
Decoding Skin Aging: A Review of Mechanisms, Markers, and Modern Therapies

 ,
,  , and
, and 
Abstract
1. Introduction
2. Clinical Changes in Aging Skin
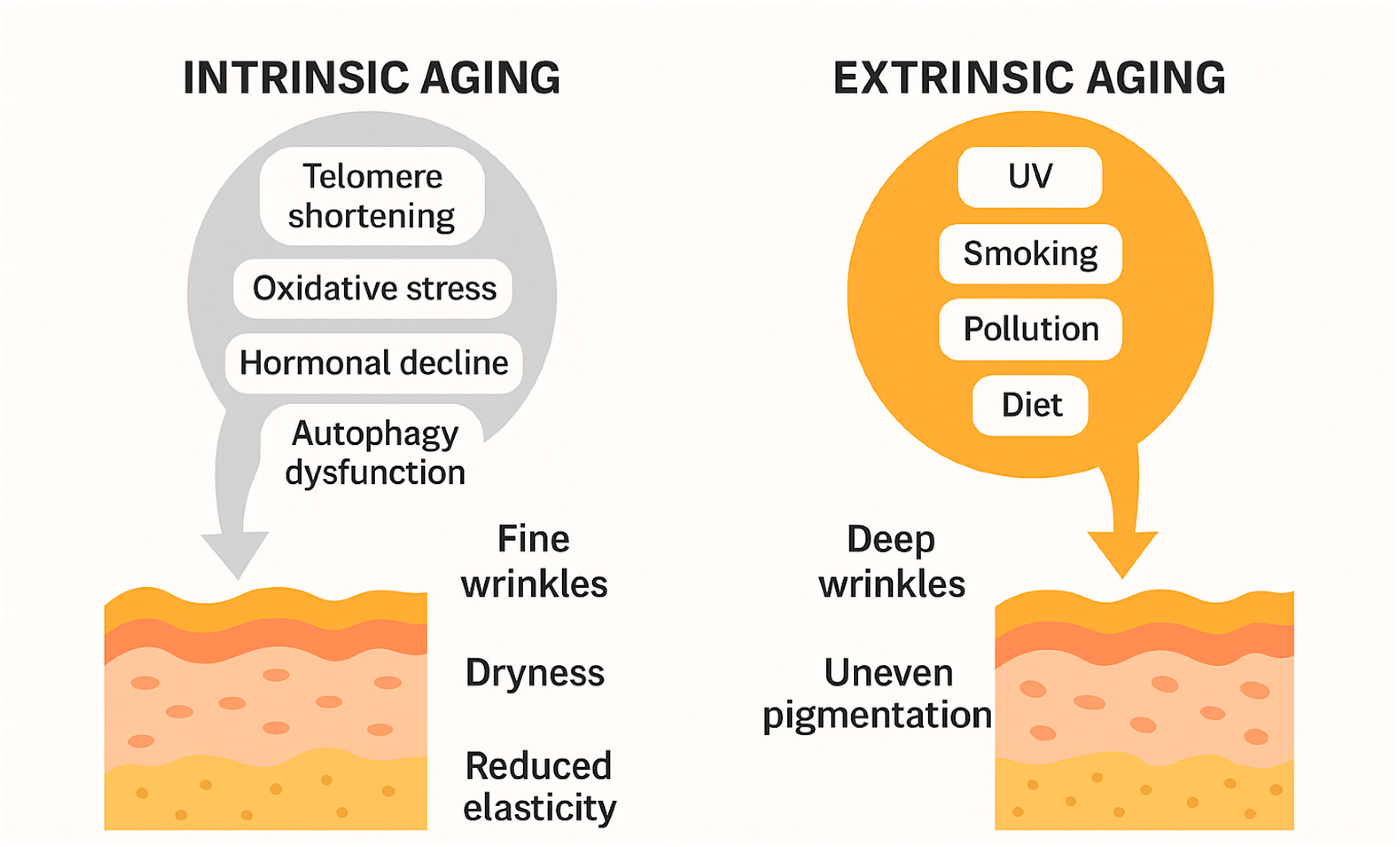
2.1. Extrinsic Aging
2.1.1. Role of UV and Blue Radiation
2.1.2. Clinical Manifestations
2.1.3. Impact of Lifestyle Factors
Environmental Pollution
Smoking
Diet
2.2. Intrinsic Aging
2.2.1. Genetic and Hormonal Influences
Genetic Changes
Hormonal Changes
2.2.2. Other Intrinsic Factors Related to Aging
Metabolic Processes
Immune System Deterioration
2.2.3. Clinical Features: Skin Thinning, Dryness, Fine Wrinkles, and Loss of Elasticity
2.2.4. Differences in Skin Aging Patterns Based on Phototypes
3. Alterations in the Histology of Aging Skin
3.1. The Molecular Mechanisms of Skin Aging
3.1.1. Telomere Shortening
3.1.2. Oxidative Stress and MMPs
3.1.3. The Role of Cytokines in Aging Skin
3.1.4. Regulation of Autophagy
3.1.5. Skin Aging and Apoptosis
3.1.6. The Function of MicroRNAs in the Aging of the Skin
3.1.7. The Microbiome of the Skin
4. Therapeutic Approaches to Skin Aging
4.1. Topical Therapies
4.2. Light-Based Therapies
4.2.1. Intense Pulsed Light (IPL)
4.2.2. Laser Therapies
4.2.3. Photodynamic Therapy (PDT)
4.3. Mechanical Rejuvenation Techniques
4.3.1. Microdermabrasion
4.3.2. Microneedling
4.3.3. Chemical Peels
4.4. Injectable and Minimally Invasive Procedures
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lai-Cheong, J.E.; McGrath, J.A. Structure and Function of Skin, Hair and Nails. Medicine 2009, 37, 223–226. [Google Scholar] [CrossRef]
- Khavkin, J.; Ellis, D.A.F. Aging Skin: Histology, Physiology, and Pathology. Facial Plast. Surg. Clin. N. Am. 2011, 19, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Farage, M.A.; Miller, K.W.; Elsner, P.; Maibach, H.I. Structural Characteristics of the Aging Skin: A Review. Cutan. Ocul. Toxicol. 2007, 26, 343–357. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.; Geyer, S.; Weninger, W.; Guimberteau, J.; Wong, J.K. The Dynamic Anatomy and Patterning of Skin. Exp. Dermatol. 2016, 25, 92–98. [Google Scholar] [CrossRef]
- Rorteau, J.; Chevalier, F.P.; Fromy, B.; Lamartine, J. Functional integrity of aging skin, from cutaneous biology to anti-aging strategies. Med. Sci. 2020, 36, 1155–1162. [Google Scholar] [CrossRef]
- Boismal, F.; Serror, K.; Dobos, G.; Zuelgaray, E.; Bensussan, A.; Michel, L. Skin aging: Pathophysiology and innovative therapies. Med. Sci. 2020, 36, 1163–1172. [Google Scholar] [CrossRef]
- Wong, Q.Y.A.; Chew, F.T. Defining Skin Aging and Its Risk Factors: A Systematic Review and Meta-Analysis. Sci. Rep. 2021, 11, 22075. [Google Scholar] [CrossRef]
- Quan, T. Molecular Insights of Human Skin Epidermal and Dermal Aging. J. Dermatol. Sci. 2023, 112, 48–53. [Google Scholar] [CrossRef]
- Brar, G.; Dhaliwal, A.; Brar, A.S.; Sreedevi, M.; Ahmadi, Y.; Irfan, M.; Golbari, R.; Zumárraga, D.; Yateem, D.; Lysak, Y.; et al. A Comprehensive Review of the Role of UV Radiation in Photoaging Processes Between Different Types of Skin. Cureus 2025, 17, e81109. [Google Scholar] [CrossRef]
- De Gálvez, E.N.; Aguilera, J.; Solis, A.; De Gálvez, M.V.; De Andrés, J.R.; Herrera-Ceballos, E.; Gago-Calderon, A. The Potential Role of UV and Blue Light from the Sun, Artificial Lighting, and Electronic Devices in Melanogenesis and Oxidative Stress. J. Photochem. Photobiol. B Biol. 2022, 228, 112405. [Google Scholar] [CrossRef]
- Austin, E.; Geisler, A.N.; Nguyen, J.; Kohli, I.; Hamzavi, I.; Lim, H.W.; Jagdeo, J. Visible Light. Part I: Properties and Cutaneous Effects of Visible Light. J. Am. Acad. Dermatol. 2021, 84, 1219–1231. [Google Scholar] [CrossRef] [PubMed]
- Laughery, M.F.; Wilson, H.E.; Sewell, A.; Stevison, S.; Wyrick, J.J. The Surprising Diversity of UV-Induced Mutations. Adv. Genet. 2024, 5, 2300205. [Google Scholar] [CrossRef]
- Solano, F. Photoprotection and Skin Pigmentation: Melanin-Related Molecules and Some Other New Agents Obtained from Natural Sources. Molecules 2020, 25, 1537. [Google Scholar] [CrossRef] [PubMed]
- Park, J.I.; Kim, S.J.; Kim, Y.J.; Lee, S.J. Protective Role of Caesalpinia Sappan Extract and Its Main Component Brazilin against Blue Light–Induced Damage in Human Fibroblasts. J. Cosmet. Dermatol. 2022, 21, 7025–7034. [Google Scholar] [CrossRef] [PubMed]
