
Supplementation with Bioactive Compounds Improves Health and Rejuvenates Biological Age in Postmenopausal Women

 , ,
, ,
Abstract

1. Introduction
2. Materials and Methods
2.1. Experimental Groups and Experimental Design
2.2. Survey on the Quality of Sleep, Diet, and Physical Activity
2.3. Perceived Scale Stress (PSS)
2.4. Hamilton Anxiety Rating Scale (HAM-A)
2.5. Collection of Human Blood Samples and Isolation of Lymphocytes and Neutrophils
2.6. Immune Functions
2.6.1. Adherence
2.6.2. Chemotaxis of Neutrophils and Lymphocytes
2.6.3. Phagocytic Neutrophil Capacity
2.6.4. Natural Killer (NK) Cell Cytotoxic Activity
2.6.5. Lymphoproliferation
2.7. Oxidative Stress Parameters
2.7.1. Glutathione Reductase Enzyme Activity
2.7.2. Glutathione Peroxidase Enzyme Activity
2.7.3. Glutathione Content Assay
2.7.4. Lipid Peroxidation (TBARS)
2.8. Protein Concentration
2.9. Biological Age
2.10. Hormonal Assays: Cortisol and DHEA
2.11. Safety
2.12. Statistical Analysis
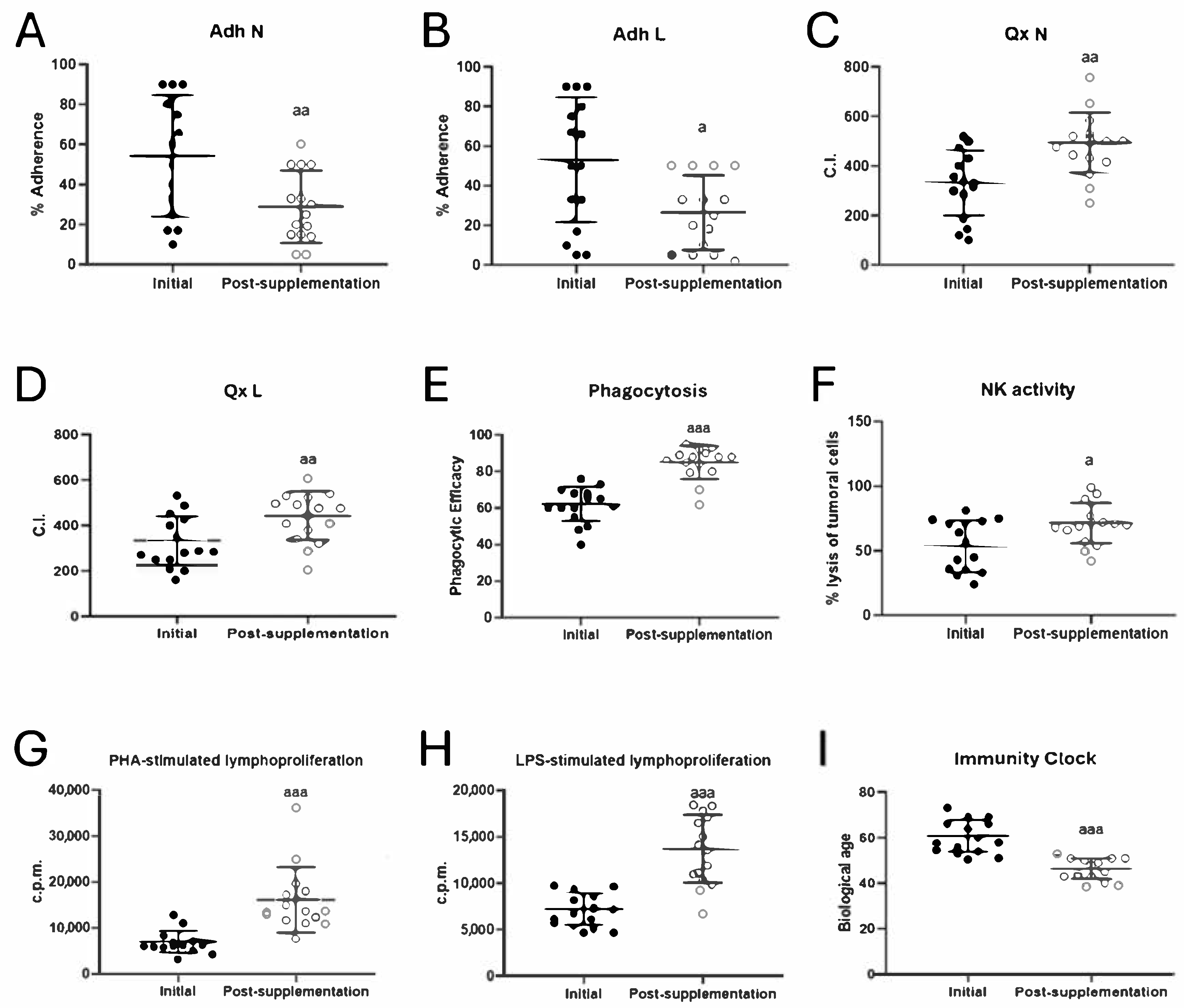
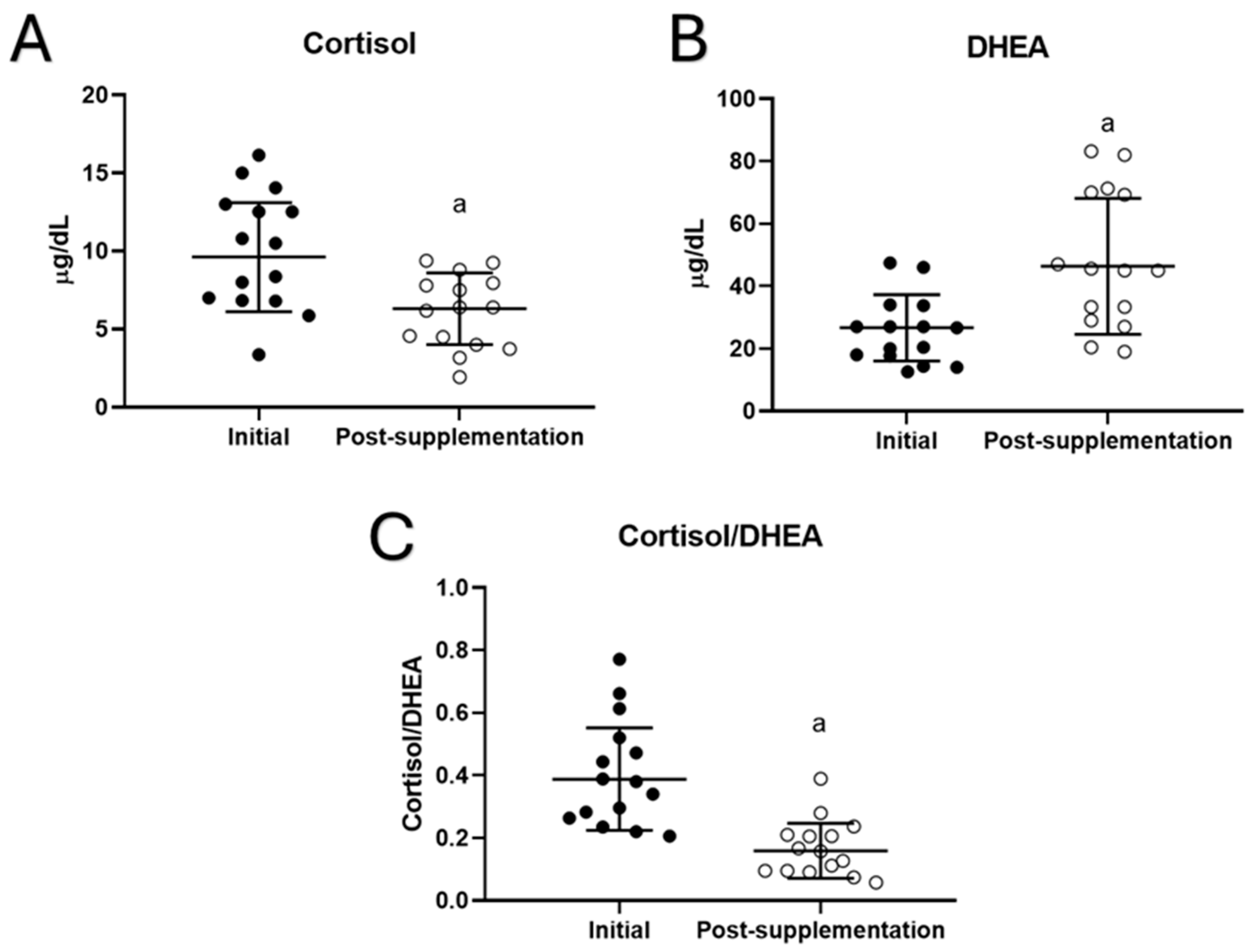
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| c.p.m. | counts per minute |
| CI | chemotaxis index |
| DHEA | dehydroepiandrosterone |
| EDTA | ethylenediaminetetraacetic acid |
| fMLP | N-formyl methionyl-leucyl-phenylalanine |
| GPx | glutathione peroxidase (enzyme) |
| GR | glutathione reductase (enzyme) |
| GSH | reduced glutathione |
| GSSH | oxidized glutathione |
| HPA | hypothalamus-pituitary-adrenal axis |
| LDH | lactate dehydrogenase (enzyme) |
| LP | lymphoproliferation |
| LPS | lipopolysaccharide |
| MLR | multiple linear regression |
| NK | natural killer |
| OPT | O-phthaldialdehyde |
| PHA | phytohemagglutinin |
| PBS | phosphate-buffered saline |
| PE | phagocytic efficacy |
| RPMI | Roswell Park Memorial Institute culture medium |
| SD | standard deviation |
| TBA | thiobarbituric acid |
| TBARS | thiobarbituric acid reactive substances |
| NRV | nutrient reference values |
References
- De la Fuente, M.; Miquel, J. An update of the oxidation-inflammation theory of aging: The involvement of the immune system in oxi-inflamm-aging. Curr. Pharm. Des. 2009, 15, 3003–3026. [Google Scholar] [CrossRef] [PubMed]
- Martínez de Toda, I.; Ceprián, N.; Díaz-Del Cerro, E.; De la Fuente, M. The Role of Immune Cells in Oxi-Inflamm-Aging. Cells 2021, 10, 2974. [Google Scholar] [CrossRef]
- Martínez de Toda, I.; Maté, I.; Vida, C.; Cruces, J.; De la Fuente, M. Immune function parameters as markers of biological age and predictors of longevity. Aging 2016, 8, 3110–3119. [Google Scholar] [CrossRef] [PubMed]
- Martínez de Toda, I.; Vida, C.; Díaz-Del Cerro, E.; De la Fuente, M. The Immunity Clock. J. Gerontol. A Biol. Sci. Med. Sci. 2021, 76, 1939–1945. [Google Scholar] [CrossRef] [PubMed]
- Harman, D. Aging: A theory based on free radical and radiation chemistry. J. Gerontol. 1956, 11, 298–300. [Google Scholar] [CrossRef]
