 22, 379–390. [Google Scholar] [CrossRef]
- Robins, B.; Dautenhahn, K.; Dubowski, J. Does appearance matter in the interaction of children with autism with a humanoid robot? Interact. Stud. 2006, 7, 479–512. [Google Scholar] [CrossRef]
- Hanson, D.; Mazzei, D.; Garver, C.; Ahluwalia, A.; De Rossi, D.; Stevenson, M.; Reynolds, K. Realistic humanlike robots for treatment of ASD, social training, and research; shown to appeal to youths with ASD, cause physiological arousal, and increase human-to-human social engagement. In Proceedings of the 5th International Conference on PErvasive Technologies Related to Assistive Environments—PETRA’12, Online, 6–12 December 2020; ACM: New York, NY, USA, 2012; pp. 1–7. [Google Scholar]
- Coeckelbergh, M.; Pop, C.; Simut, R.; Peca, A.; Pintea, S.; David, D.; Vanderborght, B. A survey of expectations about the role of robots in robot-assisted therapy for children with ASD: Ethical acceptability, trust, sociability, appearance, and attachment. Sci. Eng. Ethics 2016, 22, 47–65. [Google Scholar] [CrossRef]
- Sochanski, M.; Snyder, K.; Korneder, J.; Louie, W.-Y.G. Therapists’ perspectives after implementing a robot into autism therapy. In Proceedings of the 2021 30th IEEE International Conference on Robot & Human Interactive Communication (RO-MAN), Vancouver, BC, Canada, 8–12 August 2021; IEEE: Piscataway, NJ, USA, 2021; pp. 1216–1223, ISBN 978-1-6654-0492-1. [Google Scholar]
- Alcorn, A.M.; Ainger, E.; Charisi, V.; Mantinioti, S.; Petrović, S.; Schadenberg, B.R.; Tavassoli, T.; Pellicano, E. Educators’ views on using humanoid robots with autistic learners in special education settings in England. Front. Robot. AI 2019, 6, 107. [Google Scholar] [CrossRef]
- Richardson, K.; Coeckelbergh, M.; Wakunuma, K.; Billing, E.; Ziemke, T.; Gomez, P.; Vanderborght, B.; Belpaeme, T. Robot enhanced therapy for children with autism (DREAM): A social model of autism. IEEE Technol. Soc. Mag. 2018, 37, 30–39. [Google Scholar] [CrossRef]
- Conti, D.; Di Nuovo, S.; Buono, S.; Di Nuovo, A. Robots in education and care of children with developmental disabilities: A study on acceptance by experienced and future professionals. Int. J. Soc. Robot. 2017, 9, 51–62. [Google Scholar] [CrossRef]
- Dautenhahn, K.; Werry, I. Towards interactive robots in autism therapy. Pragmat. Cogn. 2004, 12, 1–35. [Google Scholar] [CrossRef]
- Mutlu, B.; Forlizzi, J. Robots in organizations. In Proceedings of the 3rd International Conference on Human Robot Interaction—HRI’08, Amsterdam, The Netherlands, 12–15 March 2008; Fong, T., Dautenhahn, K., Scheutz, M., Demiris, Y., Eds.; ACM Press: New York, NY, USA, 2008; pp. 287–294, ISBN 9781605580173. [Google Scholar]
- Hill, E.; Berthoz, S.; Frith, U. Brief report: Cognitive processing of own emotions in individuals with autistic spectrum disorder and in their relatives. J. Autism Dev. Disord. 2004, 34, 229–235. [Google Scholar] [CrossRef]
- Valstar, M.; Schuller, B.; Smith, K.; Eyben, F.; Jiang, B.; Bilakhia, S.; Schnieder, S.; Cowie, R.; Pantic, M. AVEC 2013: The continuous audio/visual emotion and depression recognition challenge. In AVEC’13: Proceedings of the 3rd International Workshop on Audio/Visual Emotion Challenge, Online, 6–12 December 2020; Schuller, B., Valstar, M., Cowie, R., Krajewski, J., Pantic, M., Eds.; ACM: New York City, NY, USA, 2013; pp. 3–10. [Google Scholar]
- Valstar, M.; Schuller, B.; Smith, K.; Almaev, T.; Eyben, F.; Krajewski, J.; Cowie, R.; Pantic, M. AVEC 2014. In Proceedings of the 4th International Workshop on Audio/Visual Emotion Challenge—AVEC’14, Orlando, FL, USA, 7 November 2014; Valstar, M., Schuller, B., Krajewski, J., Cowie, R., Pantic, M., Eds.; ACM: New York, NY, USA, 2014; pp. 3–10, ISBN 9781450331197. [Google Scholar]
- Wöllmer, M.; Metallinou, A.; Eyben, F.; Schuller, B.; Narayanan, S.S. Context-sensitive multimodal emotion recognition from speech and facial expression using bidirectional LSTM modeling. In Proceedings of the 11th Annual Conference of the International Speech Communication Association—INTERSPEECH’10, Dresden, Germany, 6–10 September 2015; ISCA: Baixas, France, 2010; pp. 2362–2365. [Google Scholar]
- Cowie, R.; Douglas-Cowie, E.; Tsapatsoulis, N.; Votsis, G.; Kollias, S.; Fellenz, W.; Taylor, J.G. Emotion recognition in human-computer interaction. IEEE Signal Process. Mag. 2001, 18, 32–80. [Google Scholar] [CrossRef]
- Kaburlasos, V. Social Robots as Tools in Special Education. Available online: http://humain-lab.cs.ihu.gr/index.php/portfolio-item/koiro3e/?lang=en (accessed on 19 August 2022).