- Campiche, R.; Curpen, S.J.; Lutchmanen-Kolanthan, V.; Gougeon, S.; Cherel, M.; Laurent, G.; Gempeler, M.; Schuetz, R. Pigmentation Effects of Blue Light Irradiation on Skin and How to Protect against Them. Int. J. Cosmet. Sci. 2020, 42, 399–406. [Google Scholar] [CrossRef]
- Lim, H.W.; Kohli, I.; Ruvolo, E.; Kolbe, L.; Hamzavi, I.H. Impact of Visible Light on Skin Health: The Role of Antioxidants and Free Radical Quenchers in Skin Protection. J. Am. Acad. Dermatol. 2022, 86, S27–S37. [Google Scholar] [CrossRef]
- Chung, Y.H.; Jeong, S.A.; Choi, H.S.; Ro, S.; Lee, J.S.; Park, J.K. Protective Effects of Ginsenoside Rg2 and Astaxanthin Mixture against UVB-Induced DNA Damage. Anim. Cells Syst. 2018, 22, 400–406. [Google Scholar] [CrossRef]
- Brown, A.; Trullas, C.; Jourdan, E. Cell and Tissue-Based Models for Evaluating the Cutaneous Impact of Visible Light. J. Photochem. Photobiol. 2024, 19, 100216. [Google Scholar] [CrossRef]
- Losi, A.; Gardner, K.H.; Möglich, A. Blue-Light Receptors for Optogenetics. Chem. Rev. 2018, 118, 10659–10709. [Google Scholar] [CrossRef]
- Gallego-Rentero, M.; López Sánchez, A.; Nicolás-Morala, J.; Alcaraz-Laso, P.; Zhang, N.; Juarranz, Á.; González, S.; Carrasco, E. The Effect of Fernblock® in Preventing Blue-Light-Induced Oxidative Stress and Cellular Damage in Retinal Pigment Epithelial Cells Is Associated with NRF2 Induction. Photochem. Photobiol. Sci. 2024, 23, 1471–1484. [Google Scholar] [CrossRef]
- Suh, S.; Choi, E.H.; Atanaskova Mesinkovska, N. The Expression of Opsins in the Human Skin and Its Implications for Photobiomodulation: A Systematic Review. Photoderm. Photoimm. Photomed. 2020, 36, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Portillo, M.; Mataix, M.; Alonso-Juarranz, M.; Lorrio, S.; Villalba, M.; Rodríguez-Luna, A.; González, S. The Aqueous Extract of Polypodium Leucotomos (Fernblock®) Regulates Opsin 3 and Prevents Photooxidation of Melanin Precursors on Skin Cells Exposed to Blue Light Emitted from Digital Devices. Antioxidants 2021, 10, 400. [Google Scholar] [CrossRef] [PubMed]
- Ansary, T.M.; Hossain, M.R.; Kamiya, K.; Komine, M.; Ohtsuki, M. Inflammatory Molecules Associated with Ultraviolet Radiation-Mediated Skin Aging. Int. J. Mol. Sci. 2021, 22, 3974. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Duan, E. Fighting against Skin Aging: The Way from Bench to Bedside. Cell Transpl. 2018, 27, 729–738. [Google Scholar] [CrossRef]
- Farage, M.A.; Miller, K.W.; Elsner, P.; Maibach, H.I. Intrinsic and Extrinsic Factors in Skin Ageing: A Review. Int. J. Cosmet. Sci. 2008, 30, 87–95. [Google Scholar] [CrossRef]
- Tsatsou, F.; Trakatelli, M.; Patsatsi, A.; Kalokasidis, K.; Sotiriadis, D. Extrinsic Aging: UV-Mediated Skin Carcinogenesis. Derm. Endocrinol. 2012, 4, 285–297. [Google Scholar] [CrossRef]
- Rastogi, R.P.; Richa; Kumar, A.; Tyagi, M.B.; Sinha, R.P. Molecular Mechanisms of Ultraviolet Radiation-Induced DNA Damage and Repair. J. Nucleic Acids 2010, 2010, 592980. [Google Scholar] [CrossRef]
- Krutmann, J.; Morita, A.; Chung, J.H. Sun Exposure: What Molecular Photodermatology Tells Us About Its Good and Bad Sides. J. Investig. Dermatol. 2012, 132, 976–984. [Google Scholar] [CrossRef]
- Davinelli, S.; Bertoglio, J.C.; Polimeni, A.; Scapagnini, G. Cytoprotective Polyphenols Against Chronological Skin Aging and Cutaneous Photodamage. Curr. Pharm. Des. 2018, 24, 99–105. [Google Scholar] [CrossRef]
- Imokawa, G. Intracellular Signaling Mechanisms Involved in the Biological Effects of the Xanthophyll Carotenoid Astaxanthin to Prevent the Photo-aging of the Skin in a Reactive Oxygen Species Depletion-independent Manner: The Key Role of Mitogen and Stress-activated Protein Kinase 1. Photochem. Photobiol. 2019, 95, 480–489. [Google Scholar] [CrossRef]
- Manicone, A.; Mcguire, J. Matrix Metalloproteinases as Modulators of Inflammation. Semin. Cell Dev. Biol. 2008, 19, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Parks, W.C.; Wilson, C.L.; López-Boado, Y.S. Matrix Metalloproteinases as Modulators of Inflammation and Innate Immunity. Nat. Rev. Immunol. 2004, 4, 617–629. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.-W.; Kwon, S.-H.; Choi, J.-Y.; Na, J.-I.; Huh, C.-H.; Choi, H.-R.; Park, K.-C. Molecular Mechanisms of Dermal Aging and Antiaging Approaches. Int. J. Mol. Sci. 2019, 20, 2126. [Google Scholar] [CrossRef] [PubMed]
