
Prevalence of Tinea Capitis among Children in Osogbo, Nigeria, and the Associated Risk Factors

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area and Study Population
2.2. Sample Collection and Handling
2.3. Detection, Isolation and Characterization of Fungal Pathogens
2.4. Statistical Analysis
2.5. Ethical Approval
3. Results
3.1. Prevalence of Tinea Capitis among Pupils with Clinical Symptoms
3.2. Risk Factors Associated with the Occurrence of Tinea Capitis among All the Participants
3.2.1. Frequency of Baths, and Use of Bath Soaps
3.2.2. How Often School Uniforms Are Changed
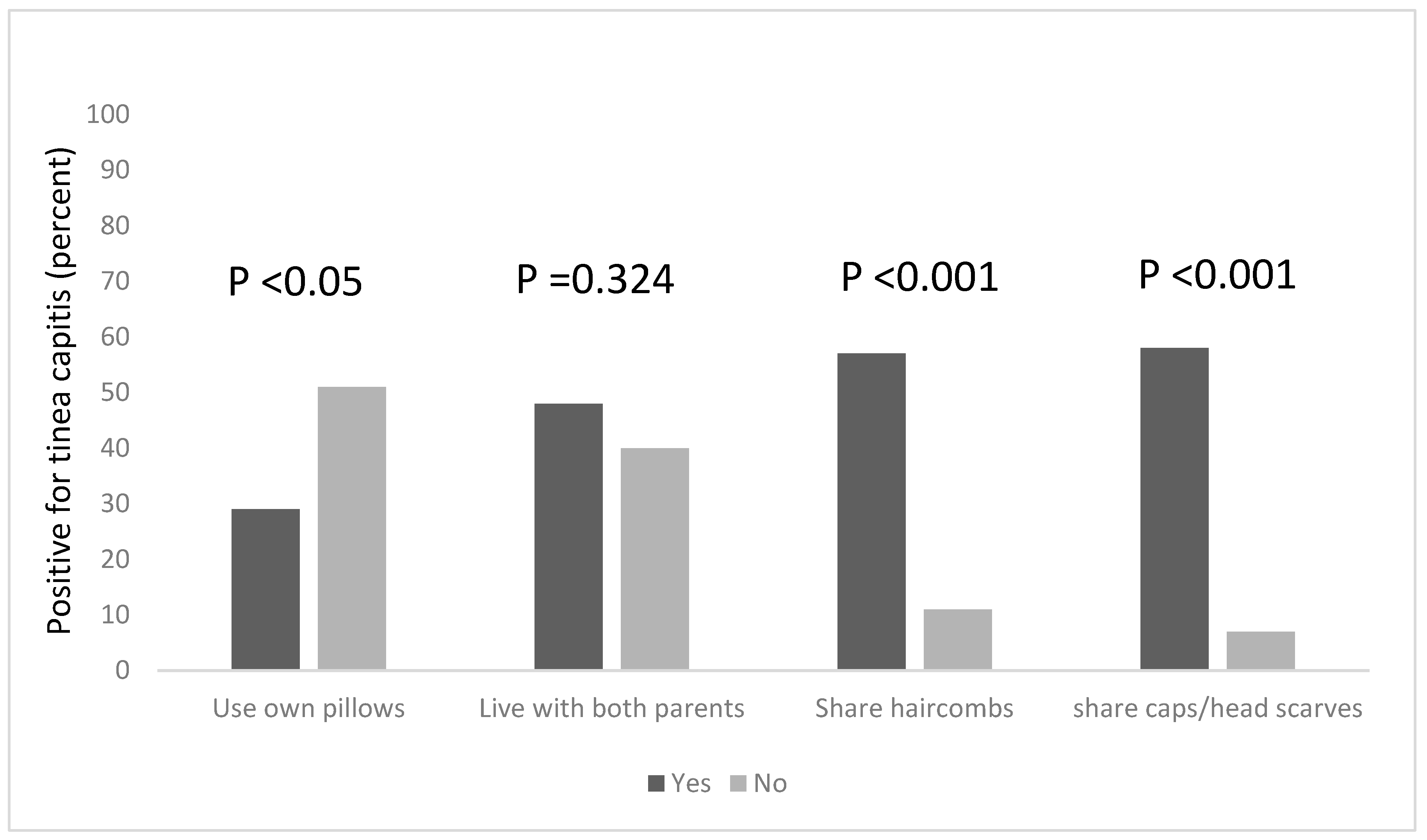
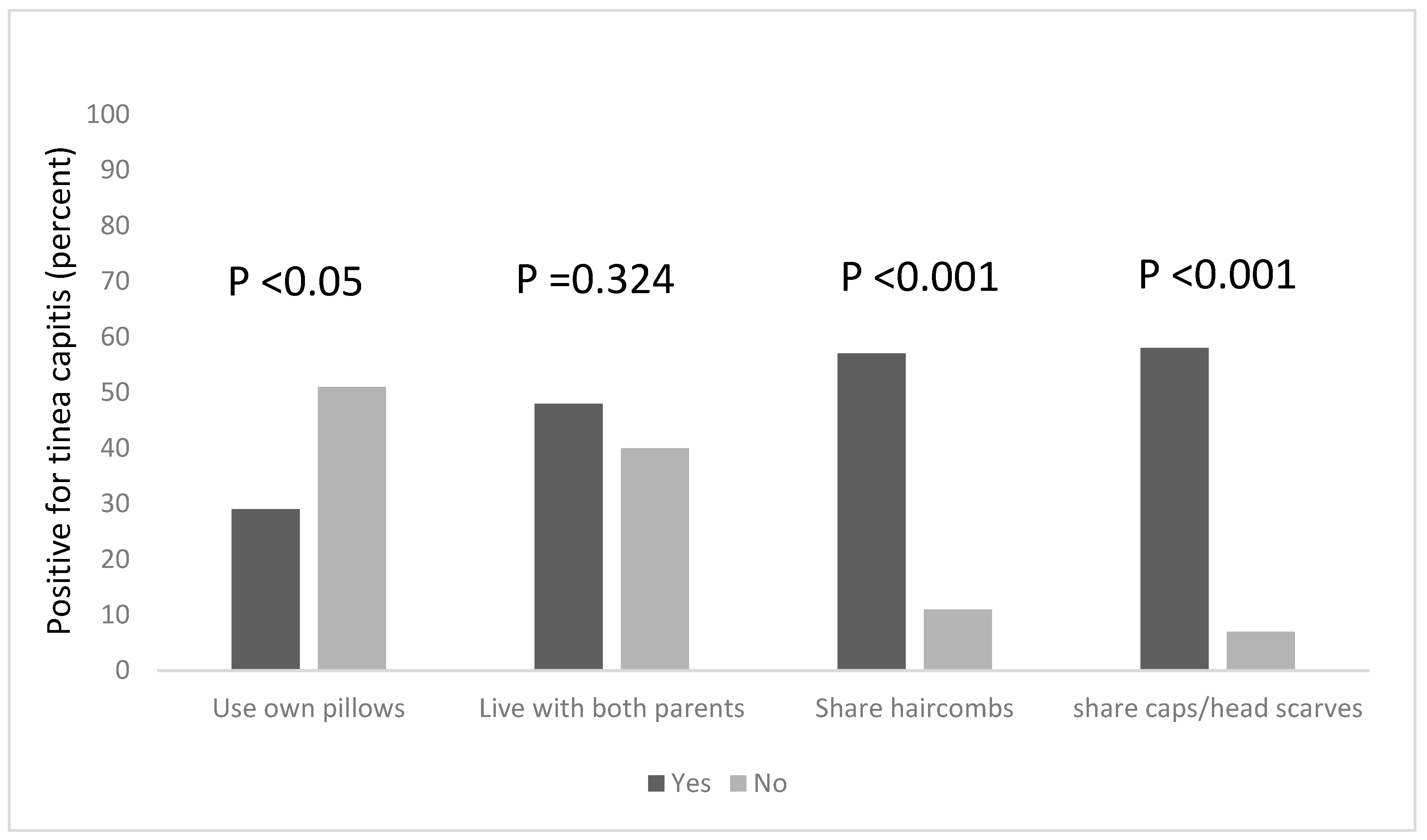
3.2.3. Hair Combs, Caps and Headscarves Sharing
3.2.4. Playing Habits
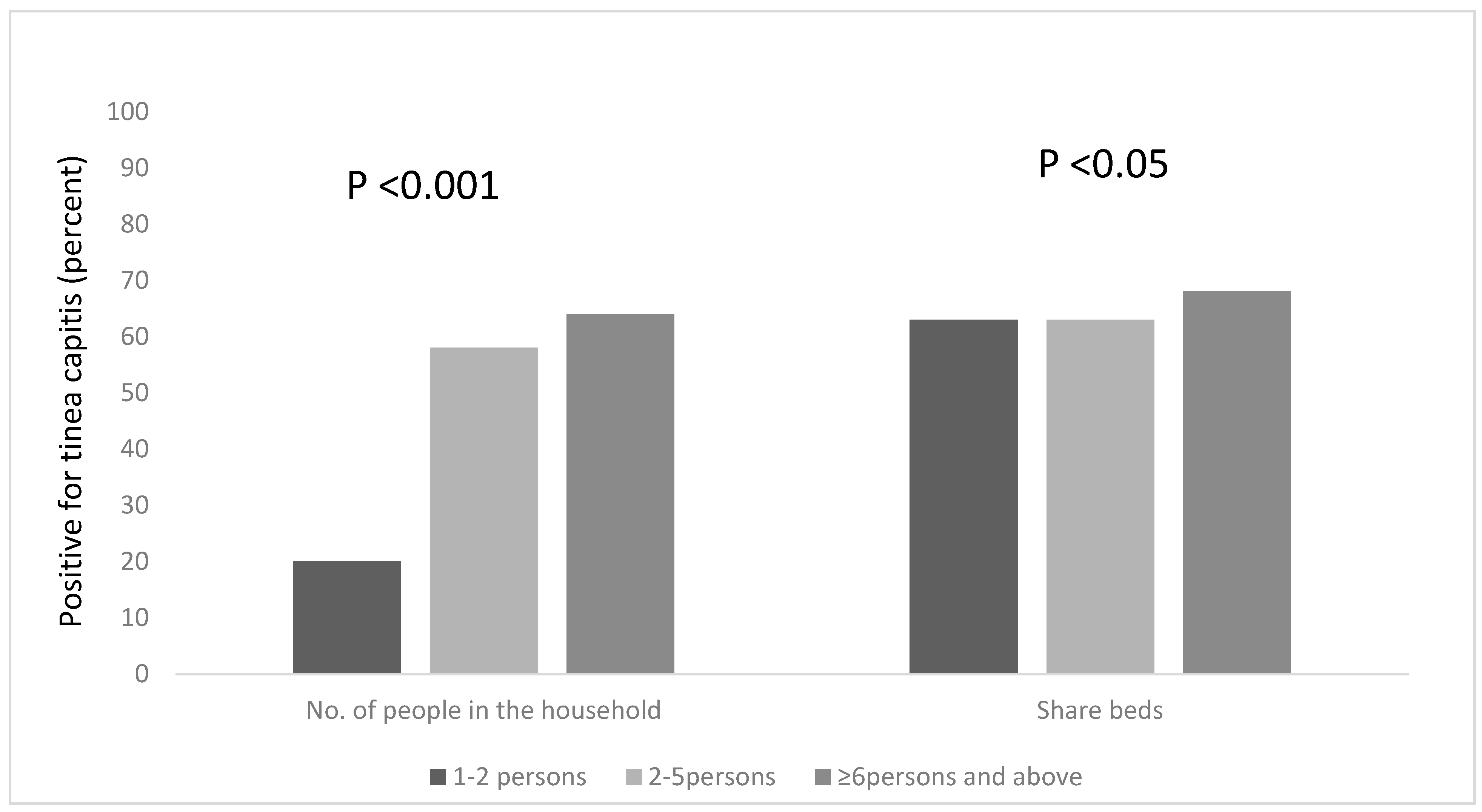
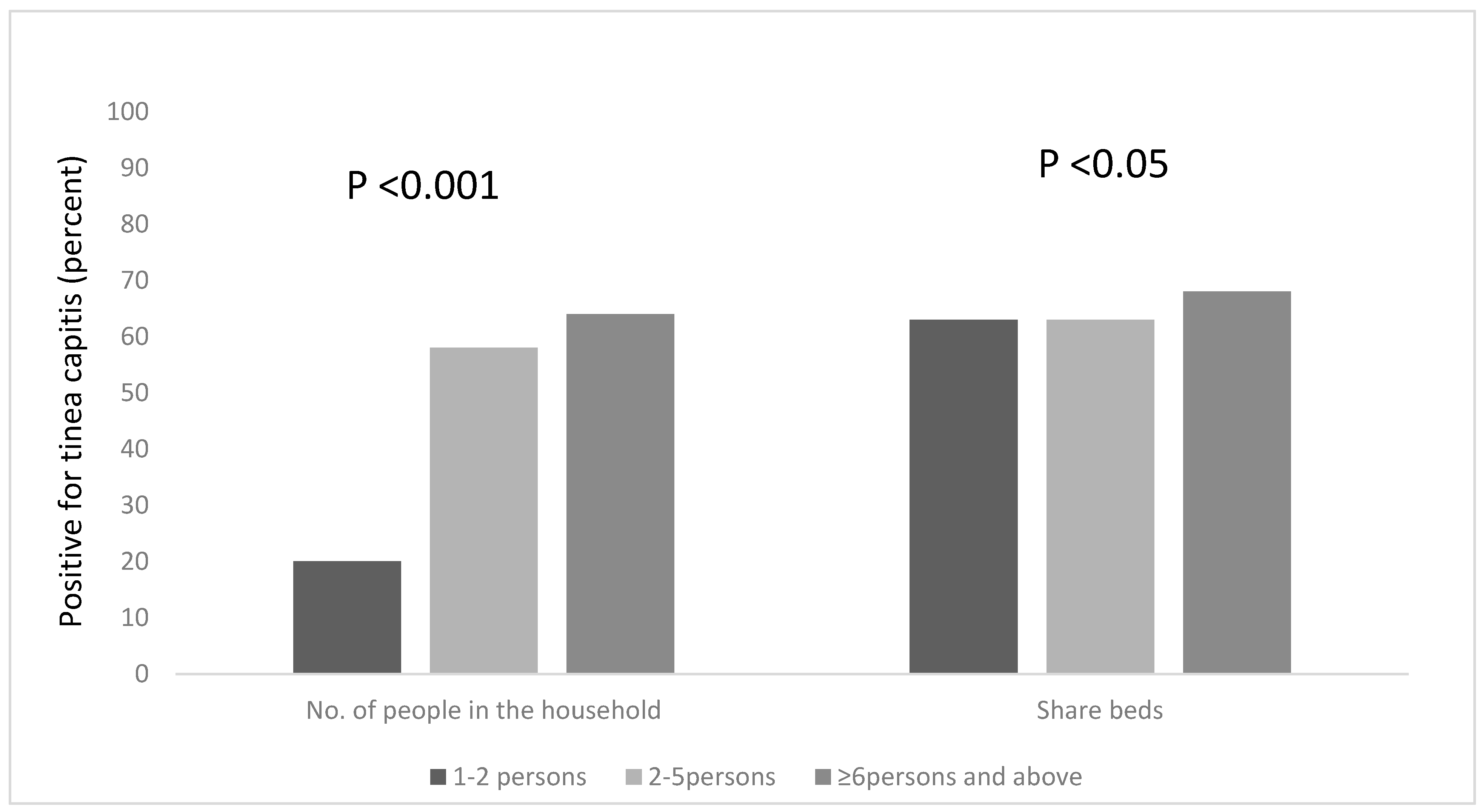
3.3. Risk Factors Associated with the Occurrence of Tinea Capitis among All the Participants, Based on Household Information
3.4. Occurrence of Tinea Capitis Based on Socio-Demographical Data of the Participants
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Oladele, R.O.; Denning, D.W. Burden of serious fungal infection in Nigeria. West Afr. J. Med. 2014, 33, 107–114. [Google Scholar] [PubMed]
- Hay, R.J. Tinea Capitis: Current Status. Mycopathologia 2017, 182, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Bennassar, A.; Grimalt, R. Management of tinea capitis in childhood. Clin. Cosmet. Investig. Dermatol. 2010, 3, 89–98. [Google Scholar] [PubMed]
