

Arrhythmia Detection Based on WGAN-GP and SE-ResNet1D

Abstract
1. Introduction
- The training of the model relies on a large number of accurately annotated datasets, while ECG, as a sensitive medical dataset involving patient privacy, is difficult to obtain in large quantities, and the datasets need to be annotated and proofread by professional doctors, which will consume a lot of medical resources [5,6].
- ECGs have a predominantly normal heart rate and a low abnormal heart rate, so the sample size between each category of the ECG dataset is often highly imbalanced. The imbalance in the number of samples of ECG signals from different categories affects the performance of the classifier. Models trained on imbalanced datasets usually do not perform well, especially in the determination of abnormal categories [7,8].
- The experiments in most papers randomly disrupted the heartbeats of all patients and then divided the training and test sets, which resulted in high test accuracy but poor practical results. This is because ECG signals vary significantly from patient to patient, and therefore, the generalization performance of the model is reduced in this training approach [9].
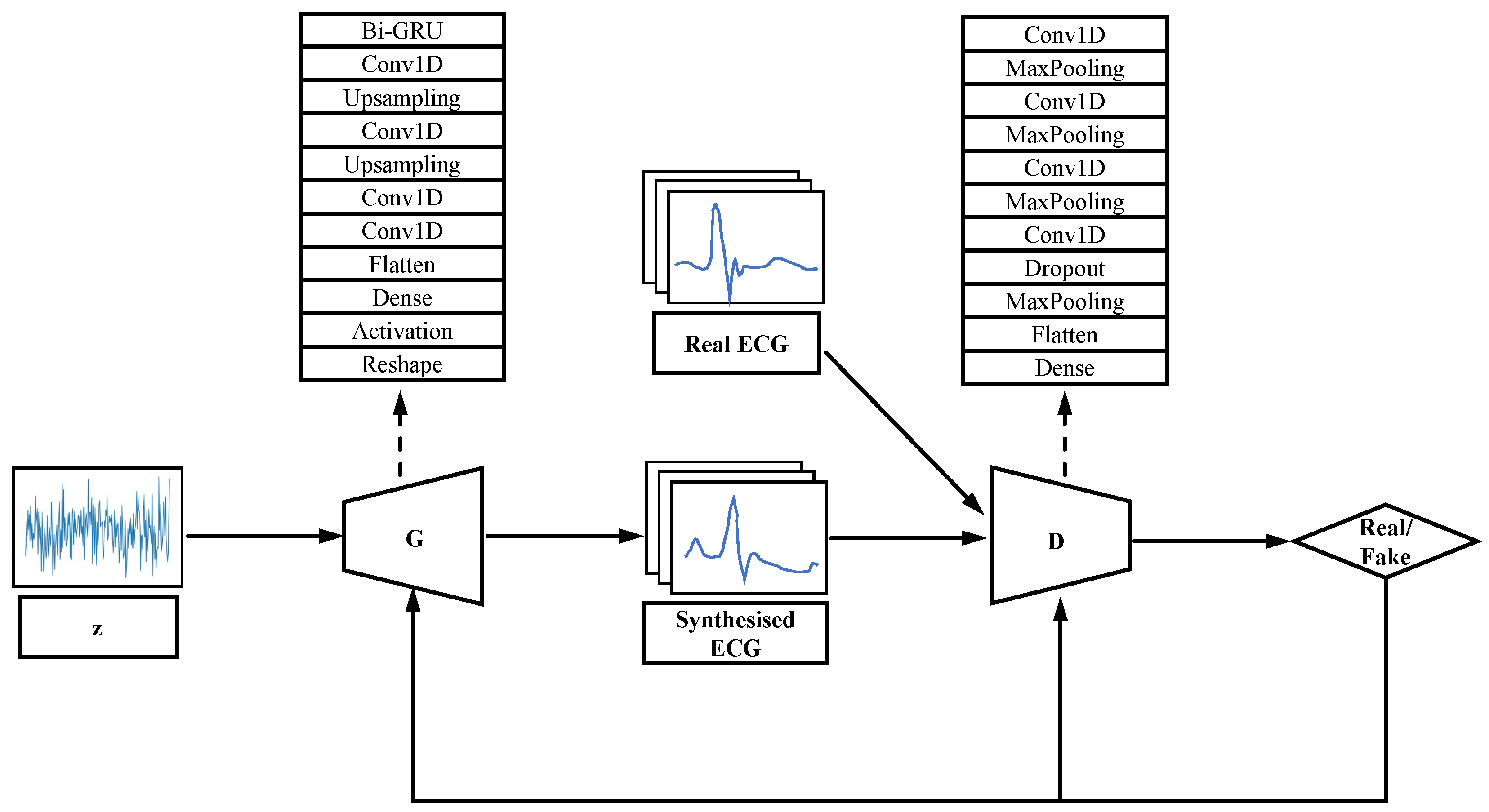
- We improve the structure of WGAN-GP. A Bi-GRU layer is embedded into the generator of the neurogenerative model to endorse the temporal constraint for better ECG synthesis.