- Quan, T.; Little, E.; Quan, H.; Qin, Z.; Voorhees, J.J.; Fisher, G.J. Elevated Matrix Metalloproteinases and Collagen Fragmentation in Photodamaged Human Skin: Impact of Altered Extracellular Matrix Microenvironment on Dermal Fibroblast Function. J. Investig. Dermatol. 2013, 133, 1362–1366. [Google Scholar] [CrossRef]
- Kruger, T.E.; Miller, A.H.; Wang, J. Collagen Scaffolds in Bone Sialoprotein-Mediated Bone Regeneration. Sci. World J. 2013, 2013, 812718. [Google Scholar] [CrossRef]
- Ansel, J.; Perry, P.; Brown, J.; Damm, D.; Phan, T.; Hart, C.; Luger, T.; Hefeneider, S. Cytokine Modulation of Keratinocyte Cytokines. J. Investig. Dermatol. 1990, 94, s101–s107. [Google Scholar] [CrossRef]
- Ortonne, J.-P. Pigmentary Changes of the Ageing Skin. Br. J. Dermatol. 1990, 122, 21–28. [Google Scholar] [CrossRef]
- Skoczyńska, A.; Budzisz, E.; Trznadel-Grodzka, E.; Rotsztejn, H. Melanin and Lipofuscin as Hallmarks of Skin Aging. Adv. Dermatol. Allergol. 2017, 2, 97–103. [Google Scholar] [CrossRef]
- Murase, D.; Hachiya, A.; Takano, K.; Hicks, R.; Visscher, M.O.; Kitahara, T.; Hase, T.; Takema, Y.; Yoshimori, T. Autophagy Has a Significant Role in Determining Skin Color by Regulating Melanosome Degradation in Keratinocytes. J. Investig. Dermatol. 2013, 133, 2416–2424. [Google Scholar] [CrossRef]
- Duval, C.; Cohen, C.; Chagnoleau, C.; Flouret, V.; Bourreau, E.; Bernerd, F. Key Regulatory Role of Dermal Fibroblasts in Pigmentation as Demonstrated Using a Reconstructed Skin Model: Impact of Photo-Aging. PLoS ONE 2014, 9, e114182. [Google Scholar] [CrossRef]
- Murase, D.; Hachiya, A.; Amano, Y.; Ohuchi, A.; Kitahara, T.; Takema, Y. The Essential Role of P53 in Hyperpigmentation of the Skin via Regulation of Paracrine Melanogenic Cytokine Receptor Signaling. J. Biol. Chem. 2009, 284, 4343–4353. [Google Scholar] [CrossRef] [PubMed]
- Cui, R.; Widlund, H.R.; Feige, E.; Lin, J.Y.; Wilensky, D.L.; Igras, V.E.; D’Orazio, J.; Fung, C.Y.; Schanbacher, C.F.; Granter, S.R.; et al. Central Role of P53 in the Suntan Response and Pathologic Hyperpigmentation. Cell 2007, 128, 853–864. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.E.; Kim, Y.; Kwon, S.; Kim, M.; Kim, Y.H.; Kim, J.-H.; Park, T.J.; Kang, H.Y. Senescent Fibroblasts Drive Ageing Pigmentation: A Potential Therapeutic Target for Senile Lentigo. Theranostics 2018, 8, 4620–4632. [Google Scholar] [CrossRef] [PubMed]
- Saarialho-Kere, U.; Kerkelä, E.; Jeskanen, L.; Ranki, A.; Vaalamo, M.; Hasan, T.; Pierce, R.; Starcher, B.; Raudasoja, R.; Oikarinen, A. Accumulation of Matrilysin (MMP-7) and Macrophage Metalloelastase (MMP-12) in Actinic Damage. J. Investig. Dermatol. 1999, 113, 664–672. [Google Scholar] [CrossRef]
- Poulopoulos, A.K. Expression of Matrix Metalloproteinases 9 and 12 in Actinic Cheilitis. World J. Exp. Med. 2013, 3, 43. [Google Scholar] [CrossRef]
- Schroeder, P.; Calles, C.; Benesova, T.; Macaluso, F.; Krutmann, J. Photoprotection beyond Ultraviolet Radiation—Effective Sun Protection Has to Include Protection against Infrared A Radiation-Induced Skin Damage. Ski. Pharmacol. Physiol. 2010, 23, 15–17. [Google Scholar] [CrossRef]
- Yano, K.; Kadoya, K.; Kajiya, K.; Hong, Y.-K.; Detmar, M. Ultraviolet B Irradiation of Human Skin Induces an Angiogenic Switch That Is Mediated by Upregulation of Vascular Endothelial Growth Factor and by Downregulation of Thrombospondin-1. Br. J. Dermatol. 2005, 152, 115–121. [Google Scholar] [CrossRef]
- Kim, M.-S.; Kim, Y.K.; Cho, K.H.; Chung, J.H. Infrared Exposure Induces an Angiogenic Switch in Human Skin That Is Partially Mediated by Heat: IR Induces Angiogenesis in Human Skin in Vivo. Br. J. Dermatol. 2006, 155, 1131–1138. [Google Scholar] [CrossRef]
- Kim, M.; Oh, Y.J.; Lee, S.; Kim, J.E.; Kim, K.H.; Chung, J.H. Ultraviolet Radiation Attenuates Thrombospondin 1 Expression via PI3K-Akt Activation in Human Keratinocytes. Photochem. Photobiol. 2006, 82, 645–650. [Google Scholar] [CrossRef]
