
Selenium Levels and Antioxidant Activity in Critically Ill Patients with Systemic Inflammatory Response Syndrome

 ,
,  , and
, and 
Abstract
:
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
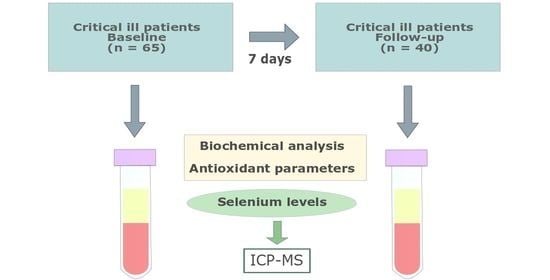
4.1. Subjects and Study Design
4.2. Data Collection
4.3. Nutritional Profile
4.4. Blood Sampling and Biochemical Parameters
4.5. Measurement of Se, GPx, and TAC
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Robertson, L.C.; Al-Haddad, M. Recognizing the Critically Ill Patient. Anaesth. Intensive Care Med. 2013, 14, 11–14. [Google Scholar]
- Van Niekerk, G.; Engelbrecht, A.-M. Inflammation-Induced Metabolic Derangements or Adaptation: An Immunometabolic Perspective. Cytokine Growth Factor Rev. 2018, 43, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, R.K.; Burns, B. Systemic inflammatory response syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Hardy, G.; Hardy, I.; Manzanares, W. Selenium Supplementation in the Critically Ill. Nutr. Clin. Pract. 2012, 27, 21–33. [Google Scholar] [CrossRef]
- Burk, R.F.; Hill, K.E. Regulation of Selenium Metabolism and Transport. Annu. Rev. Nutr. 2015, 35, 109–134. [Google Scholar] [CrossRef]
- Koekkoek, W.A.C.; Hettinga, K.; de Vries, J.H.M.; van Zanten, A.R.H. Micronutrient Deficiencies in Critical Illness. Clin. Nutr. 2021, 40, 3780–3786. [Google Scholar] [CrossRef]
- Cirino Ruocco, M.A.; Pacheco Cechinatti, E.D.; Barbosa, F.; Navarro, A.M. Zinc and Selenium Status in Critically Ill Patients According to Severity Stratification. Nutrition 2018, 45, 85–89. [Google Scholar] [CrossRef] [Green Version]
- Sakr, Y.; Reinhart, K.; Bloos, F.; Marx, G.; Russwurm, S.; Bauer, M.; Brunkhorst, F. Time Course and Relationship between Plasma Selenium Concentrations, Systemic Inflammatory Response, Sepsis, and Multiorgan Failure. Br. J. Anaesth. 2007, 98, 775–784. [Google Scholar] [CrossRef] [Green Version]
- Stefanowicz, F.A.; Talwar, D.; O’Reilly, D.S.J.; Dickinson, N.; Atkinson, J.; Hursthouse, A.S.; Rankin, J.; Duncan, A. Erythrocyte Selenium Concentration as a Marker of Selenium Status. Clin. Nutr. 2013, 32, 837–842. [Google Scholar] [CrossRef]
- Sundström Rehal, M.; Tjäder, I.; Wernerman, J. Nutritional Needs for the Critically Ill in Relation to Inflammation. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 138–143. [Google Scholar] [CrossRef]
- Mogensen, K.M.; Robinson, M.K.; Casey, J.D.; Gunasekera, N.S.; Moromizato, T.; Rawn, J.D.; Christopher, K.B. Nutritional Status and Mortality in the Critically Ill. Crit. Care Med. 2015, 43, 2605–2615. [Google Scholar] [CrossRef]
- Weitzel, L.R.B.; Mayles, W.J.; Sandoval, P.A.; Wischmeyer, P.E. Effects of pharmaconutrients on cellular dysfunction and the microcirculation in critical illness. Curr. Opin. Anaesthesiol. 2009, 22, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Guillin, O.M.; Vindry, C.; Ohlmann, T.; Chavatte, L. Selenium, Selenoproteins and Viral Infection. Nutrients 2019, 11, 2101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labunskyy, V.M.; Hatfield, D.L.; Gladyshev, V.N. Selenoproteins: Molecular Pathways and Physiological Roles. Physiol. Rev. 2014, 94, 739–777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duncan, A.; Talwar, D.; McMillan, D.C.; Stefanowicz, F.; O’Reilly, D.S.J. Quantitative Data on the Magnitude of the Systemic Inflammatory Response and Its Effect on Micronutrient Status Based on Plasma Measurements. Am. J. Clin. Nutr. 2012, 95, 64–71. [Google Scholar] [CrossRef] [Green Version]
