
An Ontology-Based Framework for a Telehealthcare System to Foster Healthy Nutrition and Active Lifestyle in Older Adults

 ,
,  , ,
, ,  ,
,
Abstract
1. Introduction
2. Related Work
3. HeNuALs Architecture
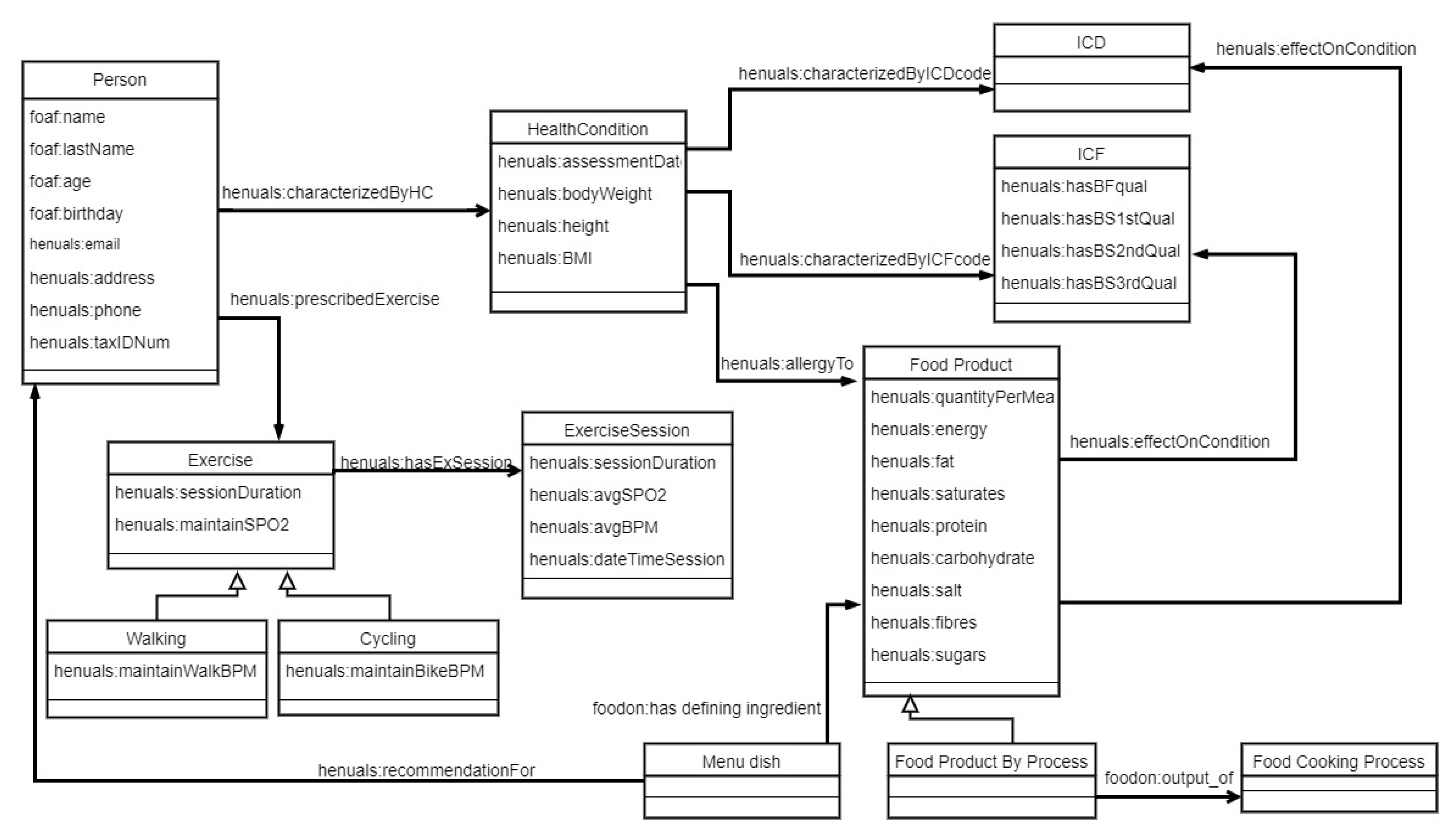
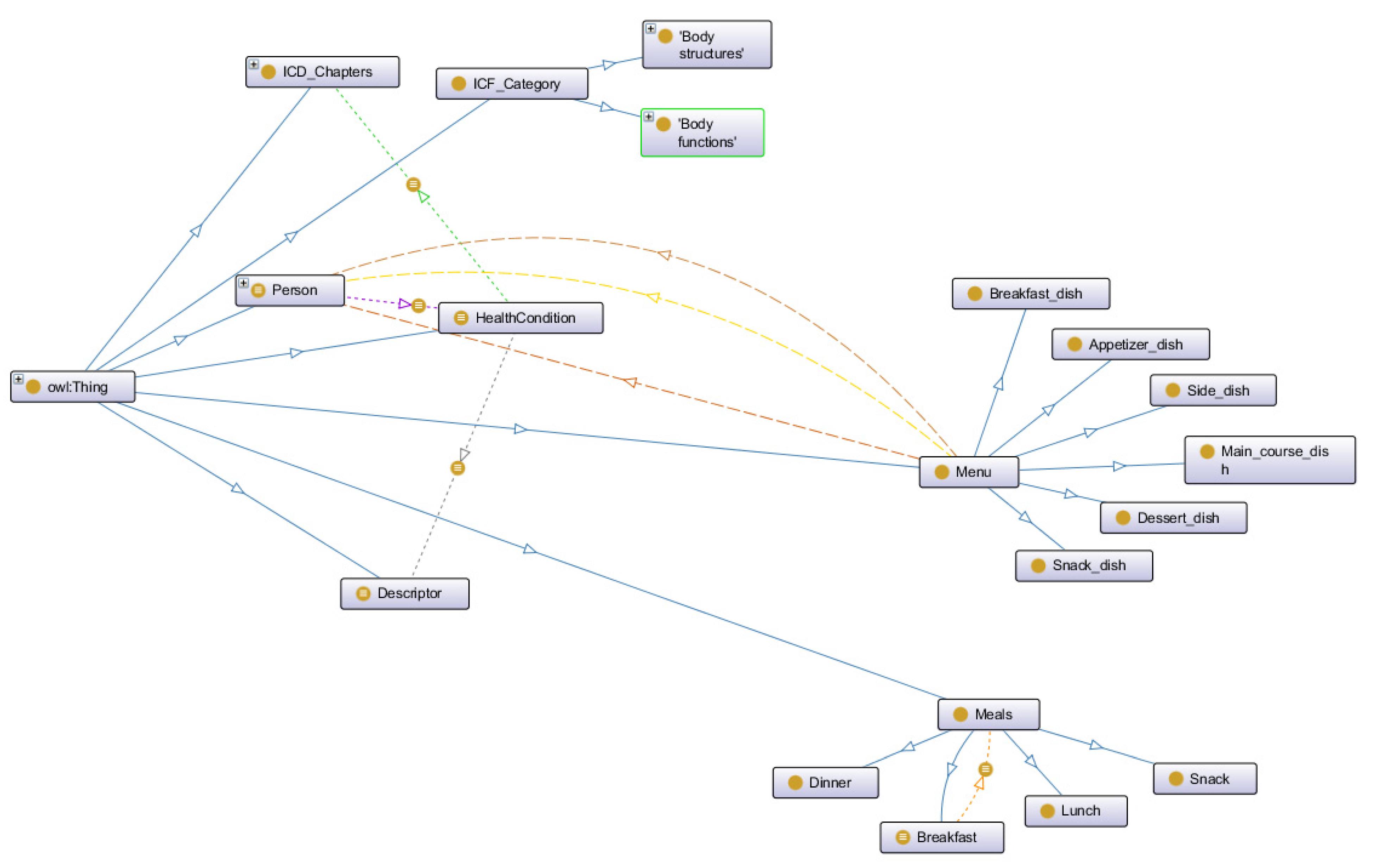
3.1. Ontological Layer
3.1.1. Patients and Health Conditions
3.1.2. Foods, Their Effects, and Diets
3.1.3. Exercise and Its Session
3.1.4. Inferences and Querying
- A set of rules leverages the descriptions of foods and their effects on specific health conditions to draw inferences on more complex foods (dishes). A dish containing at least one ingredient having a negative effect for a specific patient is not suggested as a suitable dietary option. Similarly, a dish composed of healthy ingredients but processed with a cooking method incompatible with the patient’s health condition is also not suggested.
- A second set of rules allows for detecting whether a dish composed of many ingredients is a suitable food option for a person who can experience an allergic reaction to a specific food (e.g., 4A80.1 Bronchospasm provoked by allergy to food substance) by checking its ingredients and matching them with the list of allergies characterizing such an individual.