- Yang, Y.-M.; Huang, A.; Kaley, G.; Sun, D. eNOS Uncoupling and Endothelial Dysfunction in Aged Vessels. Am. J. Physiol.-Heart Circ. Physiol. 2009, 297, H1829–H1836. [Google Scholar] [CrossRef]
- Barolet, A.C.; Litvinov, I.V.; Barolet, D. Light-Induced Nitric Oxide Release in the Skin beyond UVA and Blue Light: Red & near-Infrared Wavelengths. Nitric Oxide 2021, 117, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Holliman, G.; Lowe, D.; Cohen, H.; Felton, S.; Raj, K. Ultraviolet Radiation-Induced Production of Nitric Oxide:A Multi-Cell and Multi-Donor Analysis. Sci. Rep. 2017, 7, 11105. [Google Scholar] [CrossRef] [PubMed]
- Opländer, C.; Volkmar, C.M.; Paunel-Görgülü, A.; Van Faassen, E.E.; Heiss, C.; Kelm, M.; Halmer, D.; Mürtz, M.; Pallua, N.; Suschek, C.V. Whole Body UVA Irradiation Lowers Systemic Blood Pressure by Release of Nitric Oxide From Intracutaneous Photolabile Nitric Oxide Derivates. Circ. Res. 2009, 105, 1031–1040. [Google Scholar] [CrossRef] [PubMed]
- Fuks, K.B.; Hüls, A.; Sugiri, D.; Altug, H.; Vierkötter, A.; Abramson, M.J.; Goebel, J.; Wagner, G.G.; Demuth, I.; Krutmann, J.; et al. Tropospheric Ozone and Skin Aging: Results from Two German Cohort Studies. Environ. Int. 2019, 124, 139–144. [Google Scholar] [CrossRef]
- Flament, F.; Bourokba, N.; Nouveau, S.; Li, J.; Charbonneau, A. A Severe Chronic Outdoor Urban Pollution Alters Some Facial Aging Signs in Chinese Women. A Tale of Two Cities. Int. J. Cosmet. Sci. 2018, 40, 467–481. [Google Scholar] [CrossRef]
- Flament, F.; Ye, C.; Amar, D. Assessing the Impact of an Aerial Chronic Urban Pollution (UP) on Some Facial Signs of Differently-aged Chinese Men. Int. J. Cosmet. Sci. 2019, 41, 450–461. [Google Scholar] [CrossRef]
- Peng, F.; Xue, C.-H.; Hwang, S.K.; Li, W.-H.; Chen, Z.; Zhang, J.-Z. Exposure to Fine Particulate Matter Associated with Senile Lentigo in Chinese Women: A Cross-sectional Study. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 355–360. [Google Scholar] [CrossRef]
- Hüls, A.; Vierkötter, A.; Gao, W.; Krämer, U.; Yang, Y.; Ding, A.; Stolz, S.; Matsui, M.; Kan, H.; Wang, S.; et al. Traffic-Related Air Pollution Contributes to Development of Facial Lentigines: Further Epidemiological Evidence from Caucasians and Asians. J. Investig. Dermatol. 2016, 136, 1053–1056. [Google Scholar] [CrossRef]
- Ding, A.; Yang, Y.; Zhao, Z.; Hüls, A.; Vierkötter, A.; Yuan, Z.; Cai, J.; Zhang, J.; Gao, W.; Li, J.; et al. Indoor PM2.5 Exposure Affects Skin Aging Manifestation in a Chinese Population. Sci. Rep. 2017, 7, 15329. [Google Scholar] [CrossRef]
- Vierkötter, A.; Schikowski, T.; Ranft, U.; Sugiri, D.; Matsui, M.; Krämer, U.; Krutmann, J. Airborne Particle Exposure and Extrinsic Skin Aging. J. Investig. Dermatol. 2010, 130, 2719–2726. [Google Scholar] [CrossRef]
- Packer, L.; Valacchi, G. Antioxidants and the Response of Skin to Oxidative Stress: Vitamin E as a Key Indicator. Ski. Pharmacol. Physiol. 2002, 15, 282–290. [Google Scholar] [CrossRef] [PubMed]
- Valacchi, G.; Pagnin, E.; Corbacho, A.M.; Olano, E.; Davis, P.A.; Packer, L.; Cross, C.E. In Vivo Ozone Exposure Induces Antioxidant/Stress-Related Responses in Murine Lung and Skin. Free. Radic. Biol. Med. 2004, 36, 673–681. [Google Scholar] [CrossRef] [PubMed]
- Valacchi, G.; Van Der Vliet, A.; Schock, B.C.; Okamoto, T.; Obermuller-Jevic, U.; Cross, C.E.; Packer, L. Ozone Exposure Activates Oxidative Stress Responses in Murine Skin. Toxicology 2002, 179, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Valacchi, G.; Sticozzi, C.; Belmonte, G.; Cervellati, F.; Demaude, J.; Chen, N.; Krol, Y.; Oresajo, C. Vitamin C Compound Mixtures Prevent Ozone-Induced Oxidative Damage in Human Keratinocytes as Initial Assessment of Pollution Protection. PLoS ONE 2015, 10, e0131097. [Google Scholar] [CrossRef]
- Valacchi, G.; Pecorelli, A.; Belmonte, G.; Pambianchi, E.; Cervellati, F.; Lynch, S.; Krol, Y.; Oresajo, C. Protective Effects of Topical Vitamin C Compound Mixtures against Ozone-Induced Damage in Human Skin. J. Investig. Dermatol. 2017, 137, 1373–1375. [Google Scholar] [CrossRef]
- Krutmann, J.; Liu, W.; Li, L.; Pan, X.; Crawford, M.; Sore, G.; Seite, S. Pollution and Skin: From Epidemiological and Mechanistic Studies to Clinical Implications. J. Dermatol. Sci. 2014, 76, 163–168. [Google Scholar] [CrossRef]
