
High Versus Low Adherence to the Mediterranean Diet for Prevention of Diabetes Mellitus Type 2: A Systematic Review and Meta-Analysis

 ,
,  ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Literature Search
2.3. Study Selection and Eligibility Criteria
2.4. Data Selection and Extraction
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
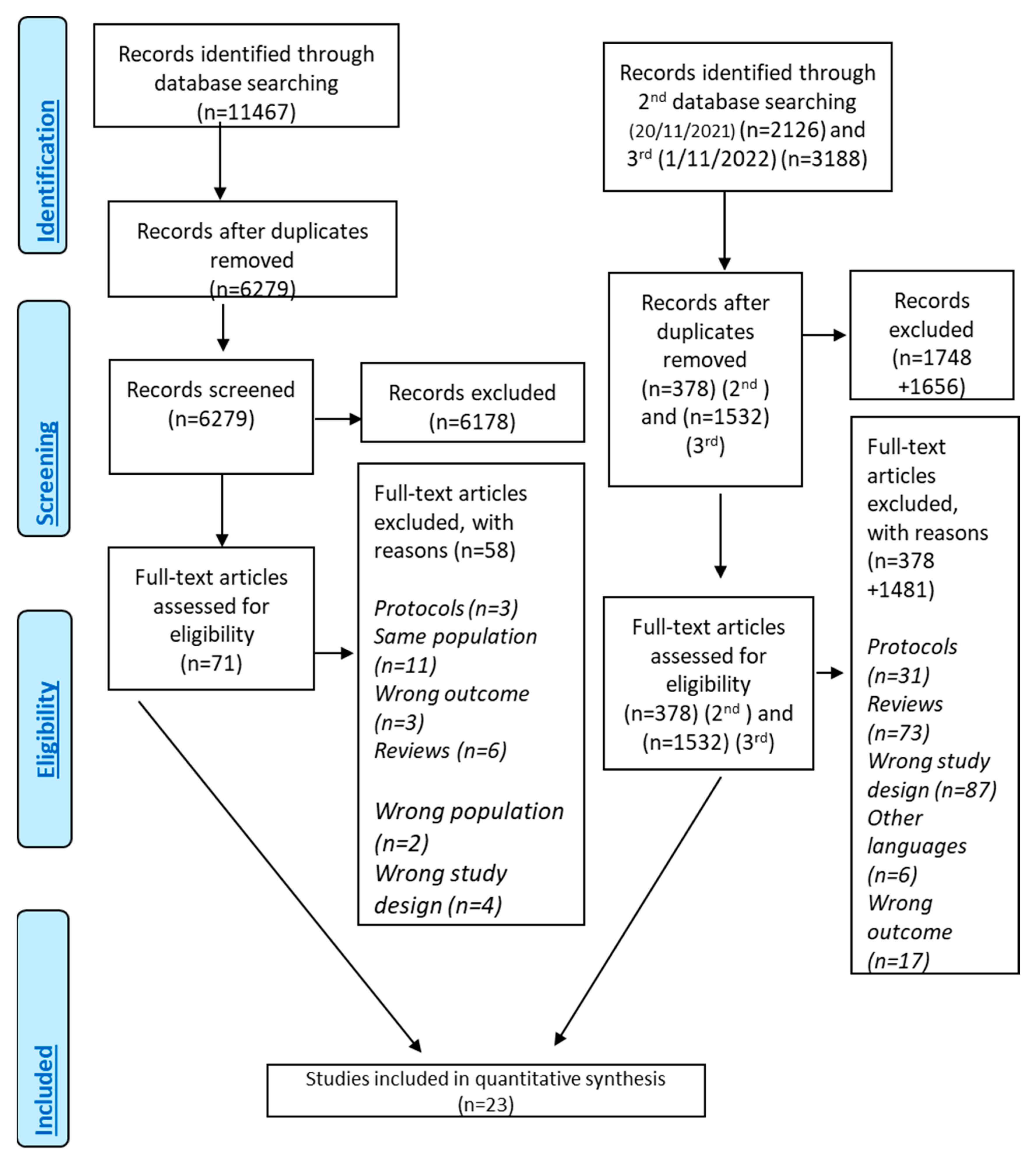
3.1. Search Results
3.2. Quality of Included Studies
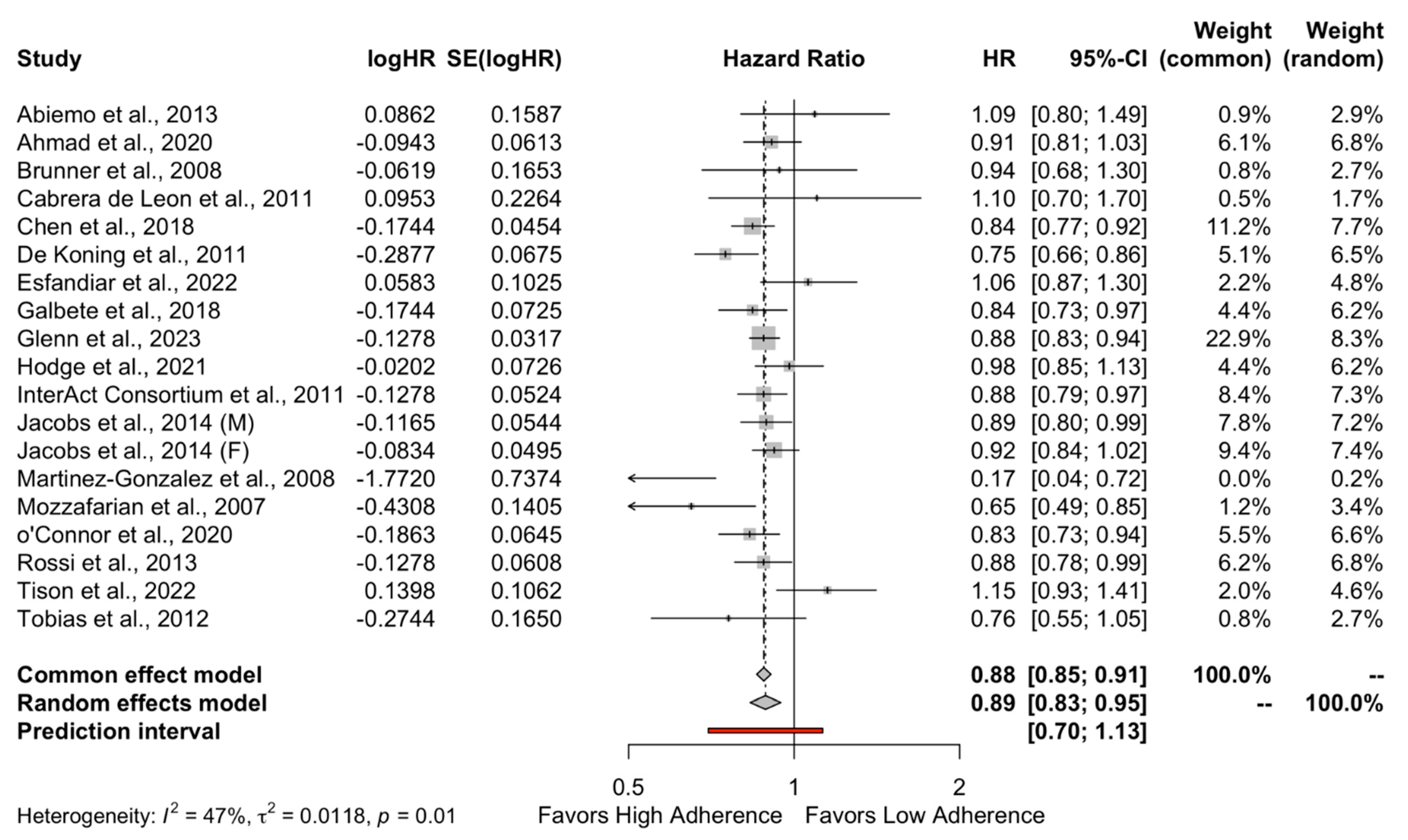
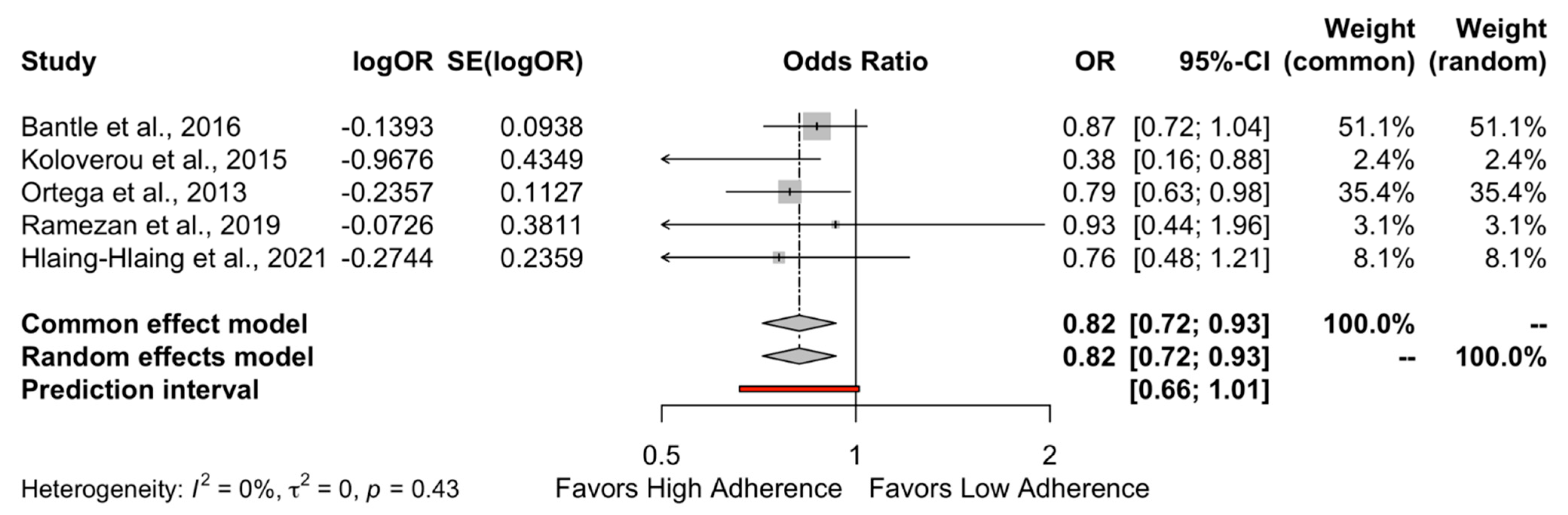
3.3. Level of MD Adherence and DMT-2 Risk
3.4. Certainty of Evidence
3.5. Subgroup Analysis
3.6. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADA | American Diabetes Association |
| aMed | Alternative Mediterranean Diet Score |
| CI | Confidence Interval |
| CVD | Cardiovascular Disease |
| DM | Diabetes Mellitus |
| DMT-2 | Diabetes Mellitus Type 2 |
| GLP-1 | Glycogen Like Peptide-1 |
| GRADE | Grading of Recommendations Assessment, Development, and Evaluation |
| HbA1c | Glycated Hemoglobin |
| HR | Hazard ratio |
| IDF | International Diabetes Federation |
| LDL Cholesterol | Low Density Lipoprotein Cholesterol |
| MD | Mediterranean Diet |
| MOOSE | Meta-analysis of Observational Studies in Epidemiology |
| MDS | Mediterranean Diet Score |
| OGTT | Oral Glucose Tolerance Test |
| OR | Odds Ratio |
| PI | Prediction Intervals |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| rMed | Relative Mediterranean Diet Score |
| RR | Risk Ratio |
References
- International Diabetes Federation. IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019. [Google Scholar]
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- Atchison, E.A.; Gridley, G.; Carreon, J.D.; Leitzmann, M.F.; McGlynn, K.A. Risk of cancer in a large cohort of U.S. veterans with diabetes. Int. J. Cancer 2011, 128, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Buckland, G.; Agudo, A.; Luján, L.; Jakszyn, P.; Bueno-de-Mesquita, H.B.; Palli, D.; Boeing, H.; Carneiro, F.; Krogh, V.; Sacerdote, C.; et al. Adherence to a Mediterranean diet and risk of gastric adenocarcinoma within the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort study. Am. J. Clin. Nutr. 2010, 91, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Diabetes and gastric cancer: The potential links. WJG 2014, 20, 1701. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022, 45 (Suppl. 1), S17–S38. [Google Scholar] [CrossRef]
- Keys, A.; Mienotti, A.; Karvonen, M.J.; Aravanis, C.; Blackburn, H.; Buzina, R.; Djordjevic, B.S.; Dontas, A.S.; Fidanza, F.; Keys, M.H.; et al. The Diet and 15-Year Death Rate in the Seven Countries Study. Am. J. Epidemiol. 1986, 124, 903–915. [Google Scholar] [CrossRef]
- Kromhout, D.; Menotti, A.; Blackburn, H.; Keys, A. The Seven Countries Study: A Scientific Adventure in Cardiovascular Disease Epidemiology; Rijksinstituut voor Volkgezondheid en Milieuhygiëne: Bilthoven, The Netherlands, 1994. [Google Scholar]
- Kromhout, D.; Bosschieter, E.B.; Coulander, C.d.L. The Inverse Relation between Fish Consumption and 20-Year Mortality from Coronary Heart Disease. N. Engl. J. Med. 1985, 312, 1205–1209. [Google Scholar] [CrossRef]
- André, P.; Proctor, G.; Driollet, B.; Garcia-Esquinas, E.; Lopez-Garcia, E.; Neyraud, E.; Rodriguez-Artalejo, F.; Morzel, M.; Féart, C. The role of overweight in the association between the Mediterranean diet and the risk of type 2 diabetes mellitus: A mediation analysis among 21,585 UK biobank participants. Int. J. Epidemiol. 2020, 49, 1582–1590. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Schroder, H. Protective mechanisms of the Mediterranean diet in obesity and type 2 diabetes. J. Nutr. Biochem. 2007, 18, 149–160. [Google Scholar] [CrossRef]