- The third set of rules leverages the nutrient prescriptions prescribed by the clinicians and the information regarding nutrients for each dish. It is possible to infer as unhealthy options those foods with specific values for some nutrients (e.g., a fruit salad containing raisins and honey is an unsuitable option for patients with diabetes due to the high sugar amount).
- SWRL rules can also provide suggestions regarding the substitution of allergen food products with other products using the foodon:has food substance analog relation.
- SWRL rules determine some thresholds for exercise programs (HRtarget and SpO2) according to the ACSM recommendations detailed in the previous subsection.
3.2. Hardware
3.3. Communication
3.4. Patient Application
3.5. HeNuALs Clinician Application
4. Use Cases
4.1. James: A Man with COPD
4.2. Grace: A Woman with Type 2 Diabetes Mellitus
4.3. Results of Use Case Processing
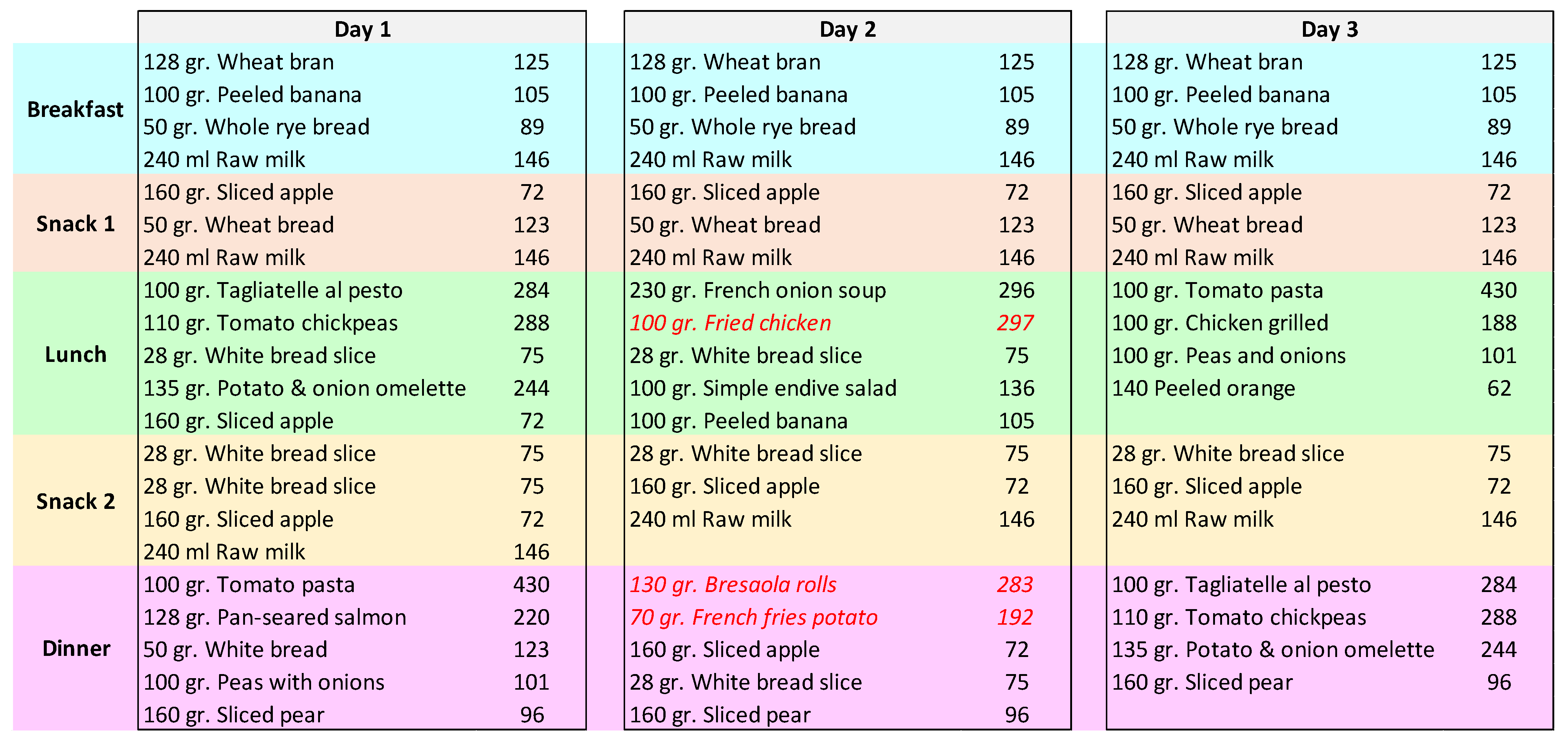
- The plan envisioned for Day 1, although containing healthy or adequate food choices, exceeded the prescribed amount for James’ health condition, and therefore it was classified as a henuals:notAppropriateDayPlan;
- The plan for Day 2 contained some dishes that were inferred to be henuals:unhealthySuggestionFor. Therefore, this plan was also classified as a henuals:notAppropriateDayPlan;
- Finally, the plan for Day 3 contained healthy choices for foods, and its caloric amount was adequate to the daily intake prescribed to the patient.