- Martínez de Toda, I.; Vida, C.; Garrido, A.; De la Fuente, M. Redox parameters as markers of the rate of aging and predictors of life span. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 613–620. [Google Scholar] [CrossRef]
- De la Fuente, M.; Cruces, J.; Hernandez, O.; Ortega, E. Strategies to improve the functions and redox state of the immune system in aged subjects. Curr. Pharm. Des. 2011, 17, 3966–3993. [Google Scholar] [CrossRef]
- Foscolou, A.; Magriplis, E.; Tyrovolas, S.; Chrysohoou, C.; Sidossis, L.; Matalas, A.L.; Rallidis, L.; Panagiotakos, D. The association of protein and carbohydrate intake with successful aging: A combined analysis of two epidemiological studies. Eur. J. Nutr. 2019, 58, 807–817. [Google Scholar] [CrossRef]
- Weyh, C.; Krüger, K.; Strasser, B. Physical activity and diet shape the immune system during aging. Nutrients 2020, 12, 622. [Google Scholar] [CrossRef]
- Abiri, B.; Vafa, M. The role of nutrition in attenuating age-related skeletal muscle atrophy. In Reviews on New Drug Targets in Age-Related Disorders; Advances in Experimental Medicine and Biology; Springer: Cham, Switzerland, 2020; Volume 1260, pp. 297–318. [Google Scholar] [CrossRef]
- Missong, H.; Joshi, R.; Khullar, N.; Thareja, S.; Navik, U.; Bhatti, G.K.; Bhatti, J.S. Nutrient-epigenome interactions: Implications for personalized nutrition against aging-associated diseases. J. Nutr. Biochem. 2024, 127, 109592. [Google Scholar] [CrossRef]
- Surugiu, R.; Iancu, M.A.; Vintilescu, Ș.B.; Stepan, M.D.; Burdusel, D.; Genunche-Dumitrescu, A.V.; Dogaru, C.A.; Dumitra, G.G. Molecular mechanisms of healthy aging: The role of caloric restriction, intermittent fasting, mediterranean diet, and ketogenic diet-A scoping review. Nutrients 2024, 16, 2878. [Google Scholar] [CrossRef] [PubMed]
- Lim, G.M.; Maharajan, N.; Cho, G.W. How calorie restriction slows aging: An epigenetic perspective. J. Mol. Med. 2024, 102, 629–640. [Google Scholar] [CrossRef] [PubMed]
- Janson, M. Orthomolecular medicine: The therapeutic use of dietary supplements for anti-aging. Clin. Interv. Aging 2006, 1, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Conti, V.; Izzo, V.; Corbi, G.; Russomanno, G.; Manzo, V.; De Lise, F.; Di Donato, A.; Filippelli, A. Antioxidant supplementation in the treatment of aging-associated diseases. Front. Pharmacol. 2016, 7, 24. [Google Scholar] [CrossRef] [PubMed]
- De la Fuente, M.; Sánchez, C.; Vallejo, C.; Díaz-Del Cerro, E.; Arnalich, F.; Hernanz, Á. Vitamin C and vitamin C plus E improve the immune function in the elderly. Exp. Gerontol. 2020, 142, 111118. [Google Scholar] [CrossRef]
- Pae, M.; Wu, D. Nutritional modulation of age-related changes in the immune system and risk of infection. Nutr. Res. 2017, 41, 14–35. [Google Scholar] [CrossRef]