- De Lorgeril, M.; Salen, P.; Martin, J.L.; Monjaud, I.; Delaye, J.; Mamelle, N. Mediterranean Diet, Traditional Risk Factors, and the Rate of Cardiovascular Complications After Myocardial Infarction: Final Report of the Lyon Diet Heart Study. Circulation 1999, 99, 779–785. [Google Scholar] [CrossRef]
- Estruch, R. Effects of a Mediterranean-Style Diet on Cardiovascular Risk Factors: A Randomized Trial. Ann. Intern. Med. 2006, 145, 1. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Kastorini, C.M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The Effect of Mediterranean Diet on Metabolic Syndrome and its Components. J. Am. Coll. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef] [PubMed]
- Marín, C.; Yubero-Serrano, E.; López-Miranda, J.; Pérez-Jiménez, F. Endothelial Aging Associated with Oxidative Stress Can Be Modulated by a Healthy Mediterranean Diet. IJMS 2013, 14, 8869–8889. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Jiménez, F.; López-Miranda, J.; Mata, P. Protective effect of dietary monounsaturated fat on arteriosclerosis: Beyond cholesterol. Atherosclerosis 2002, 163, 385–398. [Google Scholar] [CrossRef]
- Sánchez-Taínta, A.; Estruch, R.; Bulló, M.; Corella, D.; Gómez-Gracia, E.; Fiol, M.; Algorta, J.; Covas, M.-I.; Lapetra, J.; Zazpe, I.; et al. Adherence to a Mediterranean-type diet and reduced prevalence of clustered cardiovascular risk factors in a cohort of 3204 high-risk patients. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 589–593. [Google Scholar] [CrossRef]
- Sofi, F. The Mediterranean diet revisited: Evidence of its effectiveness grows. Curr. Opin. Cardiol. 2009, 24, 442–446. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Chrysoula, L.; Leonida, I.; Kotzakioulafi, E.; Theodoridis, X.; Chourdakis, M. Impact of the level of adherence to the Mediterranean Diet on blood pressure: A systematic review and meta-analysis of observational studies. Clin. Nutr. 2021, 40, 5771–5780. [Google Scholar] [CrossRef]
- Abiemo, E.E.; Alonso, A.; Nettleton, J.A.; Steffen, L.M.; Bertoni, A.G.; Jain, A.; Lutsey, P.L. Relationships of the Mediterranean dietary pattern with insulin resistance and diabetes incidence in the Multi-Ethnic Study of Atherosclerosis (MESA). Br. J. Nutr. 2013, 109, 1490–1497. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Chrysoula, L.; Kotzakioulafi, E.; Theodoridis, X.; Chourdakis, M. Impact of the Level of Adherence to Mediterranean Diet on the Parameters of Metabolic Syndrome: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2021, 13, 1514. [Google Scholar] [CrossRef]
- Esposito, K.; Kastorini, C.M.; Panagiotakos, D.B.; Giugliano, D. Prevention of Type 2 Diabetes by Dietary Patterns: A Systematic Review of Prospective Studies and Meta-Analysis. Metab. Syndr. Relat. Disord. 2010, 8, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Marfella, R.; Ciotola, M.; di Palo, C.; Giugliano, F.; Giugliano, G.; D’Armiento, M.; D’Andrea, F.; Giugliano, D. Effect of a Mediterranean-Style Diet on Endothelial Dysfunction and Markers of Vascular Inflammation in the Metabolic Syndrome: A Randomized Trial. JAMA 2004, 292, 1440. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.L.; Goldfine, I.D.; Maddux, B.A.; Grodsky, G.M. Are Oxidative Stress−Activated Signaling Pathways Mediators of Insulin Resistance and β-Cell Dysfunction? Diabetes 2003, 52, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kesse-Guyot, E.; Ahluwalia, N.; Lassale, C.; Hercberg, S.; Fezeu, L.; Lairon, D. Adherence to Mediterranean diet reduces the risk of metabolic syndrome: A 6-year prospective study. