
Integration of Metabolomic and Clinical Data Improves the Prediction of Intensive Care Unit Length of Stay Following Major Traumatic Injury

 ,
, 
 ,
,  ,
,
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Clinical Data Collection
2.3. Clinical Outcomes
2.4. Blood Sampling and Preparation of Serum
2.5. Metabolomics Sample Preparation and Analysis
2.6. Statistical Analysis
2.7. Partial Least-Squares Discriminant Analysis (PLS-DA) Analysis
3. Results
3.1. Patient Demographics
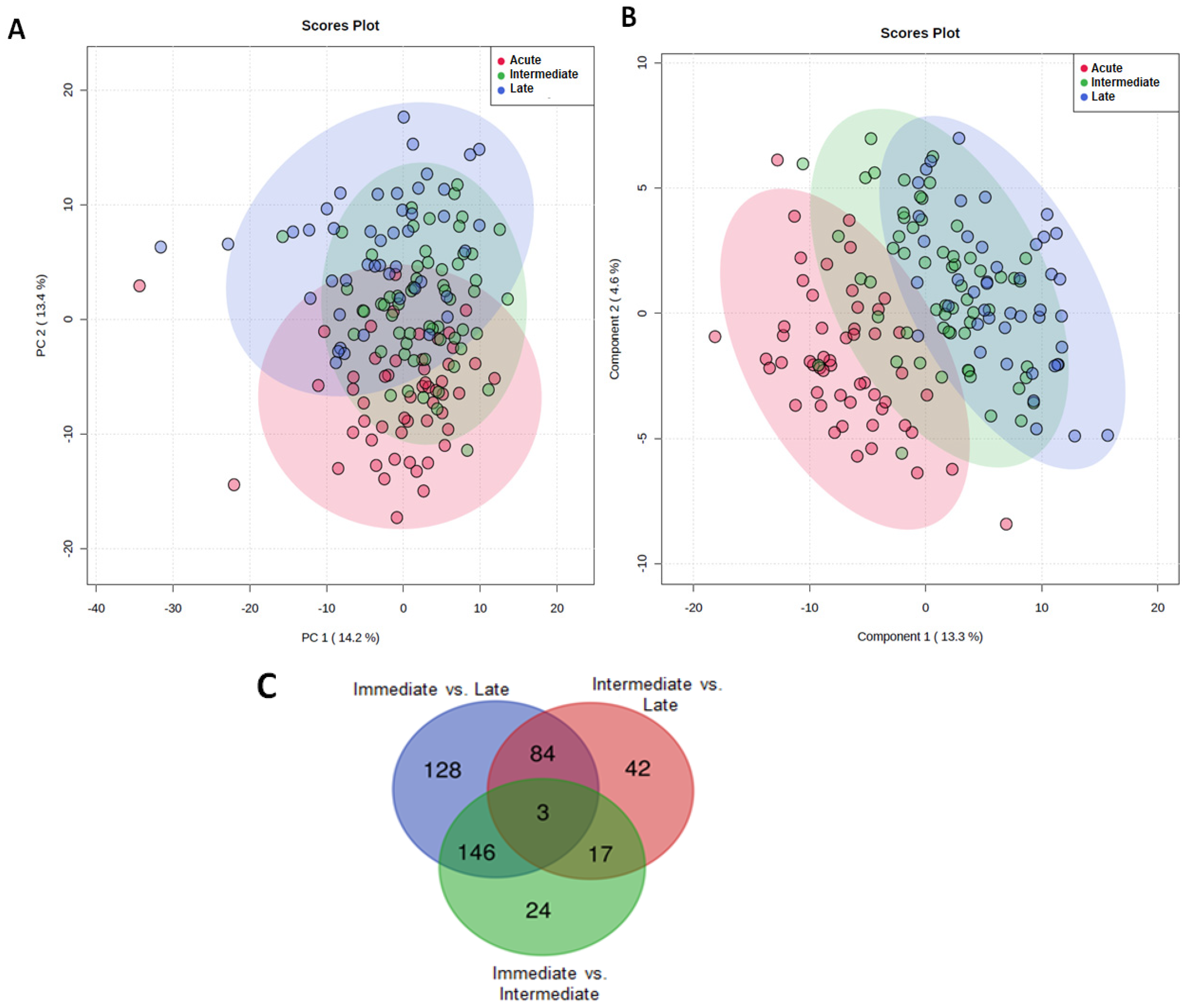
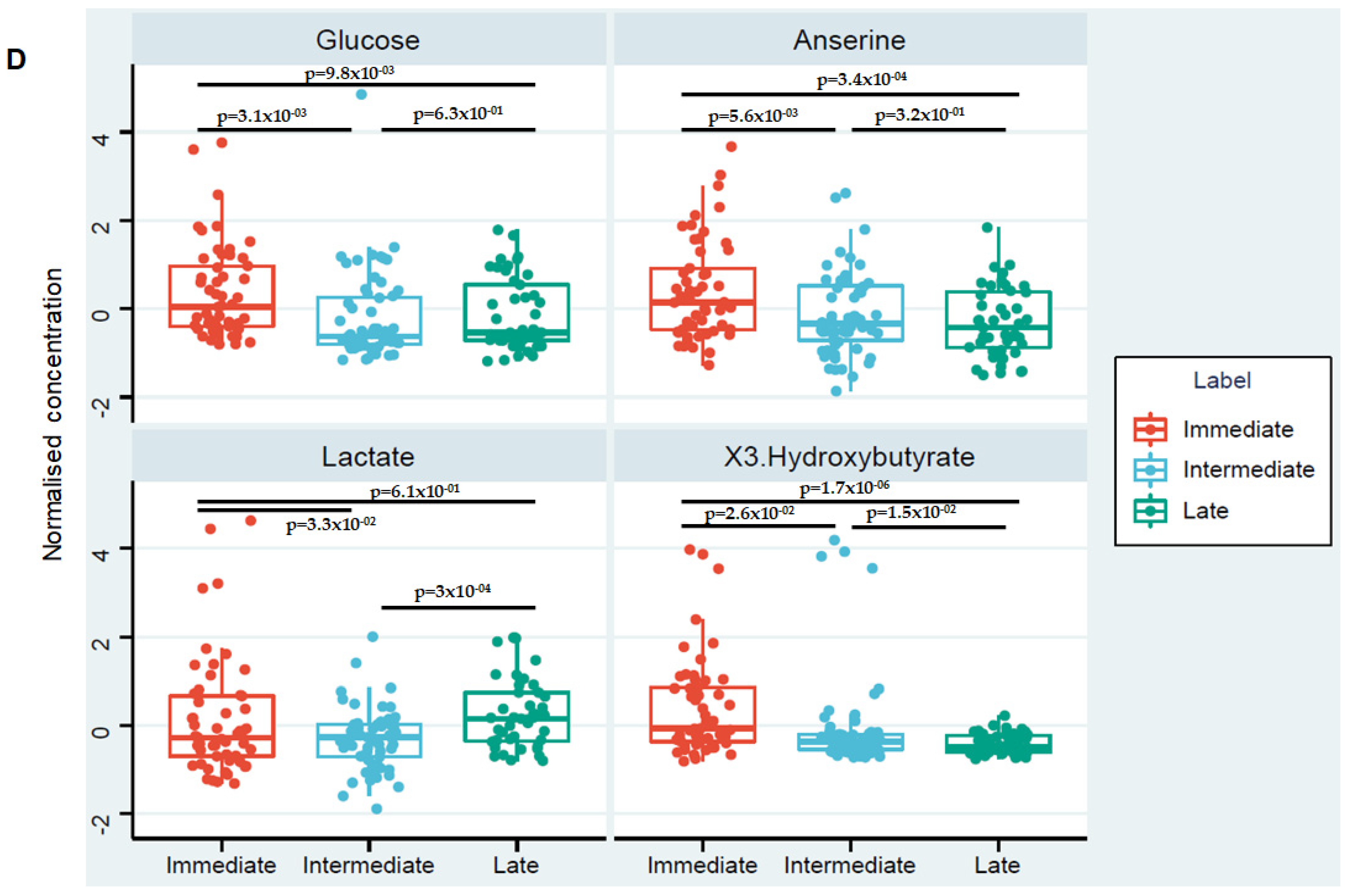
3.2. Changes in the Serum Metabolome over Time
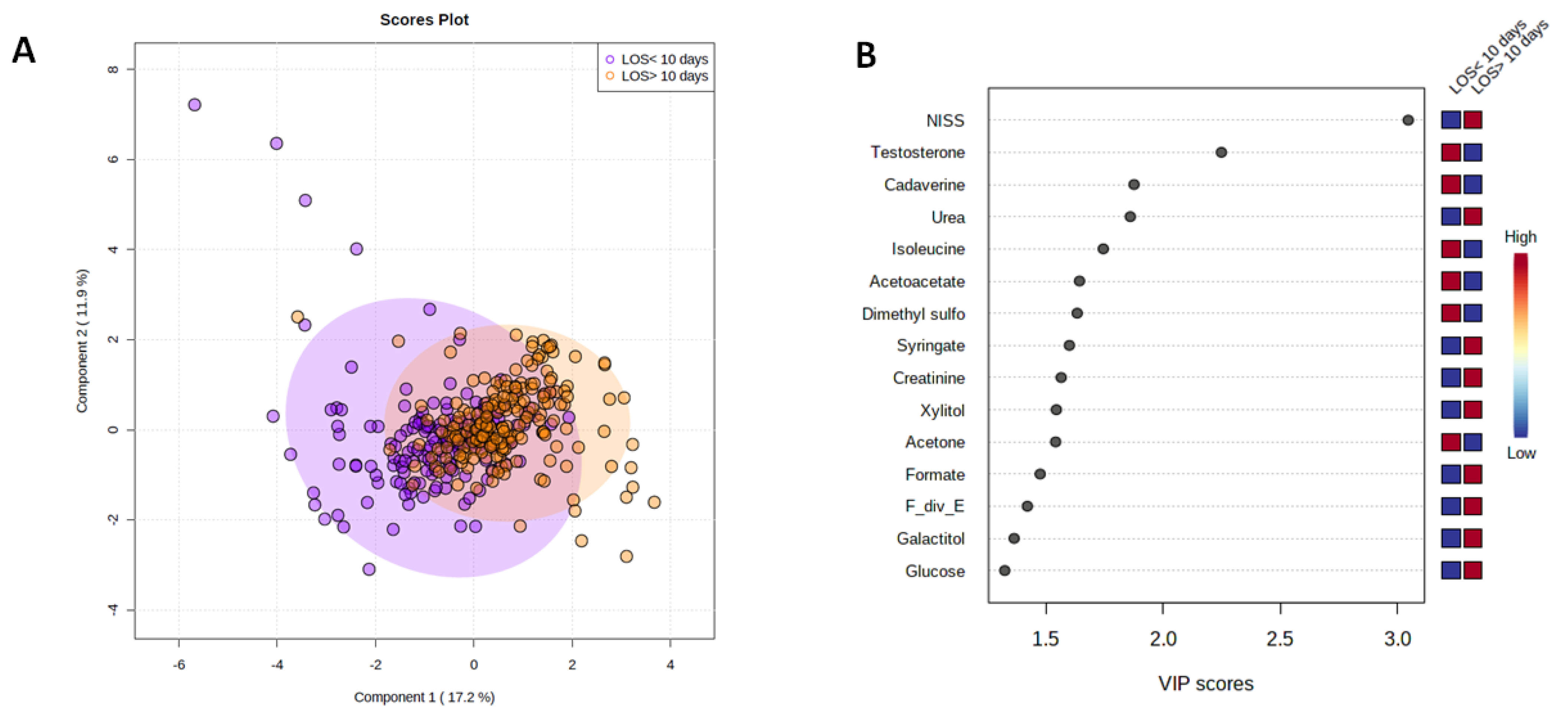
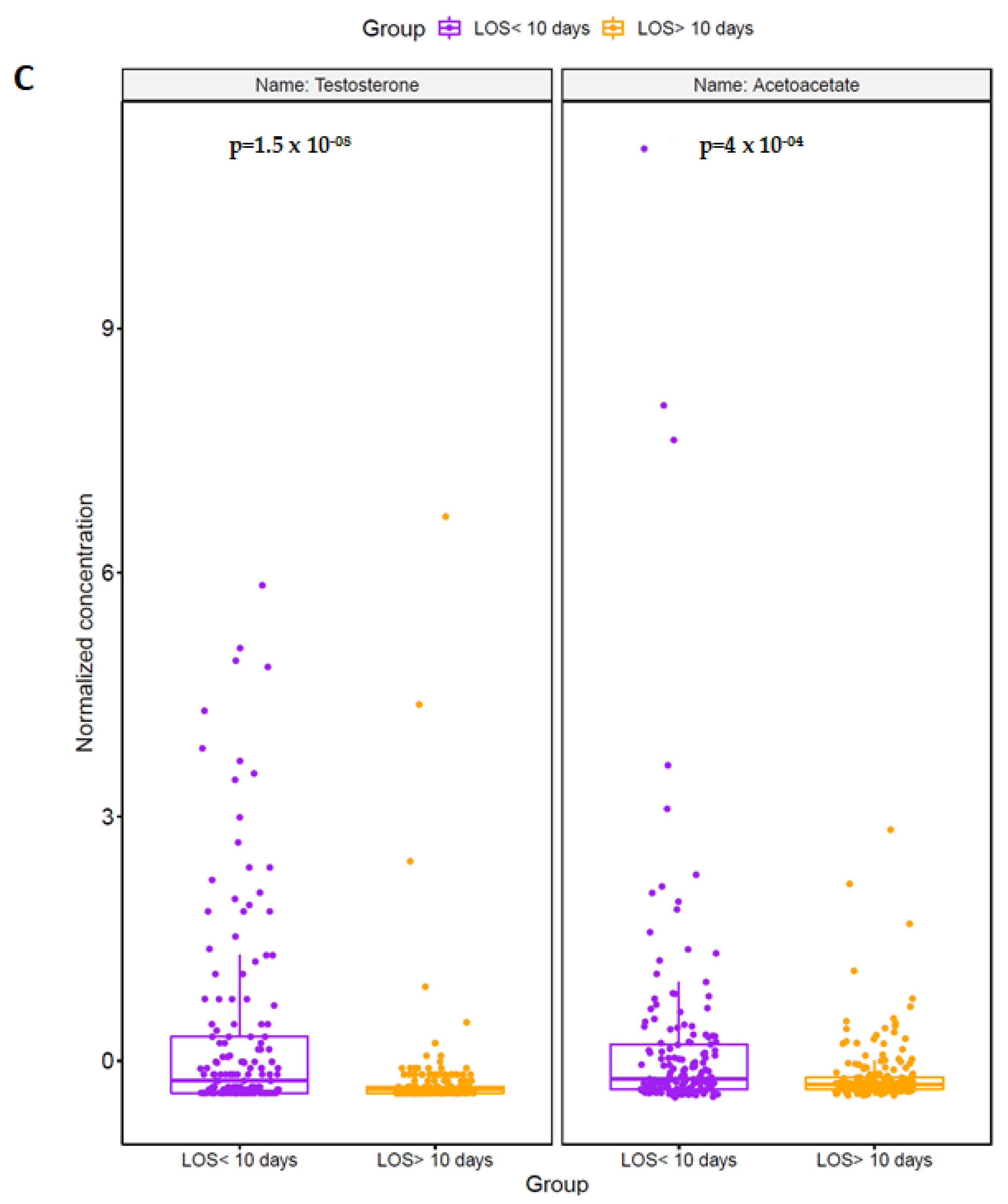
3.3. Trauma Patients with an ICU LOS ≥ 10 Days Exhibit a Distinct Metabolomic Profile in the Acute Injury Phase
3.4. Clinical Variables and the Acute Metabolic Response Can Discriminate between Patients with a Short or Extended ICU LOS
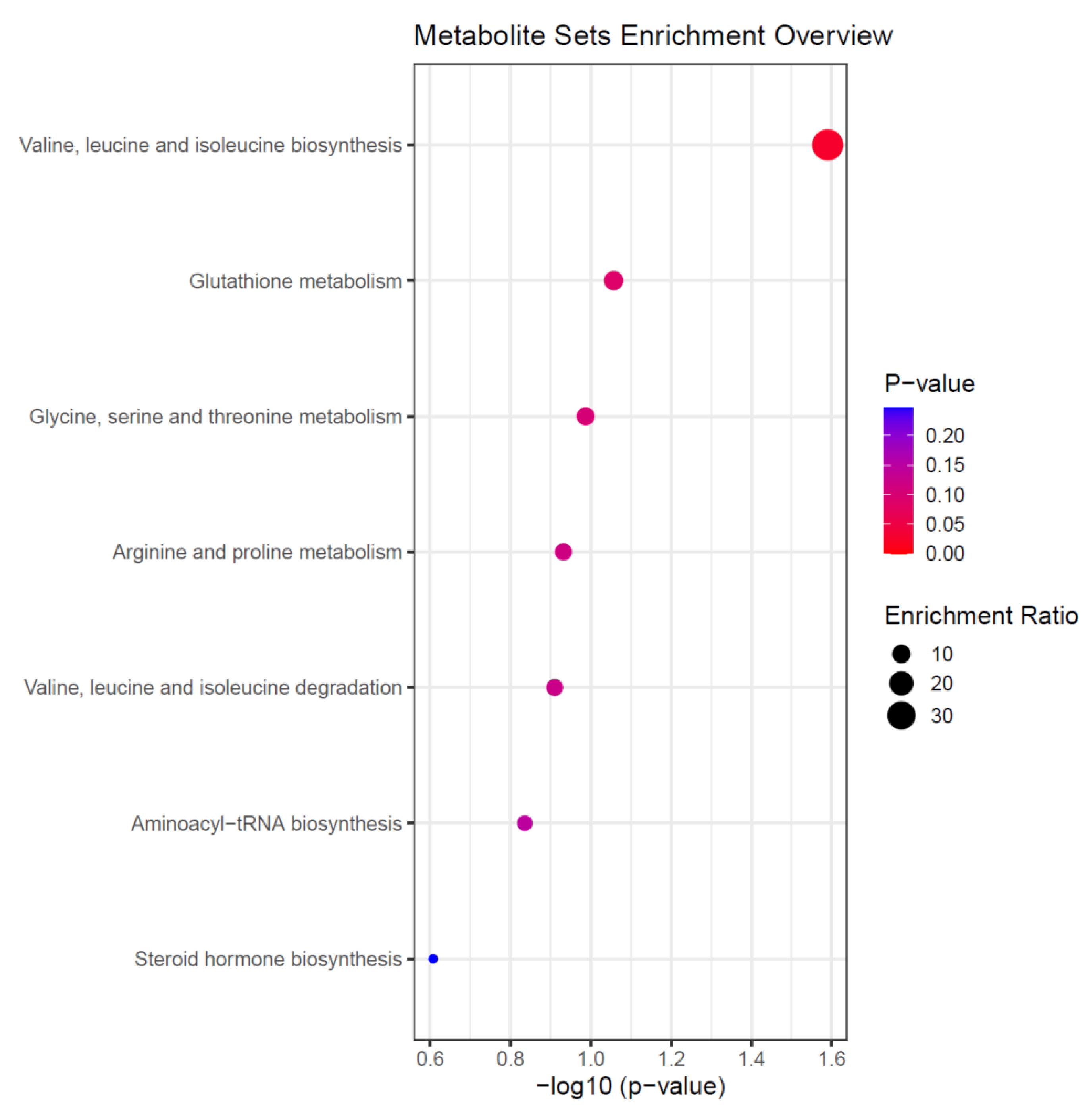
3.5. Altered Amino Acid Metabolism Is a Feature of the Acute Metabolic Response for Patients with a Prolonged ICU LOS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moran, C.G.; Lecky, F.; Bouamra, O.; Lawrence, T.; Edwards, A.; Woodford, M.; Willett, K.; Coats, T.J. Changing the System-Major Trauma Patients and Their Outcomes in the NHS (England) 2008–2017. EClinicalMedicine 2018, 2–3, 13–21. [Google Scholar] [CrossRef]
- Wong, D.T.; Gomez, M.; McGuire, G.P.; Kavanagh, B. Utilization of intensive care unit days in a Canadian medical-surgical intensive care unit. Crit. Care Med. 1999, 27, 1319–1324. [Google Scholar] [CrossRef] [PubMed]
- Wunsch, H.; Gershengorn, H.; Scales, D.C. Economics of ICU Organization and Management. Crit. Care Clin. 2012, 28, 25–37. [Google Scholar] [CrossRef]
- Pastores, S.M.; Dakwar, J.; Halpern, N.A. Costs of Critical Care Medicine. Crit. Care Clin. 2012, 2, 1–10. [Google Scholar] [CrossRef]
- Suistomaa, M.; Niskanen, M.; Kari, A.; Hynynen, M.; Takala, J. Customised prediction models based on APACHE II and SAPS II scores in patients with prolonged length of stay in the ICU. Intensive Care Med. 2002, 28, 479–485. [Google Scholar] [CrossRef]
- Ong, A.W.; Omert, L.A.; Vido, D.; Goodman, B.M.; Protetch, J.; Rodriguez, A.; Jeremitsky, E. Characteristics and outcomes of trauma patients with ICU lengths of stay 30 days and greater: A seven-year retrospective study. Crit. Care 2009, 13, R154. [Google Scholar] [CrossRef]
- Halpern, N.A.; Pastores, S.M. Critical care medicine in the United States 2000–2005: An analysis of bed numbers, occupancy rates, payer mix, and costs. Crit. Care Med. 2010, 38, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Rello, J.; Marshall, J.; Silva, E.; Anzueto, A.; Martin, C.D.; Moreno, R.; Lipman, J.; Gomersall, C.; Sakr, Y.; et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA-J. Am. Med. Assoc. 2009, 302, 2323–2329. [Google Scholar] [CrossRef]
