

Maternal Metabolites Indicative of Mental Health Status during Pregnancy


 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Mental Health Screening
2.2. Proton Nuclear Magnetic Resonance Spectroscopy (1H-NMR)
2.3. Inductively Coupled Plasma-Mass Spectrometry (ICP-MS)
2.4. Statistical Analysis
3. Results
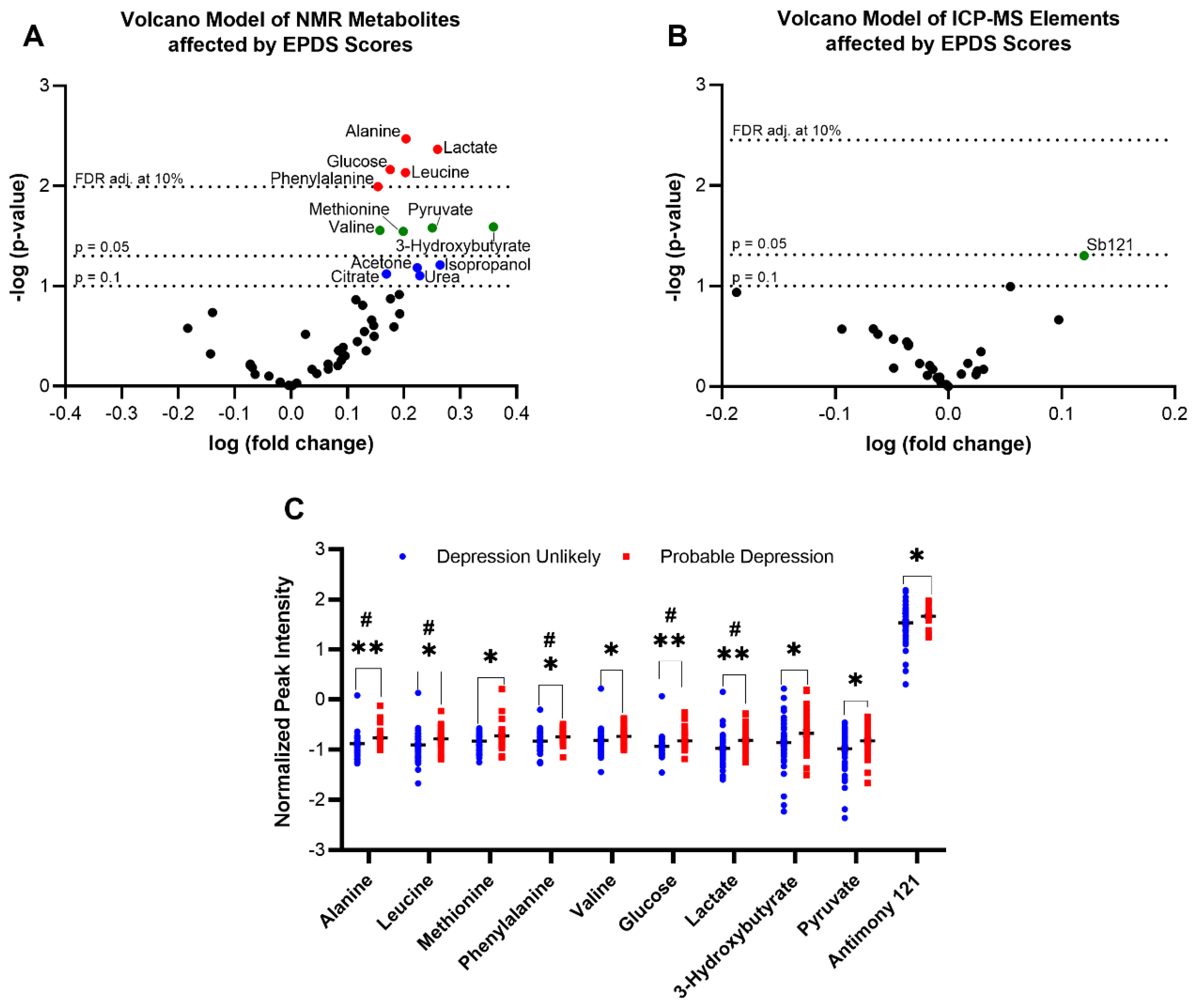
3.1. Discriminating Metabolites Associated with Depression
3.2. Discriminating Metabolites Associated with Anxiety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malhotra, R.; Mudgal, R.; Dharmarha, S.; Mehta, S.; Bhola, S.M. How happy are pregnant women?: A socio-demographic analysis. Clin. Epidemiol. Glob. Heal. 2015, 3, 117–124. [Google Scholar] [CrossRef]
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect. Disord. 2016, 191, 62–77. [Google Scholar] [CrossRef] [PubMed]
- Kingston, D.; Heaman, M.; Fell, D.; Dzakpasu, S.; Chalmers, B. Factors associated with perceived stress and stressful life events in pregnant women: Findings from the canadian maternity experiences survey. Matern. Child Health J. 2012, 16, 158–168. [Google Scholar] [CrossRef]
- Van den Bergh, B.R.H.; van den Heuvel, M.I.; Lahti, M.; Braeken, M.; de Rooij, S.R.; Entringer, S.; Hoyer, D.; Roseboom, T.; Räikkönen, K.; King, S.; et al. Prenatal developmental origins of behavior and mental health: The influence of maternal stress in pregnancy. Neurosci. Biobehav. Rev. 2020, 117, 26–64. [Google Scholar] [CrossRef] [PubMed]
- Federenko, I.S.; Wadhwa, P.D. Women’s mental health during pregnancy influences fetal and infant developmental and health outcomes. CNS Spectr. 2004, 9, 198–206. [Google Scholar] [CrossRef]
- Orr, S.T.; James, S.A.; Prince, C.B. Maternal prenatal depressive symptoms and spontaneous preterm births among African-American women in Baltimore, Maryland. Am. J. Epidemiol. 2002, 156, 797–802. [Google Scholar] [CrossRef] [PubMed]
- Dayan, J.; Creveuil, C.; Marks, M.N.; Conroy, S.; Herlicoviez, M.; Dreyfus, M.; Tordjman, S. Prenatal depression, prenatal anxiety, and spontaneous preterm birth: A prospective cohort study among women with early and regular care. Psychosom. Med. 2006, 68, 938–946. [Google Scholar] [CrossRef]
- Staneva, A.; Bogossian, F.; Pritchard, M.; Wittkowski, A. The effects of maternal depression, anxiety, and perceived stress during pregnancy on preterm birth: A systematic review. Women and Birth 2015, 28, 179–193. [Google Scholar] [CrossRef]
- Kelly, R.H.; Russo, J.; Holt, V.L.; Danielsen, B.H.; Zatzick, D.F.; Walker, E.; Katon, W. Psychiatric and substance use disorders as risk factors for low birth weight and preterm delivery. Obstet. Gynecol. 2002, 100, 297–304. [Google Scholar] [CrossRef]
- Das, A.; Gordon-Ocejo, G.; Kumar, M.; Kumar, N.; Needlman, R. Association of the previous history of maternal depression with post-partum depression, anxiety, and stress in the neonatal intensive care unit. J. Matern. Fetal. Neonatal Med. 2021, 34, 1741–1746. [Google Scholar] [CrossRef]