- Fekete, M.; Szarvas, Z.; Fazekas-Pongor, V.; Feher, A.; Csipo, T.; Forrai, J.; Dosa, N.; Peterfi, A.; Lehoczki, A.; Tarantini, S.; et al. Nutrition Strategies Promoting Healthy Aging: From Improvement of Cardiovascular and Brain Health to Prevention of Age-Associated Diseases. Nutrients 2022, 15, 47. [Google Scholar] [CrossRef]
- Tomasiewicz, A.; Polański, J.; Tański, W. Advancing the understanding of malnutrition in the elderly population: Current insights and future directions. Nutrients 2024, 16, 2502. [Google Scholar] [CrossRef]
- Cruces, J.; Venero, C.; Pereda-Pérez, I.; De la Fuente, M. The effect of psychological stress and social isolation on neuroimmunoendocrine communication. Curr. Pharm. Des. 2014, 20, 4608–4628. [Google Scholar] [CrossRef]
- Vida, C.; González, E.M.; De la Fuente, M. Increase of oxidation and inflammation in nervous and immune systems with aging and anxiety. Curr. Pharm. Des. 2014, 20, 4656–4678. [Google Scholar] [CrossRef]
- Herman, J.P. The neuroendocrinology of stress: Glucocorticoid signaling mechanisms. Psychoneuroendocrinology 2022, 137, 105641. [Google Scholar] [CrossRef] [PubMed]
- Heffner, K.L. Neuroendocrine effects of stress on immunity in the elderly: Implications for inflammatory disease. Immunol. Allergy Clin. N. Am. 2011, 31, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Vitlic, A.; Lord, J.M.; Phillips, A.C. Stress, ageing and their influence on functional, cellular and molecular aspects of the immune system. Age 2014, 36, 9631. [Google Scholar] [CrossRef]
- Fali, T.; Vallet, H.; Sauce, D. Impact of stress on aged immune system compartments: Overview from fundamental to clinical data. Exp. Gerontol. 2018, 105, 19–26. [Google Scholar] [CrossRef]
- Stamou, M.I.; Colling, C.; Dichtel, L.E. Adrenal aging and its effects on the stress response and immunosenescence. Maturitas 2023, 168, 13–19. [Google Scholar] [CrossRef]
- Aschbacher, K.; O’Donovan, A.; Wolkowitz, O.M.; Dhabhar, F.S.; Su, Y.; Epel, E. Good stress, bad stress and oxidative stress: Insights from anticipatory cortisol reactivity. Psychoneuroendocrinology 2013, 38, 1698–1708. [Google Scholar] [CrossRef] [PubMed]
- Polsky, L.R.; Rentscher, K.E.; Carroll, J.E. Stress-induced biological aging: A review and guide for research priorities. Brain Behav. Immun. 2022, 104, 97–109. [Google Scholar] [CrossRef]
- Yegorov, Y.E.; Poznyak, A.V.; Nikiforov, N.G.; Sobenin, I.A.; Orekhov, A.N. The Link between Chronic Stress and Accelerated Aging. Biomedicines 2020, 8, 198. [Google Scholar] [CrossRef]
- McCabe, D.; Lisy, K.; Lockwood, C.; Colbeck, M. The impact of essential fatty acid, B vitamins, vitamin C, magnesium and zinc supplementation on stress levels in women: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2017, 15, 402–453. [Google Scholar] [CrossRef]