5. Discussion, Limitations of This Work, and Future Work
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Weinstein, R.S.; Lopez, A.M.; Joseph, B.A.; Erps, K.A.; Holcomb, M.; Barker, G.P.; Krupinski, E.A. Telemedicine, telehealth, and mobile health applications that work: Opportunities and barriers. Am. J. Med. 2014, 127, 183–187. [Google Scholar] [CrossRef]
- Jennett, P.A.; Hall, L.A.; Hailey, D.; Ohinmaa, A.; Anderson, C.; Thomas, R.; Young, B.; Lorenzetti, D.; Scott, R.E. The socio-economic impact of telehealth: A systematic review. J. Telemed. Telecare 2003, 9, 311–320. [Google Scholar] [CrossRef]
- Smith, A.C.; Thomas, E.; Snoswell, C.L.; Haydon, H.; Mehrotra, A.; Clemensen, J.; Caffery, L.J. Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19). J. Telemed. Telecare 2020, 26, 309–313. [Google Scholar] [CrossRef]
- Jácome, C.; Marques, A.; Oliveira, A.; Rodrigues, L.; Sanches, I. Pulmonary telerehabilitation: An international call for action. Pulmonology 2020, 26, 335. [Google Scholar] [CrossRef] [PubMed]
- Polisena, J.; Coyle, D.; Coyle, K.; McGill, S. Home telehealth for chronic disease management: A systematic review and an analysis of economic evaluations. Int. J. Technol. Assess. Health Care 2009, 25, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Gray, D.J.P.; Sidaway-Lee, K.; White, E.; Thorne, A.; Evans, P.H. Continuity of care with doctors—A matter of life and death? A systematic review of continuity of care and mortality. BMJ Open 2018, 8, e021161. [Google Scholar] [CrossRef] [PubMed]
- Datta, S.K.; Bonnet, C.; Gyrard, A.; Da Costa, R.P.F.; Boudaoud, K. Applying Internet of Things for personalized healthcare in smart homes. In 2015 24th Wireless and Optical Communication Conference (WOCC); IEEE: Manhattan, NY, USA, 2015; pp. 164–169. [Google Scholar]
- Goodman, B.; Flaxman, S. European Union regulations on algorithmic decision-making and a “right to explanation”. AI Mag. 2017, 38, 50–57. [Google Scholar] [CrossRef]
- Arrieta, A.B.; Díaz-Rodríguez, N.; Del Ser, J.; Bennetot, A.; Tabik, S.; Barbado, A.; Garcia, S.; Gil-López, S.; Molina, D.; Benjamins, R.; et al. Explainable Artificial Intelligence (XAI): Concepts, taxonomies, opportunities and challenges toward responsible AI. Inf. Fusion 2020, 58, 82–115. [Google Scholar] [CrossRef]
- Peterson, M.C.; Holbrook, J.H.; Von Hales, D.; Smith, N.; Staker, L. Contributions of the history, physical examination, and laboratory investigation in making medical diagnoses. West. J. Med. 1992, 156, 163. [Google Scholar] [CrossRef]
- Roshan, M.; Rao, A. A study on relative contributions of the history, physical examination and investigations in making medical diagnosis. J. Assoc. Physicians India 2000, 48, 771–775. [Google Scholar]
- Gruber, T.R. A translation approach to portable ontology specifications. Knowl. Acquis. 1993, 5, 199–220. [Google Scholar] [CrossRef]
- Haveman-Nies, A.; de Groot, L.P.G.M.; Burema, J.; Cruz, J.A.A.; Osler, M.; van Staveren, W.A. Dietary quality and lifestyle factors in relation to 10-year mortality in older Europeans: The SENECA study. Am. J. Epidemiol. 2002, 156, 962–968. [Google Scholar] [CrossRef]
- World Health Organization. Disability-Adjusted Life Years (DALYs)-The Global Health Observatory. Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/158 (accessed on 21 August 2021).
