
Effect of 5-Alpha Reductase Inhibitors on Magnetic Resonance Imaging and Prostate Cancer Detection

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design, Setting, and Participants
2.2. MpMRI and Prostate Biopsy Characteristics
2.3. Outcome Variables of This Study
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Study Population and Comparison According to 5-ARI Exposure
3.2. Search for Independent Predictive Variables of csPCa and iPCa
3.3. Characteristics of the Randomized Matched Group According to 5-ARI Exposure
3.4. Distribution of csPCa and iPCa in 5-ARI Users and 5-ARI-Naïve Men According to PI-RADS Category
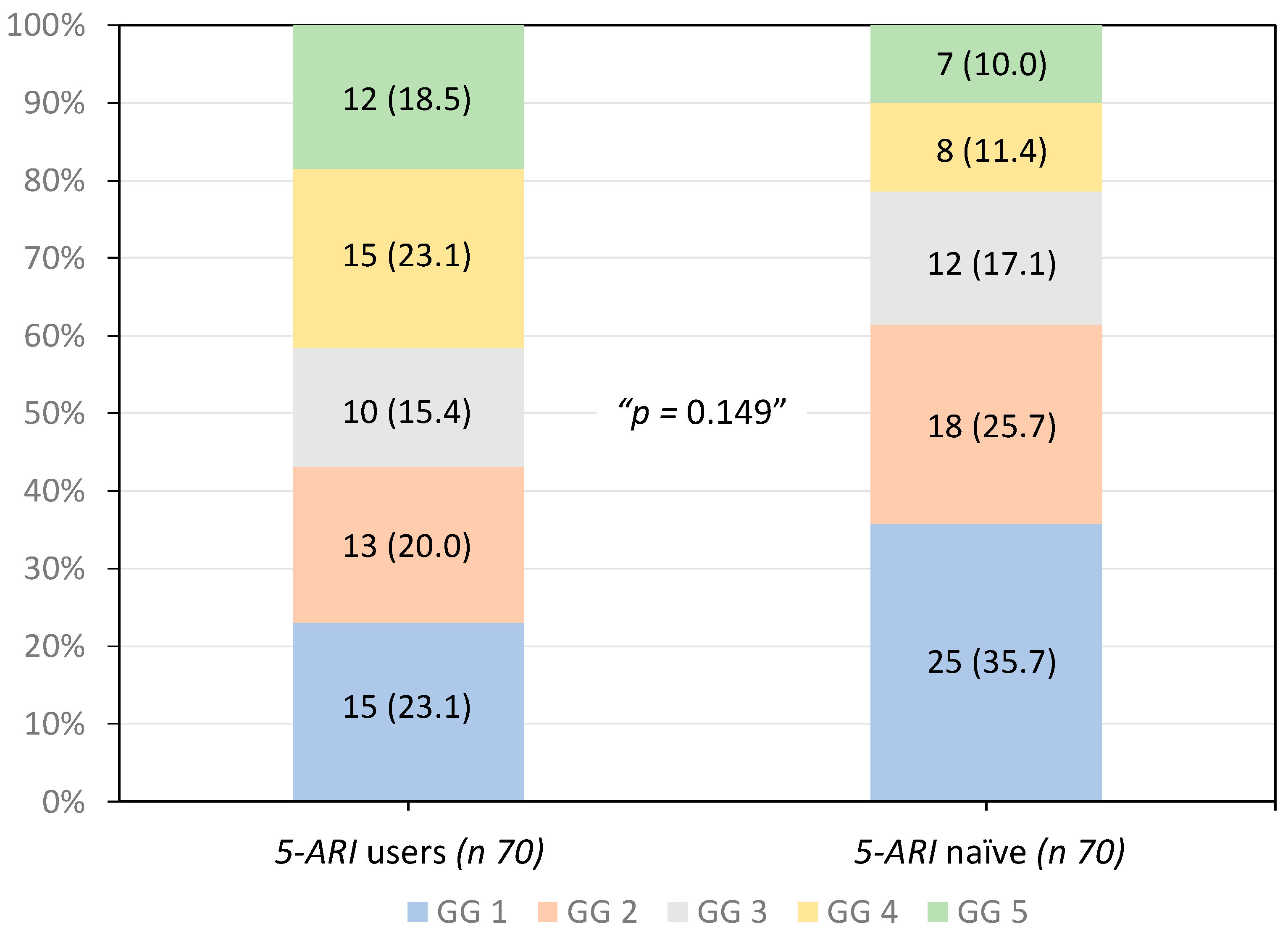
3.5. Distribution of Grade Groups in Tumors Detected in 5-ARI Users and 5-ARI-Naïve Men
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Poppel, H.; Albreht, T.; Basu, P.; Hogenhout, R.; Collen, S.; Roobol, M. Serum PSA-based early detection of prostate cancer in Europe and globally: Past, present and future. Nat. Rev. Urol. 2022, 19, 562–572. [Google Scholar] [CrossRef] [PubMed]
- Schroder, F.H.; Hugosson, J.; Roobol, M.J.; Tammela, T.L.; Ciatto, S.; Nelen, V.; Kwiatkowski, M.; Lujan, M.; Lilja, H.; Zappa, M.; et al. Screening and prostate-cancer mortality in a randomized European study. N. Engl. J. Med. 2009, 360, 1320–1328. [Google Scholar] [CrossRef]
- Frånlund, M.; Månsson, M.; Godtman, R.A.; Aus, G.; Holmberg, E.; Kollberg, K.S.; Lodding, P.; Pihl, C.G.; Stranne, J.; Lilja, H.; et al. Results from 22 years of Followup in the Göteborg Randomized Population-Based Prostate Cancer Screening Trial. J. Urol. 2022, 208, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Schoots, I.G.; Padhani, A.R.; Rouvière, O.; Barentsz, J.O.; Richenberg, J. Analysis of Magnetic Resonance Imaging-directed Biopsy Strategies for Changing the Paradigm of Prostate Cancer Diagnosis. Eur. Urol. Oncol. 2020, 3, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Rouvière, O.; Puech, P.; Renard-Penna, R.; Claudon, M.; Roy, C.; Mège-Lechevallier, F.; Decaussin-Petrucci, M.; Dubreuil-Chambardel, M.; Magaud, L.; Remontet, L.; et al. Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naive patients (MRI-FIRST): A prospective, multicentre, paired diagnostic study. Lancet Oncol. 2018, 20, 100–109. [Google Scholar] [CrossRef]
- Hagens, M.J.; Noordzij, M.A.; Mazel, J.W.; Jager, A.; Boellaard, T.N.; Tielbeek, J.A.W.; Henebiens, M.; Schoots, I.G.; van Leeuwen, P.J.; van der Poel, H.G.; et al. An Magnetic Resonance Imaging-directed Targeted-plus-perilesional Biopsy Approach for Prostate Cancer Diagnosis: “Less Is More”. Eur. Urol. Open Sci. 2022, 43, 68–73. [Google Scholar] [CrossRef]
