


Estimation of Respiratory Signals from Remote Photoplethysmography of RGB Facial Videos


Abstract
1. Introduction
- First, we aim to clarify the rationale for respiration measurement using remote photoplethysmography (rPPG).
- Second, we demonstrate the feasibility of respiration measurement through rPPG, which is governed by motion artifacts induced by respiration, rather than the influence of skin color changes caused by arterial blood flow.
- Third, we employ the luminance component to extract signals in order to confirm the presence of such motion artifacts for respiration measurement.
2. Methods
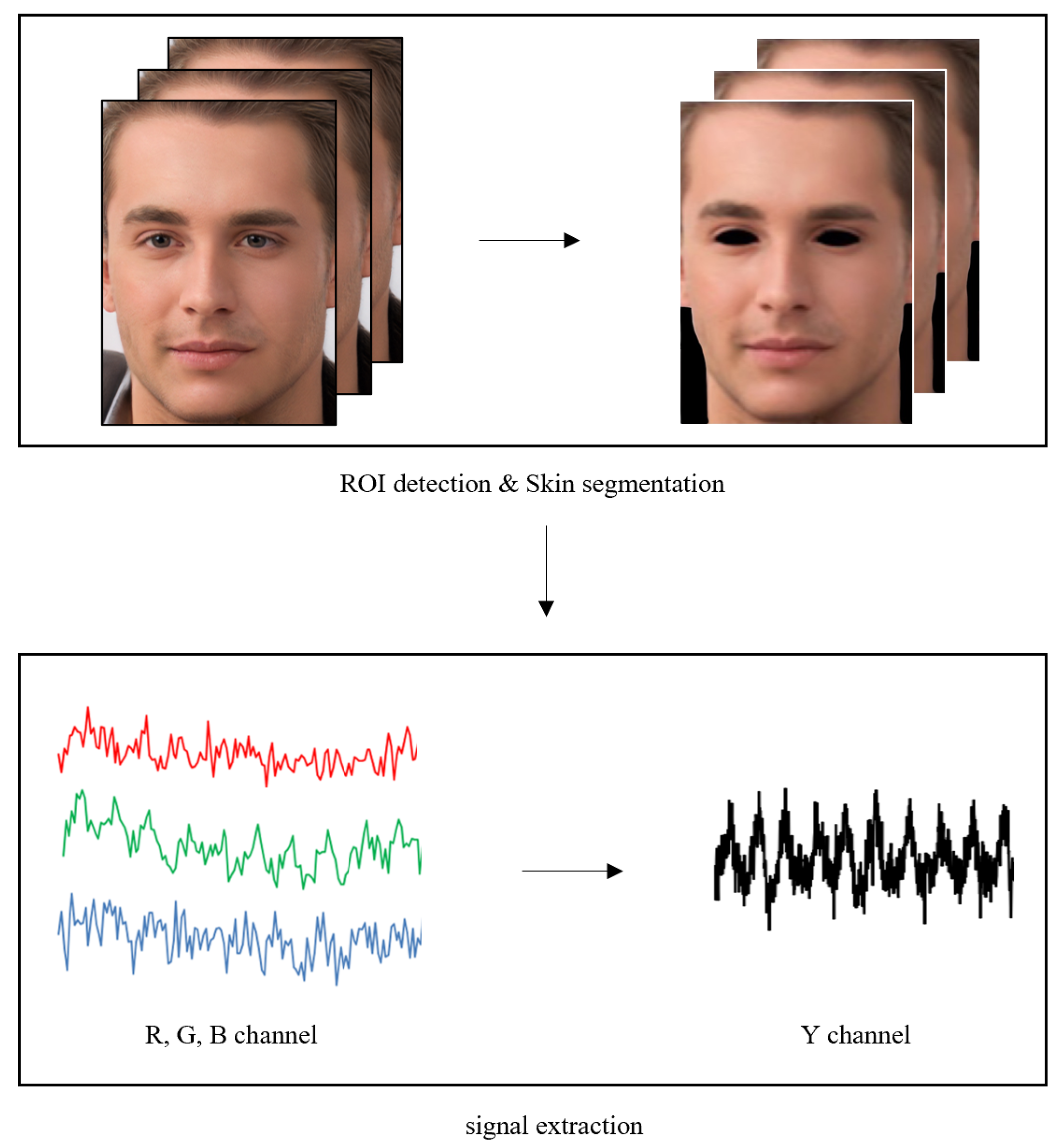
2.1. Remote Photoplethysmography Signal Extraction
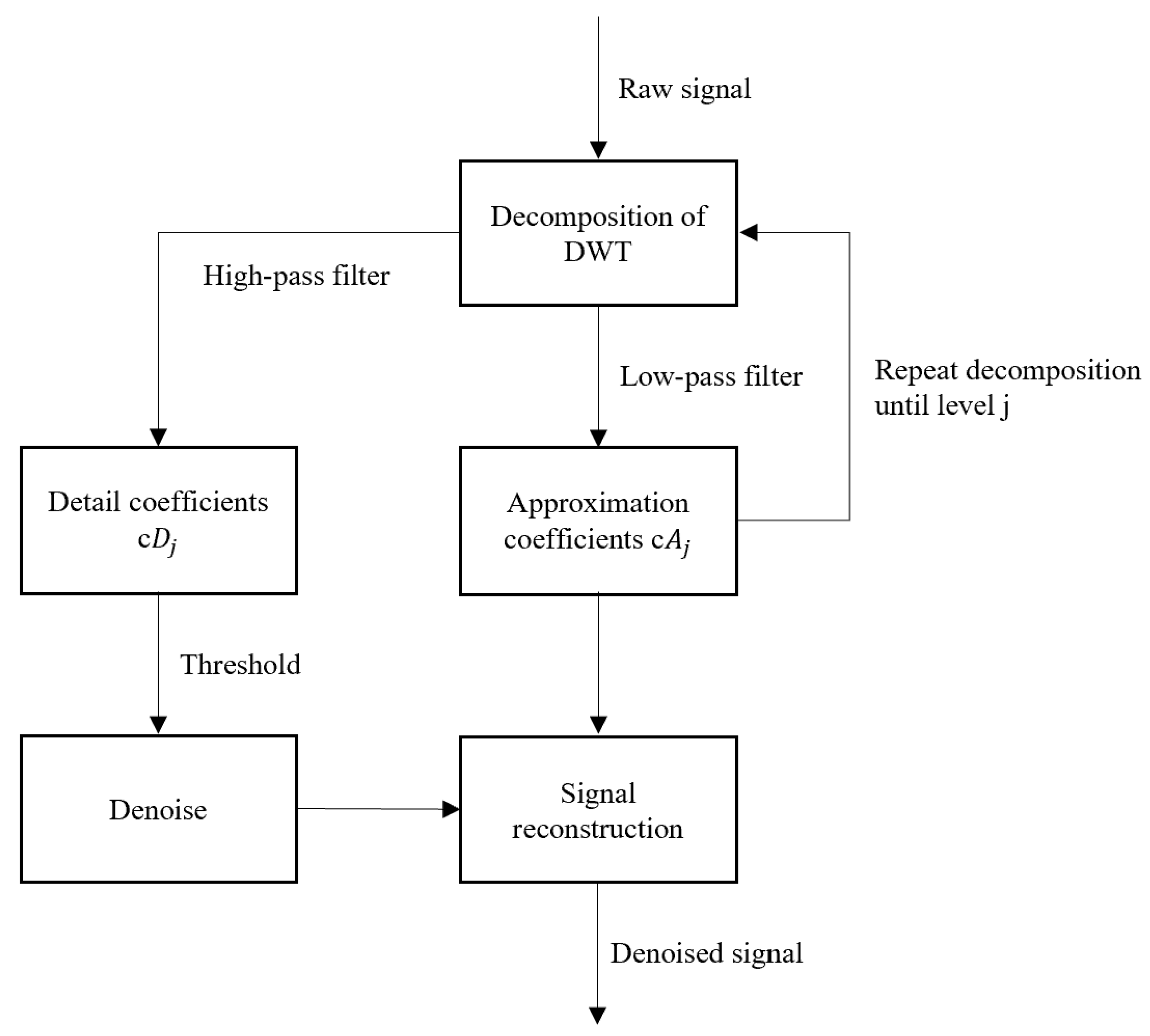
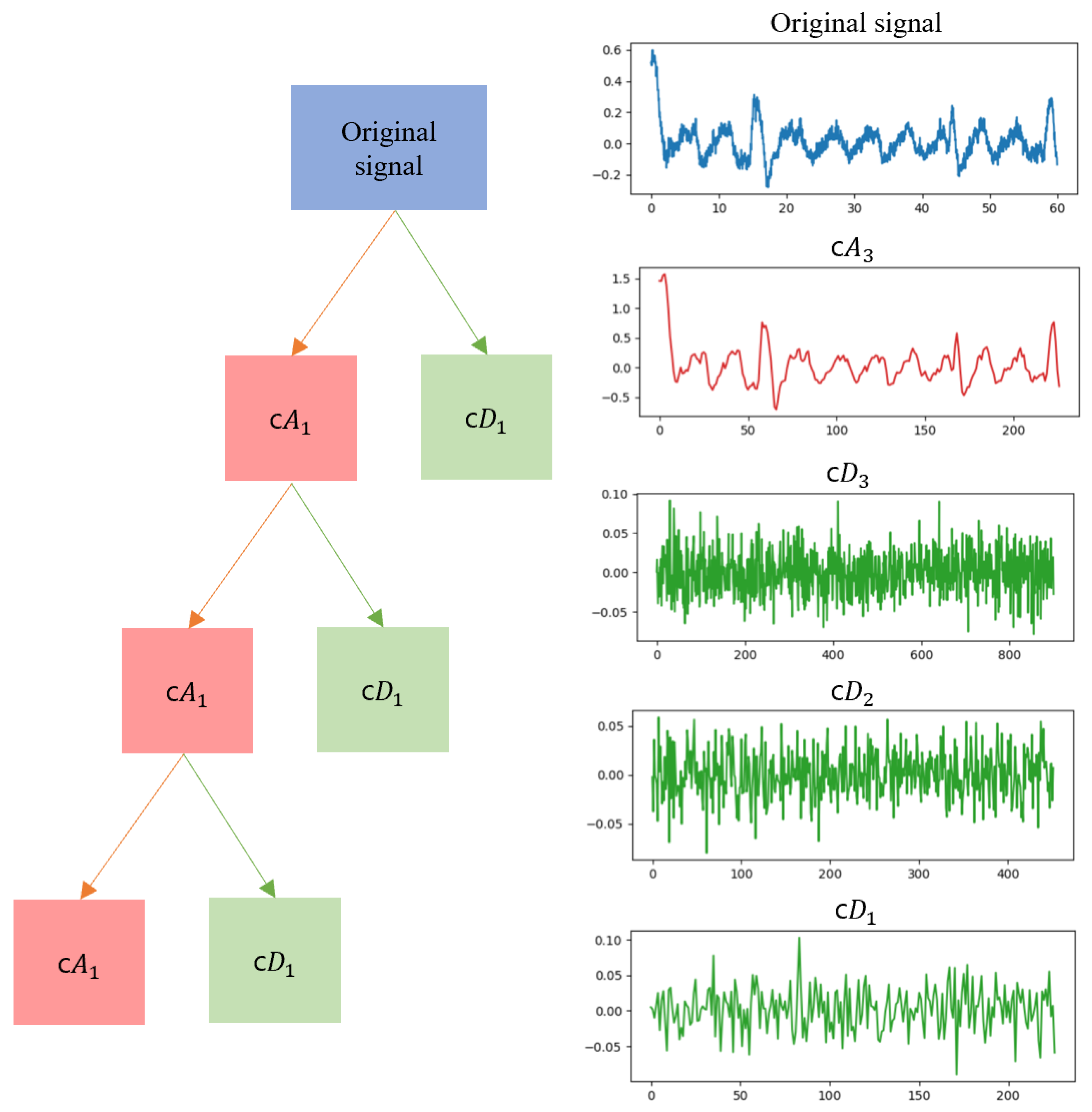
2.2. Removal of Unrelated Motion Artifacts
2.3. Evaluating Signal Quality
2.3.1. SNR (Signal-to-Noise Ratio)
2.3.2. RQI (Respiratory Quality Index)