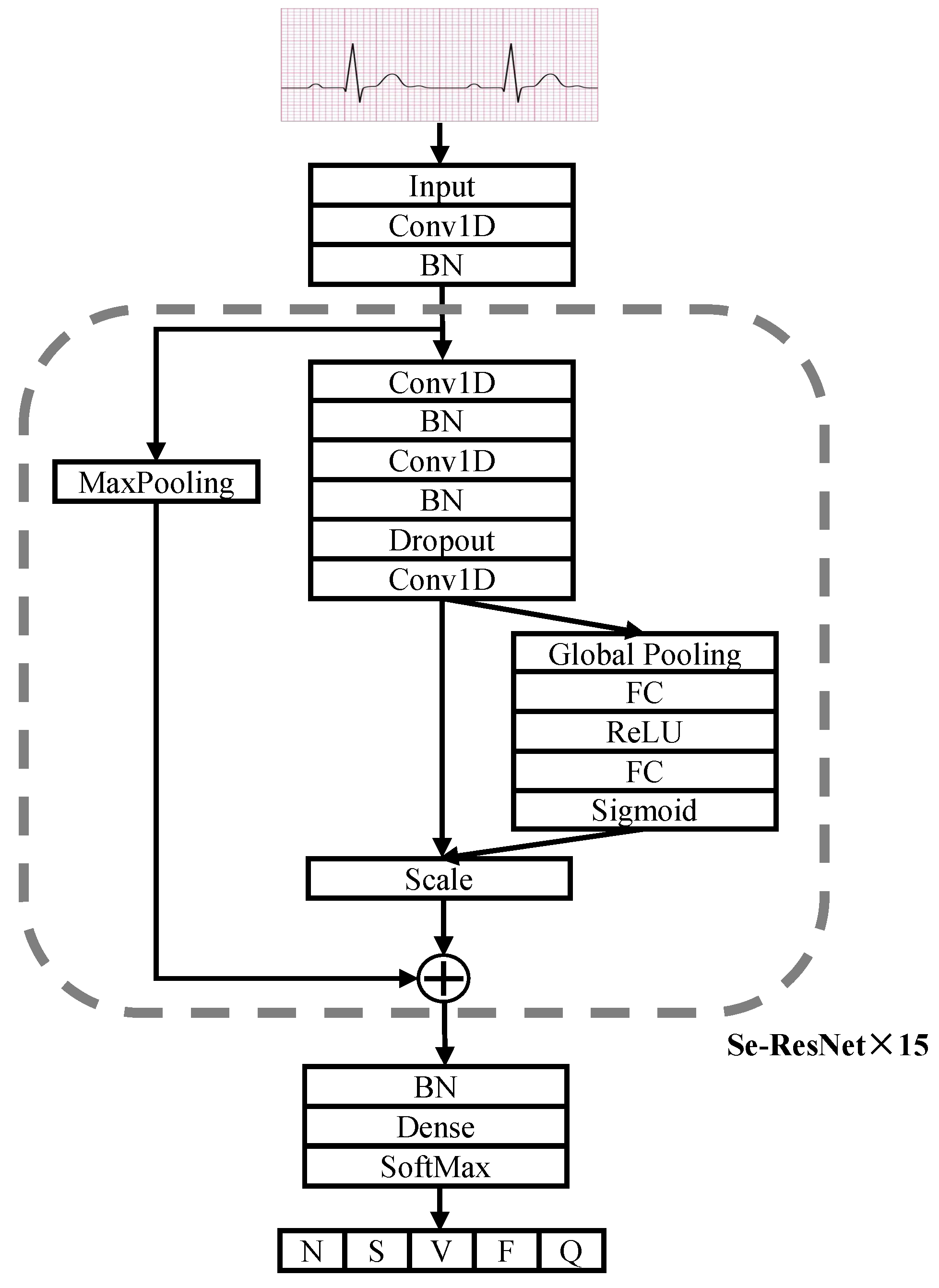
- We redesigned the structure of SE-ResNet to a one-dimensional model to classify ECG signals.