- Lytridis, C.; Kaburlasos, V.G.; Bazinas, C.; Papakostas, G.A.; Sidiropoulos, G.; Nikopoulou, V.-A.; Holeva, V.; Papadopoulou, M.; Evangeliou, A. Behavioral data analysis of robot-assisted autism spectrum disorder (ASD) interventions based on Lattice Computing techniques. Sensors 2022, 22, 621. [Google Scholar] [CrossRef]
- Kaburlasos, V.G. Lattice computing: A mathematical modelling paradigm for cyber-physical system applications. Mathematics 2022, 10, 271. [Google Scholar] [CrossRef]
- Kamp-Becker, I.; Duketis, E.; Sinzig, J.; Poustka, L.; Becker, K. Diagnostik und Therapie von Autismus-Spektrum-Störungen im Kindesalter. Kindheit und Entwicklung 2010, 19, 144–157. [Google Scholar] [CrossRef]
- Keenan, M.; Dillenburger, K.; Moderato, P.; Röttgers, H.R. Science for sale in a free market economy: But at what price? ABA and the treatment of autism in Europe. Behav. Soc. Issues 2010, 19, 126–143. [Google Scholar] [CrossRef]
- National Collaborating Centre for Mental Health. Autism: The NICE Guideline on Recognition, Referral, Diagnosis and Management of Adults on the Autism Spectrum: National Clinical Guideline Number 142; The British Psychological Society and The Royal College of Psychiatrists: London, UK, 2012. [Google Scholar]
- LuxAI. QTrobot: Humanoid Social Robot for Human AI Research & teaching. Available online: https://luxai.com/humanoid-social-robot-for-research-and-teaching/ (accessed on 19 August 2022).
- Pelikan, H.R.M.; Broth, M.; Keevallik, L. “Are You Sad, Cozmo?” How humans make sense of a home robot’s emotion displays. In Proceedings of the 2020 ACM/IEEE International Conference on Human-Robot Interaction, Cambridge UK, 23–26 March 2020; Belpaeme, T., Young, J., Gunes, H., Riek, L., Eds.; ACM: New York, NY, USA, 2020; pp. 461–470, ISBN 9781450367462. [Google Scholar]
- Hinz, N.-A.; Ciardo, F.; Wykowska, A. Individual differences in attitude toward robots predict behavior in human-robot interaction. In Social Robotics: Proceedings of the 11th International Conference on Social Robotics—ICSR’19, Madrid, Spain, 26-29 November 2019; Salichs, M.A., Ge, S.S., Barakova, E.I., Cabibihan, J.-J., Wagner, A.R., Castro-González, Á., He, H., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 64–73. ISBN 978-3-030-35887-7. [Google Scholar]
- Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. An application of hierarchical Kappa-type statistics in the assessment of majority agreement among multiple observers. Biometrics 1977, 33, 363. [Google Scholar] [CrossRef] [PubMed]
- Robins, B.; Otero, N.; Ferrari, E.; Dautenhahn, K. Eliciting requirements for a robotic toy for children with autism—Results from user panels. RO-MAN 2007—The 16th IEEE International Symposium on Robot and Human Interactive Communication, Jeju, Republic of Korea, 26–29 August 2007; IEEE: Piscataway, NJ, USA, 2007; pp. 101–106, ISBN 978-1-4244-1634-9. [Google Scholar]
- Krasnova, H.; Veltri, N.F. Privacy calculus on social networking sites: Explorative evidence from Germany and USA. In Proceedings of the 2010 43rd Hawaii International Conference on System Sciences, Honolulu, HI, USA, 5–8 January 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 1–6, ISBN 978-1-4244-5509-6. [Google Scholar]
- Fong, T.; Nourbakhsh, I.; Dautenhahn, K. A survey of socially interactive robots. Robot. Auton. Syst. 2003, 42, 143–166. [Google Scholar] [CrossRef]
- Breazeal, C. Affective interaction between humans and robots. In Advances in Artificial Life; Goos, G., Hartmanis, J., van Leeuwen, J., Kelemen, J., Sosík, P., Eds.; Springer: Berlin, Heidelberg, 2001; pp. 582–591. ISBN 978-3-540-42567-0. [Google Scholar]
- Rudovic, O.; Lee, J.; Mascarell-Maricic, L.; Schuller, B.W.; Picard, R.W. Measuring engagement in robot-assisted autism therapy: A cross-cultural study. Front. Robot. AI 2017, 4, 36. [Google Scholar] [CrossRef]