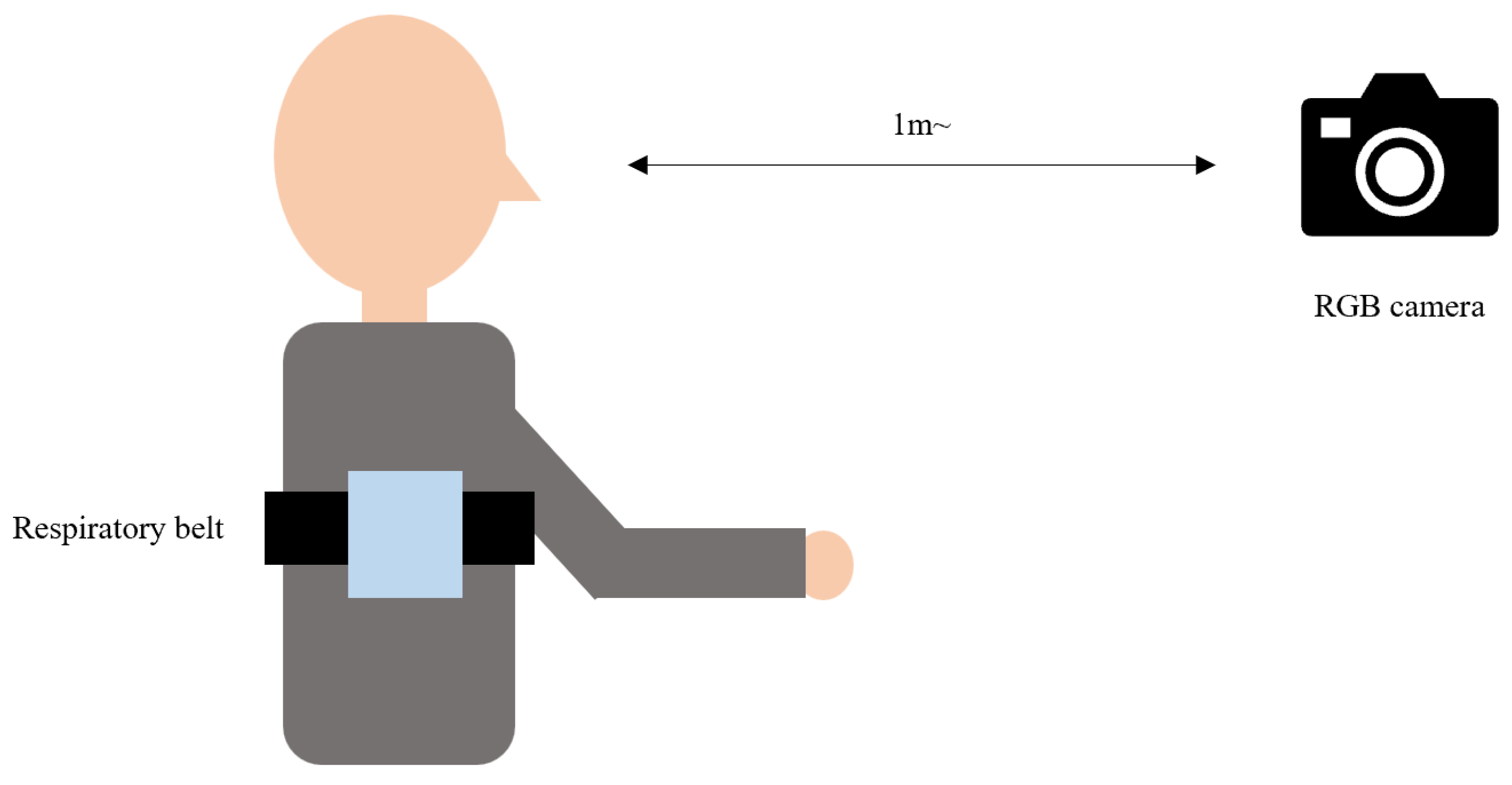
2.4. Experimental Setup
3. Results
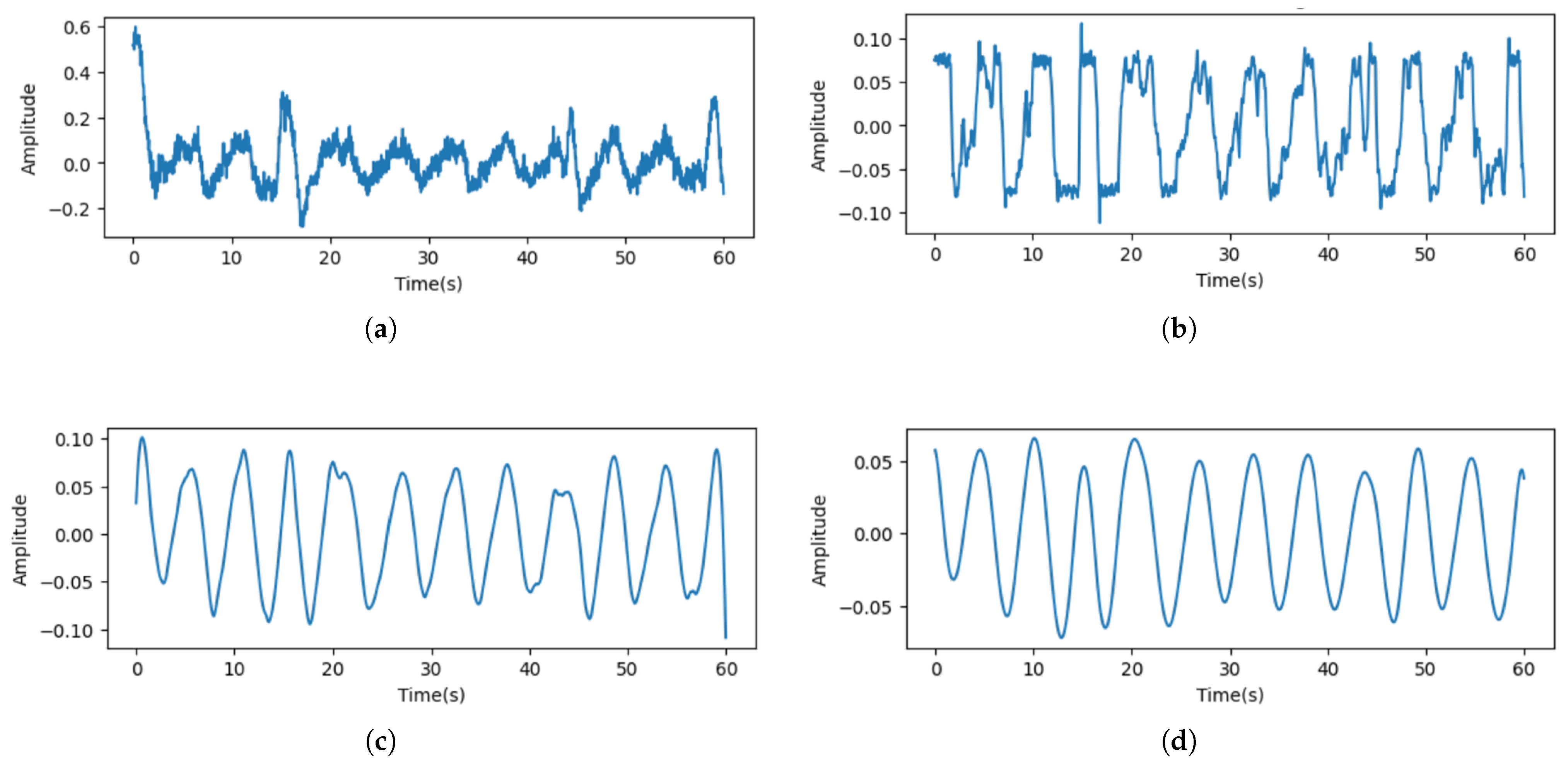
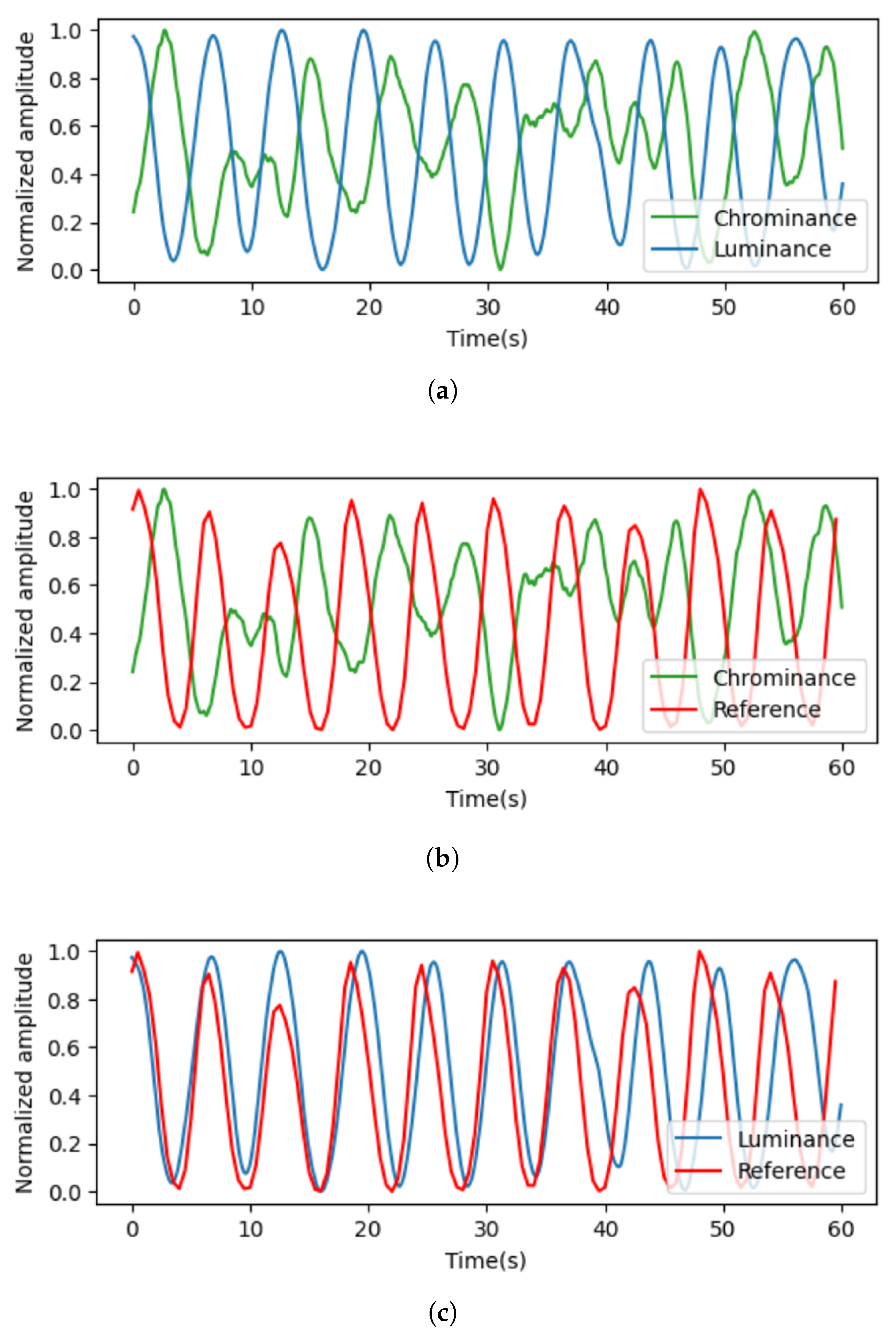
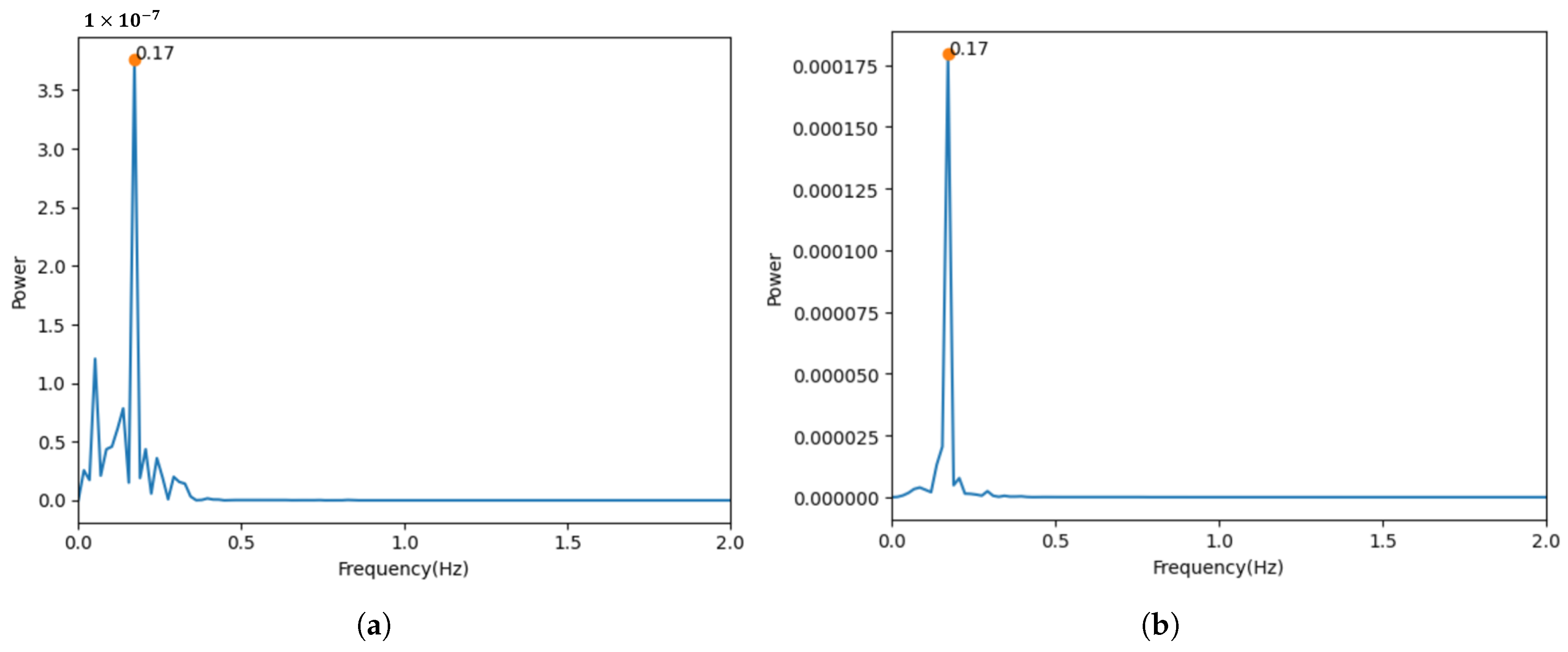
3.1. Comparison of Measurements in Luminance and Chrominance Components