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Adel, E.; El-Sappagh, S.; Barakat, S.; Elmogy, M. Ontology-based electronic health record semantic interoperability: A survey. In U-Healthcare Monitoring Systems; Elsevier: Amsterdam, The Netherlands, 2019; pp. 315–352. [Google Scholar]
- Roehrs, A.; da Costa, C.A.; da Rosa Righi, R.; Rigo, S.J.; Wichman, M.H. Toward a model for personal health record interoperability. IEEE J. Biomed. Health Inform. 2018, 23, 867–873. [Google Scholar] [CrossRef]
- Blomqvist, E. The use of Semantic Web technologies for decision support–A survey. Semant. Web 2014, 5, 177–201. [Google Scholar] [CrossRef]
- Spoladore, D. Ontology-based decision support systems for health data management to support collaboration in ambient assisted living and work reintegration. In Working Conference on Virtual Enterprises; Springer: Berlin/Heidelberg, Germany, 2017; pp. 341–352. [Google Scholar]
- Turhan, A.-Y. Description logic reasoning for semantic web ontologies. In Proceedings of the International Conference on Web Intelligence, Mining and Semantics, Sogndal, Norway, 25–27 May 2011; pp. 1–5. [Google Scholar]
- Chen, L.; Nugent, C.; Mulvenna, M.; Finlay, D.; Hong, X. Semantic smart homes: Towards knowledge rich assisted living environments. In Intelligent Patient Management; Springer: Berlin/Heidelberg, Germany, 2009; pp. 279–296. [Google Scholar]
- Spoladore, D.; Mahroo, A.; Trombetta, A.; Sacco, M. DOMUS: A domestic ontology managed ubiquitous system. J. Ambient Intell. Humaniz. Comput. 2021, 1–16. [Google Scholar] [CrossRef]
- Spoladore, D.; Arlati, S.; Colombo, V.; Modoni, G.; Sacco, M. A semantic-enabled smart home for AAL and continuity of care. In IoT in Healthcare and Ambient Assisted Living; Springer: Berlin/Heidelberg, Germany, 2021; pp. 343–371. [Google Scholar]
- Arlati, S.; Spoladore, D.; Mottura, S.; Zangiacomi, A.; Ferrigno, G.; Sacchetti, R.; Sacco, M. Analysis for the design of a novel integrated framework for the return to work of wheelchair users. Work 2018, 61, 603–625. [Google Scholar] [CrossRef]
- Bailoni, T.; Dragoni, M.; Eccher, C.; Guerini, M.; Maimone, R. Healthy lifestyle support: The perkapp ontology. In OWL: Experiences and Directions–Reasoner Evaluation; Springer: Berlin/Heidelberg, Germany, 2016; pp. 15–23. [Google Scholar]
- Chi, Y.-L.; Chen, T.-Y.; Tsai, W.-T. A chronic disease dietary consultation system using OWL-based ontologies and semantic rules. J. Biomed. Inform. 2015, 53, 208–219. [Google Scholar] [CrossRef]
- Cioara, T.; Anghel, I.; Salomie, I.; Barakat, L.; Miles, S.; Reidlinger, D.; Taweel, A.; Dobre, C.; Pop, F. Expert system for nutrition care process of older adults. Future Gener. Comput. Syst. 2018, 80, 368–383. [Google Scholar] [CrossRef]
- Lee, C.-S.; Wang, M.-H.; Lan, S.-T. Adaptive personalized diet linguistic recommendation mechanism based on type-2 fuzzy sets and genetic fuzzy markup language. IEEE Trans. Fuzzy Syst. 2014, 23, 1777–1802. [Google Scholar] [CrossRef]
- Faiz, I.; Mukhtar, H.; Qamar, A.M.; Khan, S. A semantic rules & reasoning based approach for Diet and Exercise management for diabetics. In 2014 International Conference on Emerging Technologies (ICET); IEEE: Manhattan, NY, USA, 2014; pp. 94–99. [Google Scholar]