- Slomian, J.; Honvo, G.; Emonts, P.; Reginster, J.Y.; Bruyère, O. Consequences of maternal postpartum depression: A systematic review of maternal and infant outcomes. Women’s Heal. 2019, 15, 1745506519844044. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.M.; Lam, S.K.; Sze Mun Lau, S.M.; Chong, C.S.Y.; Chui, H.W.; Fong, D.Y.T. Prevalence, course, and risk factors for antenatal anxiety and depression. Obstet. Gynecol. 2007, 110, 1102–1112. [Google Scholar] [CrossRef] [PubMed]
- Marchesi, C.; Bertoni, S.; Maggini, C. Major and minor depression in pregnancy. Obstet. Gynecol. 2009, 113, 1292–1298. [Google Scholar] [CrossRef]
- Newson, J.J.; Hunter, D.; Thiagarajan, T.C. The Heterogeneity of Mental Health Assessment. Front. Psychiatry 2020, 11, 76. [Google Scholar] [CrossRef]
- Wisco, B.E.; Miller, M.W.; Wolf, E.J.; Kilpatrick, D.; Resnick, H.S.; Badour, C.L.; Marx, B.P.; Keane, T.M.; Rosen, R.C.; Friedman, M.J. The impact of proposed changes to ICD-11 on estimates of PTSD prevalence and comorbidity. Psychiatry Res. 2016, 240, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Pu, J.; Liu, Y.; Zhang, H.; Tian, L.; Gui, S.; Yu, Y.; Chen, X.; Chen, Y.; Yang, L.; Ran, Y.; et al. An integrated meta-analysis of peripheral blood metabolites and biological functions in major depressive disorder. Mol. Psychiatry 2021, 26, 4265–4276. [Google Scholar] [CrossRef]
- Guijas, C.; Montenegro-Burke, J.R.; Warth, B.; Spilker, M.E.; Siuzdak, G. Metabolomics activity screening for identifying metabolites that modulate phenotype. Nat. Biotechnol. 2018, 36, 316–320. [Google Scholar] [CrossRef]
- Johnson, C.H.; Ivanisevic, J.; Siuzdak, G. Metabolomics: Beyond biomarkers and towards mechanisms. Nat. Rev. Mol. Cell Biol. 2016, 17, 451–459. [Google Scholar] [CrossRef]
- Bot, M.; Milaneschi, Y.; Al-Shehri, T.; Amin, N.; Garmaeva, S.; Onderwater, G.L.J.; Pool, R.; Thesing, C.S.; Vijfhuizen, L.S.; Vogelzangs, N.; et al. Metabolomics Profile in Depression: A Pooled Analysis of 230 Metabolic Markers in 5283 Cases with Depression and 10,145 Controls. Biol. Psychiatry 2020, 87, 409–418. [Google Scholar] [CrossRef]
- Humer, E.; Pieh, C.; Probst, T. Metabolomic biomarkers in anxiety disorders. Int. J. Mol. Sci. 2020, 21, 4784. [Google Scholar] [CrossRef]
- Tough, S.C.; McDonald, S.W.; Collisson, B.A.; Graham, S.A.; Kehler, H.; Kingston, D.; Benzies, K. Cohort Profile: The All Our Babies pregnancy cohort (AOB). Int. J. Epidemiol. 2017, 46, 1389–1390k. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of Postnatal Depression: Development of the 10-item Edinburgh Postnatal Depression scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E. STAI, Manual fot the State-Trait Anxiety Inventory (Self Evaluation Questionnaire). Consult. Psychol. Press. Inc. 1970. [Google Scholar]
- Gracie, S.K.; Lyon, A.W.; Kehler, H.L.; Pennell, C.E.; Dolan, S.M.; McNeil, D.A.; Siever, J.E.; McDonald, S.W.; Bocking, A.D.; Lye, S.J.; et al. All Our Babies Cohort Study: Recruitment of a cohort to predict women at risk of preterm birth through the examination of gene expression profiles and the environment. BMC Pregnancy Childbirth 2010, 10, 1–9. [Google Scholar] [CrossRef]