3.2. Comparison of Respiration Signal Quality for Each Facial Region of Interest (ROI)
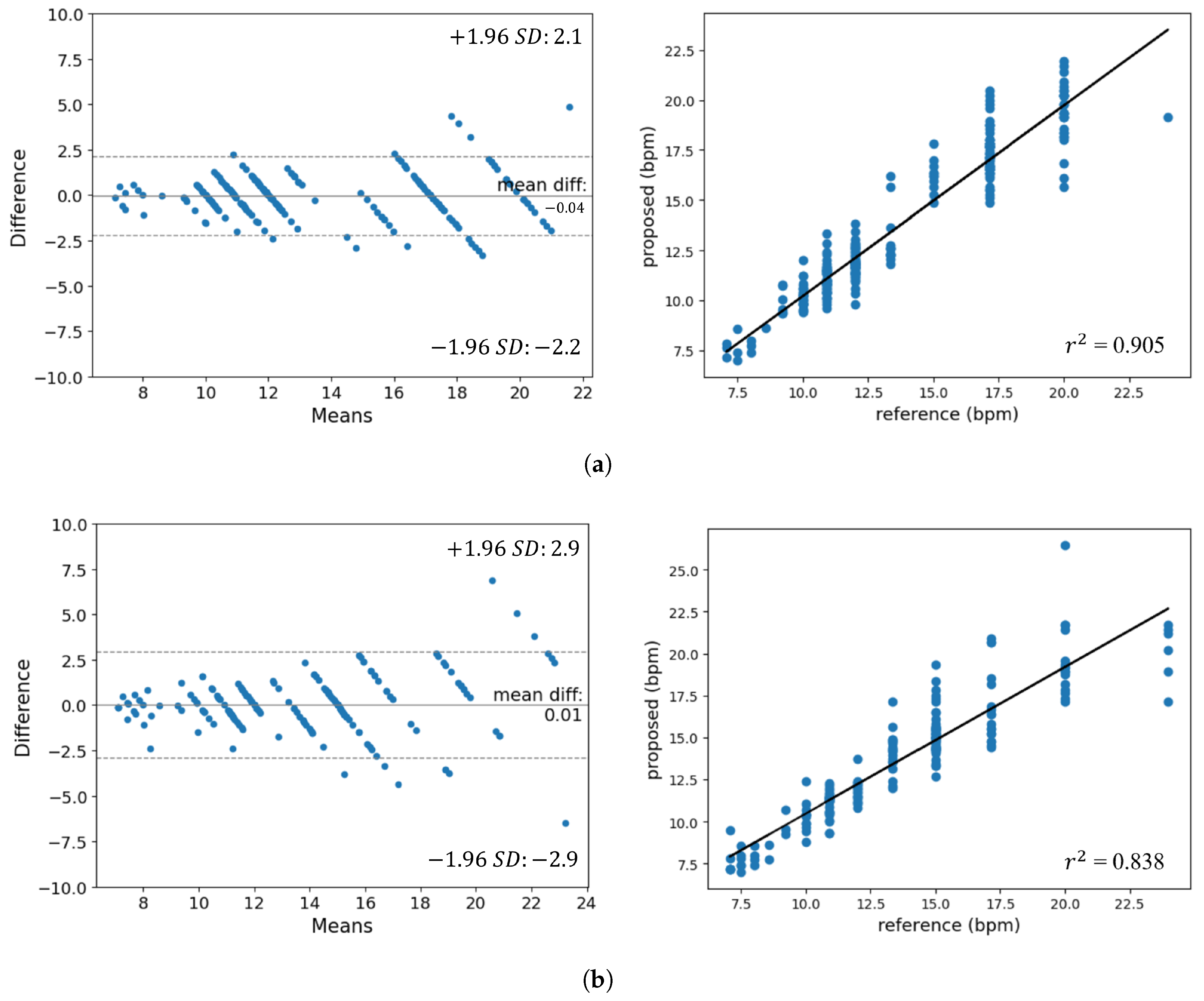
3.3. Performance Evaluation
4. Conclusions
- Investigate and apply techniques to improve the reliability of the respiratory measurement approach against other movements, background noise, and various lighting conditions.
- Broaden the scope of respiratory rate estimation research to include diverse settings, such as outdoors and inside vehicles, to better evaluate the approach’s effectiveness and generalizability.
- Conduct experiments that take into account factors such as facial expressions and talking.