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Koloverou, E.; Esposito, K.; Giugliano, D.; Panagiotakos, D. The effect of Mediterranean diet on the development of type 2 diabetes mellitus: A meta-analysis of 10 prospective studies and 136,846 participants. Metabolism 2014, 63, 903–911. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary patterns: A Mediterranean diet score and its relation to clinical and biological markers of cardiovascular disease risk. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 559–568. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Missbach, B.; König, J.; Hoffmann, G. Adherence to a Mediterranean diet and risk of diabetes: A systematic review and meta-analysis. Public Health Nutr. 2015, 18, 1292–1299. [Google Scholar] [CrossRef]
- Barzi, F.; Woodward, M.; Marfisi, R.M.; Tavazzi, L.; Valagussa, F.; Marchioli, R.; GISSI-Prevenzione Investigators. Mediterranean diet and all-causes mortality after myocardial infarction: Results from the GISSI-Prevenzione trial. Eur. J. Clin. Nutr. 2003, 57, 604–611. [Google Scholar] [CrossRef]
- Becerra-Tomás, N.; Blanco Mejía, S.; Viguiliouk, E.; Khan, T.; Kendall, C.W.C.; Kahleova, H.; Rahelić, D.; Sievenpiper, J.L.; Salas-Salvadó, J. Mediterranean diet, cardiovascular disease and mortality in diabetes: A systematic review and meta-analysis of prospective cohort studies and randomized clinical trials. Crit. Rev. Food Sci. Nutr. 2020, 60, 1207–1227. [Google Scholar] [CrossRef]
- Brunner, E.J.; Mosdøl, A.; Witte, D.R.; Martikainen, P.; Stafford, M.; Shipley, M.J.; Marmot, M.G. Dietary patterns and 15-y risks of major coronary events, diabetes, and mortality. Am. J. Clin. Nutr. 2008, 87, 1414–1421. [Google Scholar] [CrossRef]
- Fung, T.T.; Rexrode, K.M.; Mantzoros, C.S.; Manson, J.E.; Willett, W.C.; Hu, F.B. Mediterranean Diet and Incidence of and Mortality From Coronary Heart Disease and Stroke in Women. Circulation 2009, 119, 1093–1100. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Cai, X.; Mai, W.; Li, M.; Hu, Y. Association between prediabetes and risk of cardiovascular disease and all cause mortality: Systematic review and meta-analysis. BMJ 2016, 23, i5953. [Google Scholar] [CrossRef] [PubMed]
- Mitrou, P.N. Mediterranean Dietary Pattern and Prediction of All-Cause Mortality in a US Population: Results From the NIH-AARP Diet and Health Study. Arch. Intern. Med. 2007, 167, 2461. [Google Scholar] [CrossRef] [PubMed]
- Soltani, S.; Jayedi, A.; Shab-Bidar, S.; Becerra-Tomás, N.; Salas-Salvadó, J. Adherence to the Mediterranean Diet in Relation to All-Cause Mortality: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. Adv. Nutr. 2019, 10, 1029–1039. [Google Scholar] [CrossRef]
- Fung, T.T.; McCullough, M.L.; Newby, P.; Manson, J.E.; Meigs, J.B.; Rifai, N.; Willett, W.C.; Hu, F.B. Diet-quality scores and plasma concentrations of markers of inflammation and endothelial dysfunction. Am. J. Clin. Nutr. 2005, 82, 163–173. [Google Scholar] [CrossRef]
- Lopez-Garcia, E.; Schulze, M.B.; Fung, T.T.; Meigs, J.B.; Rifai, N.; Manson, J.E.; Hu, F.B. Major dietary patterns are related to plasma concentrations of markers of inflammation and endothelial dysfunction. Am. J. Clin. Nutr. 2004, 80, 1029–1035. [Google Scholar] [CrossRef]
- Mantzoros, C.S.; Williams, C.J.; Manson, J.E.; Meigs, J.B.; Hu, F.B. Adherence to the Mediterranean dietary pattern is positively associated with plasma adiponectin concentrations in diabetic women. Am. J. Clin. Nutr. 2006, 84, 328–335. [Google Scholar] [CrossRef]