- Lopresti, A.L.; Smith, S.J.; Drummond, P.D. Modulation of the hypothalamic-pituitary-adrenal (HPA) axis by plants and phytonutrients: A systematic review of human trials. Nutr. Neurosci. 2022, 25, 1704–1730. [Google Scholar] [CrossRef]
- Xia, X.; Chen, K.; Chen, Y. Change in function and homeostasis of HPA axis: The role of vitamin family. Chem. Biol. Interact. 2024, 391, 110899. [Google Scholar] [CrossRef] [PubMed]
- Fidecicchi, T.; Giannini, A.; Chedraui, P.; Luisi, S.; Battipaglia, C.; Genazzani, A.R.; Genazzani, A.D.; Simoncini, T. Neuroendocrine mechanisms of mood disorders during menopause transition: A narrative review and future perspectives. Maturitas 2024, 188, 108087. [Google Scholar] [CrossRef]
- Kalra, B.; Kalra, S.; Bhattacharya, S.; Dhingra, A. Menopause distress: A person-centered definition. J. Pak. Med. Assoc. 2020, 70, 2481–2483. [Google Scholar]
- Kuck, M.J.; Hogervorst, E. Stress, depression, and anxiety: Psychological complaints across menopausal stages. Front. Psychiatry 2024, 15, 1323743. [Google Scholar] [CrossRef] [PubMed]
- Arranz, L.; Fernández, C.; Rodríguez, A.; Ribera, J.M.; De la Fuente, M. The glutathione precursor N-acetylcysteine improves immune function in postmenopausal women. Free Radic. Biol. Med. 2008, 45, 1252–1262. [Google Scholar] [CrossRef]
- Baeza, I.; De Castro, N.M.; Arranz, L.; Fdez-Tresguerres, J.; De la Fuente, M. Ovariectomy causes immunosenescence and oxi-inflamm-ageing in peritoneal leukocytes of aged female mice similar to that in aged males. Biogerontology 2011, 12, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, C.M.; Romão, F.; Castelo-Branco, C. Menopause and aging: Changes in the immune system—A review. Maturitas 2010, 67, 316–320. [Google Scholar] [CrossRef]
- Ghosh, M.; Rodriguez-Garcia, M.; Wira, C.R. The immune system in menopause: Pros and cons of hormone therapy. J. Steroid Biochem. Mol. Biol. 2014, 142, 171–175. [Google Scholar] [CrossRef]
- Levine, M.E.; Lu, A.T.; Chen, B.H.; Hernandez, D.G.; Singleton, A.B.; Ferrucci, L.; Bandinelli, S.; Salfati, E.; Manson, J.E.; Quach, A.; et al. Menopause accelerates biological aging. Proc. Natl. Acad. Sci. USA 2016, 113, 9327–9332. [Google Scholar] [CrossRef]
- Nappi, R.E.; Cucinella, L. Long-Term Consequences of Menopause. In Female Reproductive Dysfunction; Endocrinology; Petraglia, F., Fauser, B., Eds.; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Martínez de Toda, I.; Miguélez, L.; Siboni, L.; Vida, C.; De la Fuente, M. High perceived stress in women is linked to oxidation, inflammation and immunosenescence. Biogerontology 2019, 20, 823–835. [Google Scholar] [CrossRef]
- Maier, W.; Buller, R.; Philipp, M.; Heuser, I. The Hamilton Anxiety Scale: Reliability, validity and sensitivity to change in anxiety and depressive disorders. J. Affect. Disord. 1988, 14, 61–68. [Google Scholar] [CrossRef] [PubMed]
