1. Introduction
Deep venous thrombosis (DVT) is a common disease associated with significant morbidity and mortality, and represents the third most common cause of death, after cardiovascular disease and stroke [
1,
2]. Although most events evolve without complications, DVT can be complicated with a life-threatening pulmonary embolism (PE) [
3], and approximately one-third of patients could develop moderate-to-severe post-thrombotic syndrome (PTS) [
4]. The veins of the lower limbs are among the most commonly affected, but other sites can be compromised as well [
5]. Cerebral venous thrombosis (CVT), although not very prevalent, usually occurs in young adults, especially in women under estrogen hormonal therapy, with a mortality around 10%, and up to 80% of patients recover with no neurological deficit [
6].
DVT is a multifactorial disease and there are several risk factors that contribute to its development, including acquired and genetic factors [
6,
7]. Approximately 10% of individuals who have a first unprovoked episode of DVT will present a recurrent event in the first year, after anticoagulation withdrawal [
4]. Even those patients with provoked DVT showed a high risk of recurrence, as demonstrated in studies of extended anticoagulation [
8]. Recent guidelines indicate definitive anticoagulation for male patients with unprovoked DVT or for those diagnosed with thrombotic antiphospholipid syndrome (APS) [
9,
10]. However, in other situations, there is no clear definition regarding whether anticoagulation should be interrupted or not. This decision must consider the risk–benefits of anticoagulation, bleeding, and DVT recurrence. Thus, it is very important to discover the molecules and pathways involved in the process, and although there is an increasing number of research publications on DVT, these fields remain unexplored.