- Our experimental dataset was divided using AAMI and inter-patient, which is more in line with the medical reality. Our experiments demonstrate that the above improvements can significantly improve the performance of arrhythmia classification.
2. Related Work
2.1. Deep Learning Network-Based ECG Classification
2.2. GAN Based ECG Signal Synthesize
3. Background
3.1. WGAN-GP
3.2. SE-ResNet
4. Proposed Method
4.1. WGAN-GP Based ECG Synthesised Model
4.2. SE-ResNet1D Based ECG Classification Model
5. Datasets and Data Pre-Processing
5.1. Introduction to the Data Set
5.2. Data Pre-Processing
5.2.1. Heartbeat Segmentation
5.2.2. Wavelet Threshold Noise Reduction
5.2.3. Data Set Partitioning
6. Experiments
6.1. Experimental Settings
6.2. Experimental Results and Analysis
7. Discussion and Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Nie, Z.; Xu, H.; Chen, C.; Gan, Y.; Chen, G.; Wang, C.; Yue, W.; Yan, F.; Feng, Y.; Lu, Z. Population Attributable Risks of Potential Modifiable Factors for Atrial Fibrillation in China: A National Survey. Risk Manag. Healthc. Policy 2022, 15, 1215. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.; Afghah, F. Inter-and intra-patient ecg heartbeat classification for arrhythmia detection: A sequence to sequence deep learning approach. In Proceedings of the ICASSP 2019—2019 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Brighton, UK, 12–17 May 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 1308–1312. [Google Scholar]
- Salem, M.; Taheri, S.; Yuan, J.S. ECG arrhythmia classification using transfer learning from 2-dimensional deep CNN features. In Proceedings of the 2018 IEEE Biomedical Circuits and Systems Conference (BioCAS), Cleveland, OH, USA, 17–19 October 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 1–4. [Google Scholar]
- Moody, G.B.; Mark, R.G. The impact of the MIT-BIH arrhythmia database. IEEE Eng. Med. Biol. Mag. 2001, 20, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Strodthoff, N.; Wagner, P.; Schaeffter, T.; Samek, W. Deep learning for ECG analysis: Benchmarks and insights from PTB-XL. IEEE J. Biomed. Health Inform. 2020, 25, 1519–1528. [Google Scholar] [CrossRef]
- Petmezas, G.; Haris, K.; Stefanopoulos, L.; Kilintzis, V.; Tzavelis, A.; Rogers, J.A.; Katsaggelos, A.K.; Maglaveras, N. Automated atrial fibrillation detection using a hybrid CNN-LSTM network on imbalanced ECG datasets. Biomed. Signal Process. Control 2021, 63, 102194. [Google Scholar] [CrossRef]
- Murat, F.; Yildirim, O.; Talo, M.; Baloglu, U.B.; Demir, Y.; Acharya, U.R. Application of deep learning techniques for heartbeats detection using ECG signals-analysis and review. Comput. Biol. Med. 2020, 120, 103726. [Google Scholar] [CrossRef] [PubMed]
- Mar, T.; Zaunseder, S.; Martínez, J.P.; Llamedo, M.; Poll, R. Optimization of ECG classification by means of feature selection. IEEE Trans. Biomed. Eng. 2011, 58, 2168–2177. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Boulanger, P. A survey of heart anomaly detection using ambulatory Electrocardiogram (ECG). Sensors 2020, 20, 1461. [Google Scholar] [CrossRef]