- Meigs, J.B. Biomarkers of Endothelial Dysfunction and Risk of Type 2 Diabetes Mellitus. JAMA 2004, 291, 1978. [Google Scholar] [CrossRef]
- Perez-Martinez, P.; Lopez-Miranda, J.; Blanco-Colio, L.; Bellido, C.; Jimenez, Y.; Moreno, J.A.; Delgado-Lista, J.; Egido, J.; Perez-Jimenez, F. The chronic intake of a Mediterranean diet enriched in virgin olive oil, decreases nuclear transcription factor κB activation in peripheral blood mononuclear cells from healthy men. Atherosclerosis 2007, 194, e141–e146. [Google Scholar] [CrossRef]
- Tsoukas, M.A.; Farr, O.M.; Mantzoros, C.S. Advances in metabolism. Metabolism 2013, 62, 1700–1713. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Orfanos, P.; Norat, T.; Bueno-De-Mesquita, B.; Ocké, M.C.; Peeters, P.H.; van der Schouw, Y.T.; Boeing, H.; Hoffmann, K.; Boffetta, P.; et al. Modified Mediterranean diet and survival: EPIC-elderly prospective cohort study. BMJ 2005, 330, 991. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Kouris-Blazos, A.; Wahlqvist, M.L.; Gnardellis, C.; Lagiou, P.; Polychronopoulos, E.; Vassilakou, T.; Lipworth, L.; Trichopoulos, D. Diet and overall survival in elderly people. BMJ 1995, 311, 1457–1460. [Google Scholar] [CrossRef]
- Filippatos, T.D.; Panagiotakos, D.B.; Georgousopoulou, E.N.; Pitaraki, E.; Kouli, G.-M.; Chrysohoou, C.; Tousoulis, D.; Stefanadis, C.; Pitsavos, C.; ATTICA Study Group. Mediterranean Diet and 10-year (2002–2012) Incidence of Diabetes and Cardiovascular Disease in Participants with Prediabetes: The ATTICA study. Rev. Diabet Stud. 2016, 13, 226–235. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Bulló, M.; Babio, N.; Martínez-González, M.; Ibarrola-Jurado, N.; Basora, J.; Estruch, R.; Covas, M.I.; Corella, D.; Arós, F.; et al. Reduction in the Incidence of Type 2 Diabetes With the Mediterranean Diet. Diabetes Care 2011, 34, 14–19. [Google Scholar] [CrossRef]
- Biesalski, H.K. Diabetes preventive components in the Mediterranean diet. Eur. J. Nutr. 2004, 43, 26–30. [Google Scholar] [CrossRef]
- Bonnet, F.; for the RISC Study Group; Disse, E.; Laville, M.; Mari, A.; Højlund, K.; Anderwald, C.H.; Piatti, P.; Balkau, B. Moderate alcohol consumption is associated with improved insulin sensitivity, reduced basal insulin secretion rate and lower fasting glucagon concentration in healthy women. Diabetologia 2012, 55, 3228–3237. [Google Scholar] [CrossRef]
- Chandalia, M.; Garg, A.; Lutjohann, D.; von Bergmann, K.; Grundy, S.M.; Brinkley, L.J. Beneficial Effects of High Dietary Fiber Intake in Patients with Type 2 Diabetes Mellitus. N. Engl. J. Med. 2000, 342, 1392–1398. [Google Scholar] [CrossRef]
- Georgoulis, M.; Kontogianni, M.; Yiannakouris, N. Mediterranean Diet and Diabetes: Prevention and Treatment. Nutrients 2014, 6, 1406–1423. [Google Scholar] [CrossRef]
- Rossi, M.; Turati, F.; Lagiou, P.; Trichopoulos, D.; Augustin, L.S.; la Vecchia, C.; Trichopoulou, A. Mediterranean diet and glycaemic load in relation to incidence of type 2 diabetes: Results from the Greek cohort of the population-based European Prospective Investigation into Cancer and Nutrition (EPIC). Diabetologia 2013, 56, 2405–2413. [Google Scholar] [CrossRef]
- Sarsangi, P.; Salehi-Abargouei, A.; Ebrahimpour-Koujan, S.; Esmaillzadeh, A. Association between Adherence to the Mediterranean Diet and Risk of Type 2 Diabetes: An Updated Systematic Review and Dose–Response Meta-Analysis of Prospective Cohort Studies. Adv. Nutr. 2022, 13, 1787–1798. [Google Scholar] [CrossRef]
