Common Variants in IL-20 Gene are Associated with Subclinical Atherosclerosis, Cardiovascular Risk Factors and IL-20 Levels in the Cohort of the Genetics of Atherosclerotic Disease (GEA) Mexican Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Definition of Subclinical Atherosclerosis
2.3. Quantification of IL-20 Concentration
2.4. Genetic Analysis
2.5. Statistical Analysis
3. Results
3.1. Study Samples Characteristics
3.2. Association of Polymorphisms with SA
3.3. Association of the IL-20 Polymorphisms with Cardiovascular Risk Factors
3.4. Association of the rs1400986 Genotypes with IL-20 Levels
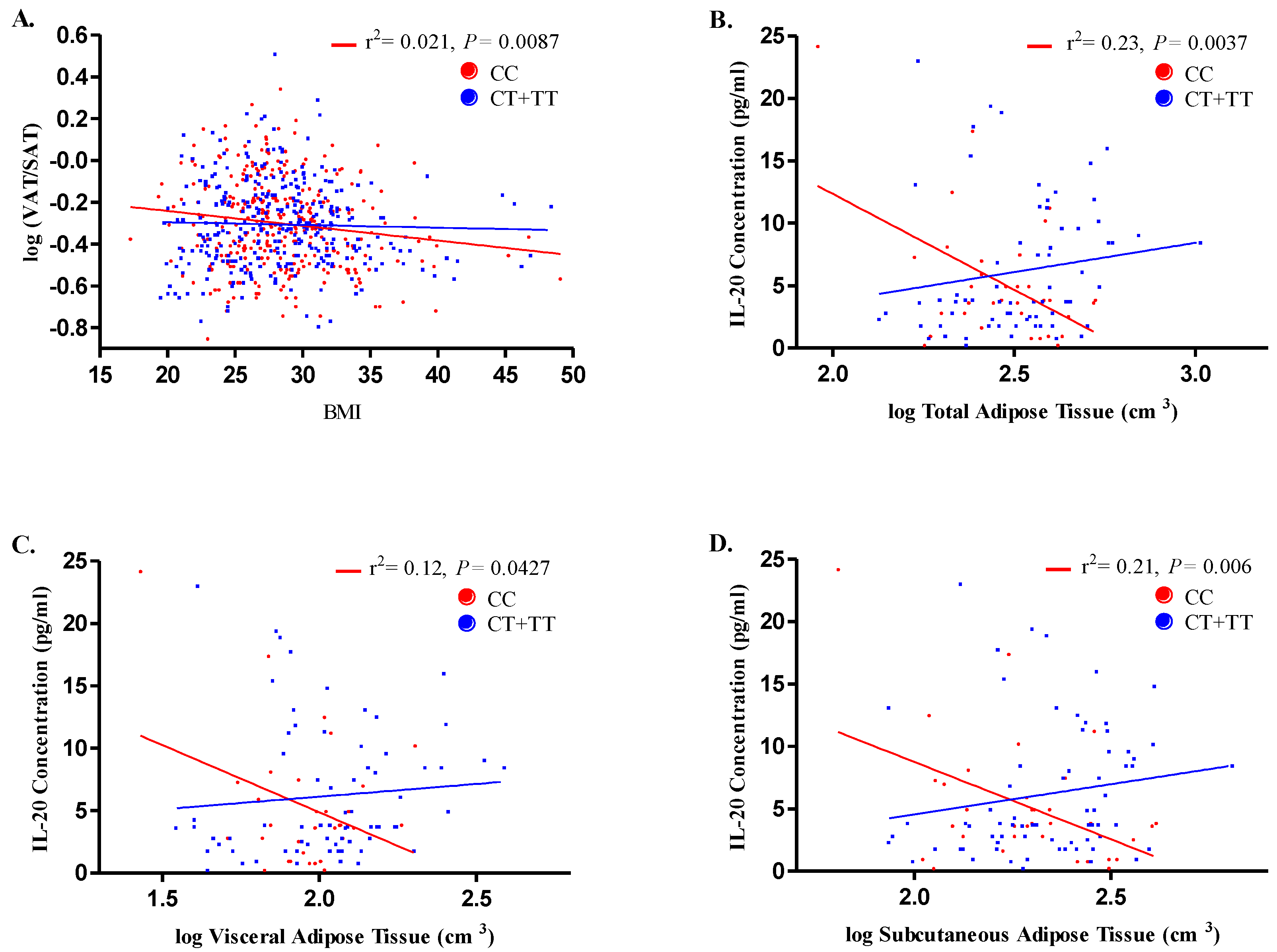
3.5. Correlation of rs1400986 Genotypes with IL-20 Levels and Adipose Tissue
3.6. Haplotypes Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Supplementary File 1Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nowbar, A.N.; Gitto, M.; Howard, J.P.; Francis, D.P.; Al-Lamee, R. Mortality From Ischemic Heart Disease: Analysis of Data From the World Health Organization and Coronary Artery Disease Risk Factors From NCD Risk Factor Collaboration. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005375. [Google Scholar] [CrossRef] [PubMed]
- Chobot, A.; Górowska-Kowolik, K.; Sokołowska, M.; Jarosz-Chobot, P. Obesity and diabetes-Not only a simple link between two epidemics. Diabetes Metab. Res. Rev. 2018, 34, 3042. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.-R.; Ann, S.H.; Won, K.-B.; Park, G.-M.; Kim, Y.-G.; Yang, D.H.; Kang, J.-W.; Lim, T.-H.; Kim, H.-K.; Choe, J.; et al. Association between insulin resistance, hyperglycemia and coronary artery disease according to the presence of diabetes. Sci. Rep. 2019, 9, 6129. [Google Scholar] [CrossRef] [PubMed]
- Fakhrzadeh, H.; Sharifi, F.; Alizadeh, M.; Arzaghi, S.M.; Tajallizade-Khoob, Y.; Tootee, A.; Alatab, S.; Mirarefin, M.; Badamchizade, Z.; Kazemi, H. Relationship between insulin resistance and subclinical atherosclerosis in individuals with and without type 2 diabetes mellitus. J. Diabetes Metab. Disord. 2015, 15, 41. [Google Scholar] [CrossRef]
- Newman, A.B.; Naydeck, B.L.; Sutton-Tyrrell, K.; Edmundowicz, D.; O’Leary, D.; Kronmal, R.; Burke, G.L.; Kuller, L.H. Relationship between coronary artery calcification and other measures of subclinical cardiovascular disease in older adults. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 1674–1679. [Google Scholar] [CrossRef][Green Version]
- Wagenknecht, L.E.; Langefeld, C.D.; Carr, J.J.; Riley, W.; Freedman, B.I.; Moossavi, S.; Bowden, D.W. Race-specific relationships between coronary and carotid artery calcification and carotid intimal medial thickness. Stroke 2004, 35, 97–99. [Google Scholar] [CrossRef]