- Maweu, B.M.; Dakshit, S.; Shamsuddin, R.; Prabhakaran, B. CEFEs: A CNN explainable framework for ECG signals. Artif. Intell. Med. 2021, 115, 102059. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.; Lin, Y.T.; Lee, S.J.; Tsai, W.C.; Huang, T.C.; Liu, Y.H.; Cheng, M.C.; Dai, C.Y. Automated ECG classification based on 1D deep learning network. Methods 2022, 202, 127–135. [Google Scholar] [CrossRef]
- Rai, H.M.; Chatterjee, K. Hybrid CNN-LSTM deep learning model and ensemble technique for automatic detection of myocardial infarction using big ECG data. Appl. Intell. 2022, 52, 5366–5384. [Google Scholar] [CrossRef]
- Jahmunah, V.; Ng, E.; Tan, R.S.; Oh, S.L.; Acharya, U.R. Explainable detection of myocardial infarction using deep learning models with Grad-CAM technique on ECG signals. Comput. Biol. Med. 2022, 146, 105550. [Google Scholar] [CrossRef]
- Attallah, O. ECG-BiCoNet: An ECG-based pipeline for COVID-19 diagnosis using Bi-Layers of deep features integration. Comput. Biol. Med. 2022, 142, 105210. [Google Scholar] [CrossRef]
- Li, W.; Tang, Y.M.; Yu, K.M.; To, S. SLC-GAN: An automated myocardial infarction detection model based on generative adversarial networks and convolutional neural networks with single-lead electrocardiogram synthesis. Inf. Sci. 2022, 589, 738–750. [Google Scholar] [CrossRef]
- Chen, J.; Liao, K.; Wei, K.; Ying, H.; Chen, D.Z.; Wu, J. ME-GAN: Learning panoptic electrocardio representations for multi-view ECG synthesis conditioned on heart diseases. In Proceedings of the International Conference on Machine Learning, PMLR, Baltimore, MD, USA, 17–23 July 2022; pp. 3360–3370. [Google Scholar]
- Rafi, T.H.; Woong-Ko, Y. HeartNet: Self Multi-Head Attention Mechanism via Convolutional Network with Adversarial Data Synthesis for ECG-based Arrhythmia Classification. IEEE Access 2022, 10, 2169–3536. [Google Scholar] [CrossRef]
- Ma, S.; Cui, J.; Chen, C.L.; Chen, X.; Ma, Y. An Effective Data Enhancement Method for Classification of ECG Arrhythmia. Measurement 2022, 203, 111978. [Google Scholar] [CrossRef]
- Ma, K.; Chang’an, A.Z.; Yang, F. Multi-classification of arrhythmias using ResNet with CBAM on CWGAN-GP augmented ECG Gramian Angular Summation Field. Biomed. Signal Process. Control. 2022, 77, 103684. [Google Scholar] [CrossRef]
- Wulan, N.; Wang, W.; Sun, P.; Wang, K.; Xia, Y.; Zhang, H. Generating electrocardiogram signals by deep learning. Neurocomputing 2020, 404, 122–136. [Google Scholar] [CrossRef]
- Jin, Q.; Lin, R.; Yang, F. E-WACGAN: Enhanced generative model of signaling data based on WGAN-GP and ACGAN. IEEE Syst. J. 2019, 14, 3289–3300. [Google Scholar] [CrossRef]
- Lee, J.; Lee, H. Improving SSH detection model using IPA time and WGAN-GP. Comput. Secur. 2022, 116, 102672. [Google Scholar] [CrossRef]
- Radford, A.; Metz, L.; Chintala, S. Unsupervised representation learning with deep convolutional generative adversarial networks. arXiv 2015, arXiv:1511.06434. [Google Scholar]
- Goodfellow, I.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative adversarial networks. Commun. ACM 2020, 63, 139–144. [Google Scholar] [CrossRef]
- Arjovsky, M.; Chintala, S.; Bottou, L. Wasserstein generative adversarial networks. In Proceedings of the International Conference on Machine Learning, PMLR, Sydney, Australia, 6–11 August 2017; pp. 214–223. [Google Scholar]