- Belpaeme, T.; Baxter, P.E.; Read, R.; Wood, R.; Cuayáhuitl, H.; Kiefer, B.; Racioppa, S.; Kruijff-Korbayová, I.; Athanasopoulos, G.; Enescu, V.; et al. Multimodal child-robot interaction: Building social bonds. J. Hum. -Robot. Interact. 2013, 1, 33–53. [Google Scholar] [CrossRef]
- Kanda, T.; Sato, R.; Saiwaki, N.; Ishiguro, H. A two-month field trial in an elementary school for long-term human–robot interaction. IEEE Trans. Robot. 2007, 23, 962–971. [Google Scholar] [CrossRef]
- Shen, J.; Rudovic, O.; Cheng, S.; Pantic, M. Sentiment apprehension in human-robot interaction with NAO. In Proceedings of the 2015 International Conference on Affective Computing and Intelligent Interaction—ACII’15, Xi’an, China, 21–24 September 2015; IEEE: Piscataway, NJ, USA, 2015; pp. 867–872, ISBN 978-1-4799-9953-8. [Google Scholar]
- Tielman, M.; Neerincx, M.; Meyer, J.-J.; Looije, R. Adaptive emotional expression in robot-child interaction. In Proceedings of the 9th ACM/IEEE International Conference on Human-Robot Interaction—HRI’14, Bielefeld, Germany, 3–6 March 2014; Sagerer, G., Imai, M., Belpaeme, T., Thomaz, A., Eds.; ACM: New York, NY, USA; pp. 407–414.
- Javed, H.; Lee, W.; Park, C.H. Toward an Automated Measure of Social Engagement for Children With Autism Spectrum Disorder-A Personalized Computational Modeling Approach. Front. Robot. AI 2020, 7, 43. [Google Scholar] [CrossRef]
- Rudovic, O.; Lee, J.; Dai, M.; Schuller, B.; Picard, R.W. Personalized machine learning for robot perception of affect and engagement in autism therapy. Sci. Robot. 2018, 3, eaao6760. [Google Scholar] [CrossRef]
- Di Nuovo, A.; Conti, D.; Trubia, G.; Buono, S.; Di Nuovo, S. Deep Learning Systems for Estimating Visual Attention in Robot-Assisted Therapy of Children with Autism and Intellectual Disability. Robotics 2018, 7, 25. [Google Scholar] [CrossRef]
- White, S.W.; Abbott, L.; Wieckowski, A.T.; Capriola-Hall, N.N.; Aly, S.; Youssef, A. Feasibility of automated training for facial emotion expression and recognition in autism. Behav. Ther. 2018, 49, 881–888. [Google Scholar] [CrossRef]
- Yirmiya, N.; Kasari, C.; Sigman, M.; Mundy, P. Facial expressions of affect in autistic, mentally retarded and normal children. J. Child Psychol. Psychiatry 1989, 30, 725–735. [Google Scholar] [CrossRef]
- Spain, D.; Sin, J.; Linder, K.B.; McMahon, J.; Happé, F. Social anxiety in autism spectrum disorder: A systematic review. Res. Autism Spectr. Disord. 2018, 52, 51–68. [Google Scholar] [CrossRef]
- Sharda, M.; Khundrakpam, B.S.; Evans, A.C.; Singh, N.C. Disruption of structural covariance networks for language in autism is modulated by verbal ability. Brain Struct. Funct. 2016, 221, 1017–1032. [Google Scholar] [CrossRef] [PubMed]
- Lemaignan, S.; Garcia, F.; Jacq, A.; Dillenbourg, P. From real-time attention assessment to “with-me-ness” in human-robot interaction. In Proceedings of the 2016 11th ACM/IEEE International Conference on Human-Robot Interaction (HRI), Christchurch, New Zealand, 7–10 March 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 157–164, ISBN 978-1-4673-8370-7. [Google Scholar]
- Kim, E.; Paul, R.; Shic, F.; Scassellati, B. Bridging the research gap: Making HRI useful to individuals with autism. J. Hum.-Robot Interact. 2012, 1, 26–54. [Google Scholar] [CrossRef]
- Lytridis, C.; Bazinas, C.; Papakostas, G.A.; Kaburlasos, V. On measuring engagement level during child-robot interaction in education. In Robotics in Education; Merdan, M., Lepuschitz, W., Koppensteiner, G., Balogh, R., Obdržálek, D., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 3–13. ISBN 978-3-030-26944-9. [Google Scholar]
- Rudovic, O.; Utsumi, Y.; Lee, J.; Hernandez, J.; Ferrer, E.C.; Schuller, B.; Picard, R.W. CultureNet: A deep learning approach for engagement intensity estimation from face images of children with autism. In Proceedings of the 2018 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Madrid, Spain, 1–5 October 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 339–346, ISBN 978-1-5386-8094-0. [Google Scholar]
