
Feasibility of Interstitial Fluid Ketone Monitoring with Microneedles



Abstract
:
1. Introduction
2. Results
2.1. MA Prototype Design and Testing
2.2. In Vivo ISF and Blood Glucose Measurements in Fasted Rats
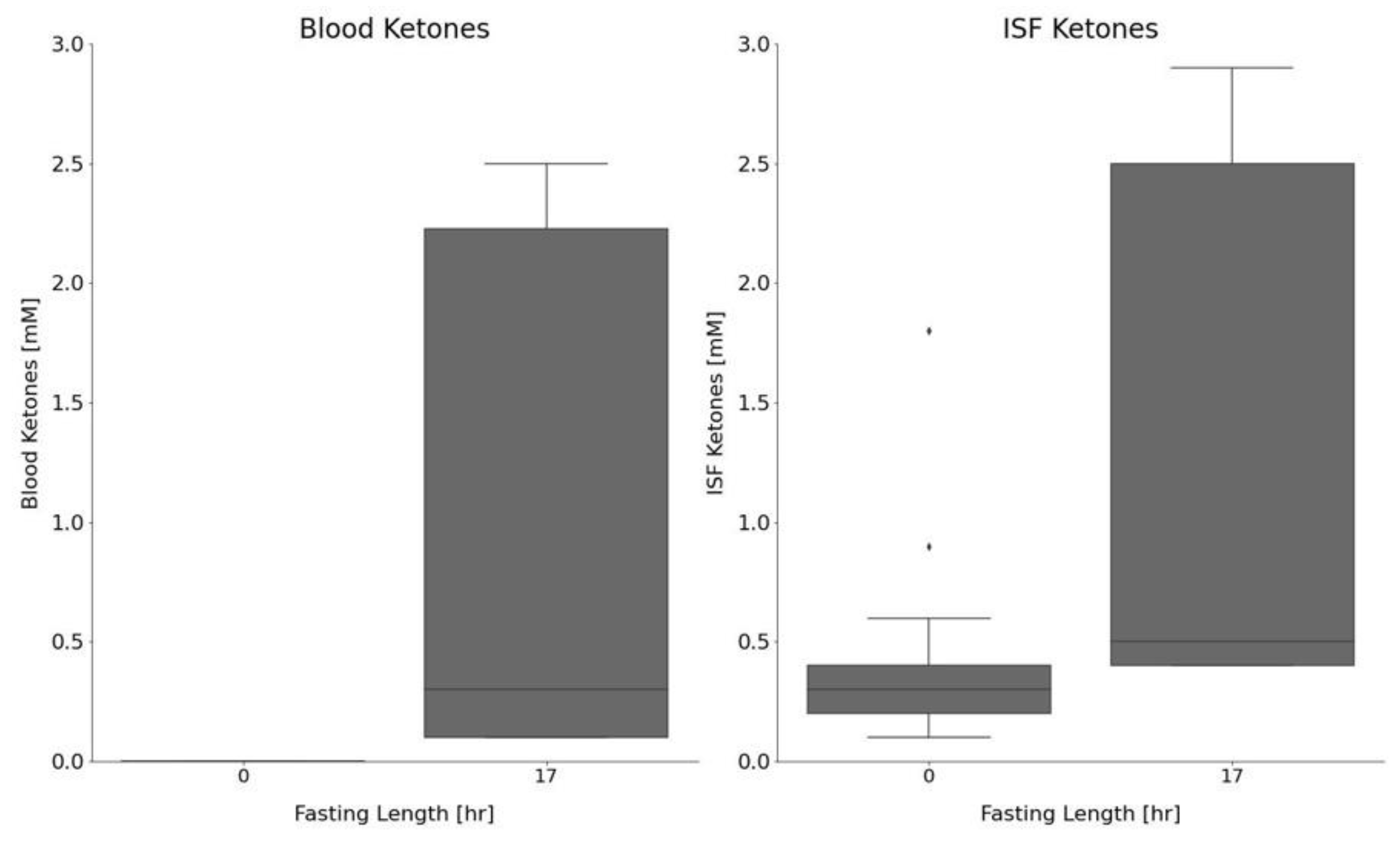
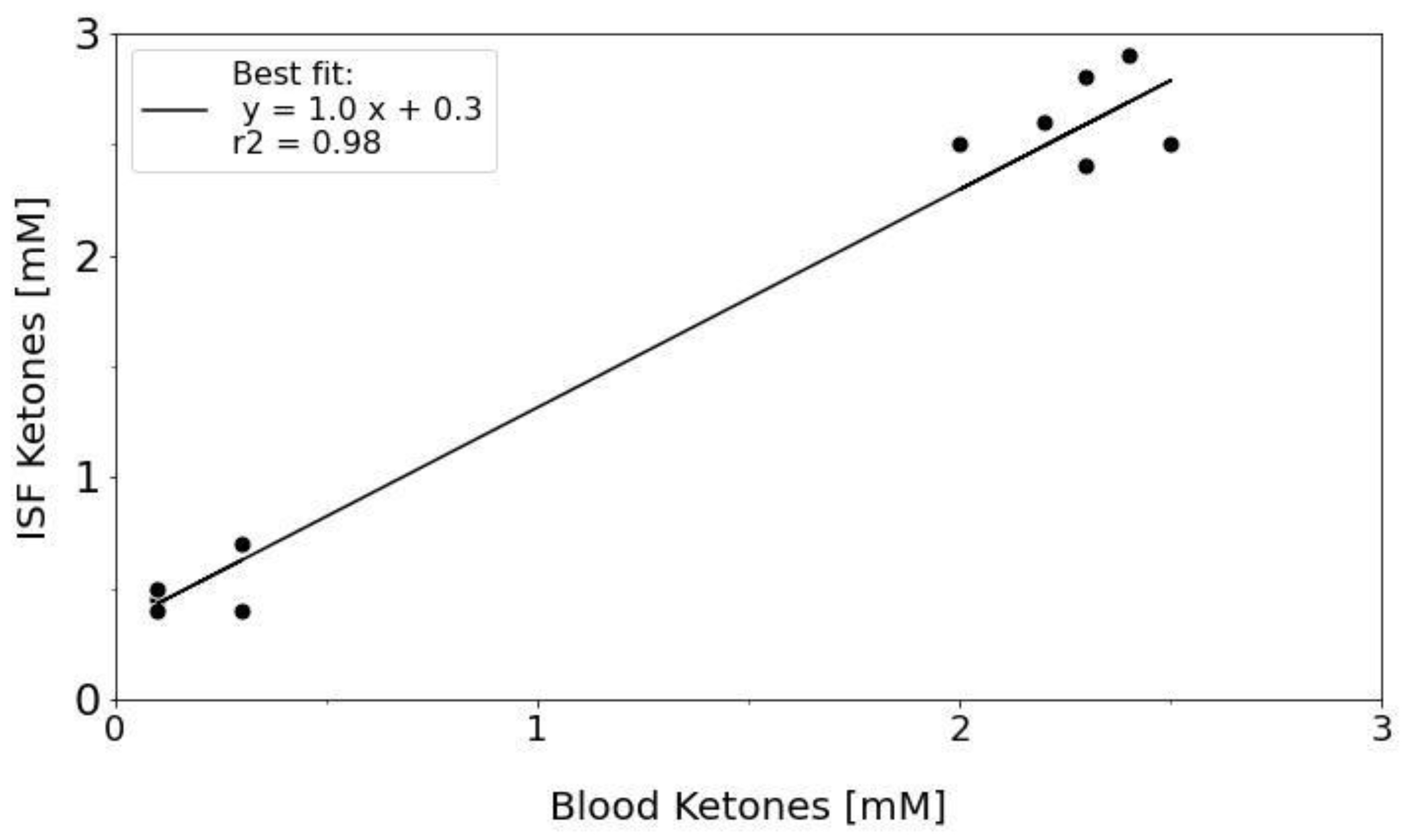
2.3. In Vivo Ketone Measurements in Fasted vs. Control Animals
3. Discussion
4. Materials and Methods
4.1. Animals, Materials, and Supplies
4.2. Fasting Model
4.3. MA Design and 3D Printing
4.4. ISF Extraction and Fluid Collection
4.5. Data Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ciechanowska, A.; Ladyzynski, P.; Wojcicki, J.M.; Sabalinska, S.; Krzymien, J.; Pulawska, E.; Karnafel, W.; Foltynski, P.; Kawiak, J. Microdialysis Monitoring of Glucose, Lactate, Glycerol, and Pyruvate in Patients with Diabetic Ketoacidosis. Int. J. Artif. Organs 2013, 36, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Fayfman, M.; Pasquel, F.J.; Umpierrez, G.E. Management of Hyperglycemic Crises: Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar State. Med. Clin. N. Am. 2017, 101, 587. [Google Scholar] [CrossRef] [PubMed]
- Lam, T.I.; Anderson, S.E.; Glaser, N.; O’Donnell, M.E. Bumetanide Reduces Cerebral Edema Formation in Rats with Diabetic Ketoacidosis. Diabetes 2005, 54, 510–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuen, N.; Anderson, S.E.; Glaser, N.; Tancredi, D.J.; O’Donnell, M.E. Cerebral Blood Flow and Cerebral Edema in Rats with Diabetic Ketoacidosis. Diabetes 2008, 57, 2588–2594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marunaka, Y. Roles of Interstitial Fluid PH in Diabetes Mellitus: Glycolysis and Mitochondrial Function. World J. Diabetes 2015, 6, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Holm, K.M.D.; Linnet, K.; Rasmussen, B.S.; Pedersen, A.J. Determination of Ketone Bodies in Blood by Headspace Gas Chromatography-Mass Spectrometry. J. Anal. Toxicol. 