- Haberka, M.; Skilton, M.; Biedroń, M.; Szóstak-Janiak, K.; Partyka, M.; Matla, M.; Gąsior, Z. Obesity, visceral adiposity and carotid atherosclerosis. J. Diabetes Complicat. 2019, 33, 302–306. [Google Scholar] [CrossRef]
- Baloglu, I.; Turkmen, K.; Selcuk, N.; Tonbul, H.; Ozcicek, A.; Hamur, H.; Iyısoy, S.; Akbas, E. The Relationship between Visceral Adiposity Index and Epicardial Adipose Tissue in Patients with Type 2 Diabetes Mellitus. Exp. Clin. Endocrinol. Diabetes 2019. [Google Scholar] [CrossRef]
- Gruzdeva, O.; Borodkina, D.; Uchasova, E.; Dyleva, Y.; Barbarash, O. Localization of fat depots and cardiovascular risk. Lipids Health Dis. 2018, 17, 218. [Google Scholar] [CrossRef]
- Lontchi-Yimagou, E.; Sobngwi, E.; Matsha, T.E.; Kengne, A.P. Diabetes Mellitus and Inflammation. Curr. Diab. Rep. 2013, 13, 435–444. [Google Scholar] [CrossRef]
- Wu, H.; Ballantyne, C.M. Skeletal muscle inflammation and insulin resistance in obesity. J. Clin. Investig. 2017, 127, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Poston, R.N. Atherosclerosis: Integration of its pathogenesis as a self-perpetuating propagating inflammation: A review. Cardiovasc. Endocrinol. Metab. 2019, 8, 51–61. [Google Scholar] [PubMed]
- Wolk, K.; Kunz, S.; Asadullah, K.; Sabat, R. Cutting edge: Immune cells as sources and targets of the IL-10 family members? J. Immunol. 2002, 168, 5397–5402. [Google Scholar] [CrossRef] [PubMed]
- Pestka, S.; Krause, C.D.; Sarkar, D.; Walter, M.R.; Shi, Y.; Fisher, P.B. Interleukin -10 and R elated C ytokines and R eceptors. Annu. Rev. Immunol. 2004, 22, 929–979. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-Y.; Cheng, B.-C.; Jiang, M.-J.; Hsieh, M.-Y.; Chang, M.-S. IL-20 is expressed in atherosclerosis plaques and promotes atherosclerosis in apolipoprotein E-deficient mice. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 2090–2095. [Google Scholar] [CrossRef]
- Truelove, A.L.; Oleksyk, T.K.; Shrestha, S.; Thio, C.L.; Goedert, J.J.; Donfield, S.M.; Kirk, G.D.; Thomas, D.L.; O’Brien, S.J.; Smith, M.W. Evaluation of IL10, IL19 and IL20 gene polymorphisms and chronic hepatitis B infection outcome. Int. J. Immunogenet. 2008, 35, 255–264. [Google Scholar] [CrossRef]
- Caligiuri, G.; Kaveri, S.V.; Nicoletti, A. IL-20 and atherosclerosis: Another brick in the wall. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 1929–1930. [Google Scholar] [CrossRef]
- Kvist, H.; Chowdhury, B.; Grangård, U.; Tylén, U.; Sjöström, L. Total and visceral adipose-tissue volumes derived from measurements with computed tomography in adult men and women: Predictive equations. Am. J. Clin. Nutr. 1988, 48, 1351–1361. [Google Scholar] [CrossRef]