- Brito, C.N.d.O.; Alves, S.V.; Ludermir, A.B.; de Araújo, T.V.B. Postpartum depression among women with unintended pregnancy. Rev. Saude Publica 2015, 49, 33. [Google Scholar] [CrossRef]
- Tomfohr-Madsen, L.M.; Bayrampour, H.; Tough, S. Maternal history of childhood abuse and risk of asthma and allergy in 2-year-old children. Psychosom. Med. 2016, 78, 1031–1042. [Google Scholar] [CrossRef]
- Marteau, T.M.; Bekker, H. The development of a six-item short-form of the state scale of the Spielberger State-Trait Anxiety Inventory (STAI). Br. J. Clin. Psychol. 1992, 31, 301–306. [Google Scholar] [CrossRef]
- Levis, B.; Negeri, Z.; Sun, Y.; Benedetti, A.; Thombs, B.D. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: Systematic review and meta-analysis of individual participant data. BMJ 2020, 371. [Google Scholar] [CrossRef]
- Kleiman, K.F. Edinburgh Postnatal Depression Scale (EPDS). Ther. Postpartum Woman 2021, 302–303. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24. [Google Scholar] [CrossRef]
- Shearer, J.; Duggan, G.; Weljie, A.; Hittel, D.S.S.; Wasserman, D.H.H.; Vogel, H.J.J. Metabolomic profiling of dietary-induced insulin resistance in the high fat-fed C57BL/6J mouse. Diabetes Obes. Metab. 2008, 10, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Duggan, G.E.; Hittel, D.S.; Sensen, C.W.; Weljie, A.M.; Vogel, H.J.; Shearer, J. Metabolomic response to exercise training in lean and diet-induced obese mice. J. Appl. Physiol. 2011, 110. [Google Scholar] [CrossRef] [PubMed]
- Klein, M.S.; Newell, C.; Bomhof, M.R.; Reimer, R.A.; Hittel, D.S.; Rho, J.M.; Vogel, H.J.; Shearer, J. Metabolomic Modeling to Monitor Host Responsiveness to Gut Microbiota Manipulation in the BTBRT+tf/j Mouse. J. Proteome Res. 2016, 15, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Lipfert, M.; Rout, M.K.; Berjanskii, M.; Wishart, D.S. Automated Tools for the Analysis of 1D-NMR and 2D-NMR Spectra. Methods Mol. Biol. 2019, 2037, 429–449. [Google Scholar] [CrossRef] [PubMed]
- Mayengbam, S.; Mickiewicz, B.; Trottier, S.K.; Mu, C.; Wright, D.C.; Reimer, R.A.; Vogel, H.J.; Shearer, J. Distinct Gut Microbiota and Serum Metabolites in Response to Weight Loss Induced by Either Dairy or Exercise in a Rodent Model of Obesity. J. Proteome Res. 2019, 18, 3867–3875. [Google Scholar] [CrossRef]
- Lee, J.Y.; Styczynski, M.P. NS-kNN: A modified k-nearest neighbors approach for imputing metabolomics data. Metabolomics 2018, 14, 1–12. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Chong, J.; Soufan, O.; Li, C.; Caraus, I.; Li, S.; Bourque, G.; Wishart, D.S.; Xia, J. MetaboAnalyst 4.0: Towards more transparent and integrative metabolomics analysis. Nucleic Acids Res. 2018, 46, W486–W494. [Google Scholar] [CrossRef]
- Han, S.Y.; Brewis, A.A.; Wutich, A. Body image mediates the depressive effects of weight gain in new mothers, particularly for women already obese: Evidence from the Norwegian Mother and Child Cohort Study. BMC Public Health 2016, 16, 1–10. [Google Scholar] [CrossRef]