- De la Fuente, M.; Hernanz, A.; Guayerbas, N.; Victor, V.M.; Arnalich, F. Vitamin E ingestion improves several immune functions in elderly men and women. Free Radic. Res. 2008, 42, 272–280. [Google Scholar] [CrossRef]
- Boyden, S.V. The chemotaxis effect of mixtures of antibody and antigen on polymorphonuclear leukocytes. J. Exp. Med. 1962, 115, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Massey, V.; Williams, C. On the reaction mechanism of yeast glutathione reductase. J. Biol. Chem. 1965, 240, 4470–4481. [Google Scholar] [CrossRef]
- Diaz-Del Cerro, E.; Martinez de Toda, I.; Félix, J.; Baca, A.; De la Fuente, M. Components of the Glutathione Cycle as Markers of Biological Age: An Approach to Clinical Application in Aging. Antioxidants 2023, 12, 1529. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, R.A.; Burk, R.F. Glutathione peroxidase activity in selenium-deficient rat liver. Biochem. Biophys. Res. Commun. 1976, 71, 952–958. [Google Scholar] [CrossRef]
- Hissin, P.J.; Hilf, R. Effects of estrogen to alter amino acid transport in R3230AC mammary carcinomas and its relationship to insulin action. Cancer Res. 1979, 39, 3381–3387. [Google Scholar]
- Díaz-Del Cerro, E.; Lambea, M.; Félix, J.; Salazar, N.; Gueimonde, M.; De la Fuente, M. Daily ingestion of Akkermansia muciniphila for one month promotes healthy aging and increases lifespan in old female mice. Biogerontology 2021, 23, 35–52. [Google Scholar] [CrossRef]
- Noguera, A.; Batle, S.; Miralles, C.; Iglesias, J.; Busquets, X.; MacNee, W.; Agustí, A.G. Enhanced neutrophil response in chronic obstructive pulmonary disease. Thorax 2001, 56, 432–437. [Google Scholar] [CrossRef]
- Maté, I.; Martínez de Toda, I.; Arranz, L.; Álvarez-Sala, J.L.; De la Fuente, M. Accelerated immunosenescence, oxidation and inflammation lead to a higher biological age in COPD patients. Exp. Gerontol. 2021, 154, 111551. [Google Scholar] [CrossRef]
- Bulut, O.; Kilic, G.; Domínguez-Andrés, J.; Netea, M.G. Overcoming immune dysfunction in the elderly: Trained immunity as a novel approach. Int. Immunol. 2020, 32, 741–753. [Google Scholar] [CrossRef] [PubMed]
- Porter, V.R.; Greendale, G.A.; Schocken, M.; Zhu, X.; Effros, R.B. Immune effects of hormone replacement therapy in post-menopausal women. Exp. Gerontol. 2001, 36, 311–326. [Google Scholar] [CrossRef] [PubMed]
- Baeza, I.; Alvarado, C.; Alvarez, P.; Salazar, V.; Castillo, C.; Ariznavarreta, C.; Fdez-Tresguerres, J.A.; De la Fuente, M. Improvement of leucocyte functions in ovariectomised aged rats after treatment with growth hormone, melatonin, oestrogens or phyto-oestrogens. J. Reprod. Immunol. 2009, 80, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Baeza, I.; De Castro, N.M.; Giménez-Llort, L.; De la Fuente, M. Ovariectomy, a model of menopause in rodents, causes a premature aging of the nervous and immune systems. J. Neuroimmunol. 2010, 219, 90–99. [Google Scholar] [CrossRef]