- Zeraattalab-Motlagh, S.; Jayedi, A.; Shab-Bidar, S. Mediterranean dietary pattern and the risk of type 2 diabetes: A systematic review and dose–response meta-analysis of prospective cohort studies. Eur. J. Nutr. 2022, 61, 1735–1748. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, A.D.; Gaston, D.R.; Permann, C.J.; Miller, J.M.; Andrš, D.; Slaughter, A.E.; Kong, F.; Hansel, J.; Carlsen, R.W.; Icenhour, C.; et al. 2.0—MOOSE: Enabling massively parallel multiphysics simulation. SoftwareX 2022, 20, 101202. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Fernández-Jarne, E.; Serrano-Martínez, M.; Marti, A.; Martinez, J.A.; Martín-Moreno, J.M. Mediterranean diet and reduction in the risk of a first acute myocardial infarction: An operational healthy dietary score. Eur. J. Nutr. 2002, 41, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Bamia, C.; Norat, T.; Overvad, K.; Schmidt, E.B.; Tjønneland, A.; Halkjaer, J.; Clavel-Chapelon, F.; Vercambre, M.N.; Boutron-Ruault, M.C.; et al. Modified Mediterranean diet and survival after myocardial infarction: The EPIC-Elderly study. Eur. J. Epidemiol. 2007, 22, 871–881. [Google Scholar] [CrossRef]
- ADA. ADA Standards of Medical Care in Diabetes. Diabetes Care 2021, 44 (Suppl. 1), 1–232. [Google Scholar]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2000. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 June 2023).
- Aromataris, E.; Munn, Z. (Eds.) JBI Manual for Evidence Synthesis [Internet]. JBI. 2020. Available online: https://wiki.jbi.global/display/MANUAL (accessed on 25 October 2022).
- Hodge, A.M.; Karim, M.N.; Hébert, J.R.; Shivappa, N.; de Courten, B. Association between Diet Quality Indices and Incidence of Type 2 Diabetes in the Melbourne Collaborative Cohort Study. Nutrients 2021, 13, 4162. [Google Scholar] [CrossRef]
- Symons, M.J.; Moore, D.T. Hazard rate ratio and prospective epidemiological studies. J. Clin. Epidemiol. 2002, 55, 893–899. [Google Scholar] [CrossRef]
- Tison, S.E.; Shikany, J.M.; Long, D.L.; Carson, A.P.; Cofield, S.S.; Pearson, K.E.; Howard, G.; Judd, S.E. Differences in the Association of Select Dietary Measures With Risk of Incident Type 2 Diabetes. Diabetes Care 2022, 45, 2602–2610. [Google Scholar] [CrossRef]
- Cabrera de León, A.; Domínguez Coello, S.; Almeida González, D.; Brito Díaz, B.; del Castillo Rodríguez, J.C.; González Hernández, A.; Aguirre-Jaime, A.; Mdel, C.P. Impaired fasting glucose, ancestry and waist-to-height ratio: Main predictors of incident diagnosed diabetes in the Canary Islands: Predictors of diabetes in the Canary Islands. Diabet. Med. 2012, 29, 399–403. [Google Scholar] [CrossRef]
- Bantle, A.E.; Chow, L.S.; Steffen, L.M.; Wang, Q.; Hughes, J.; Durant, N.H.; Ingram, K.H.; Reis, J.P.; Schreiner, P.J. Association of Mediterranean diet and cardiorespiratory fitness with the development of pre-diabetes and diabetes: The Coronary Artery Risk Development in Young Adults (CARDIA) study. BMJ Open Diab. Res. Care 2016, 4, e000229. [Google Scholar] [CrossRef]
- Esfandiar, Z.; Hosseini-Esfahani, F.; Mirmiran, P.; Azizi, F. Diet quality indices and the risk of type 2 diabetes in the Tehran Lipid and Glucose Study. BMJ Open Diab. Res. Care 2022, 10, e002818. [Google Scholar] [CrossRef]
- Schwarzer, G.; Carpenter, J.R.; Rücker, G. Meta-Analysis with R; Use R! Springer International Publishing: Cham, Switzerland, 2015; Available online: http://link.springer.com/10.1007/978-3-319-21416-0 (accessed on 25 October 2022).
- Lau, J.; Ioannidis, J.P.A.; Terrin, N.; Schmid, C.H.; Olkin, I. The case of the misleading funnel plot. BMJ 2006, 333, 597–600. [Google Scholar] [CrossRef]
- McMaster University and Evidence Prime. GRADEpro GDT: GRADEpro Guideline Developmet Tool [Internet]. McMaster University and Evidence Prime. 2022. Available online: gradepro.org (accessed on 10 February 2023).