- Ndako, J.A.; Osemwegie, O.; Olopade, B.; Yunusa, G.O. Prevalence of Dermatophytes and other associated Fungi among school children. Glob. Adv. Res. J. Med. Med. Sci. 2012, 1, 49–56. [Google Scholar]
- Vishnu Sharma, T.K.K.; Sharma, A.; Seth, R.; Chandra, S. Dermatophytes: Diagnosis of dermatophytosis and its treatment. Afr. J. Microbiol. Res. 2015, 9, 1286–1293. [Google Scholar] [CrossRef]
- Nweze, E.I. Dermatophytosis in Western Africa: A Review. Pak. J. Boil. Sci. 2010, 13, 649–656. [Google Scholar]
- Nwobu, R.A.; Odugbemi, T. Fungi causing dermatophytosis in Lagos, Nigeria. East Afr. Med. J. 1990, 67, 246–249. [Google Scholar] [PubMed]
- Ngwogu, A.C.; Otokunefor, T.V. Epidemiology of dermatophytoses in a rural community in Eastern Nigeria and review of literature from Africa. Mycopathologia 2007, 164, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Popoola, T.O.S.; Ojo, D.A.; Alabi, R.O. Prevalence of dermatophytosis in junior secondary schoolchildren in Ogun State, Nigeria. Mycoses 2006, 49, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Adefemi, S.A.; Odeigah, L.O.; Alabi, K.M. Prevalence of dermatophytosis among primary school children in Oke-Oyi community of Kwara state. Niger. J. Clin. Pract. 2011, 14, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Afolabi, O.T.; Oninla, O.; Fehintola, F. Tinea capitis: A topical disease of hygeinic concern among primary school children in an urban community in Nigeria. J. Public Health Epidemiol. 2018, 10, 313–319. [Google Scholar]