- Manzanares, W.; Lemieux, M.; Elke, G.; Langlois, P.L.; Bloos, F.; Heyland, D.K. High-Dose Intravenous Selenium Does Not Improve Clinical Outcomes in the Critically Ill: A Systematic Review and Meta-Analysis. Crit. Care 2016, 20, 356. [Google Scholar] [CrossRef] [Green Version]
- Pich, J. Selenium Supplementation for Critically Ill Adults (Review Summary). Clin. Nurse Spec. 2020, 34, 206–207. [Google Scholar] [CrossRef]
- Allingstrup, M.; Afshari, A. Selenium Supplementation for Critically Ill Adults. Cochrane Database Syst. Rev. 2015, 27, CD003703. [Google Scholar] [CrossRef]
- Broman, L.M.; Bernardson, A.; Bursell, K.; Wernerman, J.; Fläring, U.; Tjäder, I. Serum Selenium in Critically Ill Patients: Profile and Supplementation in a Depleted Region. Acta Anaesthesiol. Scand. 2020, 64, 803–809. [Google Scholar] [CrossRef]
- Manzanares, W.; Biestro, A.; Galusso, F.; Torre, M.H.; Mañay, N.; Pittini, G.; Facchin, G.; Hardy, G. Serum Selenium and Glutathione Peroxidase-3 Activity: Biomarkers of Systemic Inflammation in the Critically Ill? Intensive Care Med. 2009, 35, 882–889. [Google Scholar] [CrossRef]
- McMillan, D.C.; Maguire, D.; Talwar, D. Relationship between Nutritional Status and the Systemic Inflammatory Response: Micronutrients. Proc. Nutr. Soc. 2019, 78, 56–67. [Google Scholar] [CrossRef] [Green Version]
- Bar-Or, D.; Garrett, R.E. Is Low Plasma Selenium Concentration a True Reflection of Selenium Deficiency and Redox Status in Critically Ill Patients? Crit. Care Med. 2011, 39, 2000–2001. [Google Scholar] [CrossRef] [PubMed]
- Forceville, X.; Vitoux, D.; Gauzit, R.; Combes, A.; Lahilaire, P.; Chappuis, P. Selenium, Systemic Immune Response Syndrome, Sepsis, and Outcome in Critically Ill Patients. Crit. Care Med. 1998, 26, 1536–1544. [Google Scholar] [CrossRef] [PubMed]
- Skröder, H.M.; Hamadani, J.D.; Tofail, F.; Persson, L.Å.; Vahter, M.E.; Kippler, M.J. Selenium Status in Pregnancy Influences Children’s Cognitive Function at 1.5 Years of Age. Clin. Nutr. 2015, 34, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Haratake, M.; Fujimoto, K.; Hirakawa, R.; Ono, M.; Nakayama, M. Hemoglobin-Mediated Selenium Export from Red Blood Cells. J. Biol. Inorg. Chem. 2008, 13, 471–479. [Google Scholar] [CrossRef] [Green Version]
- Kaushal, N.; Hegde, S.; Lumadue, J.; Paulson, R.F.; Prabhu, K.S. The Regulation of Erythropoiesis by Selenium in Mice. Antioxid. Redox Signal. 2011, 14, 1403–1412. [Google Scholar] [CrossRef]
- Manzanares, W.; Langlois, P.L.; Heyland, D.K. Pharmaconutrition with Selenium in Critically Ill Patients: What Do We Know? Nutr. Clin. Pract. 2015, 30, 34–43. [Google Scholar] [CrossRef]
- European Food Safety Authority. Dietary Reference Values. Available online: https://Www.Efsa.Europa.Eu/En/Topics/Topic/Dietary-Reference-Values (accessed on 16 February 2022).