- Razak, M.A.; Begum, P.S.; Viswanath, B.; Rajagopal, S. Multifarious beneficial effect of nonessential amino acid, glycine: A review. Oxid. Med. Cell. Longev. 2017, 2017, 1716701, Erratum in Oxid. Med. Cell. Longev. 2022, 2022, 9857645. https://doi.org/10.1155/2022/9857645. [Google Scholar] [CrossRef]
- Aguayo-Cerón, K.A.; Sánchez-Muñoz, F.; Gutierrez-Rojas, R.A.; Acevedo-Villavicencio, L.N.; Flores-Zarate, A.V.; Huang, F.; Giacoman-Martinez, A.; Villafaña, S.; Romero-Nava, R. Glycine: The smallest anti-inflammatory micronutrient. Int. J. Mol. Sci. 2023, 24, 11236. [Google Scholar] [CrossRef]
- Soh, J.; Raventhiran, S.; Lee, J.H.; Lim, Z.X.; Goh, J.; Kennedy, B.K.; Maier, A.B. The effect of glycine administration on the characteristics of physiological systems in human adults: A systematic review. Geroscience 2024, 46, 219–239. [Google Scholar] [CrossRef]
- Li, P.; Wu, G. Important roles of amino acids in immune responses. Br. J. Nutr. 2022, 127, 398–402. [Google Scholar] [CrossRef]
- Egbujor, M.C.; Olaniyan, O.T.; Emeruwa, C.N.; Saha, S.; Saso, L.; Tucci, P. An insight into role of amino acids as antioxidants via NRF2 activation. Amino Acids 2024, 56, 23. [Google Scholar] [CrossRef]
- Tang, X.; Liu, H.; Xiao, Y.; Wu, L.; Shu, P. Vitamin C Intake and Ischemic Stroke. Front. Nutr. 2022, 9, 935991. [Google Scholar] [CrossRef]
- Babygirija, R.; Lamming, D.W. The regulation of healthspan and lifespan by dietary amino acids. Transl. Med. Aging 2021, 5, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Varela-López, A.; Romero-Márquez, J.M.; Navarro-Hortal, M.D.; Ramirez-Tortosa, C.L.; Battino, M.; Forbes-Hernández, T.Y.; Quiles, J.L. Dietary antioxidants and lifespan: Relevance of environmental conditions, diet, and genotype of experimental models. Exp. Gerontol. 2023, 178, 112221. [Google Scholar] [CrossRef]
- Karagianni, C.; Bazopoulou, D. Redox regulation in lifespan determination. J. Biol. Chem. 2024, 300, 105761. [Google Scholar] [CrossRef] [PubMed]
- Shirazi, T.N.; Hastings, W.J.; Rosinger, A.Y.; Ryan, C.P. Parity predicts biological age acceleration in post-menopausal, but not pre-menopausal, women. Sci. Rep. 2020, 10, 20522. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Li, C. Hormone Therapy and Biological Aging in Postmenopausal Women. JAMA Netw. Open 2024, 7, e2430839. [Google Scholar] [CrossRef]
- Bauer, M.E.; Jeckel, C.M.; Luz, C. The role of stress factors during aging of the immune system. Ann. N. Y. Acad. Sci. 2009, 1153, 139–152. [Google Scholar] [CrossRef]
- Erceg, N.; Micic, M.; Forouzan, E.; Knezevic, N.N. The Role of Cortisol and Dehydroepiandrosterone in Obesity, Pain, and Aging. Diseases 2025, 13, 42. [Google Scholar] [CrossRef]
- Labrie, F.; Bélanger, A.; Pelletier, G.; Martel, C.; Archer, D.F.; Utian, W.H. Science of intracrinology in postmenopausal women. Menopause 2017, 24, 702–712. [Google Scholar] [CrossRef]