- Kashkooe, A.; Yadollahi, M.; Pazhuheian, F. What factors affect length of hospital stay among trauma patients? A single-center study, Southwestern Iran. Chin. J. Traumatol. 2020, 23, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Böhmer, A.B.; Just, K.S.; Lefering, R.; Paffrath, T.; Bouillon, B.; Joppich, R.; Wappler, F.; Gerbershagen, M.U. Factors influencing lengths of stay in the intensive care unit for surviving trauma patients: A retrospective analysis of 30,157 cases. Crit. Care 2014, 18, R143. [Google Scholar] [CrossRef]
- Lazaridis, C.; Yang, M.; DeSantis, S.M.; Luo, S.T.; Robertson, C.S. Predictors of intensive care unit length of stay and intracranial pressure in severe traumatic brain injury. J. Crit. Care 2015, 30, 1258–1262. [Google Scholar] [CrossRef]
- Chalya, P.L.; Gilyoma, J.M.; Dass, R.M.; Mchembe, M.D.; Matasha, M.; Mabula, J.B.; Mbelenge, N.; Mahalu, W. Trauma admissions to the Intensive care unit at a reference hospital in Northwestern Tanzania. Scand. J. Trauma Resusc. Emerg. Med. 2011, 19, 61. [Google Scholar] [CrossRef] [PubMed]
- Lavoie, A.; Moore, L.; LeSage, N.; Liberman, M.; Sampalis, J.S. The Injury Severity Score or the New Injury Severity Score for predicting intensive care unit admission and hospital length of stay? Injury 2005, 36, 477–483. [Google Scholar] [CrossRef]
- Balogh, Z.J.; Varga, E.; Tomka, J.; Süveges, G.; Tóth, L.; Simonka, J.A. The new injury severity score is a better predictor of extended hospitalisation and intensive care unit admission than the injury severity score in patients with multiple orthopaedic injuries. J. Orthop. Trauma 2003, 17, 508–512. [Google Scholar] [CrossRef]
- Tamim, H.; Al Hazzouri, A.Z.; Mahfoud, Z.; Atoui, M.; El-Chemaly, S. The injury severity score or the new injury severity score for predicting mortality, intensive care unit admission and length of hospital stay: Experience from a university hospital in a developing country. Injury 2008, 39, 115–120. [Google Scholar] [CrossRef]
- Kahloul, M.; Bouida, W.; Boubaker, H.; Toumi, S.; Grissa, M.H.; Jaafar, A.; Louzi, M.; Boukef, R.; Gahbiche, M.; Nouira, S. Value of anatomic and physiologic scoring systems in outcome prediction of trauma patients. Eur. J. Emerg. Med. 2014, 21, 125–129. [Google Scholar] [CrossRef]
- Li, H.; Ma, Y.F. New injury severity score (NISS) outperforms injury severity score (ISS) in the evaluation of severe blunt trauma patients. Chin. J. Traumatol. 2021, 24, 261–265. [Google Scholar] [CrossRef]
- Huang, Y.-T.; Huang, Y.-H.; Hsieh, C.-H.; Li, C.-J.; Chiu, I.-M. Comparison of Injury Severity Score, Glasgow Coma Scale, and Revised Trauma Score in Predicting the Mortality and Prolonged ICU Stay of Traumatic Young Children: A Cross-Sectional Retrospective Study. Emerg. Med. Int. 2019, 2019, 5453624. [Google Scholar] [CrossRef]