- Dogo, J.; Afegbua, S.L.; Dung, E.C. Prevalence of Tinea Capitis among School Children in Nok Community of Kaduna State, Nigeria. J. Pathog. 2016, 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Okafor, J.I.; Agbugbaeruleke, A.K. Dermatophytoses among school children in Aba, Abia State–Nigeria and some physiological studies on the isolated etiologic agents. J. Commun. Dis. 1998, 30, 44–49. [Google Scholar] [PubMed]
- Ezeronye, O.U. Distribution of dermatomycoses in Cross River upstream bank of Eastern Nigeria. In Proceedings of the Conference, Medical Mycology: The African Perspective, Hartenbos, South Africa, July 2005; Available online: http://www.cbs.knaw.nl/research/meeting%20abstract/program (accessed on 9 December 2017).
- AL-Janabi, A.A.H.S.; AI-Tememi, N.N.; AI-Shammari, R.A.; AI-Assadi, A.H.A. Suitability of hair type for dermatophytes perforation and differential diagnosis of T. mentagrophytes from T. verrucosum. Mycoses 2016, 59, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Philpot, C.M. Geographical distribution of the dermatophytes: A review. Epidemiol. Infect. 1978, 80, 301–313. [Google Scholar] [CrossRef] [PubMed]
- George, I.O.; Altraide, D.D. Dermatophyte Infections in Children: A Prospective Study from Port Harcourt, Nigeria. Niger. Health J. 2008, 8, 3–4. [Google Scholar]
- Kligman, A.M.; Ginsberg, D. Immunity of the Adult Scalp to Infection with Microsporum audouini. J. Invest. Dermatol. 1950, 14, 345–358. [Google Scholar] [CrossRef] [PubMed]