- Fudholi, D.H.; Maneerat, N.; Varakulsiripunth, R. Ontology-based daily menu assistance system. In 2009 6th International Conference on Electrical Engineering/Electronics, Computer, Telecommunications and Information Technology; IEEE: Manhattan, NY, USA, 2009; Volume 2, pp. 694–697. [Google Scholar]
- Espín, V.; Hurtado, M.V.; Noguera, M. Nutrition for Elder Care: A nutritional semantic recommender system for the elderly. Expert Syst. 2016, 33, 201–210. [Google Scholar] [CrossRef]
- Subramaniyaswamy, V.; Manogaran, G.; Logesh, R.; Vijayakumar, V.; Chilamkurti, N.; Malathi, D.; Senthilselvan, N. An ontology-driven personalized food recommendation in IoT-based healthcare system. J. Supercomput. 2019, 75, 3184–3216. [Google Scholar] [CrossRef]
- Bianchini, D.; De Antonellis, V.; De Franceschi, N.; Melchiori, M. PREFer: A prescription-based food recommender system. Comput. Stand. Interfaces 2017, 54, 64–75. [Google Scholar] [CrossRef]
- Agapito, G.; Simeoni, M.; Calabrese, B.; Caré, I.; Lamprinoudi, T.; Guzzi, P.H.; Pujia, A.; Fuiano, G.; Cannataro, M. DIETOS: A dietary recommender system for chronic diseases monitoring and management. Comput. Methods Programs Biomed. 2018, 153, 93–104. [Google Scholar] [CrossRef]
- Pan, J.Z. Resource description framework. In Handbook on Ontologies; Springer: Berlin/Heidelberg, Germany, 2009; pp. 71–90. [Google Scholar]
- Antoniou, G.; Van Harmelen, F. Web ontology language: Owl. In Handbook on Ontologies; Springer: Berlin/Heidelberg, Germany, 2004; pp. 67–92. [Google Scholar]
- Spoladore, D.; Pessot, E. Collaborative Ontology Engineering Methodologies for the Development of Decision Support Systems: Case Studies in the Healthcare Domain. Electronics 2021, 10, 1060. [Google Scholar] [CrossRef]
- Horrocks, I.; Patel-Schneider, P.F.; Boley, H.; Tabet, S.; Grosof, B.; Dean, M. SWRL: A semantic web rule language combining OWL and RuleML. W3C Memb. Submiss. 2004, 21, 1–31. [Google Scholar]
- Union, S. Stardog-the Enterprise Knowledge Graph Platform. Available online: https://www.stardog.com/categories/knowledge-graph/ (accessed on 29 August 2021).
- Quilitz, B.; Leser, U. Querying distributed RDF data sources with SPARQL. In European Semantic Web Conference; Springer: Berlin/Heidelberg, Germany, 2008; pp. 524–538. [Google Scholar]
- Tudorache, T.; Noy, N.F.; Tu, S.; Musen, M.A. Supporting collaborative ontology development in Protégé. In International Semantic Web Conference; Springer: Berlin/Heidelberg, Germany, 2008; pp. 17–32. [Google Scholar]
- Graves, M.; Constabaris, A.; Brickley, D. Foaf: Connecting people on the semantic web. Cat. Classif. Q. 2007, 43, 191–202. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Diseases for Mortality and Morbidity Statistics (11th Revision). Available online: https://www.who.int/classifications/classification-of-diseases (accessed on 29 August 2021).
- World Health Organization. International Classification of Functioning, Disability and Health. Available online: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health (accessed on 29 August 2021).