- Malvy, J.-M.D.; Guinot, C.; Preziosi, P.; Vaillant, L.; Tenenhaus, M.; Galan, P.; Hercberg, S.; Tschachler, E. Epidemiologic Determinants of Skin Photoaging: Baseline Data of the SU.VI.MAX. Cohort. J. Am. Acad. Dermatol. 2000, 42, 47–55. [Google Scholar] [CrossRef]
- Chung, J.H.; Lee, S.H.; Youn, C.S.; Park, B.J.; Kim, K.H.; Park, K.C.; Cho, K.H.; Eun, H.C. Cutaneous Photodamage in Koreans: Influence of Sex, Sun Exposure, Smoking, and Skin Color. Arch. Dermatol. 2001, 137, 1043–1051. [Google Scholar]
- Ernster, V.L.; Grady, D.; Miike, R.; Black, D.; Selby, J.; Kerlikowske, K. Facial Wrinkling in Men and Women, by Smoking Status. Am. J. Public Health 1995, 85, 78–82. [Google Scholar] [CrossRef]
- Kadunce, D.P.; Burr, R.; Gress, R.; Kanner, R.; Lyon, J.L.; Zone, J.J. Cigarette Smoking: Risk Factor for Premature Facial Wrinkling. Ann. Int. Med. 1991, 114, 840–844. [Google Scholar] [CrossRef]
- Raduan, A.; Luiz, R.; Manela-Azulay, M. Association between Smoking and Cutaneous Ageing in a Brazilian Population. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 1312–1318. [Google Scholar] [CrossRef] [PubMed]
- Morita, A. Tobacco Smoke Causes Premature Skin Aging. J. Dermatol. Sci. 2007, 48, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Just, M.; Ribera, M.; Monsó, E.; Lorenzo, J.C.; Ferrándiz, C. Effect of Smoking on Skin Elastic Fibres: Morphometric and Immunohistochemical Analysis. Br. J. Dermatol. 2007, 156, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.; Morita, A.; Tsuji, T. Alterations of Extracellular Matrix Induced by Tobacco Smoke Extract. Arch. Dermatol. Res. 2000, 292, 188–194. [Google Scholar] [CrossRef]
- Tanaka, H.; Ono, Y.; Nakata, S.; Shintani, Y.; Sakakibara, N.; Morita, A. Tobacco Smoke Extract Induces Premature Skin Aging in Mouse. J. Dermatol. Sci. 2007, 46, 69–71. [Google Scholar] [CrossRef]
- Rodrigues, L.; Palma, L.; Tavares Marques, L.; Bujan Varela, J. Dietary Water Affects Human Skin Hydration and Biomechanics. Clin. Cosmet. Investig. Dermatol. 2015, 8, 413. [Google Scholar] [CrossRef]
- Strasser, B.; Volaklis, K.; Fuchs, D.; Burtscher, M. Role of Dietary Protein and Muscular Fitness on Longevity and Aging. Aging Dis. 2018, 9, 119. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, Q.; Rao, E.; Sun, Y.; Grossmann, M.E.; Morris, R.J.; Cleary, M.P.; Li, B. Epidermal Fatty Acid Binding Protein Promotes Skin Inflammation Induced by High-Fat Diet. Immunity 2015, 42, 953–964. [Google Scholar] [CrossRef]
- Balić, A.; Vlašić, D.; Žužul, K.; Marinović, B.; Bukvić Mokos, Z. Omega-3 Versus Omega-6 Polyunsaturated Fatty Acids in the Prevention and Treatment of Inflammatory Skin Diseases. Int. J. Mol. Sci. 2020, 21, 741. [Google Scholar] [CrossRef]
- Meksiarun, P.; Maeda, Y.; Hiroi, T.; Andriana, B.B.; Sato, H. Analysis of the Effects of Dietary Fat on Body and Skin Lipids of Hamsters by Raman Spectroscopy. Analyst 2015, 140, 4238–4244. [Google Scholar] [CrossRef]
- Rosa, D.F.; Sarandy, M.M.; Novaes, R.D.; Freitas, M.B.; Do Carmo Gouveia Pelúzio, M.; Gonçalves, R.V. High-Fat Diet and Alcohol Intake Promotes Inflammation and Impairs Skin Wound Healing in Wistar Rats. Mediat. Inflamm. 2018, 2018, 4658583. [Google Scholar] [CrossRef] [PubMed]
- Rosa, D.F.; Sarandy, M.M.; Novaes, R.D.; Da Matta, S.L.P.; Gonçalves, R.V. Effect of a High-Fat Diet and Alcohol on Cutaneous Repair: A Systematic Review of Murine Experimental Models. PLoS ONE 2017, 12, e0176240. [Google Scholar] [CrossRef] [PubMed]
- Vaid, M.; Singh, T.; Prasad, R.; Katiyar, S.K. Intake of High-Fat Diet Stimulates the Risk of Ultraviolet Radiation-Induced Skin Tumors and Malignant Progression of Papillomas to Carcinoma in SKH-1 Hairless Mice. Toxicol. Appl. Pharmacol. 2014, 274, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Herbert, D.; Franz, S.; Popkova, Y.; Anderegg, U.; Schiller, J.; Schwede, K.; Lorz, A.; Simon, J.C.; Saalbach, A. High-Fat Diet Exacerbates Early Psoriatic Skin Inflammation Independent of Obesity: Saturated Fatty Acids as Key Players. J. Investig. Dermatol. 2018, 138, 1999–2009. [Google Scholar] [CrossRef]