- Nogueira, L.S.; de Sousa, R.M.C.; Domingues, C.A. Severity of trauma victims admitted in intensive care units: Comparative study among different indexes. Rev. Lat. Am. Enferm. 2009, 17, 1037–1042. [Google Scholar] [CrossRef][Green Version]
- Cohen, M.J.; Serkova, N.J.; Wiener-Kronish, J.; Pittet, J.F.; Niemann, C.U. 1H-NMR-based metabolic signatures of clinical outcomes in trauma patients-beyond lactate and base deficit. J. Trauma-Inj. Infect. Crit. Care 2010, 69, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Yi, L.; Shi, S.; Wang, Y.; Huang, W.; Xia, Z.A.; Xing, Z.; Peng, W.; Wang, Z. Serum Metabolic Profiling Reveals Altered Metabolic Pathways in Patients with Post-traumatic Cognitive Impairments. Sci. Rep. 2016, 6, 21320. [Google Scholar] [CrossRef]
- Orešič, M.; Posti, J.P.; Kamstrup-Nielsen, M.H.; Takala, R.S.K.; Lingsma, H.F.; Mattila, I.; Jäntti, S.; Katila, A.J.; Carpenter, K.; Ala-Seppälä, H.; et al. Human Serum Metabolites Associate With Severity and Patient Outcomes in Traumatic Brain Injury. EBioMedicine 2016, 12, 118–126. [Google Scholar] [CrossRef]
- Lusczek, E.R.; Muratore, S.L.; Dubick, M.A.; Beilman, G.J. Assessment of key plasma metabolites in combat casualties. J. Trauma Acute Care Surg. 2017, 82, 309–316. [Google Scholar] [CrossRef]
- Servia, L.; Jove, M.; Sol, J.; Pamplona, R.; Badia, M.; Montserrat, N.; Portero-Otin, M.; Trujillano, J. A prospective pilot study using metabolomics discloses specific fatty acid, catecholamine and tryptophan metabolic pathways as possible predictors for a negative outcome after severe trauma. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 56. [Google Scholar] [CrossRef]
- Lusczek, E.R.; Myers, C.; Popovsky, K.; Mulier, K.; Beilman, G.; Sawyer, R. Plasma metabolomics pilot study suggests age and sex-based differences in the metabolic response to traumatic injury. Injury 2018, 49, 2178–2185. [Google Scholar] [CrossRef]
- Parent, B.A.; Seaton, M.; Sood, R.F.; Gu, H.; Djukovic, D.; Raftery, D.; O’Keefe, G.E. Use of metabolomics to trend recovery and therapy after injury in critically ill trauma patients. JAMA Surg. 2016, 151, e160853. [Google Scholar] [CrossRef]
- Daley, M.; Dekaban, G.; Bartha, R.; Brown, A.; Stewart, T.C.; Doherty, T.; Fischer, L.; Holmes, J.; Menon, R.; Rupar, C.A.; et al. Metabolomics profiling of concussion in adolescent male hockey players: A novel diagnostic method. Metabolomics 2016, 12, 185. [Google Scholar] [CrossRef]
- Cyr, A.; Zhong, Y.; Reis, S.E.; Namas, R.A.; Amoscato, A.; Zuckerbraun, B.; Sperry, J.; Zamora, R.; Vodovotz, Y.; Billiar, T.R. Analysis of the Plasma Metabolome after Trauma, Novel Circulating Sphingolipid Signatures, and In-Hospital Outcomes. J. Am. Coll. Surg. 2021, 232, 276–287. [Google Scholar] [CrossRef]