- Jacobsen, S.J.; Girman, C.J.; Lieber, M.M. Natural history of benign prostatic hyperplasia. Urology 2001, 58, 5–16. [Google Scholar] [CrossRef]
- Van Poppel, H.; Hogenhout, R.; Albers, P.; van den Bergh, R.C.N.; Barentsz, J.O.; Roobol, M.J. A European Model for an Orga-nised Risk-stratified Early Detection Programme for Prostate Cancer. Eur. Urol. Oncol. 2021, 4, 731–739. [Google Scholar] [CrossRef]
- Edwards, J.E.; Moore, R.A. Finasteride in the treatment of clinical benign prostatic hyperplasia: A systematic review of rando-mised trials. BMC Urol. 2002, 2, 14. [Google Scholar] [CrossRef] [PubMed]
- Thompson, I.M.; Goodman, P.J.; Tangen, C.M.; Lucia, M.S.; Miller, G.J.; Ford, L.G.; Lieber, M.M.; Cespedes, R.D.; Atkins, J.N.; Lippman, S.M.; et al. The influence of finasteride on the development of prostate cancer. N. Engl. J. Med. 2003, 349, 215–224. [Google Scholar] [CrossRef]
- Andriole, G.L.; Bostwick, D.G.; Brawley, O.W.; Gomella, L.G.; Marberger, M.; Montorsi, F.; Pettaway, C.A.; Tammela, T.L.; Teloken, C.; Tindall, D.J.; et al. Effect of dutasteride on the risk of prostate cancer. N. Engl. J. Med. 2010, 362, 1192–1202. [Google Scholar] [CrossRef] [PubMed]
- Thompson, I.M.; Goodman, P.J.; Tangen, C.M.; Parnes, H.L.; Minasian, L.M.; Godley, P.A.; Lucia, M.S.; Ford, L.G. Long-term survival of participants in the prostate cancer prevention trial. N. Engl. J. Med. 2013, 369, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Redman, M.W.; Tangen, C.M.; Goodman, P.J.; Lucia, M.S.; Coltman, C.A., Jr.; Thompson, I.M. Finasteride does not increase the risk of high-grade prostate cancer: A bias-adjusted modeling approach. Cancer Prev. Res. 2008, 1, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, H.; Klaassen, Z.; Chandrasekar, T.; Fleshner, N. Preventing clinical progression and need for treatment in patients on active surveillance for prostate cancer. Curr. Opin. Urol. 2018, 28, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Robertson, N.L.; Moore, C.M.; Ambler, G.; Bott, S.R.; Freeman, A.; Gambarota, G.; Jameson, C.; Mitra, A.V.; Whitcher, B.; Winkler, M.; et al. MAPPED study design: A 6 month randomised controlled study to evaluate the effect of dutasteride on prostate cancer volume using magnetic resonance imaging. Contemp. Clin. Trials 2013, 34, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.M.; Robertson, N.L.; Jichi, F.; Damola, A.; Ambler, G.; Giganti, F.; Ridout, A.J.; Bott, S.R.; Winkler, M.; Ahmed, H.U.; et al. The Effect of Dutasteride on Magnetic Resonance Imaging Defined Prostate Cancer: MAPPED-A Randomized, Placebo Controlled, Double-Blind Clinical Trial. J. Urol. 2017, 197, 1006–1013. [Google Scholar] [CrossRef] [PubMed]