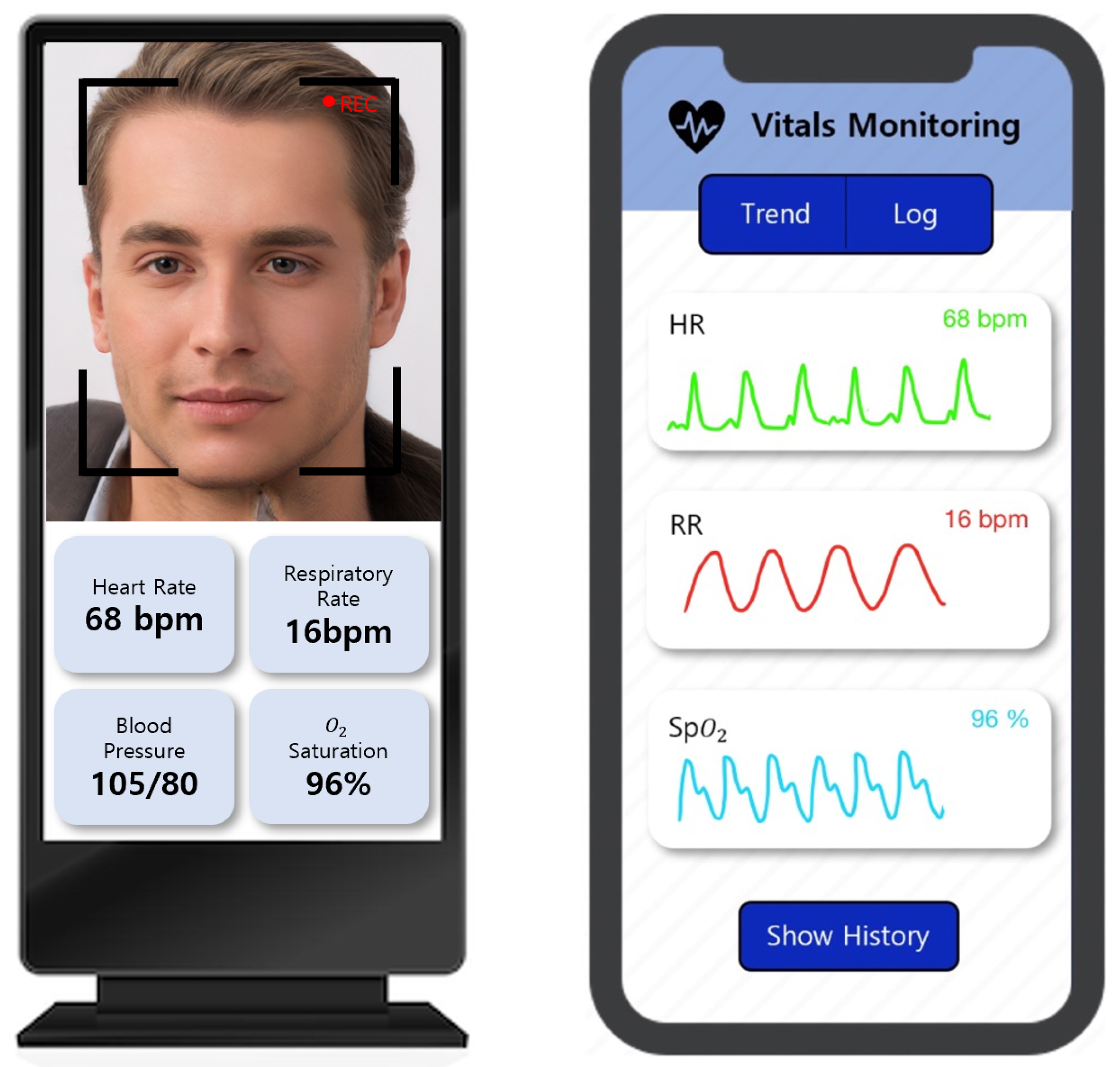
- Explore the potential of combining the proposed respiratory rate estimation method with other contact or non-contact physiological monitoring systems, such as heart rate or blood oxygen saturation (SpO2), to develop comprehensive remote health monitoring solutions.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Naji, A.; Gibson, K.; Lee, S.H.; Chahl, J. Monitoring of cardiorespiratory signal: Principles of remote measurements and review of methods. IEEE Access 2017, 5, 15776–15790. [Google Scholar] [CrossRef]
- Coffey, J.D.; Christopherson, L.A.; Glasgow, A.E.; Pearson, K.K.; Brown, J.K.; Gathje, S.R.; Sangaralingham, L.R.; Carmona Porquera, E.M.; Virk, A.; Orenstein, R.; et al. Implementation of a multisite, interdisciplinary remote patient monitoring program for ambulatory management of patients with COVID-19. NPJ Digit. Med. 2021, 4, 123. [Google Scholar] [CrossRef] [PubMed]
- Marrugo, P.P.; Franco, E.M.; Ribón, J.C.R. Systematic review of platforms used for remote monitoring of vital signs in patients with hypertension, asthma and/or chronic obstructive pulmonary disease. IEEE Access 2019, 7, 158710–158719. [Google Scholar] [CrossRef]
- Takahashi, Y.; Gu, Y.; Nakada, T.; Abe, R.; Nakaguchi, T. Estimation of respiratory rate from thermography using respiratory likelihood index. Sensors 2021, 21, 4406. [Google Scholar] [CrossRef]
- Jakkaew, P.; Onoye, T. Non-contact respiration monitoring and body movements detection for sleep using thermal imaging. Sensors 2020, 20, 6307. [Google Scholar] [CrossRef]
- Romano, C.; Schena, E.; Silvestri, S.; Massaroni, C. Non-contact respiratory monitoring using an RGB camera for real-world applications. Sensors 2021, 21, 5126. [Google Scholar] [CrossRef]
- Guo, T.; Lin, Q.; Allebach, J. Remote estimation of respiration rate by optical flow using convolutional neural networks. Electron. Imaging 2021, 8, 1–267. [Google Scholar] [CrossRef]
- Van Gastel, M.; Stuijk, S.; De Haan, G. Robust respiration detection from remote photoplethysmography. Biomed. Opt. Express 2016, 7, 4941–4957. [Google Scholar] [CrossRef]
- Park, J.; Hong, K. Robust pulse rate measurements from facial videos in diverse environments. Sensors 2022, 22, 9373. [Google Scholar] [CrossRef]
- Chen, W.; Yi, Z.; Lim, L.J.R.; Lim, R.Q.R.; Zhang, A.; Qian, Z.; Huang, J.; He, J.; Liu, B. Deep learning and remote photoplethysmography powered advancements in contactless physiological measurement. Front. Bioeng. Biotechnol. 2024, 12, 1420100. [Google Scholar] [CrossRef]
- Miao, Y.; Chen, Z.; Li, C.; Mandic, D.P. RespDiff: An End-to-End Multi-scale RNN Diffusion Model for Respiratory Waveform Estimation from PPG Signals. In Proceedings of the ICASSP 2025—2025 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Hyderabad, India, 6–11 April 2025; pp. 1–5. [Google Scholar]
- Menniti, M.; Laganà, F.; Oliva, G.; Bianco, M.; Fiorillo, A.S.; Pullano, S.A. Development of Non-Invasive Ventilator for Homecare and Patient Monitoring System. Electronics 2024, 13, 790. [Google Scholar] [CrossRef]
- Suh, K.H.; Lee, E.C. Contactless physiological signals extraction based on skin color magnification. J. Electron. Imaging 2017, 26, 063003. [Google Scholar] [CrossRef]
- Lugaresi, C.; Tang, J.; Nash, H.; McClanahan, C.; Uboweja, E.; Hays, M.; Zhang, F.; Chang, C.L.; Yong, M.G.; Lee, J.; et al. Mediapipe: A framework for building perception pipelines. arXiv 2019, arXiv:1906.08172. [Google Scholar]