- Chorianopoulou, A.; Tzinis, E.; Iosif, E.; Papoulidi, A.; Papailiou, C.; Potamianos, A. Engagement detection for children with Autism Spectrum Disorder. In Proceedings of the 2017 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), New Orleans, LA, USA, 5–9 March 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 5055–5059, ISBN 978-1-5090-4117-6. [Google Scholar]
- Zhang, Y.; Tian, Y.; Wu, P.; Chen, D. Application of skeleton data and long short-term memory in action recognition of children with Autism Spectrum Disorder. Sensors 2021, 21, 411. [Google Scholar] [CrossRef]
- Efthymiou, N.; Koutras, P.; Filntisis, P.P.; Potamianos, G.; Maragos, P. Multi-view fusion for action recognition in child-robot interaction. In Proceedings of the 2018 25th IEEE International Conference on Image Processing (ICIP), Athens, Greece, 7–10 October 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 455–459, ISBN 978-1-4799-7061-2. [Google Scholar]
- Efthymiou, N.; Filntisis, P.P.; Potamianos, G.; Maragos, P. Visual robotic perception system with incremental learning for child–robot interaction scenarios. Technologies 2021, 9, 86. [Google Scholar] [CrossRef]
- Anagnostopoulou, D.; Efthymiou, N.; Papailiou, C.; Maragos, P. Engagement estimation during child robot interaction using deep convolutional networks focusing on ASD children. In Proceedings of the 2021 IEEE International Conference on Robotics and Automation (ICRA), Xi’an, China, 30 May–5 January 2021; IEEE: Piscataway, NJ, USA, 2021; pp. 3641–3647, ISBN 978-1-7281-9077-8. [Google Scholar]
- Marinoiu, E.; Zanfir, M.; Olaru, V.; Sminchisescu, C. 3D human sensing, action and emotion recognition in robot assisted therapy of children with autism. In Proceedings of the 2018 IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Salt Lake City, UT, USA, 18–23 January 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 2158–2167, ISBN 978-1-5386-6420-9. [Google Scholar]
- Lhomment, M.; Marsella, S.C. Expressing emotion through posture and gesture. In The Oxford Handbook of Affective Computing; Calvo, R., D’Mello, S., Gratch, J., Kappas, A., Eds.; Oxford University Press: Oxford, NY, USA, 2015; pp. 273–285. ISBN 9780199942237. [Google Scholar]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horstmann, A.C.; Mühl, L.; Köppen, L.; Lindhaus, M.; Storch, D.; Bühren, M.; Röttgers, H.R.; Krajewski, J. Important Preliminary Insights for Designing Successful Communication between a Robotic Learning Assistant and Children with Autism Spectrum Disorder in Germany. Robotics 2022, 11, 141. https://doi.org/10.3390/robotics11060141
Horstmann AC, Mühl L, Köppen L, Lindhaus M, Storch D, Bühren M, Röttgers HR, Krajewski J. Important Preliminary Insights for Designing Successful Communication between a Robotic Learning Assistant and Children with Autism Spectrum Disorder in Germany. Robotics. 2022; 11(6):141. https://doi.org/10.3390/robotics11060141
Chicago/Turabian StyleHorstmann, Aike C., Lisa Mühl, Louisa Köppen, Maike Lindhaus, Dunja Storch, Monika Bühren, Hanns Rüdiger Röttgers, and Jarek Krajewski. 2022. "Important Preliminary Insights for Designing Successful Communication between a Robotic Learning Assistant and Children with Autism Spectrum Disorder in Germany" Robotics 11, no. 6: 141. https://doi.org/10.3390/robotics11060141
APA StyleHorstmann, A. C., Mühl, L., Köppen, L., Lindhaus, M., Storch, D., Bühren, M., Röttgers, H. R., & Krajewski, J. (2022). Important Preliminary Insights for Designing Successful Communication between a Robotic Learning Assistant and Children with Autism Spectrum Disorder in Germany. Robotics, 11(6), 141. https://doi.org/10.3390/robotics11060141