- Moto, J.N.; Maingi, J.M.; Nyamache, A.K. Prevalence of Tinea capitis in school going children from Mathare, informal settlement in Nairobi, Kenya. BMC Res. Notes 2015, 8, 274. [Google Scholar] [CrossRef] [PubMed]
- Falahati, M.; Akhlaghi, L.; Lari, A.R.; Alaghehbandan, R. Epidemiology of dermatophytoses in an area south of Tehran, Iran. Mycopathologia 2003, 156, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Ameh, I.G.; Olkolo, R.U. Dermatophytosis Among School Children: Domestic Animals as Predisposing Factor in Sokoto, Nigeria. Pak. J. Boil. Sci. 2004, 7, 1109–1112. [Google Scholar]
- Shehu, M.M.; Bilyaminu, R. Incidence of Tinea capitis among school children in Runjin Sambo Area, Sokoto State. J. Zoöl. Biosci. 2014, 1, 37–42. [Google Scholar]
- Akinboro, A.O.; Olasode, O.A.; Onayemi, O.; Oguntola, A.; Ajibola, A.I. Prediction of Dermatophyte Culture by Clinical Features: Saving Time and Cost in Resource-Poor Settings. Ibnosina J. Med. Biomed. Sci. 2013, 5, 189–195. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Socio-Demographic Characteristics | Frequency | Percent (%) |
|---|---|---|
| Age range (years) | ||
| 4–7 | 134 | 58 |
| 8–11 | 89 | 39 |
| 12–15 | 7 | 3 |
| Gender | ||
| Female | 110 | 48 |
| Male | 120 | 52 |
| Parents’ income status (salary per month) | ||
| ≤1#29,999 (low) | 214 | 93 |
| #3000–#74,999 (medium) | 13 | 6 |
| ≥#75,000 (high) | 3 | 1 |
| Results | Frequency | Percent (%) |
|---|---|---|
| Negative | 10 | 9 |
| Positive | 105 | 91 |
| Prevalence of Species | ||
| T. rubrum | 36 | 34 |
| T. mentagrophyte | 32 | 31 |
| M. canis | 19 | 18 |
| M. gypseum | 8 | 8 |
| E. flocussum | 6 | 6 |