In this sense, the search for biomarkers that could identify patients with a higher risk of recurrence is a challenge. Higher levels of D-dimer are considered a marker of an increased risk of recurrence, and this measurement is included in Vienna, DASH, and Herdoo2 scores [
11]. On the other hand, increased circulating metabolites, such as hyperhomocysteinemia, were thought to be part of the pathophysiologic link between B-group vitamins and venous thrombosis, but this remains controversial as well [
12]. Emerging technologies, such as metabolomics, allow for an untargeted and thus unbiased analysis of the molecular underpinnings of the disease [
13], leading to a better understanding of the disease’s pathophysiology. Metabolomics seek an analytical description of complex biological samples, aiming to characterize and quantify all the small molecules measurable in such samples [
14]. Metabonomics broadly aim to measure the global, dynamic multiparametric metabolic response of living systems to biological stimuli or genetic modifications [
15]. In practice, the terms metabolomics and metabonomics are often used interchangeably, and the analytical and modelling procedures are the same [
14]. Here, we refer to both as metabolomics. This omics discipline enables the identification and quantification of the end products of cellular metabolism and allows us to understand the systemic changes in the complex multicellular systems.
Magnetic resonance (NMR) spectroscopy, in an untargeted approach, provides information on metabolites in a given sample [
16]; however, for DVT, research is poorly explored [
17]. Preliminary studies in animal models by NMR showed metabolic dysregulations on energy metabolism, sphingolipid, and adenosine metabolism [
18]. Changes in metabolic pathways, including carbohydrates’, lipids’, and amino acids’ metabolism have been reported to be affected immediately after thrombosis [