- Mozaffarian, D.; Marfisi, R.; Levantesi, G.; Silletta, M.G.; Tavazzi, L.; Tognoni, G.; Valagussa, F.; Marchioli, R. Incidence of new-onset diabetes and impaired fasting glucose in patients with recent myocardial infarction and the effect of clinical and lifestyle risk factors. Lancet 2007, 370, 667–675. [Google Scholar] [CrossRef]
- Tobias, D.K.; Hu, F.B.; Chavarro, J.; Rosner, B.; Mozaffarian, D.; Zhang, C. Healthful Dietary Patterns and Type 2 Diabetes Mellitus Risk Among Women With a History of Gestational Diabetes Mellitus. Arch. Intern. Med. 2012, 172, 1566. [Google Scholar] [CrossRef]
- Ahmad, S.; Demler, O.V.; Sun, Q.; Moorthy, M.V.; Li, C.; Lee, I.-M.; Ridker, P.M.; Manson, J.E.; Hu, F.B.; Fall, T.; et al. Association of the Mediterranean Diet With Onset of Diabetes in the Women’s Health Study. JAMA Netw. Open 2020, 3, e2025466. [Google Scholar] [CrossRef]
- O’Connor, L.E.; Hu, E.A.; Steffen, L.M.; Selvin, E.; Rebholz, C.M. Adherence to a Mediterranean-style eating pattern and risk of diabetes in a U.S. prospective cohort study. Nutr. Diabetes 2020, 10, 8. [Google Scholar] [CrossRef]
- The InterAct Consortium. Mediterranean Diet and Type 2 Diabetes Risk in the European Prospective Investigation Into Cancer and Nutrition (EPIC) Study. Diabetes Care 2011, 34, 1913–1918. [Google Scholar] [CrossRef]
- de Koning, L.; Chiuve, S.E.; Fung, T.T.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Diet-Quality Scores and the Risk of Type 2 Diabetes in Men. Diabetes Care 2011, 34, 1150–1156. [Google Scholar] [CrossRef]
- Chen, G.C.; Koh, W.P.; Neelakantan, N.; Yuan, J.M.; Qin, L.Q.; van Dam, R.M. Diet Quality Indices and Risk of Type 2 Diabetes Mellitus. Am. J. Epidemiol. 2018, 187, 2651–2661. [Google Scholar] [CrossRef]
- Galbete, C.; Kröger, J.; Jannasch, F.; Iqbal, K.; Schwingshackl, L.; Schwedhelm, C.; Weikert, C.; Boeing, H.; Schulze, M.B. Nordic diet, Mediterranean diet, and the risk of chronic diseases: The EPIC-Potsdam study. BMC Med. 2018, 16, 99. [Google Scholar] [CrossRef] [PubMed]
- Glenn, A.J.; Li, J.; Lo, K.; Jenkins, D.J.; Boucher, B.A.; Hanley, A.J.; Kendall, C.W.; Shadyab, A.H.; Tinker, L.F.; Chessler, S.D.; et al. The Portfolio Diet and Incident Type 2 Diabetes: Findings From the Women’s Health Initiative Prospective Cohort Study. Diabetes Care 2023, 46, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, S.; Harmon, B.E.; Boushey, C.J.; Morimoto, Y.; Wilkens, L.R.; le Marchand, L.; Kröger, J.; Schulze, M.B.; Kolonel, L.N.; Maskarinec, G. A priori-defined diet quality indexes and risk of type 2 diabetes: The Multiethnic Cohort. Diabetologia 2015, 58, 98–112. [Google Scholar] [CrossRef] [PubMed]
- Koloverou, E.; Panagiotakos, D.B.; Pitsavos, C.; Chrysohoou, C.; Georgousopoulou, E.N.; Grekas, A.; Christou, A.; Chatzigeorgiou, M.; Skoumas, I.; Tousoulis, D.; et al. Adherence to Mediterranean diet and 10-year incidence (2002–2012) of diabetes: Correlations with inflammatory and oxidative stress biomarkers in the ATTICA cohort study: Mediterranean Diet and Diabetes. Diabetes Metab. Res. Rev. 2016, 32, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Ortega, E.; Franch, J.; Castell, C.; Goday, A.; Ribas-Barba, L.; Soriguer, F.; Vendrell, J.; Casamitjana, R.; Bosch-Comas, A.; Bordiú, E.; et al. Mediterranean Diet Adherence in Individuals with Prediabetes and Unknown Diabetes: The Di@bet.es Study. Ann. Nutr. Metab. 2013, 62, 339–346. [Google Scholar] [CrossRef]
- Ramezan, M.; Asghari, G.; Mirmiran, P.; Tahmasebinejad, Z.; Azizi, F. Mediterranean dietary patterns and risk of type 2 diabetes in the Islamic Republic of Iran. East. Mediterr. Health J. 2019, 25, 896–904. [Google Scholar] [CrossRef]
- Hlaing-Hlaing, H.; Dolja-Gore, X.; Tavener, M.; James, E.L.; Hodge, A.M.; Hure, A.J. Diet Quality and Incident Non-Communicable Disease in the 1946–1951 Cohort of the Australian Longitudinal Study on Women’s Health. IJERPH 2021, 18, 11375. [Google Scholar] [CrossRef]
- Iestra, J.; Knoops, K.; Kromhout, D.; de Groot, L.; Grobbee, D.; van Staveren, W. Lifestyle, Mediterranean diet and survival in European post-myocardial infarction patients. Eur. J. Cardiovasc. Prev. Rehabil. 2006, 13, 894–900. [Google Scholar] [CrossRef]
- Neuenschwander, M.; Ballon, A.; Weber, K.S.; Norat, T.; Aune, D.; Schwingshackl, L.; Schlesinger, S. Role of diet in type 2 diabetes incidence: Umbrella review of meta-analyses of prospective observational studies. BMJ 2019, 366, l2368. [Google Scholar] [CrossRef]
- Gomez-Delgado, F.; Alcala-Diaz, J.F.; Garcia-Rios, A.; Delgado-Lista, J.; Ortiz-Morales, A.; Rangel-Zuñiga, O.; Tinahones, F.J.; Gonzalez-Guardia, L.; Malagon, M.M.; Bellido-Muñoz, E.; et al. Polymorphism at the TNF -alpha gene interacts with M editerranean diet to influence triglyceride metabolism and inflammation status in metabolic syndrome patients: F rom the CORDIOPREV clinical trial. Mol. Nutr. Food Res. 2014, 58, 1519–1527. [Google Scholar] [CrossRef]