| M. nauum | 3 | 3 |
| T. verucossum | 1 | 1 |
| (a) | |||
| The frequency of baths n, (%) | |||
| Negative (row%) | Positive (row%) | Total (column%) | |
| Daily | 83 (48) | 89 (52) | 172 (75) |
| More than once daily | 42 (72) | 16 (28) | 58 (25) |
| Note.χ2 = 35.405, df = 1. * p < 0.001 | |||
| Use of soap for bath n, (%) | |||
| Negative (row%) | Positive (row%) | Total (column%) | |
| Yes | 124 (92) | 11 (8) | 135 (59) |
| No | 1 (1) | 94 (99) | 95 (41) |
| Note. χ2 = 10.804, df = 1. * p < 0.001 | |||
| How often school uniform is changed n, (%) | |||
| Negative (row%) | Positive (row%) | Total (column%) | |
| Daily | 4 (100) | 0 (0) | 4 (2) |
| Once every week | 52 (39) | 82 (61) | 134 (58) |
| Twice every week | 63 (73) | 23 (27) | 86 (37) |
| More than twice weekly | 6 (100) | 0 (0) | 6 (3) |
| Note. χ2 = 33.383, df = 3. * p < 0.001 | |||
| Playing habit n, (%) | |||
| Negative (row%) | Positive (row%) | Total (column%) | |
| Play with animals | 35 (34) | 67 (66) | 102 (44) |
| Play with sand | 90 (70) | 38 (30) | 128 (56) |
| Note. χ2 = 29.649, df = 1. * p < 0.001 | |||
| (b) | |||
| Age (years) n, (%) | |||
| Negative (row%) | Positive (row%) | Total (column%) | |
| 4–7 | 68 (51) | 66 (49) | 134 (58) |
| 8–11 | 55 (62) | 34 (38) | 89 (39) |
| 12–15 | 2 (29) | 5 (71) | 7 (3) |
| Note. χ2 = 4.566, df = 2. * p < 0.001 | |||
| Gender n, (%) | |||
| Negative (row%) | Positive (row%) | Total (column%) | |
| Female | 64 (58) | 46 (42) | 110 (48) |
| Male | 61 (51) | 59 (49) | 120 (52) |