- Higashi, Y.; Yamakuchi, M.; Fukushige, T.; Ibusuki, A.; Hashiguchi, T.; Kanekura, T. High-fat Diet Exacerbates Imiquimod-induced Psoriasis-like Dermatitis in Mice. Exp. Dermatol. 2018, 27, 178–184. [Google Scholar] [CrossRef]
- Park, K.-H.; Kim, J.; Jung, S.; Sung, K.; Son, Y.-K.; Bae, J.M.; Kim, B.-H. Alleviation of Ultraviolet B-Induced Photoaging by 7-MEGATM 500 in Hairless Mouse Skin. Toxicol. Res. 2019, 35, 353–359. [Google Scholar] [CrossRef]
- Balkrishna, A.; Nain, P.; Chauhan, A.; Sharma, N.; Gupta, A.; Ranjan, R.; Varshney, A. Super Critical Fluid Extracted Fatty Acids from Withania Somnifera Seeds Repair Psoriasis-Like Skin Lesions and Attenuate Pro-Inflammatory Cytokines (TNF-α and IL-6) Release. Biomolecules 2020, 10, 185. [Google Scholar] [CrossRef]
- Hyun, Y.J.; Piao, M.J.; Kang, K.A.; Zhen, A.X.; Madushan Fernando, P.D.S.; Kang, H.K.; Ahn, Y.S.; Hyun, J.W. Effect of Fermented Fish Oil on Fine Particulate Matter-Induced Skin Aging. Mar. Drugs 2019, 17, 61. [Google Scholar] [CrossRef]
- Wang, X.; Wu, J. Modulating Effect of Fatty Acids and Sterols on Skin Aging. J. Funct. Foods 2019, 57, 135–140. [Google Scholar] [CrossRef]
- Draelos, Z.D. Aging Skin: The Role of Diet: Facts and Controversies. Clin. Dermatol. 2013, 31, 701–706. [Google Scholar] [CrossRef]
- Nguyen, H.P.; Katta, R. Sugar Sag: Glycation and the Role of Diet in Aging Skin. Ski. Ther. Lett. 2015, 20, 1–5. [Google Scholar]
- Brescoll, J.; Daveluy, S. A Review of Vitamin B12 in Dermatology. Am. J. Clin. Dermatol. 2015, 16, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Pullar, J.; Carr, A.; Vissers, M. The Roles of Vitamin C in Skin Health. Nutrients 2017, 9, 866. [Google Scholar] [CrossRef] [PubMed]
- Schempp, C.M.; Meinke, M.C.; Lademann, J.; Ferrari, Y.; Brecht, T.; Gehring, W. Topical Antioxidants Protect the Skin from Chemical-induced Irritation in the Repetitive Washing Test: A Placebo-controlled, Double-blind Study. Contact Dermat. 2012, 67, 234–237. [Google Scholar] [CrossRef]
- Wu, Y.; Zheng, X.; Xu, X.-G.; Li, Y.-H.; Wang, B.; Gao, X.-H.; Chen, H.-D.; Yatskayer, M.; Oresajo, C. Protective Effects of a Topical Antioxidant Complex Containing Vitamins C and E and Ferulic Acid against Ultraviolet Irradiation-Induced Photodamage in Chinese Women. J. Drugs Dermatol. 2013, 12, 464–468. [Google Scholar]
- Skrobot, A.; Demkow, U.; Wachowska, M. Immunomodulatory Role of Vitamin D: A Review. In Current Trends in Immunity and Respiratory Infections; Pokorski, M., Ed.; Advances in Experimental Medicine and Biology; Springer International Publishing: Cham, Switzerland, 2018; Volume 1108, pp. 13–23. ISBN 978-3-030-01634-0. [Google Scholar]
- Scott, J.F.; Das, L.M.; Ahsanuddin, S.; Qiu, Y.; Binko, A.M.; Traylor, Z.P.; Debanne, S.M.; Cooper, K.D.; Boxer, R.; Lu, K.Q. Oral Vitamin D Rapidly Attenuates Inflammation from Sunburn: An Interventional Study. J. Investig. Dermatol. 2017, 137, 2078–2086. [Google Scholar] [CrossRef]
- Lin, Z.; Marepally, S.R.; Goh, E.S.Y.; Cheng, C.Y.S.; Janjetovic, Z.; Kim, T.-K.; Miller, D.D.; Postlethwaite, A.E.; Slominski, A.T.; Tuckey, R.C.; et al. Investigation of 20S-Hydroxyvitamin D3 Analogs and Their 1α-OH Derivatives as Potent Vitamin D Receptor Agonists with Anti-Inflammatory Activities. Sci. Rep. 2018, 8, 1478. [Google Scholar] [CrossRef]
- Postlethwaite, A.E.; Tuckey, R.C.; Kim, T.-K.; Li, W.; Bhattacharya, S.K.; Myers, L.K.; Brand, D.D.; Slominski, A.T. 20S-Hydroxyvitamin D3, a Secosteroid Produced in Humans, Is Anti-Inflammatory and Inhibits Murine Autoimmune Arthritis. Front. Immunol. 2021, 12, 678487. [Google Scholar] [CrossRef]
- Wöbke, T.K.; Sorg, B.L.; Steinhilber, D. Vitamin D in Inflammatory Diseases. Front. Physiol. 2014, 5, 244. [Google Scholar] [CrossRef]
- Janjetovic, Z.; Tuckey, R.C.; Nguyen, M.N.; Thorpe, E.M.; Slominski, A.T. 20,23-dihydroxyvitamin D3, Novel P450scc Product, Stimulates Differentiation and Inhibits Proliferation and NF-κB Activity in Human Keratinocytes. J. Cell. Physiol. 2010, 223, 36–48. [Google Scholar] [CrossRef]