19]. Studies using mass spectrometry (MS) showed decreased acylcarnitines in the blood samples of patients with DVT and in those with a high risk of PE [
18,
19]. These findings suggest that carnitine metabolism may be dysregulated in venous thromboembolism (VTE), and provide evidence that metabolomic platforms might have the potential to be used to stratify the risks of patients with this condition [
15]. An early and correct diagnosis of DVT is necessary for a pertinent treatment decision and a better result. The stages of clot maturation and resolution are not completely elucidated and defined, and there is no accurate biomarker of clot chronicity. The rise of VTE incidence, especially in the elderly, necessitates new diagnostic and prognostic biomarkers. However, it is also necessary to clarify the collecting time of biological samples to understand when the metabolites appear and when they become indicative of a diagnosis [
20].
This work aimed to evaluate patients retrospectively, using a metabolomic point of view to find metabolic alterations, even months after an acute DVT episode.
3. Discussion
Research efforts are currently seeking alternative blood biomarkers that are capable of improving patient diagnosis, treatment, and stratification, identifying those patients that may benefit from different treatment schedules, and particularly in thrombosis, extended anticoagulation [
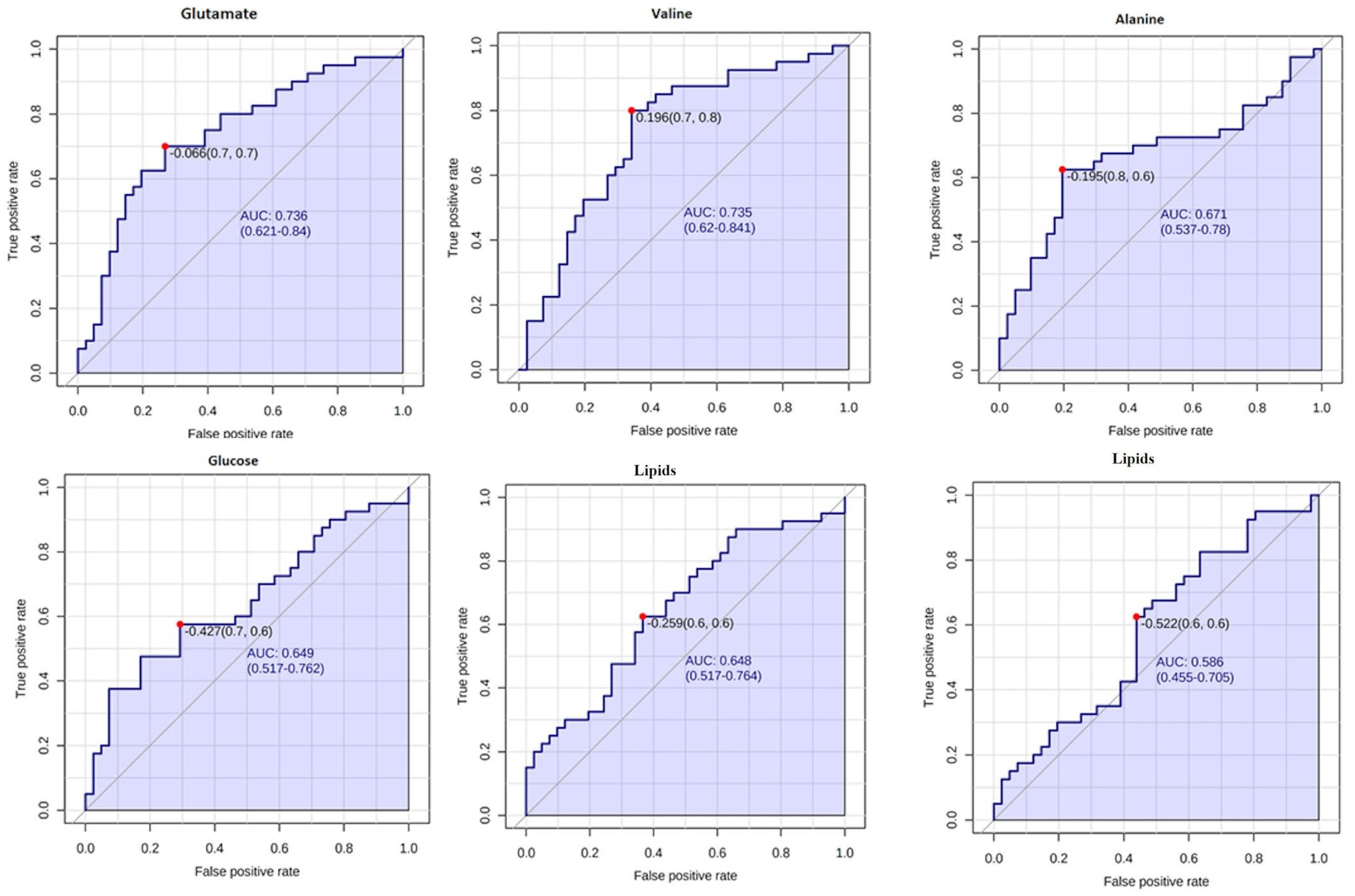
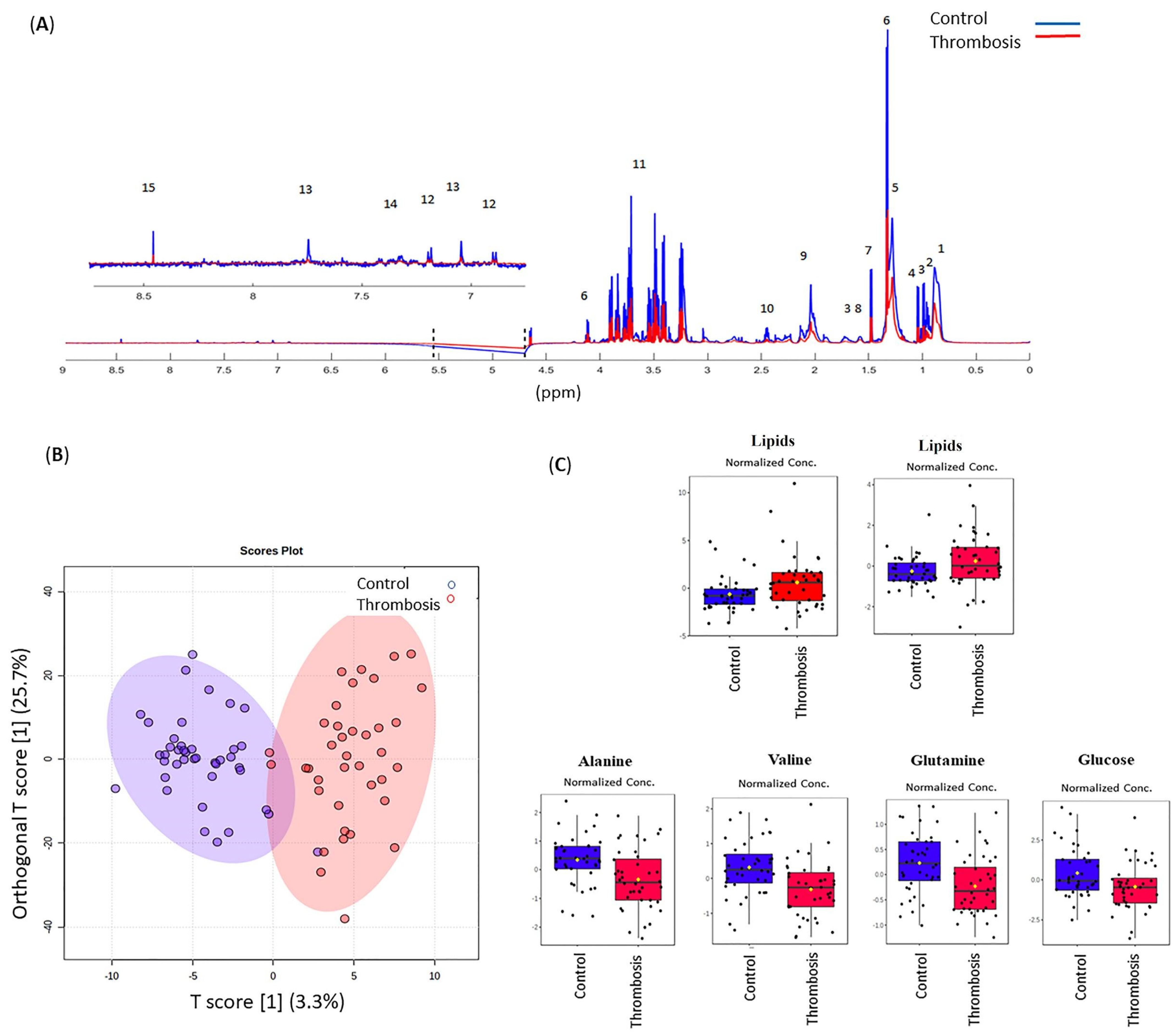
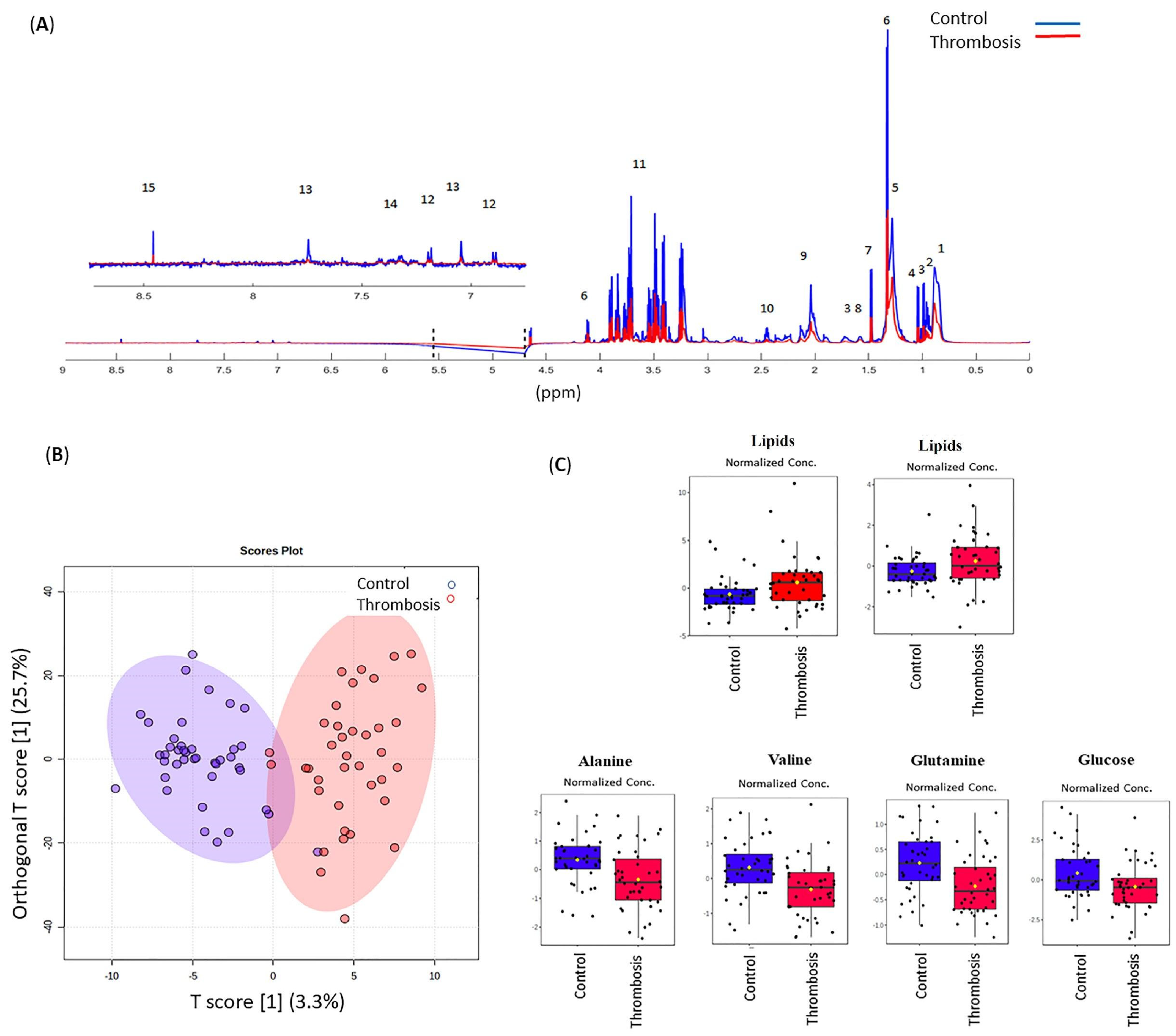
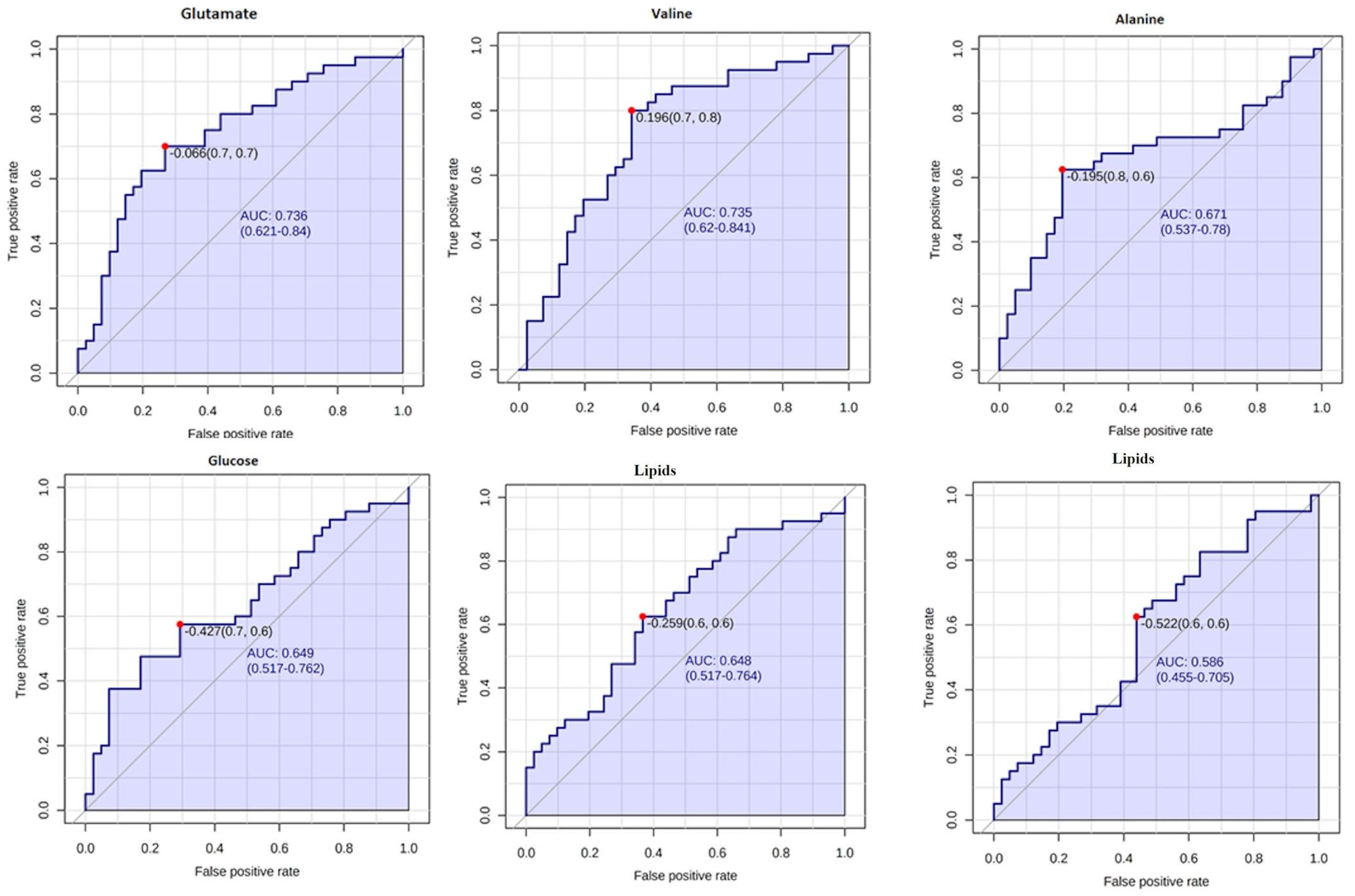
18]. In this study, using a metabolomic approach, we observed global differences among the serum metabolic patterns of thrombotic patients and controls. As seen in