- Giganti, F.; Moore, C.M.; Robertson, N.L.; McCartan, N.; Jameson, C.; Bott, S.R.J.; Winkler, M.; Gambarota, G.; Whitcher, B.; Castro, R.; et al. MRI findings in men on active surveillance for prostate cancer: Does dutasteride make MRI visible lesions less conspicuous? Results from a placebo-controlled, randomised clinical trial. Eur. Radiol. 2017, 27, 4767–4774. [Google Scholar] [CrossRef]
- Ginsburg, S.B.; Algohary, A.; Pahwa, S.; Gulani, V.; Ponsky, L.; Aronen, H.J.; Boström, P.J.; Böhm, M.; Haynes, A.M.; Brenner, P.; et al. Radiomic features for prostate cancer detection on MRI differ between the transition and peripheral zones: Preliminary findings from a multi-institutional study. J. Magn. Reason. Imaging 2017, 46, 184–193. [Google Scholar] [CrossRef]
- Starobinets, O.; Kurhanewicz, J.; Noworolski, S.M. Improved multiparametric MRI discrimination between low-risk prostate cancer and benign tissues in a small cohort of 5α-reductase inhibitor treated individuals as compared with an untreated cohort. NMR Biomed. 2017, 30, e3696. [Google Scholar] [CrossRef]
- Kim, J.K.; Lee, H.J.; Hwang, S.I.; Choe, G.; Kim, H.J.; Hong, S.K. The effect of 5 alpha-reductase inhibitor therapy on prostate cancer detection in the era of multi-parametric magnetic resonance imaging. Sci. Rep. 2019, 9, 17862. [Google Scholar] [CrossRef] [PubMed]
- Forte, V.; Cavallo, A.U.; Bertolo, R.; de Soccio, V.; Sperandio, M.; Bove, P.; Ciccariello, M. PI-RADS score v.2 in predicting malignancy in patients undergoing 5α-reductase inhibitor therapy. Prostate Cancer Prostatic. Dis. 2021, 24, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, K.; Ong, H.Y.; Tsang, W.C.; Wu, Q.H.; Chiong, E. 5-alpha reductase inhibitors and MRI prostates: Actively reducing prostate sizes and ambiguity. BMC Urol. 2023, 23, 61. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; Confort, P.; van den Bergh, R.C.N.; Briers, E.; Eberli, D.; De Meerleer, G.; De Santis, M.; Gillessen, S.; Grummet, J.; Henry, A.M.; et al. EAU–EANM–ESTRO–ESUR–ISUP–SIOG Guidelines on Prostate Cancer. 2023. Available online: http://uroweb.org/guidelines/compilations-of-all-guidelines/ (accessed on 1 November 2023).