- Du, B.; Fernandez-Reyes, D.; Barucca, P. Image processing tools for financial time series classification. arXiv 2020, arXiv:2008.06042. [Google Scholar]
- Li, W.; Piao, M.L.; Alam, M.A.; Kim, N. Noise reduction in digital hologram using wavelet transforms and smooth filter for three-dimensional display. IEEE Photonics J. 2013, 5, 6800414. [Google Scholar]
- Schafer, R.W. What is a savitzky-golay filter? [lecture notes]. IEEE Signal Process. Mag. 2011, 28, 111–117. [Google Scholar] [CrossRef]
- Ma, D.; Shang, X.; Ridler, N.M.; Wu, W. Assessing the impact of data filtering techniques on material characterization at millimeter-wave frequencies. IEEE Trans. Instrum. Meas. 2021, 70, 1–4. [Google Scholar] [CrossRef]
- Hyndman, R. Moving Averages. Int. Encycl. Stat. Sci. 2010, 01, 866–869. [Google Scholar]
- Matsumura, K.; Toda, S.; Kato, Y. RGB and near-infrared light reflectance/transmittance photoplethysmography for measuring heart rate during motion. IEEE Access 2020, 8, 80233–80242. [Google Scholar] [CrossRef]
- Birrenkott, D. Respiratory Quality Index Design and Validation for ECG and PPG Derived Respiratory Data; Report for Transfer of Status; Department of the Engineering Science, University of Oxford: Oxford, UK, 2015. [Google Scholar]
- Birrenkott, D.A.; Pimentel, M.A.; Watkinson, P.J.; Clifton, D.A. A robust fusion model for estimating respiratory rate from photoplethysmography and electrocardiography. IEEE Trans. Biomed. Eng. 2017, 65, 2033–2041. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Strengths | Weaknesses |
|---|---|---|
| Thermal camera-based | Once the ROI is reliably recognized, it is unaffected by variations in illumination. | Advanced thermographic cameras are costly, and their resolution significantly affects their performance. |
| Body movement-based | Measurement is available with a low-cost camera without the need for additional devices. | Motion noise and individual factors like clothing and background can affect measurement. Optical flow-based techniques may result in longer processing times. |
| Remote photoplethysmography (PPG)-based | Measurement is available with a low-cost camera. Utilizing frequency transformation methods enhances its resilience to other types of noise. | The underlying principle of respiratory measurement using rPPG remains only partially understood, particularly regarding signal separation and physiological interpretation. |
| Chrominance | Luminance | |
|---|---|---|
| SNR | 0.9762 | 3.7623 |
| R1 | R2 | R3 | R4 | |
|---|---|---|---|---|
| RQI | 0.9567 | 0.9587 | 0.9613 | 0.9608 |
| MAE | Correlation | MOD | LoA | ||
|---|---|---|---|---|---|
| Experiment 1 | 0.789 | 0.905 | 0.953 | −0.04 | |
| Experiment 2 | 1.024 | 0.838 | 0.916 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, H.; Kim, S.; Lee, E.C. Estimation of Respiratory Signals from Remote Photoplethysmography of RGB Facial Videos. Electronics 2025, 14, 2152. https://doi.org/10.3390/electronics14112152
Seo H, Kim S, Lee EC. Estimation of Respiratory Signals from Remote Photoplethysmography of RGB Facial Videos. Electronics. 2025; 14(11):2152. https://doi.org/10.3390/electronics14112152
Chicago/Turabian StyleSeo, Hyunsoo, Seunghyun Kim, and Eui Chul Lee. 2025. "Estimation of Respiratory Signals from Remote Photoplethysmography of RGB Facial Videos" Electronics 14, no. 11: 2152. https://doi.org/10.3390/electronics14112152
APA StyleSeo, H., Kim, S., & Lee, E. C. (2025). Estimation of Respiratory Signals from Remote Photoplethysmography of RGB Facial Videos. Electronics, 14(11), 2152. https://doi.org/10.3390/electronics14112152