- Langley, R.J.; Tsalik, E.L.; Van Velkinburgh, J.C.; Glickman, S.W.; Rice, B.J.; Wang, C.; Chen, B.; Carin, L.; Suarez, A.; Mohney, R.P.; et al. Sepsis: An integrated clinico-metabolomic model improves prediction of death in sepsis. Sci. Transl. Med. 2013, 5. [Google Scholar] [CrossRef]
- Foster, M.A.; Taylor, A.E.; Hill, N.E.; Bentley, C.; Bishop, J.; Gilligan, L.C.; Shaheen, F.; Bion, J.; Fallowfield, J.L.; Woods, D.R.; et al. Mapping the Steroid Response to Major Trauma From Injury to Recovery: A Prospective Cohort Study. J. Clin. Endocrinol. Metab. 2020, 105, 925–937. [Google Scholar] [CrossRef]
- Gentile, L.F.; Cuenca, A.G.; Efron, P.A.; Ang, D.; Bihorac, A.; McKinley, B.A.; Moldawer, L.L.; Moore, F.A. Persistent inflammation and immunosuppression: A common syndrome and new horizon for surgical intensive care. J. Trauma Acute Care Surg. 2012, 72, 1491–1501. [Google Scholar] [CrossRef]
- Tiziani, S.; Emwas, A.H.; Lodi, A.; Ludwig, C.; Bunce, C.M.; Viant, M.R.; Günther, U.L. Optimised metabolite extraction from blood serum for 1H nuclear magnetic resonance spectroscopy. Anal. Biochem. 2008, 377, 16–23. [Google Scholar] [CrossRef]
- Young, S.P.; Kapoor, S.R.; Viant, M.R.; Byrne, J.J.; Filer, A.; Buckley, C.D.; Kitas, G.D.; Raza, K. The impact of inflammation on metabolomic profiles in patients with arthritis. Arthritis Rheum. 2013, 65, 2015–2023. [Google Scholar] [CrossRef]
- Kapoor, S.R.; Filer, A.; Fitzpatrick, M.A.; Fisher, B.A.; Taylor, P.C.; Buckley, C.D.; McInnes, I.; Raza, K.; Young, S.P. Metabolic profiling predicts response to anti-tumor necrosis factor α therapy in patients with rheumatoid arthritis. Arthritis Rheum. 2013, 65, 1448–1456. [Google Scholar] [CrossRef]
- Ludwig, C.; Günther, U.L. MetaboLab-advanced NMR data processing and analysis for metabolomics. BMC Bioinform. 2011, 12, 366. [Google Scholar] [CrossRef]
- Dieterle, F.; Ross, A.; Schlotterbeck, G.; Senn, H. Probabilistic quotient normalisation as robust method to account for dilution of complex biological mixtures. Application in1H NMR metabonomics. Anal. Chem. 2006, 78, 4281–4290. [Google Scholar] [CrossRef]
- Parsons, H.M.; Ludwig, C.; Günther, U.L.; Viant, M.R. Improved classification accuracy in 1- and 2-dimensional NMR metabolomics data using the variance stabilising generalised logarithm transformation. BMC Bioinform. 2007, 8, 234. [Google Scholar] [CrossRef]
- Leek, J.T.; Johnson, W.E.; Parker, H.S.; Jaffe, A.E.; Storey, J.D. The SVA package for removing batch effects and other unwanted variation in high-throughput experiments. Bioinformatics 2012, 28, 882–883. [Google Scholar] [CrossRef]
- Wishart, D.S.; Feunang, Y.D.; Marcu, A.; Guo, A.C.; Liang, K.; Vázquez-Fresno, R.; Sajed, T.; Johnson, D.; Li, C.; Karu, N.; et al. HMDB 4.0: The human metabolome database for 2018. Nucleic Acids Res. 2018, 46, D608–D617. [Google Scholar] [CrossRef]