- Longo, R.; Ricci, C.; Masutti, F.; Vidimari, R.; Crocé, L.S.; Bercich, L.; Tiribelli, C.; Dalla Palma, L. Fatty infiltration of the liver. Quantification by 1H localized magnetic resonance spectroscopy and comparison with computed tomography. Investig. Radiol. 1993, 28, 297–302. [Google Scholar] [CrossRef]
- Mautner, G.C.; Mautner, S.L.; Froehlich, J.; Feuerstein, I.M.; Proschan, M.A.; Roberts, W.C.; Doppman, J.L. Coronary artery calcification: Assessment with electron beam CT and histomorphometric correlation. Radiology 1994, 192, 619–623. [Google Scholar] [CrossRef]
- Posadas-Sánchez, R.; Ocampo-Arcos, W.A.; López-Uribe, A.R.; González-Salazar, M.C.; Cardoso-Saldaña, G.; Mendoza-Pérez, E.; Medina-Urrutia, A.; Jorge-Galarza, E.; Posadas-Romero, C. Asociación del ácido úrico con factores de riesgo cardiovascular y aterosclerosis subclínica en adultos mexicanos. Rev. Mex. Endocrinol. Metab. Nutr. 2014, 1, 14–21. [Google Scholar]
- Medina-Urrutia, A.; Posadas-Romero, C.; Posadas-Sánchez, R.; Jorge-Galarza, E.; Villarreal-Molina, T.; González-Salazar, M.D.C.; Cardoso-Saldaña, G.; Vargas-Alarcón, G.; Torres-Tamayo, M.; Juárez-Rojas, J.G. Role of adiponectin and free fatty acids on the association between abdominal visceral fat and insulin resistance. Cardiovasc. Diabetol. 2015, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Posadas-Sánchez, R.; Pérez-Hernández, N.; Rodríguez-Pérez, J.M.; Coral-Vázquez, R.M.; Roque-Ramírez, B.; Llorente, L.; Lima, G.; Flores-Dominguez, C.; Villarreal-Molina, T.; Posadas-Romero, C.; et al. Interleukin-27 polymorphisms are associated with premature coronary artery disease and metabolic parameters in the Mexican population: The genetics of atherosclerotic disease (GEA) Mexican study. Oncotarget 2017, 8, 64459–64470. [Google Scholar] [CrossRef] [PubMed]
- Faggiano, P.; Dasseni, N.; Gaibazzi, N.; Rossi, A.; Henein, M.; Pressman, G. Cardiac calcification as a marker of subclinical atherosclerosis and predictor of cardiovascular events: A review of the evidence. Eur. J. Prev. Cardiol. 2019, 26, 1191–1204. [Google Scholar] [CrossRef] [PubMed]
- Detrano, R.; Guerci, A.D.; Carr, J.J.; Bild, D.E.; Burke, G.; Folsom, A.R.; Liu, K.; Shea, S.; Szklo, M.; Bluemke, D.A.; et al. Coronary Calcium as a Predictor of Coronary Events in Four Racial or Ethnic Groups. N. Engl. J. Med. 2008, 358, 1336–1345. [Google Scholar] [CrossRef] [PubMed]
- Greenland, P.; LaBree, L.; Azen, S.P.; Doherty, T.M.; Detrano, R.C. Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. JAMA 2004, 291, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, D.K.; Nurnberger, J.I. A rapid non-enzymatic method for the preparation of HMW DNA from blood for RFLP studies. Nucleic Acids Res. 1991, 19, 5444. [Google Scholar] [CrossRef]