- Gundogan, K.; Emur Gunay, Y.; Ozer, N.T.; Gunes Sahin, G.; Alptekinoglu Mendil, N.O.; Sahin, S.; Temel, S.; Guven, M.; Sungur, M. Serum Trace Elements Levels in Patients Transferred from the Intensive Care Unit to Wards. Clin. Nutr. ESPEN 2021, 44, 218–223. [Google Scholar] [CrossRef]
- Valla, F.V.; Bost, M.; Roche, S.; Pitance, M.; Cuerq, C.; Ridout, J.; Ecochard, R.; Ginhoux, T.; Bellon, A.; Ford-Chessel, C.; et al. Multiple Micronutrient Plasma Level Changes Are Related to Oxidative Stress Intensity in Critically Ill Children. Pediatr. Crit. Care Med. 2018, 19, e455–e463. [Google Scholar] [CrossRef]
- Koekkoek, K.W.A.C.; van Zanten, A.R.H. Nutrition in the ICU: New Trends versus Old-Fashioned Standard Enteral Feeding? Curr. Opin. Anaesthesiol. 2018, 31, 136–143. [Google Scholar] [CrossRef]
- de Oliveira Nascimento, R.G.B.; Nogueira, R.J.N.; Cozzolino, S.M.F.; Vasques, A.C.J.; Hessel, G. Influence of Selenium Supplementation on Patients with Inflammation: A Pilot Double Blind Randomized Study. Nutrition 2017, 41, 32–36. [Google Scholar]
- Zhao, Y.; Yang, M.; Mao, Z.; Yuan, R.; Wang, L.; Hu, X.; Zhou, F.; Kang, H. The Clinical Outcomes of Selenium Supplementation on Critically Ill Patients: A Meta-Analysis of Randomized Controlled Trials. Medicine 2019, 98, e15473. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, M.A.; Saghaleini, S.H.; Mahmoodpoor, A.; Ghojazadeh, M.; Mousavi, S.N. Daily Parenteral Selenium Therapy in Critically Ill Patients: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin. Nutr. ESPEN 2021, 41, 49–58. [Google Scholar] [CrossRef]
- Stefanowicz, F.; Gashut, R.A.; Talwar, D.; Duncan, A.; Beulshausen, J.F.; McMillan, D.C.; Kinsella, J. Assessment of Plasma and Red Cell Trace Element Concentrations, Disease Severity, and Outcome in Patients with Critical Illness. J. Crit. Care 2014, 29, 214–218. [Google Scholar] [CrossRef]
- Roman, M.; Jitaru, P.; Barbante, C. Selenium Biochemistry and Its Role for Human Health. Metallomics 2014, 6, 25–54. [Google Scholar] [CrossRef] [PubMed]
- Vavrova, L.; Rychlikova, J.; Mrackova, M.; Novakova, O.; Zak, A.; Novak, F. Increased Inflammatory Markers with Altered Antioxidant Status Persist after Clinical Recovery from Severe Sepsis: A Correlation with Low HDL Cholesterol and Albumin. Clin. Exp. Med. 2016, 16, 557–569. [Google Scholar] [CrossRef] [PubMed]
- Krenzlin, H.; Wesp, D.; Schmitt, J.; Frenz, C.; Kurz, E.; Masomi-Bornwasser, J.; Lotz, J.; Ringel, F.; Kerz, T.; Keric, N. Decreased Superoxide Dismutase Concentrations (SOD) in Plasma and CSF and Increased Circulating Total Antioxidant Capacity (TAC) Are Associated with Unfavorable Neurological Outcome after Aneurysmal Subarachnoid Hemorrhage. J. Clin. Med. 2021, 10, 1188. [Google Scholar] [CrossRef]
- World Medical Association World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [Green Version]
- Gemma Salvador Castell, L.S.M.; Ribas-Barba, L. ¿Qué y cuánto comemos? El método Recuerdo de 24 horas. Rev. Esp. Nutr. Comunitaria 2015, 21, 42–44. [Google Scholar]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN Guideline on Clinical Nutrition in the Intensive Care Unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef] [Green Version]
- Millán, E.; Florea, D.; Sáez, L.; Molina, J.; López-González, B.; Pérez, A.; Planells, E. Deficient selenium status of a healthy adult Spanish population. Nutr. Hosp. 2012, 27, 524–528. [Google Scholar]