- Gulrajani, I.; Ahmed, F.; Arjovsky, M.; Dumoulin, V.; Courville, A.C. Improved training of wasserstein gans. Adv. Neural Inf. Process. Syst. 2017, 30, 5769–5779. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. Imagenet large scale visual recognition challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef]
- Hu, J.; Shen, L.; Sun, G. Squeeze-and-excitation networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–22 June 2018; pp. 7132–7141. [Google Scholar]
- Zhao, Z.; Fang, H.; Relton, S.D.; Yan, R.; Liu, Y.; Li, Z.; Qin, J.; Wong, D.C. Adaptive lead weighted resnet trained with different duration signals for classifying 12-lead ecgs. In Proceedings of the 2020 Computing in Cardiology, Rimini, Italy, 13–16 September 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 1–4. [Google Scholar]
- Zhang, X.; Li, R.; Dai, H.; Liu, Y.; Zhou, B.; Wang, Z. Localization of myocardial infarction with multi-lead bidirectional gated recurrent unit neural network. IEEE Access 2019, 7, 161152–161166. [Google Scholar] [CrossRef]
- Salimans, T.; Goodfellow, I.; Zaremba, W.; Cheung, V.; Radford, A.; Chen, X. Improved techniques for training gans. Adv. Neural Inf. Process. Syst. 2016, 29, 2234–2242. [Google Scholar]
- Lourenço, A.; Silva, H.; Carreiras, C. Outlier detection in non-intrusive ECG biometric system. In Proceedings of the International Conference Image Analysis and Recognition; Springer: Berlin/Heidelberg, Germany, 2013; pp. 43–52. [Google Scholar]
- Shark, L.K.; Yu, C. Denoising by optimal fuzzy thresholding in wavelet domain. Electron. Lett. 2000, 36, 1. [Google Scholar] [CrossRef]
- Stergiou, G.S.; Alpert, B.; Mieke, S.; Asmar, R.; Atkins, N.; Eckert, S.; Frick, G.; Friedman, B.; Graßl, T.; Ichikawa, T.; et al. A universal standard for the validation of blood pressure measuring devices: Association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO) Collaboration Statement. Hypertension 2018, 71, 368–374. [Google Scholar] [CrossRef]
- Garcia, G.; Moreira, G.; Menotti, D.; Luz, E. Inter-patient ECG heartbeat classification with temporal VCG optimized by PSO. Sci. Rep. 2017, 7, 1–11. [Google Scholar] [CrossRef]
- Lai, J.; Chen, Y.; Han, B.; Ji, L.; Shi, Y.; Huang, Z.; Yang, W.; Feng, Q. A DenseNet-based diagnosis algorithm for automated diagnosis using clinical ECG data. J. South. Med. Univ. 2019, 39, 69–75. [Google Scholar]
- Ali, O.M.A.; Kareem, S.W.; Mohammed, A.S. Comparative Evaluation for Two and Five Classes ECG Signal Classification: Applied Deep Learning. J. Algebr. Stat. 2022, 13, 580–596. [Google Scholar]
- Rahul, J.; Sharma, L.D. Automatic cardiac arrhythmia classification based on hybrid 1-D CNN and Bi-LSTM model. Biocybern. Biomed. Eng. 2022, 42, 312–324. [Google Scholar] [CrossRef]
- Li, Y.; Qian, R.; Li, K. Inter-patient arrhythmia classification with improved deep residual convolutional neural network. Comput. Methods Progr. Biomed. 2022, 214, 106582. [Google Scholar] [CrossRef]
- Kaur, A.; Kumar, S.; Agarwal, R.; Agarwal, A. Intra and inter-patient arrhythmia classification using feature fusion with novel feature set based on fractional-order and fibonacci series. Biomed. Signal Process. Control 2022, 72, 103365. [Google Scholar] [CrossRef]