Figure 1, discriminatory metabolites such as lipids, glucose, alanine, glutamine, and valine were identified, and showed significant differences between patients and controls. The area-under-the-curve (AUC) values of the receiver operating characteristic (ROC) curves were compared for every single individual metabolite. Glutamate and valine were the most influential metabolites in discriminating between the thrombotic and control groups. Even though this is not a study with a diagnostic objective, and as there is no predictive model or independent cohort testing in this study, we indicate that this is one of the caveats of this study.
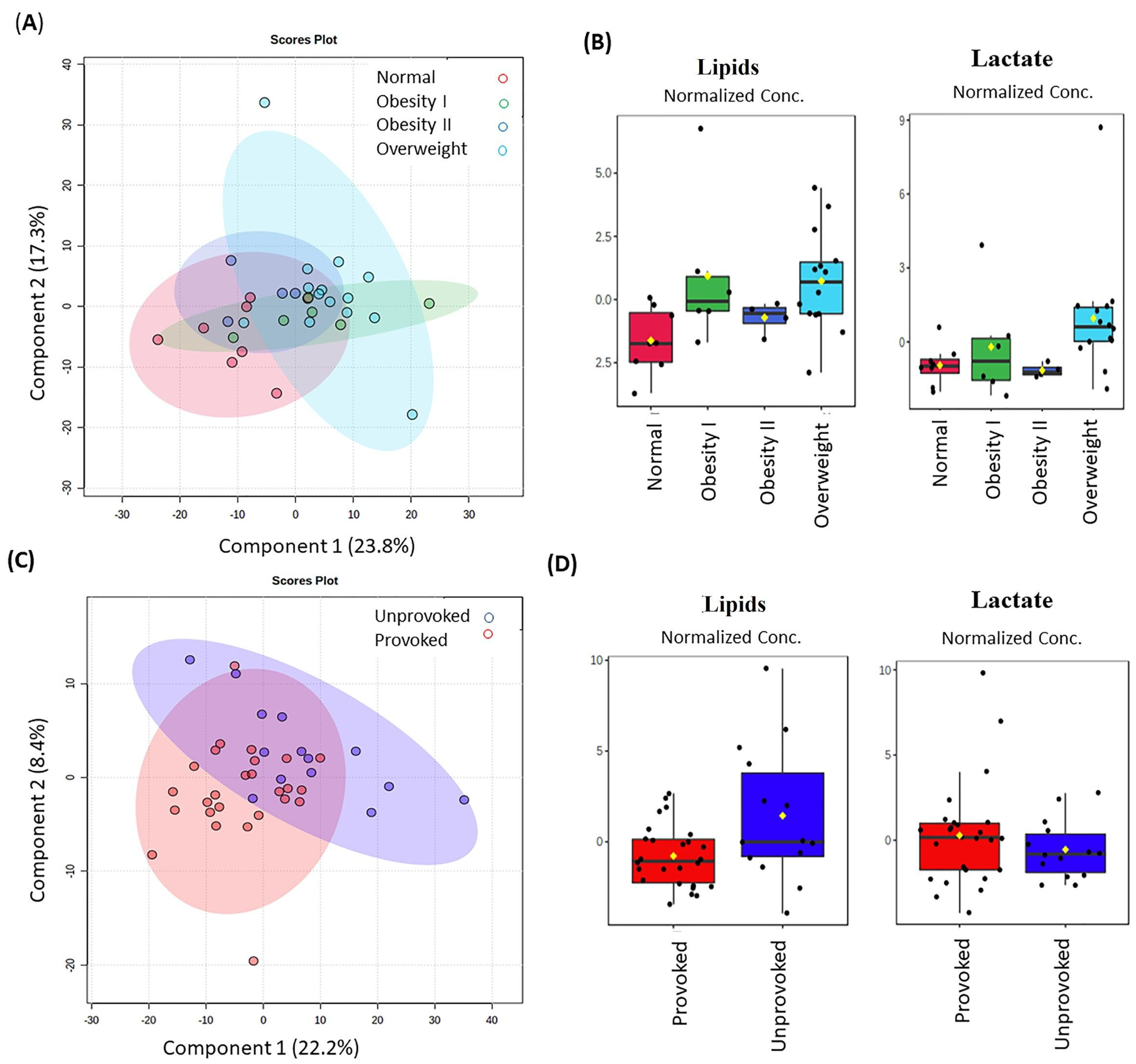
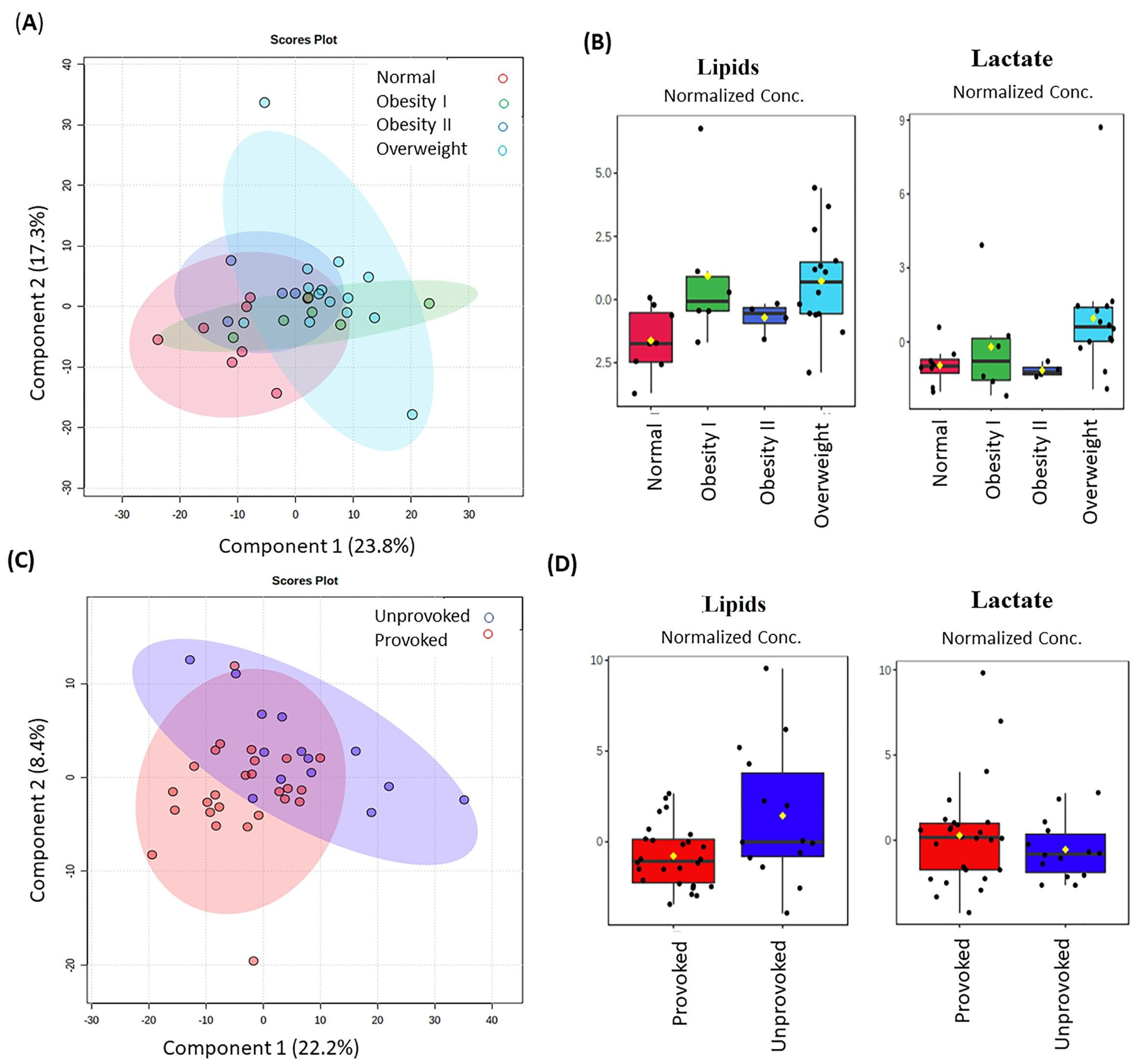
Common variables, called confounders, such as age, sex, lifestyle, BMI, estrogen use, and others, might explain the alterations of lipids in thrombotic patients [
22]. However, it is important to note that significant differences between patients and controls were observed only regarding BMI and estrogen use. When we explored the intrinsic differences related to the BMI condition between the groups, alterations in lipids (from δ 0.89 to δ 1.31) and lactate (at δ 1.32) were observed in overweight and obesity I patients.
As the blood samples were collected months after the thrombotic episode, we can only speculate that if lipid alteration was present before the thrombosis, it could interfere with hemostasis and inflammation [
23]. This can be demonstrated by changes in levels of hemostatic factors [
24] and C-reactive proteins (CRP) [
25]. Otherwise, even if these alterations occurred a long time after the venous episode, they differentiate patients and controls. The role of these alterations for DVT complications, such as recurrence, can be investigated in a study with longer follow-ups and with a higher number of patients.