- Fransvea, A.; Celano, G.; Pagliarone, C.N.; Disanto, C.; Balzaretti, C.; Celano, G.V.; Bonerba, E. Food labelling: A brief analysis of European Regulation 1169/2011. Ital. J. Food Saf. 2014, 3, 1703. [Google Scholar] [CrossRef][Green Version]
- Dooley, D.M.; Griffiths, E.J.; Gosal, G.S.; Buttigieg, P.L.; Hoehndorf, R.; Lange, M.C.; Schriml, L.M.; Brinkman, F.S.; Hsiao, W.W. FoodOn: A harmonized food ontology to increase global food traceability, quality control and data integration. NPJ Sci. Food 2018, 2, 1–10. [Google Scholar] [CrossRef]
- Collins, P.F.; Yang, I.A.; Chang, Y.-C.; Vaughan, A. Nutritional support in chronic obstructive pulmonary disease (COPD): An evidence update. J. Thorac. Dis. 2019, 11, S2230. [Google Scholar] [CrossRef]
- Mann, J.; De Leeuw, I.; Hermansen, K.; Karamanos, B.; Karlström, B.; Katsilambros, N.; Riccardi, G.; Rivellese, A.; Rizkalla, S.; Slama, G.; et al. Evidence-based nutritional approaches to the treatment and prevention of diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2004, 14, 373–394. [Google Scholar] [CrossRef]
- Rawal, G.; Yadav, S. Nutrition in chronic obstructive pulmonary disease: A review. J. Transl. Intern. Med. 2015, 3, 151. [Google Scholar] [CrossRef]
- Schols, A.M.; Ferreira, I.M.; Franssen, F.M.; Gosker, H.R.; Janssens, W.; Muscaritoli, M.; Pison, C.; Rutten-van Mölken, M.; Slinde, F.; Steiner, M.C.; et al. Nutritional assessment and therapy in COPD: A European Respiratory Society statement. Eur. Respir. J. 2014, 44, 1504–1520. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef]
- Kim, C.; Park, Y.B.; Park, S.Y.; Park, S.; Kim, C.-H.; Park, S.M.; Lee, M.-G.; Hyun, I.-G.; Jung, K.-S.; Kim, D.-G. COPD patients with exertional desaturation are at a higher risk of rapid decline in lung function. Yonsei Med. J. 2014, 55, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Arlati, S.; Colombo, V.; Spoladore, D.; Greci, L.; Pedroli, E.; Serino, S.; Cipresso, P.; Goulene, K.; Stramba-Badiale, M.; Riva, G.; et al. A social virtual reality-based application for the physical and cognitive training of the elderly at home. Sensors 2019, 19, 261. [Google Scholar] [CrossRef]
- Baldassini, D.; Colombo, V.; Spoladore, D.; Sacco, M.; Arlati, S. Customization of domestic environment and physical training supported by virtual reality and semantic technologies: A use-case. In 2017 IEEE 3rd International Forum on Research and Technologies for Society and Industry (RTSI); IEEE: Manhattan, NY, USA, 2017; pp. 1–6. [Google Scholar]
- Spoladore, D.; Sacco, M. Towards a collaborative ontology-based decision support system to foster healthy and tailored diets. In Working Conference on Virtual Enterprises; Springer: Berlin/Heidelberg, Germany, 2020; pp. 634–643. [Google Scholar]
- Gandy, J. Water intake: Validity of population assessment and recommendations. Eur. J. Nutr. 2015, 54, 11–16. [Google Scholar] [CrossRef]
- Mahroo, A.; Spoladore, D.; Nolich, M.; Buqi, R.; Carciotti, S.; Sacco, M. Smart cabin: A semantic-based framework for indoor comfort customization inside a cruise cabin. In Fourth International Congress on Information and Communication Technology; Springer: Berlin/Heidelberg, Germany, 2020; pp. 41–53. [Google Scholar]
- Unity 3D Real-Time Development Platform. Available online: https://www.unity.com/ (accessed on 29 August 2021).
- Pizzagalli, S.; Spoladore, D.; Arlati, S.; Sacco, M.; Greci, L. HIC: An interactive and ubiquitous home controller system for the smart home. In 2018 IEEE 6th International Conference on Serious Games and Applications for Health (SeGAH); IEEE: Manhattan, NY, USA, 2018; pp. 1–6. [Google Scholar]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.-C.; et al. An official American Thoracic Society/European Respiratory Society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef] [PubMed]
- Celjuska, D.; Vargas-Vera, M. Ontosophie: A semi-automatic system for ontology population from text. In Proceedings of the International Conference on Natural Language Processing (ICON), Hyderabad, India, 19–22 December 2004; Volume 60. [Google Scholar]