- Pavlik, L.B.; Rosculet, K. Maternal Obesity and Perinatal Depression: An Updated Literature Review. Cureus 2020, 12. [Google Scholar] [CrossRef]
- Muraca, G.M.; Joseph, K.S. The Association Between Maternal Age and Depression. J. Obstet. Gynaecol. Canada 2014, 36, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Benny, C.; Yamamoto, S.; McDonald, S.; Chari, R.; Pabayo, R. Modelling Maternal Depression: An Agent-Based Model to Examine the Complex Relationship between Relative Income and Depression. Int. J. Environ. Res. Public Health 2022, 19, 4208. [Google Scholar] [CrossRef] [PubMed]
- Dunkel Schetter, C.; Tanner, L. Anxiety, depression and stress in pregnancy: Implications for mothers, children, research, and practice. Curr. Opin. Psychiatry 2012, 25, 141. [Google Scholar] [CrossRef] [PubMed]
- Pereira, B.; Figueiredo, B.; Pinto, T.M.; Míguez, M.C. Effects of Tobacco Consumption and Anxiety or Depression during Pregnancy on Maternal and Neonatal Health. Int. J. Environ. Res. Public Health 2020, 17, 8138. [Google Scholar] [CrossRef]
- Gu, X.; Ke, S.; Wang, Q.; Zhuang, T.; Xia, C.; Xu, Y.; Yang, L.; Zhou, M. Energy metabolism in major depressive disorder: Recent advances from omics technologies and imaging. Biomed. Pharmacother. 2021, 141, 111869. [Google Scholar] [CrossRef]
- Sharma, S.; Akundi, R.S. Mitochondria: A Connecting Link in the Major Depressive Disorder Jigsaw. Curr. Neuropharmacol. 2018, 17, 550–562. [Google Scholar] [CrossRef]
- Gardner, A.; Boles, R.G. Beyond the serotonin hypothesis: Mitochondria, inflammation and neurodegeneration in major depression and affective spectrum disorders. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2011, 35, 730–743. [Google Scholar] [CrossRef]
- Østergaard, L.; Jørgensen, M.B.; Knudsen, G.M. Low on energy? An energy supply-demand perspective on stress and depression. Neurosci. Biobehav. Rev. 2018, 94, 248–270. [Google Scholar] [CrossRef]
- Achanta, L.B.; Rae, C.D. β-Hydroxybutyrate in the Brain: One Molecule, Multiple Mechanisms. Neurochem. Res. 2017, 42, 35–49. [Google Scholar] [CrossRef]
- Krivosova, M.; Gondas, E.; Murin, R.; Dohal, M.; Ondrejka, I.; Tonhajzerova, I.; Hutka, P.; Ferencova, N.; Visnovcova, Z.; Hrtanek, I.; et al. The Plasma Levels of 3-Hydroxybutyrate, Dityrosine, and Other Markers of Oxidative Stress and Energy Metabolism in Major Depressive Disorder. Diagnostics 2022, 12, 813. [Google Scholar] [CrossRef]
- Saito, N.; Itoga, M.; Minakawa, S.; Kayaba, H. Serum 3-hydroxybutyrate in patients with psychogenic somatoform symptoms may be a predictor of the effectiveness of sertraline and venlafaxine. Int. J. Gen. Med. 2021, 14, 1785–1795. [Google Scholar] [CrossRef] [PubMed]
- Setoyama, D.; Kato, T.A.; Hashimoto, R.; Kunugi, H.; Hattori, K.; Hayakawa, K.; Sato-Kasai, M.; Shimokawa, N.; Kaneko, S.; Yoshida, S.; et al. Plasma metabolites predict severity of depression and suicidal ideation in psychiatric patients-a multicenter pilot analysis. PLoS One 2016, 11, e0165267. [Google Scholar] [CrossRef]