Lactate was also found to be important for the provoked thrombosis. This alteration was previously reported as caused by a number of conditions, including shock, cardiac arrest, trauma, ischemia, diabetic ketoacidosis, genetic disorders, and other conditions, which is an indicator of a non-specific factor unless thoughtfully coupled with the overall clinical picture [
26]. Maekawa et al. identified lactate as one of the blood metabolites reflecting fresh venous thrombus in a jugular model of venous thrombosis in 2019, probably as a result of active glycolysis of thrombus cellular components, predominantly erythrocytes [
27]. As our samples were not obtained during the acute phase, and were obtained even months after the thrombotic episode, these results nonetheless demonstrated that lactate alterations appear to remain for a long time.
As mentioned above, in our cohort of patients, hormonal contraceptives and obesity were the principal acquired risk factors. Normally, obesity interacts with other environmental or genetic factors, increasing the risk of thrombosis [
28]. Particularly, central and abdominal obesity is associated with increased thrombin formation and decreased fibrinolysis [
29]. On the other hand, one of the common risk factors for thrombosis in women is the use of hormonal contraceptives. The contraceptives showed a strong association with thrombosis due to their estrogenic component, as estrogen increases the levels of coagulation factors and decreases the levels of anticoagulant proteins such as protein S [
29,
30]. Hormonal contraceptive use increases the risk of CVT in women of reproductive age seven-fold when compared to those not using this method of contraception [
31]. Of the 19 patients that presented CVT, 75% were using hormonal contraceptives, emphasizing the importance of this risk factor in this population. However, when blood samples for metabolomic analysis were collected, hormonal use was already discontinued.