- Chong, J.; Soufan, O.; Li, C.; Caraus, I.; Li, S.; Bourque, G.; Wishart, D.S.; Xia, J. MetaboAnalyst 4.0: Towards more transparent and integrative metabolomics analysis. Nucleic Acids Res. 2018, 46, W486–W494. [Google Scholar] [CrossRef]
- Monteleone, P.; Monteleone, A.M.; Troisi, J.; Dalle Grave, R.; Corrivetti, G.; Calugi, S.; Scala, G.; Patriciello, G.; Zanetti, A.; Maj, M. Metabolomics signatures of acutely ill and short-term weight recovered women with anorexia nervosa. Mol. Psychiatry 2019, 26, 3980–3991. [Google Scholar] [CrossRef]
- Orhon, R.; Eren, S.H.; Karadayi, S.; Korkmaz, I.; Coskun, A.; Eren, M.; Katrancioglu, N. Comparison of trauma scores for predicting mortality and morbidity on trauma patients. Turk. J. Trauma Emerg. Surg. 2014, 20, 258–264. [Google Scholar] [CrossRef]
- Peltz, E.D.; D’Alessandro, A.; Moore, E.E.; Chin, T.; Silliman, C.C.; Sauaia, A.; Hansen, K.C.; Banerjee, A. Pathologic metabolism: An exploratory study of the plasma metabolome of critical injury. J. Trauma Acute Care Surg. 2015, 78, 742–751. [Google Scholar] [CrossRef] [PubMed]
- Horn, D.L.; Bettcher, L.F.; Navarro, S.L.; Pascua, V.; Neto, F.C.; Cuschieri, J.; Raftery, D.; O’Keefe, G.E. Persistent metabolomic alterations characterise chronic critical illness after severe trauma. J. Trauma Acute Care Surg. 2021, 90, 35–45. [Google Scholar] [CrossRef]
- D’Alessandro, A.; Moore, H.B.; Moore, E.E.; Reisz, J.A.; Wither, M.J.; Ghasasbyan, A.; Chandler, J.; Silliman, C.C.; Hansen, K.C.; Banerjee, A. Plasma succinate is a predictor of mortality in critically injured patients. J. Trauma Acute Care Surg. 2017, 83, 491–495. [Google Scholar] [CrossRef]
- Wilcox, G. Insulin and insulin resistance. Clin. Biochem. Rev. 2005, 26, 19–39. [Google Scholar]
- Bessey, P.Q.; Brooks, D.C.; Black, P.R.; Aoki, T.T.; Wilmore, D.W. Epinephrine acutely mediates skeletal muscle insulin resistance. Surgery 1983, 94, 172–179. [Google Scholar]
- Desborough, J.P. The stress response to trauma and surgery. Br. J. Anaesth 2000, 85, 109–117. [Google Scholar] [CrossRef]
- Mizock, B.A. Alterations in fuel metabolism in critical illness: Hyperglycaemia. Best Pract. Res. Clin. Endocrinol. Metab. 2001, 15, 533–551. [Google Scholar] [CrossRef]
- Thorell, A.; Rooyackers, O.; Myrenfors, P.; Soop, M.; Nygren, J.; Ljungqvist, O.H. Intensive insulin treatment in critically ill trauma patients normalises glucose by reducing endogenous glucose production. J. Clin. Endocrinol. Metab. 2004, 89, 5382–5386. [Google Scholar] [CrossRef]