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A.; Grading, C. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Marberger, M.; Freedland, S.J.; Andriole, G.L.; Emberton, M.; Pettaway, C.; Montorsi, F.; Teloken, C.; Rittmaster, R.S.; Somerville, M.C.; Castro, R. Usefulness of prostate-specific antigen (PSA) rise as a marker of prostate cancer in men treated with dutasteride: Lessons from the REDUCE study. BJU Int. 2012, 109, 1162–1169. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.W.; Wang, S.S.; Yang, C.K.; Lu, K.; Chen, C.S.; Cheng, C.L.; Hung, S.C.; Chiu, K.Y.; Hsu, C.Y.; Li, J.R. Risk Analysis of Prostate Cancer Development Following Five-alpha Reductase Inhibitor Treatment for Benign Prostate Hyperplasia. Anticancer Res. 2023, 43, 485–491. [Google Scholar] [CrossRef]
- Falagario, U.G.; Lantz, A.; Jambor, I.; Busetto, G.M.; Bettocchi, C.; Finati, M.; Ricapito, A.; Luzzago, S.; Ferro, M.; Musi, G.; et al. Diagnosis of prostate cancer with magnetic resonance imaging in men treated with 5-alpha-reductase inhibitors. World J. Urol. 2023, 41, 2967–2974. [Google Scholar] [CrossRef]
- Artiles Medina, A.; Rodríguez-Patrón Rodríguez, R.; Ruiz Hernández, M.; Mata Alcaraz, M.; García Barreras, S.; Fernández Conejo, G.; Fraile Poblador, A.; Sanz Mayayo, E.; Burgos Revilla, F.J. Identifying Risk Factors for MRI-Invisible Prostate Cancer in Patients Undergoing Transperineal Saturation Biopsy. Res. Rep. Urol. 2021, 13, 723–731. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic | 5-ARI Users | 5-ARI Naïve | p Value |
|---|---|---|---|
| Number of men, (%) | 120 (5.4) | 2092 (94.6) | - |
| Median age (IQR), years | 72 (68–76) | 68 (62–73) | <0.001 |
| Median PSA (IQR), ng/mL | 8.0 (5.0–13.0) | 7.3 (5.3–11.0) | 0.107 |
| Suspicious DRE, n (%) | 42 (35.0) | 561 (26.8) | 0.057 |
| Repeated biopsy, n (%) | 44 (36.7) | 657 (31.4) | 0.228 |
| PCa family history, (%) | 5 (4.2) | 169 (8.1) | 0.160 |
| Median prostate volume, cc (IQR), cc | 69 (49–97) | 53 (38–74) | <0.001 |
| PSA density, ng/mL/cc | 0.12 (0.08–0.21) | 0.14 (0.09–0.22) | 0.025 |
| PI-RADS score, n (%) | |||
| ≤2 | 15 (12.5) | 320 (14.5) | 0.328 |
| 3 | 20 (16.7) | 429 (20.5) | |
| 4 | 57 (47.5) | 903 (43.2) | |
| 5 | 28 (23.6) | 440 (21.0) | |
| PCa, n (%) | 66 (55.0) | 1336 (63.9) | 0.052 |
| csPCa, n (%) | 51 (42.5) | 935 (44.7) | 0.706 |
| iPCa, n (%) | 15 (12.5) | 401 (19.2) | 0.072 |
| Predictive Variable | csPCa | iPCa | ||
|---|---|---|---|---|
| Odd Ratio (95% CI) | p Value | Odd Ratio (95% CI) | p Value | |
| 5-ARI exposure, Ref. no | 0.826 (0.521–1.311) | 0.418 | 0.628 (0.357–1.104) | 0.106 |
| Age, Ref. year | 1.059 (1.044–1.072) | <0.001 | 1.010 (0.995–1.024) | 0.186 |
| Serum PSA, Ref. ng/mL | 1.014 (1.006–1.021) | <0.001 | 0.986 (0.976–0.997) | 0.012 |
| DRE. Ref. normal | 2.254 (1.781–2.853) | <0.001 | 0.626 (0.475–0.825) | <0.001 |
| Type of biopsy, Ref. initial | 0.792 (0.633–0.990) | 0.040 | 1.780 (1.420–2.230) | <0.001 |