- Janjetovic, Z.; Zmijewski, M.A.; Tuckey, R.C.; DeLeon, D.A.; Nguyen, M.N.; Pfeffer, L.M.; Slominski, A.T. 20-Hydroxycholecalciferol, Product of Vitamin D3 Hydroxylation by P450scc, Decreases NF-κB Activity by Increasing IκBα Levels in Human Keratinocytes. PLoS ONE 2009, 4, e5988. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, M.; Werner, S. Nrf2—A Regulator of Keratinocyte Redox Signaling. Free. Radic. Biol. Med. 2015, 88, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Chaiprasongsuk, A.; Janjetovic, Z.; Kim, T.-K.; Jarrett, S.G.; D’Orazio, J.A.; Holick, M.F.; Tang, E.K.Y.; Tuckey, R.C.; Panich, U.; Li, W.; et al. Protective Effects of Novel Derivatives of Vitamin D3 and Lumisterol against UVB-Induced Damage in Human Keratinocytes Involve Activation of Nrf2 and P53 Defense Mechanisms. Redox Biol. 2019, 24, 101206. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Dixon, K.M.; Deo, S.S.; Holliday, C.J.; Slater, M.; Halliday, G.M.; Reeve, V.E.; Mason, R.S. Photoprotection by 1,25 Dihydroxyvitamin D3 Is Associated with an Increase in P53 and a Decrease in Nitric Oxide Products. J. Investig. Dermatol. 2007, 127, 707–715. [Google Scholar] [CrossRef]
- Dixon, K.M.; Sequeira, V.B.; Deo, S.S.; Mohan, R.; Posner, G.H.; Mason, R.S. Differential Photoprotective Effects of 1,25-Dihydroxyvitamin D3 and a Low Calcaemic Deltanoid. Photochem. Photobiol. Sci. 2012, 11, 1825–1830. [Google Scholar] [CrossRef]
- Sequeira, V.B.; Rybchyn, M.S.; Gordon-Thomson, C.; Tongkao-On, W.; Mizwicki, M.T.; Norman, A.W.; Reeve, V.E.; Halliday, G.M.; Mason, R.S. Opening of Chloride Channels by 1α,25-Dihydroxyvitamin D3 Contributes to Photoprotection against UVR-Induced Thymine Dimers in Keratinocytes. J. Investig. Dermatol. 2013, 133, 776–782. [Google Scholar] [CrossRef]
- Wong, G.; Gupta, R.; Dixon, K.M.; Deo, S.S.; Choong, S.M.; Halliday, G.M.; Bishop, J.E.; Ishizuka, S.; Norman, A.W.; Posner, G.H.; et al. 1,25-Dihydroxyvitamin D and Three Low-Calcemic Analogs Decrease UV-Induced DNA Damage via the Rapid Response Pathway. J. Steroid Biochem. Mol. Biol. 2004, 89–90, 567–570. [Google Scholar] [CrossRef]
- Cao, C.; Xiao, Z.; Wu, Y.; Ge, C. Diet and Skin Aging—From the Perspective of Food Nutrition. Nutrients 2020, 12, 870. [Google Scholar] [CrossRef]
- Wang, L.; Wang, Q.; Qian, J.; Liang, Q.; Wang, Z.; Xu, J.; He, S.; Ma, H. Bioavailability and Bioavailable Forms of Collagen after Oral Administration to Rats. J. Agric. Food Chem. 2015, 63, 3752–3756. [Google Scholar] [CrossRef]
- Farré, X.; Blay, N.; Cortés, B.; Carreras, A.; Iraola-Guzmán, S.; De Cid, R. Skin Phototype and Disease: A Comprehensive Genetic Approach to Pigmentary Traits Pleiotropy Using PRS in the GCAT Cohort. Genes 2023, 14, 149. [Google Scholar] [CrossRef]
- Palmer, D.; Fabris, F.; Doherty, A.; Freitas, A.A.; De Magalhães, J.P. Ageing Transcriptome Meta-Analysis Reveals Similarities and Differences between Key Mammalian Tissues. Aging 2021, 13, 3313–3341. [Google Scholar] [CrossRef] [PubMed]
- Roy, T.; Boateng, S.T.; Uddin, M.B.; Banang-Mbeumi, S.; Yadav, R.K.; Bock, C.R.; Folahan, J.T.; Siwe-Noundou, X.; Walker, A.L.; King, J.A.; et al. The PI3K-Akt-mTOR and Associated Signaling Pathways as Molecular Drivers of Immune-Mediated Inflammatory Skin Diseases: Update on Therapeutic Strategy Using Natural and Synthetic Compounds. Cells 2023, 12, 1671. [Google Scholar] [CrossRef] [PubMed]
- Hussein, R.S.; Bin Dayel, S.; Abahussein, O.; El-Sherbiny, A.A. Influences on Skin and Intrinsic Aging: Biological, Environmental, and Therapeutic Insights. J. Cosmet. Dermatol. 2025, 24, e16688. [Google Scholar] [CrossRef] [PubMed]
- Wollina, U.; Abdel-Naser, M.B.; Ganceviciene, R.; Zouboulis, C.C. Receptors of Eccrine, Apocrine, and Holocrine Skin Glands. Dermatol. Clin. 2007, 25, 577–588, ix. [Google Scholar] [CrossRef]
- Lephart, E.D.; Naftolin, F. Factors Influencing Skin Aging and the Important Role of Estrogens and Selective Estrogen Receptor Modulators (SERMs). Clin. Cosmet. Investig. Dermatol. 2022, 15, 1695–1709. [Google Scholar] [CrossRef]
- Lephart, E.D.; Naftolin, F. Menopause and the Skin: Old Favorites and New Innovations in Cosmeceuticals for Estrogen-Deficient Skin. Dermatol. Ther. 2021, 11, 53–69. [Google Scholar] [CrossRef]
- Woodby, B.; Penta, K.; Pecorelli, A.; Lila, M.A.; Valacchi, G. Skin Health from the Inside Out. Annu. Rev. Food Sci. Technol. 2020, 11, 235–254. [Google Scholar] [CrossRef]