- Leonard, B.E.; Wegener, G. Inflammation, insulin resistance and neuroprogression in depression. Acta Neuropsychiatr. 2019, 32, 1–9. [Google Scholar] [CrossRef]
- Kobayashi, H.; Amrein, K.; Lasky-Su, J.A.; Christopher, K.B. Procalcitonin metabolomics in the critically ill reveal relationships between inflammation intensity and energy utilization pathways. Sci. Rep. 2021, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Holmes, M.V.; Smith, G.D.; Ala-Korpela, M. Genetic support for a causal role of insulin resistance on circulating branched-chain amino acids and inflammation. Diabetes Care 2017, 40, 1779–1786. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.H.; Raison, C.L. The role of inflammation in depression: From evolutionary imperative to modern treatment target. Nat. Rev. Immunol. 2016, 16, 22–34. [Google Scholar] [CrossRef]
- Osborne, L.M.; Monk, C. Perinatal depression-The fourth inflammatory morbidity of pregnancy?. Theory and literature review. Psychoneuroendocrinology 2013, 38, 1929–1952. [Google Scholar] [CrossRef]
- Lustman, P.J.; Anderson, R.J.; Freedland, K.E.; De Groot, M.; Carney, R.M.; Clouse, R.E. Depression and poor glycemic control: A meta-analytic review of the literature. Diabetes Care 2000, 23, 934–942. [Google Scholar] [CrossRef]
- Belmaker, R.H.; Agam, G. Major Depressive Disorder. N. Engl. J. Med. 2008, 1, 55–68. [Google Scholar] [CrossRef]
- Huang, T.; Rifas-Shiman, S.L.; Ertel, K.A.; Rich-Edwards, J.; Kleinman, K.; Gillman, M.W.; Oken, E.; James-Todd, T. Pregnancy hyperglycaemia and risk of prenatal and postpartum depressive symptoms. Paediatr. Perinat. Epidemiol. 2015, 29, 281–289. [Google Scholar] [CrossRef]
- Mocking, R.J.T.; Naviaux, J.C.; Li, K.; Wang, L.; Monk, J.M.; Bright, A.T.; Figueroa, C.A.; Schene, A.H.; Ruhé, H.G.; Assies, J.; et al. Metabolic features of recurrent major depressive disorder in remission, and the risk of future recurrence. Transl. Psychiatry 2021, 11, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Pfost, K.S.; Stevens, M.J.; Lum, C.U. The relationship of demographic variables, antepartum depression, and stress to postpartum depression. J. Clin. Psychol. 1990, 46, 588–592. [Google Scholar] [CrossRef] [PubMed]
- Dachew, B.A.; Ayano, G.; Betts, K.; Alati, R. The impact of pre-pregnancy BMI on maternal depressive and anxiety symptoms during pregnancy and the postpartum period: A systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Meltzer-Brody, S.; Boschloo, L.; Jones, I.; Sullivan, P.F.; Penninx, B.W. The EPDS-Lifetime: Assessment of lifetime prevalence and risk factors for perinatal depression in a large cohort of depressed women. Arch. Womens. Ment. Health 2013, 16, 465–473. [Google Scholar] [CrossRef]
- Kiewa, J.; Meltzer-Brody, S.; Milgrom, J.; Bennett, E.; MacKle, T.; Guintivano, J.; Hickie, I.B.; Colodro-Conde, L.; Medland, S.E.; Martin, N.; et al. Lifetime prevalence and correlates of perinatal depression in a case-cohort study of depression. BMJ Open 2022, 12, e059300. [Google Scholar] [CrossRef] [PubMed]