- Kushimoto, S.; Akaishi, S.; Sato, T.; Nomura, R.; Fujita, M.; Kudo, D.; Kawazoe, Y.; Yoshida, Y.; Miyagawa, N. Lactate, a useful marker for disease mortality and severity but an unreliable marker of tissue hypoxia/hypoperfusion in critically ill patients. Acute Med. Surg. 2016, 3, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, G.; Bellomo, R.; Bakker, J. The ten pitfalls of lactate clearance in sepsis. Instensive Care Med. 2019, 45, 82–85. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, K.; Zeng, J.; Li, W.; Peng, J.; Zhou, Z.; Deng, P.; Sun, M.; Yang, H.; Li, S.; et al. Metabolic dynamics in critically injured patients: A prospective cohort study integrated with 1H NMR metabolomics. Asia Pac. J. Clin. Nutr. 2019, 28, 411–418. [Google Scholar] [CrossRef]
- Blaise, B.J.; Gouel-Chéron, A.; Floccard, B.; Monneret, G.; Allaouchiche, B. Metabolic phenotyping of traumatised patients reveals a susceptibility to sepsis. Anal. Chem. 2013, 85, 10850–10855. [Google Scholar] [CrossRef]
- Barton, D.J.; Kumar, R.G.; McCullough, E.H.; Galang, G.; Arenth, P.M.; Berga, S.L.; Wagner, A.K. Persistent hypogonadotropic hypogonadism in men after severe traumatic brain injury: Temporal hormone profiles and outcome prediction. J. Head Trauma Rehabil. 2016, 31, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Young, T.P.; Hoaglin, H.M.; Burke, D.T. The role of serum testosterone and TBI in the in-patient rehabilitation setting. Brain Inj. 2007, 21, 645–649. [Google Scholar] [CrossRef]
- Almoosa, K.F.; Gupta, A.; Pedroza, C.; Watts, N.B. Low testosterone levels are frequent in patients with acute respiratory failure and are associated with poor outcomes. Endocr. Pract. 2014, 20, 1057–1063. [Google Scholar] [CrossRef] [PubMed]
- Rastrelli, G.; Di Stasi, V.; Inglese, F.; Beccaria, M.; Garuti, M.; Di Costanzo, D.; Spreafico, F.; Greco, G.F.; Cervi, G.; Pecoriello, A.; et al. Low testosterone levels predict clinical adverse outcomes in SARS-CoV-2 pneumonia patients. Andrology 2021, 9, 88–98. [Google Scholar] [CrossRef]
- Al-Tarrah, K.; Moiemen, N.; Lord, J. The influence of sex steroid hormones on the response to trauma and burn injury. Burn. Trauma 2017, 5, 29. [Google Scholar] [CrossRef]
- Preiser, J.C.; Ichai, C.; Orban, J.C.; Groeneveld, A.B.J. Metabolic response to the stress of critical illness. Br. J. Anaesth 2014, 113, 945–954. [Google Scholar] [CrossRef]
- Li, H.; Guo, Y.; Yang, Z.; Roy, M.; Guo, Q. The efficacy and safety of oxandrolone treatment for patients with severe burns: A systematic review and meta-analysis. Burns 2016, 42, 717–727. [Google Scholar] [CrossRef]
- Hausmann, D.F.; Nutz, V.; Rommelsheim, K.; Caspari, R.; Mosebach, K.O. Anabolic Steroids in Polytrauma Patients. Influence on Renal Nitrogen and Amino Acid Losses: A Double-Blind Study. J. Parenter Enter. Nutr. 1990, 14, 111–114. [Google Scholar] [CrossRef]
- Mosebach, K.O.; Hausmann, D.; Caspari, R.; Stoeckel, H. Deca-Durabolin® and parenteral nutrition in post-traumatic patients. Acta Endocrinol. Suppl. 1985, 110, 60–69. [Google Scholar] [CrossRef]
- Bulger, E.M.; Jurkovich, G.J.; Farver, C.L.; Klotz, P.; Maier, R.V. Oxandrolone does not improve outcome of ventilator dependent surgical patients. Ann. Surg. 2004, 240, 472–480. [Google Scholar] [CrossRef]