- Hidalgo-Moyano, C.; Rangel-Zuñiga, O.A.; Gomez-Delgado, F.; Alcala-Diaz, J.F.; Rodriguez-Cantalejo, F.; Yubero-Serrano, E.M.; Torres-Pena, J.D.; Arrenas-de-Larriva, A.P.; Camargo, A.; Perez-Martinez, P.; et al. Diet and SIRT1 Genotype Interact to Modulate Aging-Related Processes in Patients with Coronary Heart Disease: From the CORDIOPREV Study. Nutrients 2022, 14, 3789. [Google Scholar] [CrossRef]
- Esposito, S.; Sparaco, M.; Maniscalco, G.T.; Signoriello, E.; Lanzillo, R.; Russo, C.; Carmisciano, L.; Cepparulo, S.; Lavorgna, L.; Gallo, A.; et al. Lifestyle and Mediterranean diet adherence in a cohort of Southern Italian patients with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2021, 47, 102636. [Google Scholar] [CrossRef]
- Urpi-Sarda, M.; Casas, R.; Sacanella, E.; Corella, D.; Andrés-Lacueva, C.; Llorach, R.; Garrabou, G.; Cardellach, F.; Sala-Vila, A.; Ros, E.; et al. The 3-Year Effect of the Mediterranean Diet Intervention on Inflammatory Biomarkers Related to Cardiovascular Disease. Biomedicines 2021, 9, 862. [Google Scholar] [CrossRef]
- Wang, D.D.; Nguyen, L.H.; Li, Y.; Yan, Y.; Ma, W.; Rinott, E.; Ivey, K.L.; Shai, I.; Willett, W.C.; Hu, F.B.; et al. The gut microbiome modulates the protective association between a Mediterranean diet and cardiometabolic disease risk. Nat. Med. 2021, 27, 333–343. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study (Author, Year) | Population | Presence of Diabetes in Study Start | Age Years (Range) | N Gender (M%/W%) | BMI Study Population | Effect Size | Score for MD | Low Adherence to MD (L) | High Adherence to MD (H) (HR (95%CI)) | Person Years | Number of Cases | Incidence Rate Per 1000 Person Years |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abiemo et al., 2013 [1] | Multi-Ethnic Study of Atherosclerosis MESA | * | 62 ± 10.3 45–84 | 5390 46.5/53.5 | 27.88 ± 5 | HR/incidence rate | 127 item FFQ Alternate med diet | 1 | 1.09 (0.80–1.49) | L: 4936 H: 5013 | L: 99 H: 89 | L: 20.1 H: 17.8 |
| Ahmad et al., 2020 [2] | Women’s Health Study | * | 52.9 ± 9.9 | 25,317 W | HR | Med diet score | 1 | 0.70 (0.62–0.79) | ||||
| Andre et al., 2020 [3] | UK Biobank | * | 56.5 (40–71) | 21,585 48/52 | Diab: 30.7 ± 5.5 Non diab: 26.4 ± 4.3 | HR /OR | Med diet score by Sofi et al. | 1 | 0.90 (0.84–0.96) A | |||
| Bantle et al., 2016 [4] | CARDIA | Excluded diabetes and prediabetes | (43–55) | 3358 1445/1913 | 24.4 kg/m2 (at baseline) | OR | AmMedDiet | 1 | 0.87 (0.72–1.04) (OR) | 393 (total) | ||
| Brunner et al., 2008 [5] | Whitehall II | Healthy | 50 (35–69) | 7731 69.7/30.3 (N: 5391) | ~25 | HR | 127 item FFQ | 1 | 0.94 (0.68–1.30) | L: 167 H: 65 | ||
| Cabrera de Leon et al., 2011 [6] | CDC de Canarias | Excluded diabetes in baseline | 18–75 42 ± 16.3 y | 5521 42.2% M/57.8% W | NA | HR | Med diet adh by Trichopoulou | 1.1 (0.7–1.7) | 21,106 | 7.5 | ||
| Chen et al., 2018 [7] | Singapore Chinese Health Study (SCHS) | Free from Diabetes | 45–74 | 45,411 total L: 8916 H: 9358 | 23 | HR | aMed | 1 | 0.84 (0.77–0.92) | L: 91,711 H: 99,269 | L: 1097 H: 1008 | |
| DeKoning et al., 2011 [8] | Health Professionals Follow Up (HPFS) | Without DM | 41,615 M | ~25 | HR | aMed | 1 | 0.75 (0.66–0.86) | L: 151,824 H: 141,248 | L: 705 H: 405 | ||
| Esfandiar et al., 2022 [9] | Tehran Glucose and Lipids (TGLS) | Excluded diabetes from analysis | 41.2 ± 14.1 | 3265/4003 | 27.1 ± 4.5 | HR | Med diet adh by Trichopoulou | 1 | 1.06 (0.87–1.30) | |||
| Galbete et al., 2018 [10] | EPIC Potsdam | Excluded diabetes | 49.8 ± 8.9 | 38.9% M | 26.1 ± 4.2 | HR | Med diet adh by Trichopoulou | 1 | 0,84 (0,73–0,97) | L: 73,939 H: 70,578 | L: 445 H: 353 | |
| Glenn et al., 2023 [11] | WHI (Women’s Health Initiative) | Free from diabetes | 63 ± 7 | 56,717 W | L: 28.7 ± 6.1 H: 26.7 ± 5.4 | HR | aMed | 1 | 0.88 (0.83–0.94) | L: 406,039 H: 498,638 | L: 2957 H: 2411 | |
| Hlaing Hlaing et al., 2021 [12] | Australia Longitudinal Study on Women’s Health (ALSWH) | Free from Non communicable diseases | L: 52.4 ± 1.5 H: 52.6 ± 1.4 | L: 1769 H: 642 W | OR | MDS | 1 | 0.76 (0.48–1.21) | ||||
| Hodge et al., 2021 [13] | Melbourne Collaborative Cohort | Excluded diabetes | 55.2 ± 8.7 | 40.3% M 59.7% W | 26.8 ± 4 | IRR | Med Diet Adh by Trichopoulou | 1 | IRR 0.98 (0.85–1.13) | |||
| InterAct Consortium (Romaguera et al.,2011) [14] | InterAct EPIC | * | 52.9 ± 8.9 (25–75) | 15,798 37.8/62.2 | 26.6 ±3.6 25.7 ± 4.5 | HR | rMed | 1 | 0.88 (0.79–0.98) | L: 3879/3.902 H: 4380/7.392 | ||