- Kingo, K.; Kõks, S.; Nikopensius, T.; Silm, H.; Vasar, E. Polymorphisms in the interleukin-20 gene: Relationships to plaque-type psoriasis. Genes Immun. 2004, 5, 117–121. [Google Scholar] [CrossRef]
- Yamamoto-Furusho, J.K.; De-León-Rendón, J.L.; de la Torre, M.G.; Alvarez-León, E.; Vargas-Alarcón, G. Genetic polymorphisms of interleukin 20 (IL-20) in patients with ulcerative colitis. Immunol. Lett. 2013, 149, 50–53. [Google Scholar] [CrossRef]
- Galimova, E.; Rätsep, R.; Traks, T.; Kingo, K.; Escott-Price, V.; Kõks, S. Interleukin-10 family cytokines pathway: Genetic variants and psoriasis. Br. J. Dermatol. 2017, 176, 1577–1587. [Google Scholar] [CrossRef]
- Zhao, L.; Zheng, M.; Guo, Z.; Li, K.; Liu, Y.; Chen, M.; Yang, X. Circulating Serpina3 levels predict the major adverse cardiac events in patients with myocardial infarction. Int. J. Cardiol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.S.; Lee, J.S.; Kim, J.A.; Roh, E.; Lee, Y.B.; Hong, S.H.; Yoo, H.J.; Baik, S.H.; Kim, N.H.; Seo, J.A.; et al. γ-Glutamyltransferase Variability and the Risk of Mortality, Myocardial Infarction and Stroke: A Nationwide Population-Based Cohort Study. J. Clin. Med. 2019, 8, 832. [Google Scholar] [CrossRef] [PubMed]
- Bobrus-Chociej, A.; Flisiak-Jackiewicz, M.; Daniluk, U.; Wojtkowska, M.; Kłusek-Oksiuta, M.; Tarasów, E.; Lebensztejn, D. Estimation of gamma-glutamyl transferase as a suitable simple biomarker of the cardiovascular risk in children with non-alcoholic fatty liver disease. Acta Biochim. Pol. 2018, 65, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Gaggini, M.; Morelli, M.; Buzzigoli, E.; DeFronzo, R.A.; Bugianesi, E.; Gastaldelli, A. Non-alcoholic fatty liver disease (NAFLD) and its connection with insulin resistance, dyslipidemia, atherosclerosis and coronary heart disease. Nutrients 2013, 5, 1544–1560. [Google Scholar] [CrossRef] [PubMed]
- Estep, J.M.; Goodman, Z.; Sharma, H.; Younossi, E.; Elarainy, H.; Baranova, A.; Younossi, Z. Adipocytokine expression associated with miRNA regulation and diagnosis of NASH in obese patients with NAFLD. Liver Int. 2015, 35, 1367–1372. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Kishi, S.; Ninomiya, K.; Tomii, D.; Koseki, K.; Sato, Y.; Okuno, T.; Sato, K.; Koike, H.; Yahagi, K.; et al. Impact of abdominal fat distribution, visceral fat and subcutaneous fat on coronary plaque scores assessed by 320-row computed tomography coronary angiography. Atherosclerosis 2019, 287, 155–161. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Control (n = 672) | SA (n = 274) | p | |
|---|---|---|---|