- Woods, N.F.; Mitchell, E.S.; Smith-Dijulio, K. Cortisol levels during the menopausal transition and early postmenopause: Observations from the Seattle Midlife Women’s Health Study. Menopause 2009, 16, 708–718. [Google Scholar] [CrossRef]
- Chakraborty, S.; Tripathi, S.J.; Raju, T.R.; Shankaranarayana Rao, B.S. Mechanisms underlying remediation of depression-associated anxiety by chronic N-acetyl cysteine treatment. Psychopharmacology 2020, 237, 2967–2981. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Pre (N = 15) | Post (N = 15) |
|---|---|---|
| Female, sex, n (%) | 15 (100) | |
| Age, mean (SD), years | 59.3 (6.5) | |
| Age group, n (%) 40–50 years 51–60 years 61–70 years 71–80 years | 1 (6.7) 10 (66.7) 3 (20) 1 (6.7) | |
| Employment status, n (%) Full-time work Part-time work Unemployed Retired Not working for other reasons | 13 (86.7) 0 (0) 0 (0) 2 (13.3) 0 (0) | |
| Smoking regularly 1, n (number of cigarretes/day) Alcohol intake, regularly 2, n (%) | 1 (15) 0 (0) | |
| Sleep quality Poor (1–4), n (%) Acceptable (5–7), n (%) Optimal (8–10), n (%) | 1 (6.7) 13 (86.7) 1 (6.7) | 0 (0) 13 (86.7) 2 (13.3) |
| Balanced diet Poor (1–4), n (%) Acceptable (5–7), n (%) Optimal (8–10), n (%) | 1 (6.7) 12 (80) 2 (13.3) | 1 (6.7) 12 (80) 2 (13.3) |
| Physical activity Poor (1–4), n (%) Acceptable (5–7), n (%) Optimal (8–10), n (%) | 2 (13.3) 12 (80) 1 (6.7) | 1 (6.7) 13 (86.7) 1 (6.7) |
| Perceived stress, mean score obtained in the survey (SD) Score group, n (%) Low stress (0–13) Moderate stress (14–26) High stress (27–40) | 19.25 (4) 11 (73.3) 4 (26.7) 0 (0) | 18.75 (4.5) 11 (73.3) 4 (26.7) 0 (0) |
| Hamilton Anxiety Scale, Mean Score (SD) Score group, n (%) Mild anxiety or no anxiety (0–17) Moderate anxiety (18–24) Severe anxiety (25–30) Very severe anxiety (31–56) | 13.43 (9.3) 13 (86.7) 2 (13.3) 0 (0) 0 (0) | 10.92 (8.7) 13 (86.7) 2 (13.3) 0 (0) 0 (0) |
| Characteristic | Overall (N = 15) |
|---|---|
| Family history, n (%) None Aneurysm Cancer (larynx, lung, lymphoma) Myocardial infarction | 7 (46.7) 2 (13.3) 4 (26.6) 2 (13.3) |
| Previous illnesses (more than 5 years ago), n (%) None Ovarian Cancer Endometriosis Arrhythmia | 12 (80) 1 (6.7) 1 (6.7) 1 (6.7) |
| Operation (more than 5 years ago), n (%) None Total Hysterectomy Cholecystectomy Appendicitis Herniated discs Cesarean section Osteochondroma | 8 (53.3) 2 (13.3) 1 (6.7) 1 (6.7) 1 (6.7) 1 (6.7) 1 (6.7) |
| Blood pressure, n (%) Low Normal High | 3 (20) 12 (80) 0 (0) |
| Daily medication, n (%) Nothing Hormone Replacement Therapy Probiotics supplement Antiarrhythmic medication | 10 (66.7) 2 (13.3) 1 (6.7) 1 (6.7) |
| Frequent fainting/seizure, n (%) Genitourinary tract diseases, n (%) Skin diseases, n (%) Respiratory diseases, n (%) | 0 (0) 0 (0) 0 (0) 0 (0) |
| Gastrointestinal diseases and discomfort, n (%) None Celiac disease/gluten intolerance Gastroesophageal Reflux | 12 (80) 2 (13.3) 1 (6.7) |