- Su, M.-H.; Wu, C.-H.; Shih, P.-C. Automatic ontology population using deep learning for triple extraction. In 2019 Asia-Pacific Signal and Information Processing Association Annual Summit and Conference (APSIPA ASC); IEEE: Manhattan, NY, USA, 2019; pp. 262–267. [Google Scholar]
- Meydani, M. Nutrition interventions in aging and age-associated disease. Ann. N. Y. Acad. Sci. 2001, 928, 226–235. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ICD Code | CA22: Chronic Obstructive Pulmonary Diseases |
|---|---|
| ICF Code | Qualifier |
| s430 Structure of Respiratory System | |
| s4301 Lungs | |
| s43011 Alveoli | 2 |
| s770 Additional Musculoskeletal Structures Related to Movement | 1 |
| s7702 Muscles | |
| b130 Energy and Drive Functions | |
| b1301 Motivation | 1 |
| b1302 Appetite | 1 |
| b430 Hematological System Functions | |
| b4301 Oxygen-Carrying Functions of the Blood | 2 |
| b440 Respiration Functions | 2 |
| b445 Respiratory Muscle Functions | 2 |
| b455 Exercise Tolerance Functions | 2 |
| b460 Sensations Associated with Cardiovascular and Respiratory Functions | 2 |
| b530 Weight Maintenance Functions | 2 |
| b730 Muscle Power Functions | 2 |
| b740 Muscle Endurance Functions | 2 |
| ICD Code | C5A11: Type 2 Diabetes Mellitus |
|---|---|
| ICF Code | Qualifier |
| s410 Structure of Cardiovascular System | 1 |
| S610 Structure of Urinary System | |
| S6100 Kidney | 2 |
| b410 Heart Functions | 1 |
| b415 Blood Vessel Functions | 1 |
| b420 Blood Pressure Functions | 1 |
| b435 Immunological System Functions | 2 |
| b455 Exercise Tolerance Functions | 2 |
| b540 General Metabolic Functions | 2 |
| b610 Urinary Excretory Functions | 1 |
| Dish | James | Grace |
|---|---|---|
| Black tea | Adequate | Healthy |
| Green tea | Adequate | Healthy |
| Milk (low fat) | Healthy | Adequate |
| Milk (skimmed, pasteurized) | Healthy | Adequate |
| Wheat bran | Healthy | Healthy |
| Rye bran | Healthy | Healthy |
| Wheat bread | Healthy | Adequate |
| White bread (slice) | Adequate | Unhealthy |
| Whole rye bread | Healthy | Adequate |
| Boiled carrots | Healthy | Healthy |
| Endive salad with olive oil | Healthy | Healthy |
| Raw carrot salad with olive oil | Healthy | Healthy |
| Tomato chickpeas | Healthy | Healthy |
| Peas and onions | Healthy | Adequate |
| Boiled beans | Adequate | Healthy |
| French fries | Unhealthy | Unhealthy |
| Bresaola and stracchino rolls | Unhealthy | Healthy |
| Potato and onions omelet | Healthy | Adequate |
| Fried chicken | Unhealthy | Unhealthy |
| Grilled chicken | Healthy | Healthy |
| Fried cod fillet | Unhealthy | Unhealthy |
| Poached cod fillet | Healthy | Healthy |
| Pan-seared salmon | Healthy | Healthy |
| French onion soup | Unhealthy | Unhealthy |
| Tomato pasta | Adequate | Unhealthy |
| Tagliatelle with pesto sauce | Adequate | Unhealthy |
| Rosemary risotto | Healthy | Adequate |
| Sliced apple | Healthy | Healthy |
| Sliced pear | Healthy | Healthy |
| Peeled banana | Healthy | Healthy |
| Peeled orange | Healthy | Healthy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spoladore, D.; Colombo, V.; Arlati, S.; Mahroo, A.; Trombetta, A.; Sacco, M. An Ontology-Based Framework for a Telehealthcare System to Foster Healthy Nutrition and Active Lifestyle in Older Adults. Electronics 2021, 10, 2129. https://doi.org/10.3390/electronics10172129
Spoladore D, Colombo V, Arlati S, Mahroo A, Trombetta A, Sacco M. An Ontology-Based Framework for a Telehealthcare System to Foster Healthy Nutrition and Active Lifestyle in Older Adults. Electronics. 2021; 10(17):2129. https://doi.org/10.3390/electronics10172129
Chicago/Turabian StyleSpoladore, Daniele, Vera Colombo, Sara Arlati, Atieh Mahroo, Alberto Trombetta, and Marco Sacco. 2021. "An Ontology-Based Framework for a Telehealthcare System to Foster Healthy Nutrition and Active Lifestyle in Older Adults" Electronics 10, no. 17: 2129. https://doi.org/10.3390/electronics10172129
APA StyleSpoladore, D., Colombo, V., Arlati, S., Mahroo, A., Trombetta, A., & Sacco, M. (2021). An Ontology-Based Framework for a Telehealthcare System to Foster Healthy Nutrition and Active Lifestyle in Older Adults. Electronics, 10(17), 2129. https://doi.org/10.3390/electronics10172129