2010, 34, 549–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teymourian, H.; Moonla, C.; Tehrani, F.; Vargas, E.; Aghavali, R.; Barfidokht, A.; Tangkuaram, T.; Mercier, P.P.; Dassau, E.; Wang, J. Microneedle-Based Detection of Ketone Bodies along with Glucose and Lactate: Toward Real-Time Continuous Interstitial Fluid Monitoring of Diabetic Ketosis and Ketoacidosis. Anal. Chem. 2020, 92, 2291–2300. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.M.; Miller, P.R.; Ebrahimi, P.; Polsky, R.; Baca, J.T. Minimally-Invasive, Microneedle-Array Extraction of Interstitial Fluid for Comprehensive Biomedical Applications: Transcriptomics, Proteomics, Metabolomics, Exosome Research, and Biomarker Identification. Lab. Anim. 2018, 52, 526–530. [Google Scholar] [CrossRef] [PubMed]
- Miller, P.R.; Taylor, R.M.; Tran, B.Q.; Boyd, G.; Glaros, T.; Chavez, V.H.; Krishnakumar, R.; Sinha, A.; Poorey, K.; Williams, K.P.; et al. Extraction and Biomolecular Analysis of Dermal Interstitial Fluid Collected with Hollow Microneedles. Commun. Biol. 2018, 1, 173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, B.Q.; Miller, P.R.; Taylor, R.M.; Boyd, G.; Mach, P.M.; Rosenzweig, C.N.; Baca, J.T.; Polsky, R.; Glaros, T. Proteomic Characterization of Dermal Interstitial Fluid Extracted Using a Novel Microneedle-Assisted Technique. J. Proteome Res. 2018, 17, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, S.; Dave, K.; Vamsi, V.; Venuganti, K. Microneedles in the Clinic. J. Control. Release 2017, 260, 164–182. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, R.F.; Mooney, K.; Caffarel-Salvador, E.; Torrisi, B.M.; Eltayib, E.; McElnay, J.C. Microneedle-Mediated Minimally Invasive Patient Monitoring. Ther. Drug Monit. 2013, 36, 1. [Google Scholar] [CrossRef] [PubMed]
- Herfst, M.J.; van Rees, H. Suction Blister Fluid as a Model for Interstitial Fluid in Rats. Arch. Dermatol. Res. 1978, 263, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Kayashima, S.; Arai, T.; Kikuchi, M.; Nagata, N.; Ito, N.; Kuriyama, T.; Kimura, J. Suction Effusion Fluid from Skin and Constituent Analysis: New Candidate for Interstitial Fluid. Am. J. Physiol. 1992, 263, H1623–H1627. [Google Scholar] [CrossRef] [PubMed]