| Note. χ2 = 1.249, df = 1. * p = 0.264 | |||
| Socio-economic status n, (%) | |||
| Negative (row%) | Positive (row%) | Total (column%) | |
| Low | 120 (56) | 94 (48) | 214 (93) |
| Medium | 5 (38) | 8 (62) | 13 (6) |
| High | 0 (0) | 3 (100) | 3 (1) |
| Note. χ2 = 5.151, df = 2. * p = 0.076 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adesiji, Y.O.; Omolade, B.F.; Aderibigbe, I.A.; Ogungbe, O.V.; Adefioye, O.A.; Adedokun, S.A.; Adekanle, M.A.; Ojedele, R.O. Prevalence of Tinea Capitis among Children in Osogbo, Nigeria, and the Associated Risk Factors. Diseases 2019, 7, 13. https://doi.org/10.3390/diseases7010013
Adesiji YO, Omolade BF, Aderibigbe IA, Ogungbe OV, Adefioye OA, Adedokun SA, Adekanle MA, Ojedele RO. Prevalence of Tinea Capitis among Children in Osogbo, Nigeria, and the Associated Risk Factors. Diseases. 2019; 7(1):13. https://doi.org/10.3390/diseases7010013
Chicago/Turabian StyleAdesiji, Yemisi O., Busayo F. Omolade, Isaac A. Aderibigbe, Oluwabunmi V. Ogungbe, Olusegun A. Adefioye, Samuel A. Adedokun, Margaret A. Adekanle, and Richard O. Ojedele. 2019. "Prevalence of Tinea Capitis among Children in Osogbo, Nigeria, and the Associated Risk Factors" Diseases 7, no. 1: 13. https://doi.org/10.3390/diseases7010013
APA StyleAdesiji, Y. O., Omolade, B. F., Aderibigbe, I. A., Ogungbe, O. V., Adefioye, O. A., Adedokun, S. A., Adekanle, M. A., & Ojedele, R. O. (2019). Prevalence of Tinea Capitis among Children in Osogbo, Nigeria, and the Associated Risk Factors. Diseases, 7(1), 13. https://doi.org/10.3390/diseases7010013