| Age (years) | 52 ± 9 | 59 ± 8 | <0.0001 |
| Gender (% male) | 38.2 | 72.6 | <0.0001 |
| Body Mass Index (kg/m2) | 27.9 (25.4–30.9) | 28.1 (25.6–31.3) | 0.219 |
| Waist Circumferences (cm) | 93.4 ± 11.7 | 97.4 ± 11.1 | <0.0001 |
| Systolic Blood Pressure (mmHg) | 115 (106–126) | 124 (113–137) | <0.0001 |
| Diastolic Blood Pressure (mmHg) | 72 (66–78) | 77 (70–83) | <0.0001 |
| Total Adipose Fat (cm3) | 443 (350–542) | 442 (353–569) | 0.391 |
| Visceral Adipose fat (cm3) | 146 (105–188) | 180 (141–230) | <0.0001 |
| Subcutaneous Adipose fat (cm3) | 286 (218–371) | 260 (193–340) | 0.002 |
| Total Cholesterol (mg/dL) | 190 (168–209) | 198 (171–221) | 0.002 |
| HDL-C (mg/dL) | 47 (37–57) | 43 (36–50) | <0.0001 |
| LDL-C (mg/dL) | 115.6 (96.2–133.2) | 124.4 (102.3–145.2) | <0.0001 |
| Triglycerides (mg/dL) | 141 (107–194) | 158 (118–206) | 0.007 |
| Non-HDL-Cholesterol (mg/dL) | 140 (120–162) | 153 (129–175) | <0.0001 |
| ALT (IU/L) | 23 (17–32) | 22 (17–32) | 0.819 |
| AST (IU/L) | 25 (21–30) | 25 (21–31) | 0.542 |
| GGT (IU/L) | 24 (17–41) | 29 (21–41) | 0.001 |
| Alkaline Phosphatase (IU/L) | 81 (68–98) | 77 (65–93) | 0.013 |
| Apo B (mg/dL) | 86 (72–106) | 96 (79–119) | <0.0001 |
| Apo A1 (mg/dL) | 132 (113–157) | 133 (113–157) | 0.81 |
| Apo-B/Apo-A | 0.65 (0.51–0.84) | 0.7 (0.6–0.9) | 0.001 |
| Glucose (mg/dL) | 90 (84–97) | 95 (87–107) | <0.0001 |
| Insulin (µIU/mL) | 18 (13–24) | 19 (13–25) | 0.212 |
| HOMA-IR | 3.9 (2.7–5.8) | 4.7 (3.1–6.8) | <0.0001 |
| hsCRP (mg/dL) | 1.69 (0.87–3.46) | 1.71 (0.89–3.45) | 0.76 |
| Creatinine (mg/dL) | 0.8 (0.7–0.9) | 0.9 (0.7–1.1) | <0.0001 |
| Adiponectin (µg/mL) | 8.4 (5–12.9) | 6.4 (4.2–10.2) | <0.0001 |
| Uric Acid (mg/dL) | 5.4 (4.4–6.4) | 5.9 (4.9–6.9) | <0.0001 |
| Albumin (µg/mL) | 6.3 (2.9–12) | 7.2 (2.9–19) | 0.026 |
| Free Fatty Acid (mEq/L) | 0.5 (0.4–0.7) | 0.6 (0.4–0.7) | 0.631 |
| IR of the Adipose Tissue | 9.7 (6.2–14.5) | 10.2 (6.6–13.9) | 0.629 |
| Control (n = 672) | SA (n = 274) | * P | |
|---|---|---|---|
| Total Cholesterol >200 mg/dL (%) | 35.4 | 47.1 | 0.001 |
| LDL-Cholesterol > 130 mg/dL (%) | 29.3 | 42.9 | <0.0001 |
| Hypoalphalipoproteinemia (%) | 47.7 | 45.3 | 0.518 |
| Hypertriglyceridemia (%) | 45.2 | 53.5 | 0.022 |
| Non-HDL-Cholesterol > 160 mg/dL (%) | 25.9 | 42 | <0.0001 |
| Overweight (%) | 45.8 | 47.4 | 0.114 |
| Obesity (%) | 31.1 | 33.9 | 0.083 |
| Abdominal Obesity (%) | 79.6 | 82.1 | 0.417 |
| Type 2 Diabetes Mellitus (%) | 10.6 | 23 | <0.0001 |
| Hyperinsulinemia (%) | 55.4 | 62.8 | 0.023 |
| Insulin resistance (%) | 57.5 | 67.9 | 0.002 |
| Metabolic Syndrome (%) | 40.6 | 54 | <0.0001 |
| Hypertension (%) | 29.2 | 49.6 | <0.0001 |