- Mitro, S.D.; Larrabure-Torrealva, G.T.; Sanchez, S.E.; Molsberry, S.A.; Williams, M.A.; Clish, C.; Gelaye, B. Metabolomic markers of antepartum depression and suicidal ideation. J. Affect. Disord. 2020, 262, 422–428. [Google Scholar] [CrossRef]
- Swardfager, W.; Herrmann, N.; Mazereeuw, G.; Goldberger, K.; Harimoto, T.; Lanctôt, K.L. Zinc in depression: A meta-analysis. Biol. Psychiatry 2013, 74, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Młyniec, K.; Davies, C.L.; Budziszewska, B.; Opoka, W.; Reczyński, W.; Sowa-Kućma, M.; Doboszewska, U.; Pilc, A.; Nowak, G. Time course of zinc deprivation-induced alterations of mice behavior in the forced swim test. Pharmacol. Reports 2012, 64, 567–575. [Google Scholar] [CrossRef]
- Młyniec, K.; Nowak, G. Zinc deficiency induces behavioral alterations in the tail suspension test in mice. Effect of antidepressants. Pharmacol. Reports 2012, 64, 249–255. [Google Scholar] [CrossRef]
- Cope, E.C.; Levenson, C.W. Role of zinc in the development and treatment of mood disorders. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 685–689. [Google Scholar] [CrossRef]
- Szewczyk, B.; Kubera, M.; Nowak, G. The role of zinc in neurodegenerative inflammatory pathways in depression. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2011, 35, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Roomruangwong, C.; Kanchanatawan, B.; Sirivichayakul, S.; Mahieu, B.; Nowak, G.; Maes, M. Lower Serum Zinc and Higher CRP Strongly Predict Prenatal Depression and Physio-somatic Symptoms, Which All Together Predict Postnatal Depressive Symptoms. Mol. Neurobiol. 2017, 54, 1500–1512. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, W.G. Recent Observations on Mineral Interrelationships. Fed. Proc. 1964, 23, 1068–1076. [Google Scholar] [PubMed]
- Spencer, H.; Rubio, N.; Kramer, L.; Norris, C.; Osis, D. Effect of zinc supplements on the intestinal absorption of calcium. J. Am. Coll. Nutr. 1987, 6, 47–51. [Google Scholar] [CrossRef]
- Stephenson, N.L.; Hornaday, K.K.; Doktorchik, C.T.A.; Lyon, A.W.; Tough, S.C.; Slater, D.M. Quality assessment of RNA in long-term storage: The All Our Families biorepository. PLoS One 2020, 15, e0242404. [Google Scholar] [CrossRef]
- McDonald, S.W.; Lyon, A.W.; Benzies, K.M.; McNeil, D.A.; Lye, S.J.; Dolan, S.M.; Pennell, C.E.; Bocking, A.D.; Tough, S.C. The All Our Babies pregnancy cohort: Design, methods, and participant characteristics. BMC Pregnancy Childbirth 2013, 13, 1–12. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Depression Unlikely 1 (n = 65) | Probable Depression 1 (n = 34) | p-Value | |
|---|---|---|---|
| Maternal Characteristics | |||
| Mid-pregnancy anxiety, n ≥ 40 STAI 2 Score (%) | 12 (19) | 31 (91) | <0.001 * |
| Mid-pregnancy stress, n ≥ 14 PSS 3 Score (%) | 27 (42) | 34 (100) | <0.001 * |
| Pre-pregnancy BMI, mean (SD), kg/m2 | 24.3 (5.15) | 27.4 (7.42) | 0.05 |
| Met GWG Guidelines 4, n yes (%) | 46 (71) | 16 (48) | 0.02 * |
| Household income, n ≥ $80,000 (%) | 43 (68) | 21 (66) | 0.75 |
| Education, n only high school completion (%) | 8 (12) | 6 (18) | 0.27 |