| Jacobs et al., 2014 [15] | Hawaii—MEC | Excluded diabetes | Men L: 56 (16) H: 61 (17) Women: L: 54 (16) H: 61 (16) | M: 12,557 W: 21,683 | Men: L: 25.3 (4.7) H: 24.6 (4.3) Women L: 23.7 (5.7) H: 23.2 (5.3) | HR | aMed | 1 | 0.89 (0.80–0.99) M 0.92 (0.84–1.02) F | Men L: 7403 H: 5154 Women L: 8902 H: 12,781 | Men L: 1090 H: 659 Women L: 1018 H: 1433 | |
| Koloverou et al., 2015 [17] | ATTICA | * | (18–89) | 3043 49.8/50.2 | L: 29 ± 4.2 H: 22 ± 2.5 | Cases /OR/10 y incidence | Med diet by Panagiotakos et al. | 1 | 0.38 (0.16–0.88) (RR) | L: 83 H: 8 | ||
| Martinez-Gonzalez et al., 2008 [18] | SUN Navarra | Without DM | 37.8 (20–90) | 13,380 39.7/60.3 | 23.4 ± 3.4 | Incidence/RR | 136 FFQ-Med diet by Trichopoulou | 0.17 (0.04–0.75) (incidence rate ratio) | ||||
| Mozaffarian et al., 2007 [19] | GISSI Prevezione | * | 59 ± 11 (20–90) | 8291 87.03/12.97 | 26.3 + 3.4 | HR | FFQ | 1 | 0.65 (0.49–0.85) | L: 1423 H: 6289 | L: 83 H: 179 | L: 58 H: 28 |
| oConnor et al., 2020 [20] | Atherosclerosis risk in Communities Study ARIC | * | 54 ± 5 (45–65) | 11,991 43.7/56.3 | 27.3 ± 5.2 | HR | aMed | 1 | 0.94 (0.82–1.07) | L: 796 H: 376 | L: 1.8 H: 1.6 (per 100 person years) | |
| Ortega et al., 2013 [21] | The Di@bet.es Study | Differentiated free from diabetes with diabetes | 45 | 5076 2177 (43%) M 2899 (57%) W | L: 28.1 ± 5.6 H: 28.1 ± 4.8 | OR | Med diet by Panagiotakos et al. | 1 | 0.73 (0.69–0.98) | |||
| Ramezan et al., 2019 [22] | Tehran Glucose and Lipid Study b | Free of diabetes in previous reports | L: 48.1 ± 12.9 H: 52.8 ± 12.7 | L: 45.6% men H: 41.2% men | L: 29 ± 5.7 H: 29.1 ± 5.2 | OR | Med diet adh by Trichopoulou | 1 | 0.93 (0.44–1.96) | |||
| Rossi et al., 2013 [23] | EPIC | * | ~50 (20–80) baseline (39–63) $ | 22,295 | ~27–28 | HR | MDS by FFQ | 1 | 0.88 (0.78–0.99) | L: 73.997 H: 59.542 | L: 716 H: 582 | |
| Tison et al., 2022 [24] | REasons for Geographic and Racial Differences in Stroke (REGARDS) study | Without diabetes | 63.2 ± 8.5 | Men: 3834 (43.8%) Women: 4916 (56.2%) | NA | RR | Adjusted for dementia(Block98 FFQ) Med diet by Trichopoulou | 1 | 1.15 (0.93–1.41) | L: 13.6 H: 10.3 | ||
| Tobias et al., 2012 [25] | Nurses Health Study II | History of GDM | 37.8 ± 4.8 24–44 | 4413 W | 25–28 | HR | aMed | 1 | 0.60 (0.44–0.82) | L: 12.198 H: 13.423 | L: 137 H: 106 |
| Number of Studies (N) | HR (95%CI) | Prediction Interval | τ2 (95%CI) | I2 (%), (95%CI), Pheterogeneity | Pbetween | |
|---|---|---|---|---|---|---|
| All Studies | 14 | 0.89 (0.83–0.95) | 0.70–1.13 | 0.0118 (0.00–0.08) | 47.4%, (10.3–69.2), 0.01 | NA |
| Sex | 0.57 | |||||
| Male | 3 | 0.85 (0.71–1.01) | 0.13–5.52 | 0.0139 (0.00–1.49) | 62.6%, (0.0–89.3) 0.07 | |
| Female | 5 | 0.89 (0.85–0.94) | 0.83–0.97 | 0 (0.00–0.12) | 0%, (0.0–79.2) 0.6 | |
| Continents | 0.57 | |||||
| USA | 9 | 0.89 (0.82–0.96) | 0.70–1.13 | 0.0085 (0.00–0.06) | 51.5%, (0.0–77.3) 0.04 | |
| Europe | 7 | 0.83 (0.67–1.03) | 0.43–1.63 | 0.0568 (0.00–1.53) | 44%, (0.0–76.4) 0.10 | |
| Asia | 2 | 0.93 (0.74–1.16) | NA | 0.0208 | 76.8%, (0.0–94.7) 0.04 | |
| Australia | 1 | 0.98 (0.85–1.13) | NA | NA | NA | |
| Follow-up (years) | 0.89 | |||||
| <10 | 6 | 0.86 (0.60–1.24) | 0.25–2.94 | 0.1617 (0.01–2.75) | 67.6%, (23.2–86.4) <0.01 | |
| ≥10 | 13 | 0.88 (0.84–0.92) | 0.77–1.01 | 0.0033 (0.00–0.02) | 35.2%, (0.00–66.5) 0.1 | |
| BMI status (kg/m2) | 0.47 | |||||
| BMI < 25 | 3 | 0.94 (0.76–1.15) | 0.15–5.84 | 0.0097 (0.00–1.10) | 34%, (0.0–78.5) 0.22 | |
| BMI ≥ 25 | 3 | 0.86 (0.80–0.93) | 0.73–1.02 | 0 (0.00–0.00) | 0%, (0.0–84.7) 0.97 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotzakioulafi, E.; Bakaloudi, D.R.; Chrysoula, L.; Theodoridis, X.; Antza, C.; Tirodimos, I.; Chourdakis, M. High Versus Low Adherence to the Mediterranean Diet for Prevention of Diabetes Mellitus Type 2: A Systematic Review and Meta-Analysis. Metabolites 2023, 13, 779. https://doi.org/10.3390/metabo13070779
Kotzakioulafi E, Bakaloudi DR, Chrysoula L, Theodoridis X, Antza C, Tirodimos I, Chourdakis M. High Versus Low Adherence to the Mediterranean Diet for Prevention of Diabetes Mellitus Type 2: A Systematic Review and Meta-Analysis. Metabolites. 2023; 13(7):779. https://doi.org/10.3390/metabo13070779
Chicago/Turabian StyleKotzakioulafi, Evangelia, Dimitra Rafailia Bakaloudi, Lydia Chrysoula, Xenophon Theodoridis, Christina Antza, Ilias Tirodimos, and Michail Chourdakis. 2023. "High Versus Low Adherence to the Mediterranean Diet for Prevention of Diabetes Mellitus Type 2: A Systematic Review and Meta-Analysis" Metabolites 13, no. 7: 779. https://doi.org/10.3390/metabo13070779
APA StyleKotzakioulafi, E., Bakaloudi, D. R., Chrysoula, L., Theodoridis, X., Antza, C., Tirodimos, I., & Chourdakis, M. (2023). High Versus Low Adherence to the Mediterranean Diet for Prevention of Diabetes Mellitus Type 2: A Systematic Review and Meta-Analysis. Metabolites, 13(7), 779. https://doi.org/10.3390/metabo13070779