- Romanyuk, A.V.; Zvezdin, V.N.; Samant, P.; Grenader, M.I.; Zemlyanova, M.; Prausnitz, M.R. Collection of Analytes from Microneedle Patches. Anal. Chem. 2014, 86, 10520–10523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, R.M.; Maharjan, D.; Moreu, F.; Baca, J.T. Parametric Study of 3D Printed Microneedle (MN) Holders for Interstitial Fluid (ISF) Extraction. Microsyst. Technol. 2020, 26, 2067–2073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cengiz, E.; Tamborlane, W.V. A Tale of Two Compartments: Interstitial Versus Blood Glucose Monitoring. Diabetes Technol. Ther. 2009, 11, S-11–S-16. [Google Scholar] [CrossRef] [PubMed]
- Behdad, S.; Mortazavizadeh, A.; Ayatollahi, V.; Khadiv, Z.; Khalilzadeh, S. The Effects of Propofol and Isoflurane on Blood Glucose during Abdominal Hysterectomy in Diabetic Patients. Diabetes Metab. J. 2014, 38, 311–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | 17 h Fast | |
|---|---|---|
| Number of animals (N) | 3 | 2 |
| Glucose | ||
| Number of samples (n) | 34 | 20 |
| Mean Glucose [mg/dL] | 318 | 155 |
| Stdev Glucose [mg/dL] | 86 | 44 |
| Blood Ketones | ||
| Number of samples (n) | 34 | 20 |
| Mean Blood Ketones [mM] | 0.0 | 1.0 |
| Stdev Blood Ketones [mM] | 0.0 | 1.0 |
| ISF Ketones | ||
| Number of samples (n) | 31 | 17 |
| Mean ISF Ketones [mM] | 0.4 | 1.3 |
| Stdev ISF Ketones [mM] | 0.3 | 1.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taylor, R.M.; Baca, J.T. Feasibility of Interstitial Fluid Ketone Monitoring with Microneedles. Metabolites 2022, 12, 424. https://doi.org/10.3390/metabo12050424
Taylor RM, Baca JT. Feasibility of Interstitial Fluid Ketone Monitoring with Microneedles. Metabolites. 2022; 12(5):424. https://doi.org/10.3390/metabo12050424
Chicago/Turabian StyleTaylor, Robert M., and Justin T. Baca. 2022. "Feasibility of Interstitial Fluid Ketone Monitoring with Microneedles" Metabolites 12, no. 5: 424. https://doi.org/10.3390/metabo12050424
APA StyleTaylor, R. M., & Baca, J. T. (2022). Feasibility of Interstitial Fluid Ketone Monitoring with Microneedles. Metabolites, 12(5), 424. https://doi.org/10.3390/metabo12050424