| Maternal age at delivery, mean (SD), years | 31.6 (5.51) | 31.3 (5.91) | 0.83 |
| Pre-pregnancy smoking, n yes (%) | 14 (22) | 5 (15) | 0.41 |
| Birth Characteristics | |||
| Sex, n male (%) | 29 (45) | 20 (59) | 0.18 |
| Gestational age at birth, mean (SD), weeks | 38.8 (1.51) | 37.8 (2.46) | 0.03 * |
| Birth weight, mean (SD), grams | 3316 (490) | 3098 (717) | 0.13 |
| Large for gestational age 5, n LGA (%) | 4 (7.1) | 3 (9.1) | 0.71 |
| Small for gestational age 6, n SGA (%) | 4 (7.1) | 4 (12) | 0.46 |
| Preterm birth (≤36 weeks), n preterm (%) | 4 (6.2) | 8 (24) | 0.02 * |
| Results with p < 0.1 | Unadj. p-Value | FDR q-Value | BMI 1 | Smoking 2 | Maternal Age | Household Income 3 | Stress 4 + Anxiety 5 | All | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p-Value | q-Value | p-Value | q-Value | p-Value | q-Value | P-Value | q-Value | p-Value | q-Value | p-Value | q-Value | |||
| Alanine | 0.003 | 0.090 | 0.002 | 0.088 | 0.003 | 0.082 | 0.003 | 0.082 | 0.001 | 0.049 | 0.045 | 0.315 | 0.012 | 0.245 |
| Leucine | 0.007 | 0.090 | 0.016 | 0.112 | 0.013 | 0.114 | 0.012 | 0.118 | 0.015 | 0.123 | 0.094 | 0.512 | 0.156 | 0.640 |
| Methionine | 0.028 | 0.155 | 0.004 | 0.088 | 0.014 | 0.114 | 0.009 | 0.110 | 0.009 | 0.088 | 0.036 | 0.315 | 0.042 | 0.294 |
| Phenylalanine | 0.010 | 0.099 | 0.009 | 0.088 | 0.010 | 0.114 | 0.015 | 0.123 | 0.007 | 0.086 | 0.188 | 0.709 | 0.196 | 0.640 |
| Valine | 0.028 | 0.155 | 0.028 | 0.172 | 0.037 | 0.201 | 0.039 | 0.191 | 0.026 | 0.182 | 0.293 | 0.763 | 0.222 | 0.640 |
| Glucose | 0.007 | 0.090 | 0.008 | 0.088 | 0.005 | 0.082 | 0.005 | 0.082 | 0.007 | 0.086 | 0.025 | 0.315 | 0.018 | 0.245 |
| Lactate | 0.004 | 0.090 | 0.006 | 0.088 | 0.004 | 0.082 | 0.005 | 0.082 | 0.003 | 0.074 | 0.129 | 0.588 | 0.066 | 0.404 |
| 3-BHB 6 | 0.026 | 0.155 | 0.049 | 0.240 | 0.030 | 0.184 | 0.026 | 0.182 | 0.040 | 0.192 | 0.139 | 0.588 | 0.222 | 0.640 |
| Pyruvate | 0.026 | 0.155 | 0.067 | 0.278 | 0.030 | 0.184 | 0.039 | 0.191 | 0.031 | 0.190 | 0.010 | 0.315 | 0.002 | 0.098 |
| Antimony 121 | 0.052 | 0.877 | 0.055 | 0.935 | 0.109 | 0.972 | 0.114 | 0.965 | 0.075 | 0.946 | 0.223 | 0.659 | 0.204 | 0.640 |
| Acetone | 0.066 | 0.292 | 0.068 | 0.278 | 0.061 | 0.270 | 0.058 | 0.258 | 0.050 | 0.204 | 0.372 | 0.829 | 0.374 | 0.746 |
| IPA 7 | 0.061 | 0.292 | 0.168 | 0.492 | 0.066 | 0.270 | 0.077 | 0.314 | 0.126 | 0.386 | 0.817 | 0.960 | 0.690 | 0.867 |
| Citrate | 0.076 | 0.297 | 0.016 | 0.112 | 0.043 | 0.211 | 0.038 | 0.191 | 0.041 | 0.192 | 0.040 | 0.315 | 0.037 | 0.294 |
| Urea | 0.079 | 0.297 | 0.087 | 0.328 | 0.112 | 0.392 | 0.110 | 0.415 | 0.094 | 0.327 | 0.042 | 0.315 | 0.037 | 0.294 |
| Anxiety Unlikely 1 (n = 173) | Probable Anxiety 1 (n = 96) | p-Value | |
|---|---|---|---|
| Maternal Characteristics | |||
| Mid-pregnancy depression, n ≥ 13 EPDS 2 Score (%) | 2 (1.2) | 31 (33) | <0.001 * |
| Mid-pregnancy stress, n ≥ 14 PSS 3 Score (%) | 60 (35) | 88 (92) | <0.001 * |
| Pre-pregnancy BMI, mean (SD), kg/m2 | 24.3 (5.20) | 25.6 (5.71) | 0.037 * |