- Niu, J.; Tang, Y.; Sun, Z.; Zhang, W. Inter-patient ECG classification with symbolic representations and multi-perspective convolutional neural networks. IEEE J. Biomed. Health Inform. 2019, 24, 1321–1332. [Google Scholar] [CrossRef]
- Liu, T.; Si, Y.; Yang, W.; Huang, J.; Yu, Y.; Zhang, G.; Zhou, R. Inter-Patient Congestive Heart Failure Detection Using ECG-Convolution-Vision Transformer Network. Sensors 2022, 22, 3283. [Google Scholar] [CrossRef]
- Liaqat, S.; Dashtipour, K.; Zahid, A.; Assaleh, K.; Arshad, K.; Ramzan, N. Detection of atrial fibrillation using a machine learning approach. Information 2020, 11, 549. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AAMI | MIT-BIH | Number of Original | Number of Balanced |
|---|---|---|---|
| Normal (N) | N, L, R | 4551 | 5000 |
| Supraventricular (S) | A, a, J, S, j, e | 1010 | 5000 |
| Ventricular (V) | V, E | 2177 | 5000 |
| Fusion1 (F) | F | 552 | 5000 |
| Unkonwn (Q) | /, f, Q | 792 | 5000 |
| Data Set | Record |
|---|---|
| Train | 101,103,112,113,115,117,121,122,123,124,200,201,203, 205,207,208,209,210,212,213,214,215,217,219,220,221, 222,223,228,231,232,233,234 |
| Test | 100,102,104,105,106,107,108,109,111,114,116,118,119,213 |
| Methods | Original Data | Balanced Data | ||||
|---|---|---|---|---|---|---|
| Precision | Recall | F1 | Precision | Recall | F1 | |
| SE-Resnet1D | 93.16 | 93.31 | 93.23 | 95.80 | 96.75 | 96.27 |
| DenseNet | 91.55 | 92.13 | 91.84 | 93.76 | 93.39 | 93.75 |
| VGGNet | 88.16 | 90.22 | 89.13 | 93.90 | 94.18 | 94.04 |
| CNN+Bi-LSTM | 86.12 | 89.50 | 87.78 | 90.36 | 91.92 | 91.13 |
| References | Classes | Algorithm | Performance |
|---|---|---|---|
| Li et al. [40] | 5 classes | ResNet | Sensitivity of 94.54% , Positive predictivity of 93.33% and Specificity of 80.80% |
| Liu et al. [43] | 2 classes | ECVT-Net | Accuracy of 98.88%, Precision of 98.84% and Sensitivity of 98.94% |
| kaur et al. [41] | 5 classes | feature fusion with novel feature set based on fractional-order and fibonacci series | Accuracy of 92.5%, Sensitivity of 89.89% and Positive predictivity of 95.54% |
| Sidrah et al. [44] | 2 classes | 2 LSTM layers, 1 fully connected layer and 1 dropout layer | Accuracy of 86.5% |
| Niu et al. [42] | 5 classes | MPCNN | Accuracy of 96.4% and F1 of 76.6% for SVEB, 89.7% for VEB |
| Proposed method | 5 classes | WGAN-GP and SE-ResNet1D | Precision of 95.8%, Recall of 96.75% and F1 of 96.27% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qin, J.; Gao, F.; Wang, Z.; Liu, L.; Ji, C. Arrhythmia Detection Based on WGAN-GP and SE-ResNet1D. Electronics 2022, 11, 3427. https://doi.org/10.3390/electronics11213427
Qin J, Gao F, Wang Z, Liu L, Ji C. Arrhythmia Detection Based on WGAN-GP and SE-ResNet1D. Electronics. 2022; 11(21):3427. https://doi.org/10.3390/electronics11213427
Chicago/Turabian StyleQin, Jing, Fujie Gao, Zumin Wang, Lu Liu, and Changqing Ji. 2022. "Arrhythmia Detection Based on WGAN-GP and SE-ResNet1D" Electronics 11, no. 21: 3427. https://doi.org/10.3390/electronics11213427
APA StyleQin, J., Gao, F., Wang, Z., Liu, L., & Ji, C. (2022). Arrhythmia Detection Based on WGAN-GP and SE-ResNet1D. Electronics, 11(21), 3427. https://doi.org/10.3390/electronics11213427