- White, H.; Venkatesh, B. Clinical review: Ketones and brain injury. Crit. Care 2011, 15, 219. [Google Scholar] [CrossRef]
- Stubbs, B.J.; Koutnik, A.P.; Volek, J.S.; Newman, J.C. From bedside to battlefield: Intersection of ketone body mechanisms in geroscience with military resilience. GeroScience 2020, 43, 1071–1081. [Google Scholar] [CrossRef]
- Bradshaw, P.C.; Seeds, W.A.; Miller, A.C.; Mahajan, V.R.; Curtis, W.M. COVID-19: Proposing a Ketone-Based Metabolic Therapy as a Treatment to Blunt the Cytokine Storm. Oxid. Med. Cell Longev. 2020, 2020, 6401341. [Google Scholar] [CrossRef]
- Rinehart, D.; Johnson, C.H.; Nguyen, T.; Ivanisevic, J.; Benton, H.P.; Lloyd, J.; Arkin, A.; Deutschbauer, A.M.; Patti, G.J.; Siuzdak, G. Metabolomic data streaming for biology-dependent data acquisition. Nat. Biotechnol. 2014, 32, 524–527. [Google Scholar] [CrossRef]
- Karl, J.P.; Margolis, L.M.; Murphy, N.E.; Carrigan, C.T.; Castellani, J.W.; Madslien, E.H.; Teien, H.; Martini, S.; Montain, S.J.; Pasiakos, S.M. Military training elicits marked increases in plasma metabolomic signatures of energy metabolism, lipolysis, fatty acid oxidation, and ketogenesis. Physiol. Rep. 2017, 5, e13407. [Google Scholar] [CrossRef] [PubMed]
- Reijnen, A.; Geuze, E.; Vermetten, E. The effect of deployment to a combat zone on testosterone levels and the association with the development of posttraumatic stress symptoms: A longitudinal prospective Dutch military cohort study. Psychoneuroendocrinology 2015, 51, 525–533. [Google Scholar] [CrossRef]
- Warren, H.S.; Elson, C.M.; Hayden, D.L.; Schoenfeld, D.A.; Cobb, J.P.; Maier, R.V.; Moldawer, L.L.; Moore, E.E.; Harbrecht, B.G.; Pelak, K.; et al. A genomic score prognostic of outcome in trauma patients. Mol. Med. 2009, 15, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Cuenca, A.G.; Gentile, L.F.; Lopez, M.C.; Ungaro, R.; Liu, H.; Xiao, W.; Seok, J.; Mindrinos, M.N.; Ang, D.; Baslanti, T.O.; et al. Development of a genomic metric that can be rapidly used to predict clinical outcome in severely injured trauma patients. Crit. Care Med. 2013, 41, 1175–1185. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Patients (N = 55) | ICU LOS < 10 Days (N = 29) | ICU LOS ≥ 10 Days (N = 26) | p-Value |
|---|---|---|---|---|
| Age, years | 29 (18–50) | 27.5 (18–49) | 31 (21–49.5) | 0.17 |
| Male, n (%) | 55 (100) | 29 (100) | 26 (100) | N/A |
| Mechanism of Injury Explosive, n (%) GSW, n (%) Electrical, n (%) Blunt, n (%) Penetration, n (%) | 31 (56.3 %) 8 (14.5 %) 1 (1.8 %) 13 (23.6%) 2 (3.6 %) | 16 (55.2%) 5 (17.2 %) 0 7 (24.1%) 1 (3.5%) | 15 (57.7%) 3 (11.5%) 1 (3.8 %) 6 (23.1 %) 1 (3.9%) | NA |
| ISS | 25.5 (9–75) | 21 (9–38) | 30 (13–75) | 0.005 |
| NISS | 37.3 (16–75) | 34.4 (17–59) | 40.6 (16–75) | 0.07 |