| PCa family history, Ref. no | 1.230 (0.853–1.772) | 0.267 | 1.166 (0.793–1.713) | 0.435 |
| Prostate volume, Ref. cc | 0.980 (0.976–0.983) | 0.001 | 0.997 (0.993–1.001) | 0.092 |
| PI-RADS score, Ref. ≤ 2 | 2.350 (2.277–2.855) | 0.001 | 0.907 (0.832–0.989) | 0.027 |
| Characteristic | 5-ARI Users | 5-ARI Naïve | p Value |
|---|---|---|---|
| Number of men, (%) | 118 (50.0) | 118 (50.0) | - |
| Median age (IQR), years | 72 (68–76) | 71 (68–76) | 0.799 |
| Median PSA (IQR), ng/mL | 8.0 (5.2–12.9) | 7.5 (5.6–10.6) | 0.304 |
| Suspicious DRE, n (%) | 42 (35.6) | 43 (36.4) | 0.892 |
| Repeated biopsy, n (%) | 43 (36.4) | 43 (36.4) | 1.000 |
| PCa family history, (%) | 5 (4.2) | 5 (4.2) | 1.000 |
| Median prostate volume (IQR), cc | 67 (49–95) | 66 (49–96) | 0.852 |
| PI-RADS score, n (%) | |||
| ≤2 | 15 (45.5) | 18 (54.5) | 0.685 |
| 3 | 20 (58.8) | 14 (41.2) | |
| 4 | 56 (50.0) | 56 (50.0) | |
| 5 | 27 (47.4) | 30 (52.6) | |
| PCa, n (%) | 65 (48.1) | 70 (51.9) | 0.599 |
| csPCa, n (%) | 50 (52.6) | 45 (47.4) | 0.596 |
| iPCa, n (%) | 15 (37.5) | 25 (62.5) | 0.089 |
| PI-RADS Score | n | csPCa | iPCa | ||||
|---|---|---|---|---|---|---|---|
| 5-ARI Users | 5-ARI Naïve | p Value | 5-ARI Users | 5-ARI Naïve | p Value | ||
| ≤3, n (%) | 33 | 0/15 (0) | 3/18 (16.7) | 0.233 | 1/15 (6.7) | 1/18 (5.6) | 0.894 |
| 3, n (%) | 34 | 2/20 (10.0) | 3/14 (21.4) | 0.627 | 3/20 (15.0) | 1/14 (7.1) | 0.627 |
| 4, n (%) | 112 | 26/56 (46.4) | 16/56 (28.6) | 0.078 | 10/56 (17.9) | 18/56 (32.1) | 0.126 |
| 5, n (%) | 57 | 22/27 (81.5) | 23/30 (76.7) | 0.751 | 1/27 (3.7) | 5/30 (16.7) | 0.080 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morote, J.; Picola, N.; Muñoz-Rodriguez, J.; Paesano, N.; Ruiz-Plazas, X.; Muñoz-Rivero, M.V.; Celma, A.; Manuel, G.G.-d.; Miró, B.; Servian, P.; et al. Effect of 5-Alpha Reductase Inhibitors on Magnetic Resonance Imaging and Prostate Cancer Detection. Biomolecules 2024, 14, 193. https://doi.org/10.3390/biom14020193
Morote J, Picola N, Muñoz-Rodriguez J, Paesano N, Ruiz-Plazas X, Muñoz-Rivero MV, Celma A, Manuel GG-d, Miró B, Servian P, et al. Effect of 5-Alpha Reductase Inhibitors on Magnetic Resonance Imaging and Prostate Cancer Detection. Biomolecules. 2024; 14(2):193. https://doi.org/10.3390/biom14020193
Chicago/Turabian StyleMorote, Juan, Natàlia Picola, Jesús Muñoz-Rodriguez, Nahuel Paesano, Xavier Ruiz-Plazas, Marta V. Muñoz-Rivero, Ana Celma, Gemma García-de Manuel, Berta Miró, Pol Servian, and et al. 2024. "Effect of 5-Alpha Reductase Inhibitors on Magnetic Resonance Imaging and Prostate Cancer Detection" Biomolecules 14, no. 2: 193. https://doi.org/10.3390/biom14020193
APA StyleMorote, J., Picola, N., Muñoz-Rodriguez, J., Paesano, N., Ruiz-Plazas, X., Muñoz-Rivero, M. V., Celma, A., Manuel, G. G.-d., Miró, B., Servian, P., & Abascal, J. M. (2024). Effect of 5-Alpha Reductase Inhibitors on Magnetic Resonance Imaging and Prostate Cancer Detection. Biomolecules, 14(2), 193. https://doi.org/10.3390/biom14020193