| Allergy (food, drugs), n (%) | 3 (20) |
| Autoimmune/endocrine diseases, n (%) None Hypothyroidism | 13 (86.7) 2 (13.3) |
| Oral health Good (daily care/no missing parts), n (%) Bad n, (missing parts) (%) | 14 (93.3) 1 (3 pieces) (6.7) |
| Ingredients | Weight (g) |
|---|---|
| UNAMINA A (g) | |
| Glycine | 5.00 g |
| L-lysine | 0.99 g |
| L-arginine | 0.50 g |
| L-proline | 0.50 g |
| L-leucine | 0.25 g |
| L-isoleucine | 0.25 g |
| L-valine | 0.25 g |
| L-tryptophan | 0.05 g |
| Hydrolyzed collagen | 0.50 g |
| Magnesium citrate | 0.35 g (15% NRV) |
| Calcium carbonate | 0.30 g (15% NRV) |
| Methyl-sulfonyl-methane | 0.50 g |
| UNAMINA B [Weight per dose 1 capsule (mg) amount supplied NRV] | |
| Magnesium oxide | 93.28 mg |
| L-ornithine HCl | 50 50 - |
| L-beta-alanine | 50 50 - |
| N-acetyl L-cysteine | 50 50 - |
| L-threonine | 50 50 - |
| L-histidine | 50 50 - |
| L-glutamine | 50 50 - |
| L-taurine | 50 50 - |
| Ferrous fumarate | 42.59 14 100% |
| Chondroitin sulphate | 40 40 - |
| Glucosamine sulphate | 40 40 - |
| Zinc sulphate hydrate | 27.45 10 100% |
| Niacin (B3) | 16 16 100% |
| Magnesium stearate | 10.123 - - |
| Pantothenic acid (B5) | 6.5221 6 100% |
| Manganese sulphate | 6.152 2 100% |
| Sodium hyaluronate | 5 5 - |
| Pyridoxine (B6) | 1.694 1.4 100% |
| Riboflavin (B2) | 1.4 1.4 100% |
| Thiamine (B1) | 1.39854 1.1 100% |
| Folate (B9) | 0.2 200 µg 100% |
| Sodium selenite | 0.1319 55 µg 100% |
| Biotin (B8) | 0.05 50 µg 100% |
| Cobalamin (B12) | 0.0025 2.5 µg 100% |
| UNAMINA C [amount (g) provided per daily dose (2 sachets)] | |
| Citric acid | 1.5 g |
| Malic acid | 1.5 g |
| Ascorbic acid | 1.0 g |
| 1000 mg vitamin C (1250% NRV) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díaz-Del Cerro, E.; Félix, J.; Martínez-Poyato, M.C.; De la Fuente, M. Supplementation with Bioactive Compounds Improves Health and Rejuvenates Biological Age in Postmenopausal Women. Biomolecules 2025, 15, 739. https://doi.org/10.3390/biom15050739
Díaz-Del Cerro E, Félix J, Martínez-Poyato MC, De la Fuente M. Supplementation with Bioactive Compounds Improves Health and Rejuvenates Biological Age in Postmenopausal Women. Biomolecules. 2025; 15(5):739. https://doi.org/10.3390/biom15050739
Chicago/Turabian StyleDíaz-Del Cerro, Estefanía, Judith Félix, Mª Carmen Martínez-Poyato, and Mónica De la Fuente. 2025. "Supplementation with Bioactive Compounds Improves Health and Rejuvenates Biological Age in Postmenopausal Women" Biomolecules 15, no. 5: 739. https://doi.org/10.3390/biom15050739
APA StyleDíaz-Del Cerro, E., Félix, J., Martínez-Poyato, M. C., & De la Fuente, M. (2025). Supplementation with Bioactive Compounds Improves Health and Rejuvenates Biological Age in Postmenopausal Women. Biomolecules, 15(5), 739. https://doi.org/10.3390/biom15050739