| GCS | 10.3 (3–15) | 10.7 (3–15) | 9.9 (3–15) | 0.61 |
| SOFA (Day 1) | 8.3 (0–17) | 15 (7.72–17) | 8.6 (0–15) | 0.41 |
| APACHE II (Day 1) | 20.3 (0–34) | 17.9 (0–29) | 22.4 (7–34) | 0.04 |
| SAPS II (Day 1) | 42.2 (0–69) | 38.6 (11–62) | 44.7 (0–69) | 0.21 |
| TRISS (Day 1) | 77.13 (2.55–99.4) | 78.23 (2.55–99.4) | 75.9 (13.27–98.6) | 0.76 |
| RTS (Day 1) | 6.3 (2.6–7.8) | 6.4 (2.91–7.84) | 6.1 (2.63–7.84) | 0.55 |
| Ventilator days | 7.8 (0–25) | 3.3 (0–10) | 12.9 (4–25) | <0.0001 |
| Operative procedures | 5.8 (0–24) | 5 (0–15) | 6.8 (0–24) | 0.12 |
| ICU LOS | 10 (0–34) | 4.6 (0–9) | 16.2 (10–33) | <0.0001 |
| Hospital LOS | 46 (7–217) | 34 (7–72) | 59 (17–217) | 0.02 |
| Feature | AUROC | Confidence Interval | p Value |
|---|---|---|---|
| NISS | 0.69434 | 0.639–0.748 | 2.62 × 10−12 |
| Testosterone | 0.668566 | 0.612–0.728 | 3.27 × 10−7 |
| Dimethyl sulfone | 0.636886 | 0.577–0.694 | 0.000234 |
| Cadaverine | 0.628626 | 0.55–0.682 | 2.25 × 10−5 |
| Isoleucine | 0.625872 | 0.568–0.68 | 8.30 × 10−5 |
| Acetoacetate | 0.609176 | 0.558–0.675 | 0.000214 |
| Urea | 0.595153 | 0.536–0.652 | 2.64 × 10−5 |
| Syringate | 0.591759 | 0.537–0.645 | 0.000314 |
| Acetone | 0.589022 | 0.434–0.621 | 0.000523 |
| Xylitol | 0.583723 | 0.522–0.64 | 0.000509 |
| Creatinine | 0.552331 | 0.512-0.612 | 0.000426 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acharjee, A.; Hazeldine, J.; Bazarova, A.; Deenadayalu, L.; Zhang, J.; Bentley, C.; Russ, D.; Lord, J.M.; Gkoutos, G.V.; Young, S.P.; et al. Integration of Metabolomic and Clinical Data Improves the Prediction of Intensive Care Unit Length of Stay Following Major Traumatic Injury. Metabolites 2022, 12, 29. https://doi.org/10.3390/metabo12010029
Acharjee A, Hazeldine J, Bazarova A, Deenadayalu L, Zhang J, Bentley C, Russ D, Lord JM, Gkoutos GV, Young SP, et al. Integration of Metabolomic and Clinical Data Improves the Prediction of Intensive Care Unit Length of Stay Following Major Traumatic Injury. Metabolites. 2022; 12(1):29. https://doi.org/10.3390/metabo12010029
Chicago/Turabian StyleAcharjee, Animesh, Jon Hazeldine, Alina Bazarova, Lavanya Deenadayalu, Jinkang Zhang, Conor Bentley, Dominic Russ, Janet M. Lord, Georgios V. Gkoutos, Stephen P. Young, and et al. 2022. "Integration of Metabolomic and Clinical Data Improves the Prediction of Intensive Care Unit Length of Stay Following Major Traumatic Injury" Metabolites 12, no. 1: 29. https://doi.org/10.3390/metabo12010029
APA StyleAcharjee, A., Hazeldine, J., Bazarova, A., Deenadayalu, L., Zhang, J., Bentley, C., Russ, D., Lord, J. M., Gkoutos, G. V., Young, S. P., & Foster, M. A. (2022). Integration of Metabolomic and Clinical Data Improves the Prediction of Intensive Care Unit Length of Stay Following Major Traumatic Injury. Metabolites, 12(1), 29. https://doi.org/10.3390/metabo12010029