| High Total Abdominal Tissue (%) | 55.4 | 61.7 | 0.045 |
| High Subcutaneous Abdominal Tissue (%) | 50 | 54.7 | 0.106 |
| High Visceral Abdominal Tissue (%) | 58.8 | 73.7 | <0.0001 |
| Fatty Liver (%) | 32.1 | 39.3 | 0.024 |
| SNP | Model | Genotypes and Alleles | SA | Control | p | OR | 95% CI |
|---|---|---|---|---|---|---|---|
| n | n | ||||||
| rs1400986 | CC | 177 | 336 | ||||
| CT | 87 | 293 | |||||
| TT | 10 | 43 | |||||
| C | 441 | 965 | 0.0001 | 0.61 | 0.48–0.78 | ||
| T | 107 | 379 | |||||
| codominant1 | CC | 177 | 336 | 0.0001 | 0.51 | 0.36–0.73 | |
| CT | 87 | 293 | |||||
| codominant2 | CC | 177 | 336 | 0.014 | 0.36 | 0.16–0.81 | |
| TT | 10 | 43 | |||||
| dominant | CC | 177 | 336 | 0.0001 | 0.49 | 0.35–0.69 | |
| CT + TT | 97 | 336 | |||||
| recessive | CC + CT | 264 | 629 | 0.063 | 0.47 | 0.21–1.04 | |
| TT | 10 | 43 | |||||
| additive | – | – | – | 0.0001 | 0.55 | 0.41–0.73 | |
| rs1518108 | CC | 79 | 181 | ||||
| CT | 140 | 336 | |||||
| TT | 55 | 155 | |||||
| C | 298 | 698 | 0.229 | 0.89 | 0.75–1.06 | ||
| T | 250 | 646 | |||||
| codominant1 | CC | 79 | 181 | 0.246 | 0.79 | 0.54–1.16 | |
| CT | 140 | 336 | |||||
| codominant2 | CC | 79 | 181 | 0.048 | 0.62 | 0.39–0.99 | |
| TT | 55 | 155 | |||||
| dominant | CC | 79 | 181 | 0.102 | 0.74 | 0.51–1.06 | |
| CT + TT | 195 | 491 | |||||
| recessive | CC + CT | 219 | 517 | 0.110 | 0.72 | 0.49–1.07 | |
| TT | 55 | 155 | |||||
| additive | – | – | – | 0.0480 | 0.79 | 0.63–0.99 |
| SNP | Model | Genotypes | Variable | p | OR | 95% CI | |
|---|---|---|---|---|---|---|---|
| (i) Controls | |||||||
| rs1400986 | Inflammation | ||||||
| Yes n = 203 | No n = 469 | ||||||
| codominant1 | CC | 91 | 245 | 0.047 | 1.45 | 1.01–2.10 | |
| CT | 101 | 192 | |||||
| GGT > 75 | |||||||
| Yes n = 267 | No n = 400 | ||||||
| codominant2 | CC | 140 | 196 | 0.023 | 0.41 | 0.19–0.88 | |
| TT | 10 | 32 | |||||
| recessive | CC + CT | 257 | 368 | 0.024 | 0.42 | 0.19–0.89 | |
| TT | 10 | 32 | |||||
| rs1518108 | Hypertension | ||||||
| Yes n = 196 | No n = 476 | ||||||
| codominant1 | CC | 38 | 143 | 0.008 | 1.83 | 1.16–2.86 | |
| CT | 113 | 223 | |||||
| dominant | CC | 38 | 143 | 0.016 | 1.68 | 1.10–2.59 | |
| CT + TT | 158 | 333 | |||||
| Inflammation | |||||||
| Yes n = 203 | No n = 469 | ||||||
| codominant2 | CC | 43 | 138 | 0.037 | 1.73 | 1.03–2.89 | |
| TT | 51 | 104 | |||||
| recessive | CC + CT | 152 | 365 | 0.036 | 1.31 | 1.01–1.70 | |
| TT | 51 | 104 | |||||
| Total abdominal tissue >75 | |||||||
| Yes n = 360 | No n = 290 | ||||||
| codominant1 | CC | 96 | 79 | 0.025 | 1.69 | 1.07–2.69 | |
| CT | 179 | 146 | |||||
| dominant | CC | 96 | 79 | 0.048 | 1.54 | 1.004–2.37 | |
| CT + TT | 264 | 211 | |||||