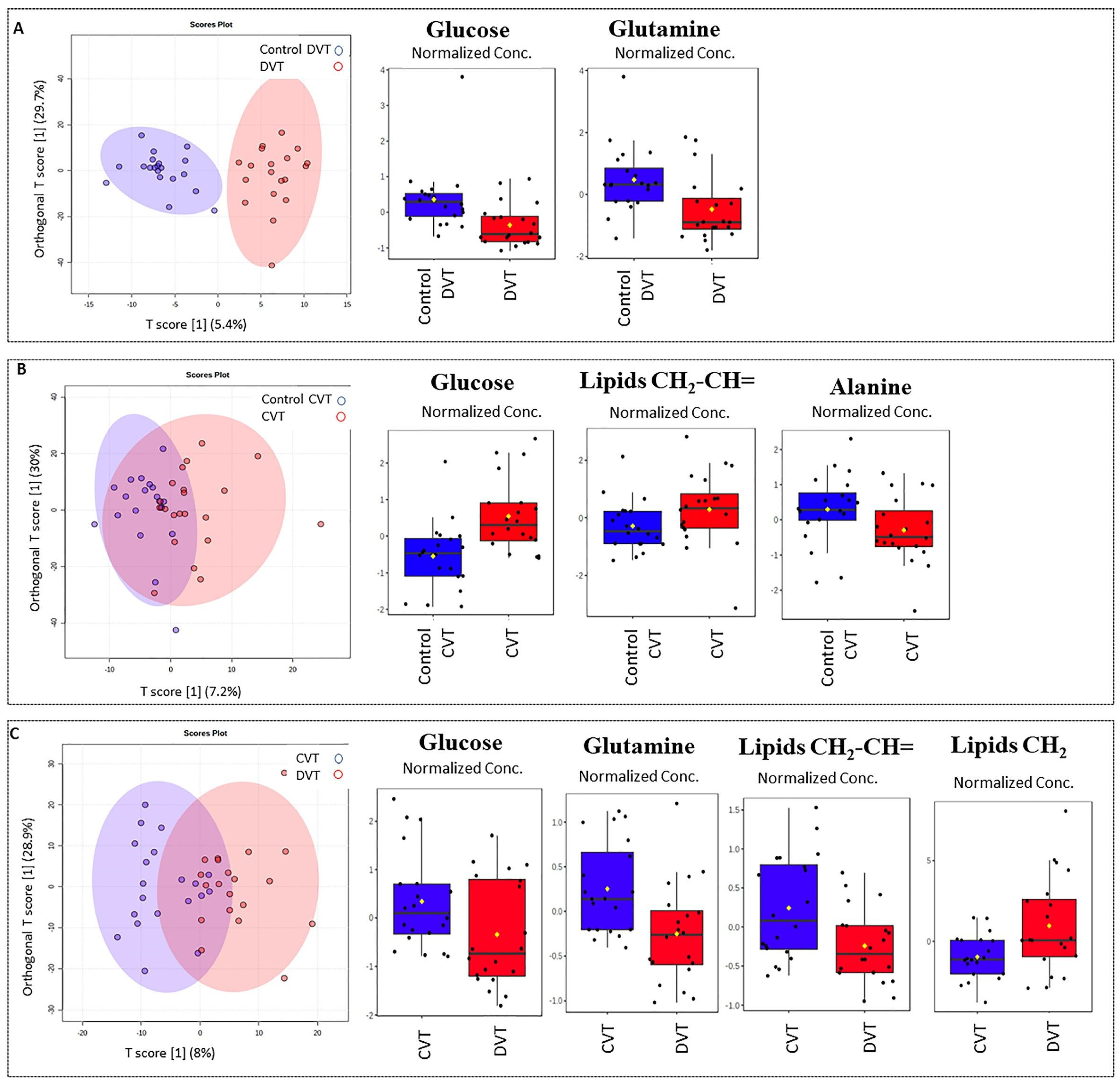
A comparison between thrombotic patients and controls showed differences in blood serum lipids (fatty acyls, especially, in very-low-density lipoproteins, VLDL) (
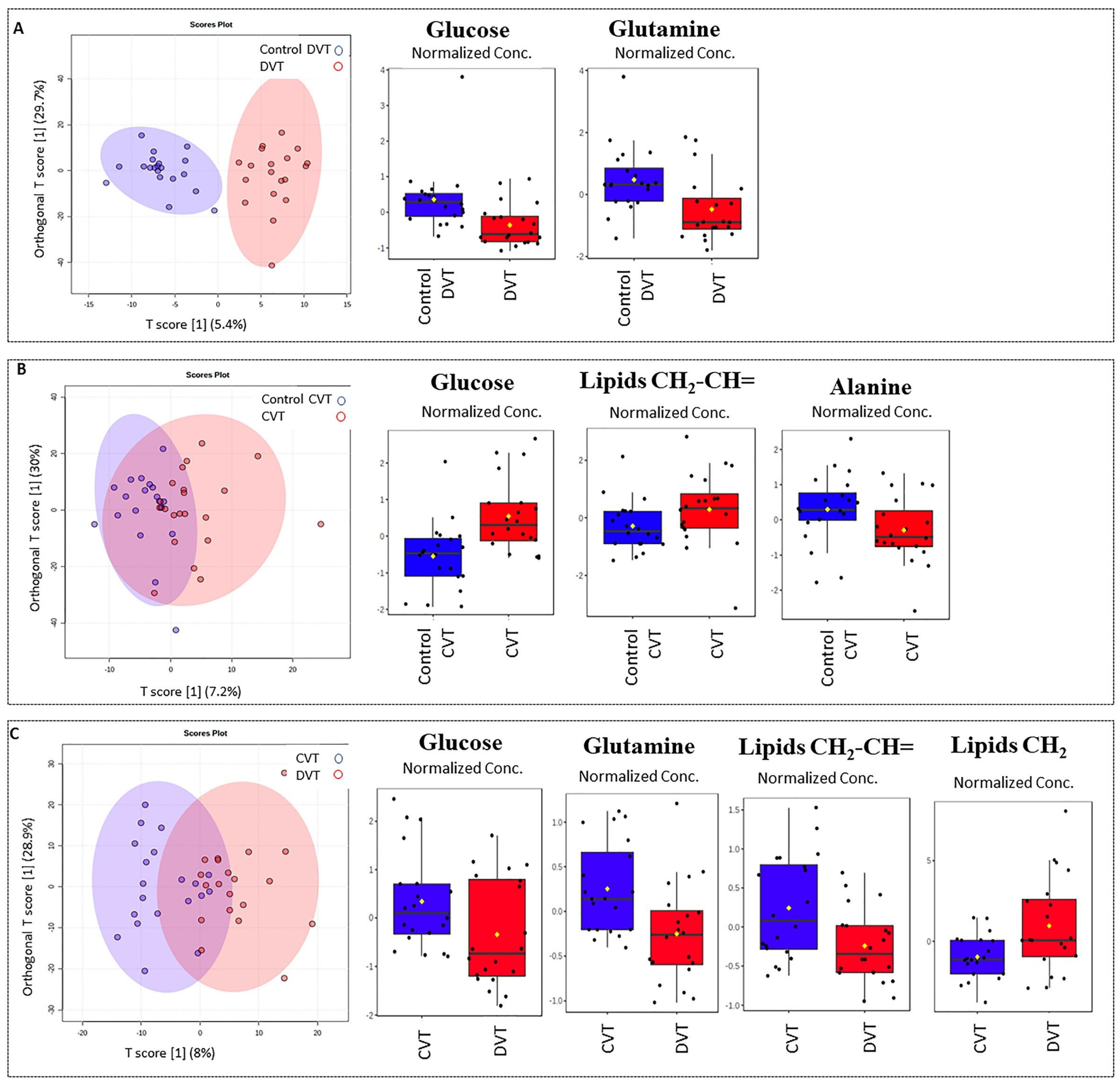
Figure 1C), as well in the DVT subgroup (
Figure 3C). There is evidence that VLDL and remnant lipoproteins induce a procoagulant state. These lipoproteins have the capacity to activate platelets and the coagulation pathway, and to assemble the prothrombinase complex. There are differences in the capacity of lipoproteins to generate thrombin, and this effect is further altered for low-density lipoproteins (LDL), in particular by the oxidation of the unsaturated fatty acids [
32]. While platelets have the largest capacity to generate thrombin via the prothrombinase complex pathway, VLDL has a much higher capacity than oxidized LDL. VLDL compared to oxidized LDL has the ability to increase thrombin formation by approximately 10-fold [
33]. Once an individual presents thrombosis, the predisposition probably remains, mediated by the interaction between triglyceride-rich lipoproteins, platelets, and the vascular endothelium. Since our study is retrospective, we can speculate that these alterations could contribute as a causal factor or as a consequence of the thrombotic episode, and could participate in future complications. We have to point out that the altered profile still remains, even after the statistical correction of BMI, sex, and age.
Other metabolites’ alterations were identified and could be linked to energy or amino acids’ metabolism pathways. Alterations in glucose are associated with the VTE as a risk factor, given that hyperglycemia can activate coagulation [