- Vassalle, C.; Petrozzi, L.; Botto, N.; Andreassi, M.G.; Zucchelli, G.C. Oxidative Stress and Its Association with Coronary Artery Disease and Different Atherogenic Risk Factors. J. Intern. Med. 2004, 256, 308–315. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Healthy Controls Mean (SD) N = 56 | ICU Patients Mean (SD) N = 65 | p-Value |
|---|---|---|---|
| BMI (kg/m2) | 25.0 (3.26) | 26.7 (4.77) | 0.069 |
| Patient 7-day mortality (n/N, %) | - | 25/65 (38.5) | - |
| APACHE-II score | - | 17.2 (4.94) | - |
| SOFA score | - | 9.34 (3.90) | - |
| Total proteins (g/dL) | 7.39 (0.37) | 5.19 (0.84) | 0.001 |
| Albumin (g/dL) | 4.41 (0.27) | 2.73 (0.62) | 0.001 |
| Prealbumin (mg/dL) | 27.9 (5.10) | 12.7 (6.72) | 0.001 |
| Triglycerides (mg/dL) | 110.7 (58.1) | 186.8 (124.0) | 0.001 |
| Total cholesterol (mg/dL) | 206.0 (40.8) | 108.9 (38.1) | 0.001 |
| Hemoglobin (g/dL) | 13.4 (1.88) | 10.9 (2.70) | 0.001 |
| CRP (mg/L) | 0.22 (0.25) | 19.9 (13.1) | 0.001 |
| Se support (µg/day) | 69.4 (30.3) | 37.8 (23.1) | 0.001 |
| Plasma Se (µg/L) | 76.4 (18.1) | 56.2 (12.9) | 0.001 |
| Erythrocyte Se (µg/L) | 109.3 (22.5) | 79.7 (14.9) | 0.001 |
| Erythrocyte Se (µg/g Hb) | 0.84 (0.24) | 0.76 (0.22) | 0.098 |
| GPx activity (U/g Hb) | 42.2 (28.7) | 29.0 (14.3) | 0.004 |
| SOD activity (U/g Hb) | 1628.1 (1439.0) | 1501.1 (551.1) | 0.546 |
| TAC (µmol/L) | 801.5 (374.7) | 1100.6 (490.5) | 0.001 |
| Parameters | Baseline Mean (SD) N = 65 | Follow-Up Mean (SD) N = 40 | ΔChange (%) | p-Value |
|---|---|---|---|---|
| SOFA score | 9.04 (3.39) | 5.12 (3.50) | −43.4 | 0.001 |
| Albumin (g/dL) | 2.85 (0.58) | 2.63 (0.67) | −7.71 | 0.139 |
| Prealbumin (mg/dL) | 12.5 (4.65) | 16.3 (9.80) | 30.4 | 0.143 |
| CRP (mg/L) | 19.8 (11.8) | 10.7 (8.63) | −46.0 | 0.001 |
| Plasma Se (µg/L) | 57.8 (11.6) | 42.6 (10.9) | −26.3 | 0.001 |
| Erythrocyte Se (µg/L) | 84.0 (15.4) | 69.2 (14.9) | −17.6 | 0.001 |
| Erythrocyte Se (µg/g Hb) | 0.80 (0.24) | 0.76 (0.20) | −5.00 | 0.343 |
| GPx activity (U/g Hb) | 30.6 (18.6) | 47.3 (27.9) | 54.6 | 0.016 |
| SOD activity (U/g Hb) | 1528.6 (587.2) | 1377.2 (652.2) | −9.90 | 0.265 |
| TAC (µmol/L) | 1016.3 (445.1) | 849.8 (509.4) | −16.4 | 0.061 |
| Selenium adequacy | ||||
| Plasma Se < 45.6 µg/L (n,%) | 10 (15.4) | 25 (62.5) | 150.0 | 0.033 |
| Erythrocyte Se < 69.0 µg/L (n,%) | 19 (29.2) | 20 (50.0) | 5.26 | 0.167 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrera-Quintana, L.; Vázquez-Lorente, H.; Molina-López, J.; Gamarra-Morales, Y.; Planells, E. Selenium Levels and Antioxidant Activity in Critically Ill Patients with Systemic Inflammatory Response Syndrome. Metabolites 2022, 12, 274. https://doi.org/10.3390/metabo12040274
Herrera-Quintana L, Vázquez-Lorente H, Molina-López J, Gamarra-Morales Y, Planells E. Selenium Levels and Antioxidant Activity in Critically Ill Patients with Systemic Inflammatory Response Syndrome. Metabolites. 2022; 12(4):274. https://doi.org/10.3390/metabo12040274
Chicago/Turabian StyleHerrera-Quintana, Lourdes, Héctor Vázquez-Lorente, Jorge Molina-López, Yenifer Gamarra-Morales, and Elena Planells. 2022. "Selenium Levels and Antioxidant Activity in Critically Ill Patients with Systemic Inflammatory Response Syndrome" Metabolites 12, no. 4: 274. https://doi.org/10.3390/metabo12040274
APA StyleHerrera-Quintana, L., Vázquez-Lorente, H., Molina-López, J., Gamarra-Morales, Y., & Planells, E. (2022). Selenium Levels and Antioxidant Activity in Critically Ill Patients with Systemic Inflammatory Response Syndrome. Metabolites, 12(4), 274. https://doi.org/10.3390/metabo12040274