| (ii) SA | |||||||
| rs1518108 | GGT > 75 | ||||||
| Yes n = 111 | No n = 163 | ||||||
| codominant1 | CC | 43 | 36 | 0.023 | 0.51 | 0.28–0.91 | |
| CT | 51 | 88 | |||||
| codominant2 | CC | 43 | 36 | 0.006 | 0.35 | 0.16–0.74 | |
| TT | 17 | 39 | |||||
| dominant | CC | 43 | 36 | 0.006 | 0.46 | 0.26–0.79 | |
| CT + TT | 68 | 127 | |||||
| additive | - | - | - | 0.004 | 0.58 | 0.40–0.99 | |
| ALP > 75 | |||||||
| Yes n = 91 | No n = 183 | ||||||
| codominant1 | CC | 36 | 43 | 0.011 | 0.46 | 0.26–0.84 | |
| CT | 38 | 101 | |||||
| dominant | CC | 36 | 43 | 0.01 | 0.48 | 0.28–0.83 | |
| CT + TT | 55 | 140 | |||||
| additive | - | - | - | 0.046 | 0.68 | 0.47–0.99 | |
| Haplotypes | SA (n = 274) | Control (n = 672) | Χ2 | P | OR | 95% CI | ||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | |||||
| CC | 134 | 48.9 | 298 | 44.4 | 3.88 | 0.077 | 1.19 | 1.01–1.42 |
| CT | 87 | 31.6 | 184 | 27.4 | 3.376 | 0.066 | 1.22 | 1.00–1.48 |
| TT | 39 | 14.2 | 139 | 20.7 | 10.684 | 0.00016 | 0.63 | 0.50–0.80 |
| TC | 14 | 5.4 | 51 | 7.6 | 2.94 | 0.086 | 0.69 | 0.48–0.99 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angeles-Martínez, J.; Posadas-Sánchez, R.; Bravo-Flores, E.; González-Salazar, M.d.C.; Vargas-Alarcón, G. Common Variants in IL-20 Gene are Associated with Subclinical Atherosclerosis, Cardiovascular Risk Factors and IL-20 Levels in the Cohort of the Genetics of Atherosclerotic Disease (GEA) Mexican Study. Biomolecules 2020, 10, 75. https://doi.org/10.3390/biom10010075
Angeles-Martínez J, Posadas-Sánchez R, Bravo-Flores E, González-Salazar MdC, Vargas-Alarcón G. Common Variants in IL-20 Gene are Associated with Subclinical Atherosclerosis, Cardiovascular Risk Factors and IL-20 Levels in the Cohort of the Genetics of Atherosclerotic Disease (GEA) Mexican Study. Biomolecules. 2020; 10(1):75. https://doi.org/10.3390/biom10010075
Chicago/Turabian StyleAngeles-Martínez, Javier, Rosalinda Posadas-Sánchez, Eyerahi Bravo-Flores, María del Carmen González-Salazar, and Gilberto Vargas-Alarcón. 2020. "Common Variants in IL-20 Gene are Associated with Subclinical Atherosclerosis, Cardiovascular Risk Factors and IL-20 Levels in the Cohort of the Genetics of Atherosclerotic Disease (GEA) Mexican Study" Biomolecules 10, no. 1: 75. https://doi.org/10.3390/biom10010075
APA StyleAngeles-Martínez, J., Posadas-Sánchez, R., Bravo-Flores, E., González-Salazar, M. d. C., & Vargas-Alarcón, G. (2020). Common Variants in IL-20 Gene are Associated with Subclinical Atherosclerosis, Cardiovascular Risk Factors and IL-20 Levels in the Cohort of the Genetics of Atherosclerotic Disease (GEA) Mexican Study. Biomolecules, 10(1), 75. https://doi.org/10.3390/biom10010075