27]. However, here we observed that glucose decreased in the thrombotic group and the DVT subgroup when compared with their controls, and surprisingly, increased in the CVT group. However, it is already known that hyperglycemia was reported as a strong predictor of poor clinical outcomes in patients with CVT [
34]. We also found alterations in the
1H-NMR spectral region that correspond to glycoprotein A (GlycA). Recently, glycoprotein profiles by NMR have emerged as a potential biomarker that reflects systemic inflammation in type 2 diabetes, obesity, cardiovascular events, and other pathological processes [
35,
36,
37,
38,
39,
40]. Levels of GlycA show an abundance of mobile
N-acetyl sugar groups present on glycoproteins in circulating blood, which are involved in the acute phase response of different inflammatory disease states [
40]. This inflammatory biomarker could also be associated with thrombotic events and could be used as an analytic or clinical tool that may complement or provide advantages over existing clinical markers of systemic inflammation. It is well understood that inflammation can activate the coagulation cascade by several mechanics: down-regulation of antithrombin and other anticoagulant mechanisms, tissue-factor-mediated thrombin generation, and impaired fibrinolysis. Thrombin itself is known to induce IL-6 and IL-8 in endothelial cells, which play a role in the maintenance of inflammation. Furthermore, the endothelial injury induced by pro-inflammatory cytokines worsens the coagulation balance [
41]. Nevertheless, it will be interesting to analyze samples in the acute phase to confirm this finding, and to make additional studies to evaluate its role.