| Met GWG Guidelines 4, n yes (%) | 105 (62) | 58 (61) | 0.14 |
| Household income, n ≥ $80,000 (%) | 126 (76) | 56 (60) | 0.017 * |
| Education, n only high school completion (%) | 17 (.9.8) | 15 (16) | 0.23 |
| Maternal age at delivery, mean (SD), years | 31.7 (4.30) | 31.8 (4.96) | 0.83 |
| Pre-pregnancy smoking, n yes (%) | 24 (14) | 21 (22) | 0.096 |
| Birth Characteristics | |||
| Sex, n male (%) | 91 (53) | 48 (50) | 0.68 |
| Gestational age at birth, mean (SD), weeks | 38.9 (1.90) | 38.5 (2.04) | 0.11 |
| Birth weight, mean (SD), grams | 3307 (544) | 3257 (599) | 0.52 |
| Large for gestational age 5, n LGA (%) | 12 (7.8) | 9 (10) | 0.53 |
| Small for gestational age 6, n SGA (%) | 16 (10) | 9 (10) | 0.95 |
| Preterm birth (≤36 weeks), n preterm (%) | 10 (5.9) | 13 (14) | 0.033 * |
| Results with p < 0.1 | Unadj. p-Value | FDR q-Value | BMI 1 | Smoking 2 | Maternal Age | Household Income 3 | Stress 4 + Depression 5 | All | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p-Value | q-Value | p-Value | q-Value | p-Value | q-Value | p-Value | q-Value | p-Value | q-Value | p-Value | q-Value | |||
| 3-BHB 6 | 0.049 | 0.765 | 0.054 | 0.822 | 0.075 | 0.787 | 0.056 | 0.756 | 0.084 | 0.732 | 0.272 | 0.956 | 0.493 | 0.952 |
| Zinc 66 | 0.030 | 0.769 | 0.049 | 0.654 | 0.036 | 0.644 | 0.030 | 0.658 | 0.061 | 0.758 | 0.050 | 0.467 | 0.036 | 0.815 |
| IPA 7 | 0.052 | 0.765 | 0.061 | 0.822 | 0.068 | 0.787 | 0.062 | 0.756 | 0.120 | 0.732 | 0.314 | 0.956 | 0.734 | 0.952 |
| Butyrate | 0.088 | 0.765 | 0.114 | 0.822 | 0.096 | 0.787 | 0.098 | 0.756 | 0.085 | 0.732 | 0.288 | 0.956 | 0.405 | 0.952 |
| Citrate | 0.100 | 0.765 | 0.129 | 0.822 | 0.126 | 0.787 | 0.124 | 0.756 | 0.153 | 0.732 | 0.548 | 0.956 | 0.758 | 0.952 |
| Calcium 44 | 0.061 | 0.769 | 0.031 | 0.654 | 0.046 | 0.644 | 0.047 | 0.658 | 0.070 | 0.758 | 0.033 | 0.467 | 0.080 | 0.815 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laketic, K.; Lalonde-Bester, S.; Smyth, K.; Slater, D.M.; Tough, S.C.; Ishida, H.; Vogel, H.J.; Giesbrecht, G.F.; Mu, C.; Shearer, J. Maternal Metabolites Indicative of Mental Health Status during Pregnancy. Metabolites 2023, 13, 24. https://doi.org/10.3390/metabo13010024
Laketic K, Lalonde-Bester S, Smyth K, Slater DM, Tough SC, Ishida H, Vogel HJ, Giesbrecht GF, Mu C, Shearer J. Maternal Metabolites Indicative of Mental Health Status during Pregnancy. Metabolites. 2023; 13(1):24. https://doi.org/10.3390/metabo13010024
Chicago/Turabian StyleLaketic, Katarina, Sophie Lalonde-Bester, Kim Smyth, Donna M. Slater, Suzanne C. Tough, Hiroaki Ishida, Hans J. Vogel, Gerald F. Giesbrecht, Chunlong Mu, and Jane Shearer. 2023. "Maternal Metabolites Indicative of Mental Health Status during Pregnancy" Metabolites 13, no. 1: 24. https://doi.org/10.3390/metabo13010024
APA StyleLaketic, K., Lalonde-Bester, S., Smyth, K., Slater, D. M., Tough, S. C., Ishida, H., Vogel, H. J., Giesbrecht, G. F., Mu, C., & Shearer, J. (2023). Maternal Metabolites Indicative of Mental Health Status during Pregnancy. Metabolites, 13(1), 24. https://doi.org/10.3390/metabo13010024