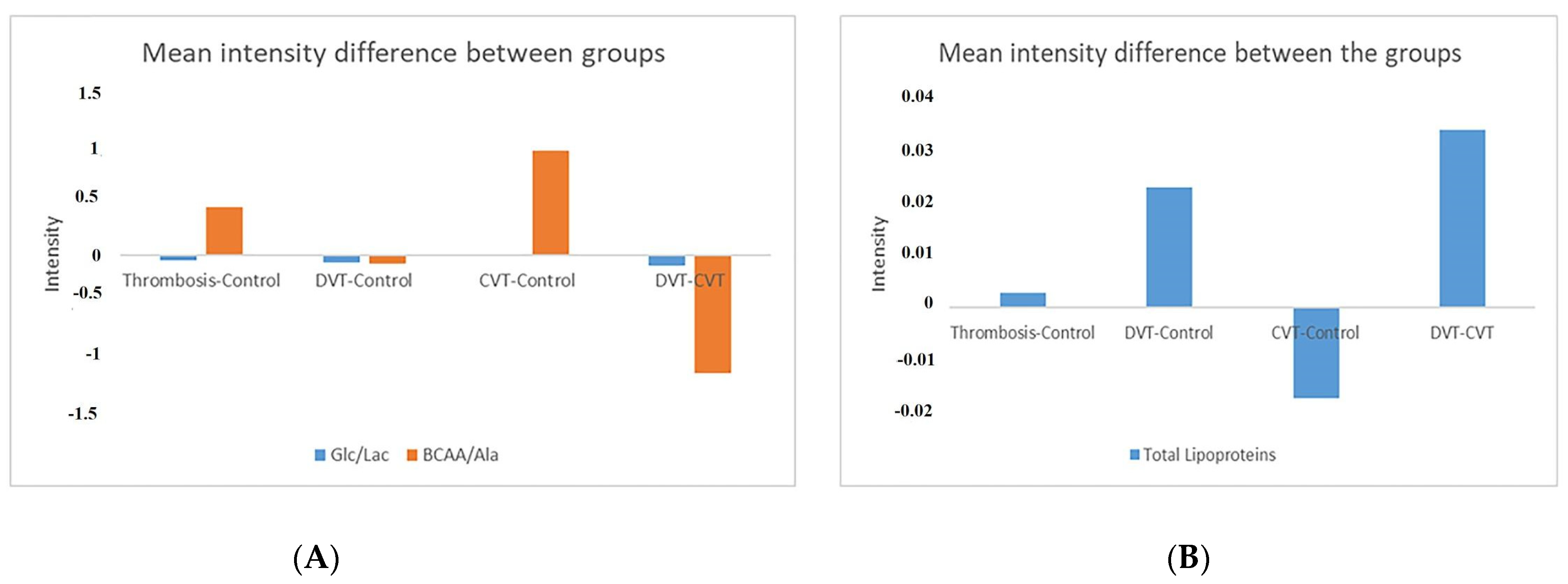
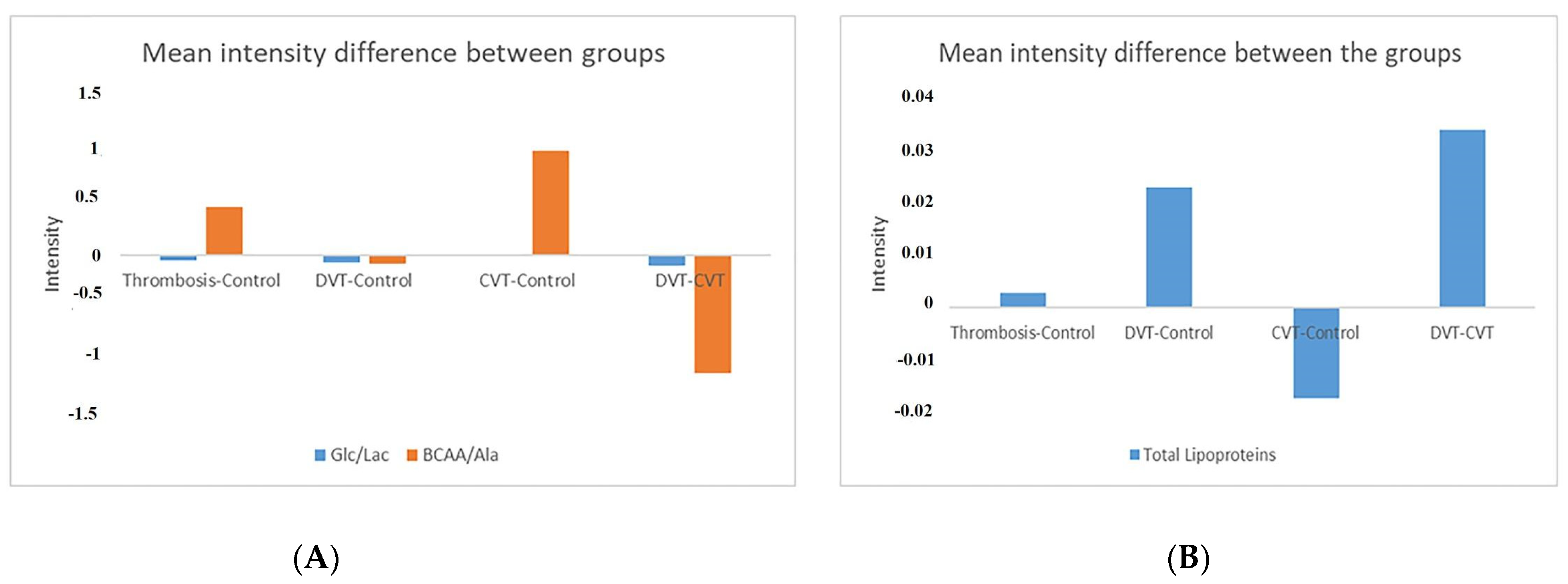
The branched-chain amino acids (BCAAs) leucine, isoleucine, and valine are important resources for energy production and regulators of metabolic and nutrient signals. BCAA catabolism is a regulator of platelet activation, and BCAA dysfunction could be associated with arterial thrombosis risk [
42]. Although BCAAs have not yet been reported to be associated with venous thrombosis, in this study, we showed alterations in leucine, valine, alanine, and lipoproteins in the thrombosis group (
Figure A1).
Previous studies reported that aspirin, an anti-aggregating drug, can reduce the risk of recurrence of DVT by 30% [
43]. An elucidation of the multiple mechanisms involved in platelet induction of venous thrombosis provides opportunities to selectively inhibit this pathway that is relevant to the pathophysiology. Sung et al., 2018 proposed that thrombosis could have a perturbed turnover in the TCA cycle [
18], and this could be indicated by metabolites such as valine, alanine, and glutamine that were also found to be decreased in thrombotic patients. These metabolites could be associated with the pathological condition, as previously reported [
18].
Strengths and Limitations
Strengths of this study include a well characterized investigated cohort selected based on rigorous exclusion criteria—no DVT recurrence, APS, cancer, infection, renal, hepatic or inflammatory disease, as well as, the use of corticosteroids, and tobacco. The use of a homogenous cohort matched with a similar control group, and inclusion of a metabolomics analysis to highlight the alterations that remain after thrombotic episodes.
The limitations of this study are the relatively small number of patients having in mind such a common disease, the lack of inflammatory or thrombotic markers at the time the blood samples were collected for the metabolomic analysis, as well as the design of the retrospective study.
Although the data obtained herein provided important features in patients with previous venous thromboembolic disease that distinguish them from controls, future studies are still needed to confirm the findings in patients with acute DVT.
Since the purpose of the current study was to identify metabolic alterations even months after acute DVT episode, the next step is a validation analysis including diverse populations and different disease subtypes.


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}