- Bartke, A.; Hascup, E.; Hascup, K.; Masternak, M.M. Growth Hormone and Aging: New Findings. World J. Mens Health 2021, 39, 454. [Google Scholar] [CrossRef]
- Zomer, H.D.; Cooke, P.S. Targeting Estrogen Signaling and Biosynthesis for Aged Skin Repair. Front. Physiol. 2023, 14, 1281071. [Google Scholar] [CrossRef]
- Taghizadeh, B.; Moradi, R.; Mirzavi, F.; Barati, M.; Soleimani, A.; Jaafari, M.-R.; Zarghami, N. The Protection Role of Human Growth Hormone on Skin Cells Following Ultraviolet B Exposure. J. Photochem. Photobiol. B Biol. 2024, 257, 112961. [Google Scholar] [CrossRef]
- Laron, Z. Insulin-like Growth Factor 1 (IGF-1): A Growth Hormone. Mol. Pathol. 2001, 54, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Maity, P.; Singh, K.; Krug, L.; Koroma, A.; Hainzl, A.; Bloch, W.; Kochanek, S.; Wlaschek, M.; Schorpp-Kistner, M.; Angel, P.; et al. Persistent JunB Activation in Fibroblasts Disrupts Stem Cell Niche Interactions Enforcing Skin Aging. Cell Rep. 2021, 36, 109634. [Google Scholar] [CrossRef] [PubMed]
- Edmondson, S.R.; Thumiger, S.P.; Werther, G.A.; Wraight, C.J. Epidermal Homeostasis: The Role of the Growth Hormone and Insulin-like Growth Factor Systems. Endocr. Rev. 2003, 24, 737–764. [Google Scholar] [CrossRef]
- Böhm, M.; Stegemann, A.; Paus, R.; Kleszczyński, K.; Maity, P.; Wlaschek, M.; Scharffetter-Kochanek, K. Endocrine Controls of Skin Aging. Endocr. Rev. 2025, 46, 349–375. [Google Scholar] [CrossRef] [PubMed]
- Bocheva, G.; Slominski, R.M.; Janjetovic, Z.; Kim, T.-K.; Böhm, M.; Steinbrink, K.; Reiter, R.J.; Kleszczyński, K.; Slominski, A.T. Protective Role of Melatonin and Its Metabolites in Skin Aging. Int. J. Mol. Sci. 2022, 23, 1238. [Google Scholar] [CrossRef]
- Su, Z.; Hu, Q.; Li, X.; Wang, Z.; Xie, Y. The Influence of Circadian Rhythms on DNA Damage Repair in Skin Photoaging. Int. J. Mol. Sci. 2024, 25, 10926. [Google Scholar] [CrossRef]
- Gendimenico, G.J.; Mezick, J.A. Pharmacological Effects of Retinoids on Skin Cells. Ski. Pharmacol. 1993, 6 (Suppl. 1), 24–34. [Google Scholar] [CrossRef]
- Morinobu, T.; Tamai, H.; Tanabe, T.; Murata, T.; Manago, M.; Mino, M.; Hirahara, F. Plasma Alpha-Tocopherol, Beta-Carotene, and Retinol Levels in the Institutionalized Elderly Individuals and in Young Adults. Int. J. Vitam. Nutr. Res. 1994, 64, 104–108. [Google Scholar]
- Budzianowska, A.; Banaś, K.; Budzianowski, J.; Kikowska, M. Antioxidants to Defend Healthy and Youthful Skin—Current Trends and Future Directions in Cosmetology. Appl. Sci. 2025, 15, 2571. [Google Scholar] [CrossRef]
- Papaccio, F.; D′Arino, A.; Caputo, S.; Bellei, B. Focus on the Contribution of Oxidative Stress in Skin Aging. Antioxidants 2022, 11, 1121. [Google Scholar] [CrossRef]
- Zgutka, K.; Tkacz, M.; Tomasiak, P.; Tarnowski, M. A Role for Advanced Glycation End Products in Molecular Ageing. Int. J. Mol. Sci. 2023, 24, 9881. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Yu, Y.; Sun, S.; Lu, C.; Zhai, J.; Lei, Y.; Bai, F.; Wang, R.; Chen, J. Immune Alterations with Aging: Mechanisms and Intervention Strategies. Nutrients 2024, 16, 3830. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, R.; Hu, A.; Bollag, W.B. The Skin and Inflamm-Aging. Biology 2023, 12, 1396. [Google Scholar] [CrossRef] [PubMed]
- Levine, J.M. Clinical Aspects of Aging Skin: Considerations for the Wound Care Practitioner. Adv. Ski. Wound Care 2020, 33, 12–19. [Google Scholar] [CrossRef]
- Venkatesh, S.; Maymone, M.B.C.; Vashi, N.A. Aging in Skin of Color. Clin. Dermatol. 2019, 37, 351–357. [Google Scholar] [CrossRef]
- Levine, J.M. Skin Failure: An Emerging Concept. J. Am. Med. Dir. Assoc. 2016, 17, 666–669. [Google Scholar] [CrossRef]
- Gould, L.; Abadir, P.; Brem, H.; Carter, M.; Conner-Kerr, T.; Davidson, J.; DiPietro, L.; Falanga, V.; Fife, C.; Gardner, S.; et al. Chronic Wound Repair and Healing in Older Adults: Current Status and Future Research. J. Am. Geriatr. Soc. 2015, 63, 427–438. [Google Scholar] [CrossRef]
- Langemo, D.K.; Brown, G. Skin Fails Too: Acute, Chronic, and End-Stage Skin Failure. Adv. Ski. Wound Care 2006, 19, 206–212. [Google Scholar] [CrossRef]
- Shaw, T.J.; Martin, P. Wound Repair at a Glance. J. Cell Sci. 2009, 122, 3209–3213. [Google Scholar] [CrossRef]
- Fenske, N.A.; Lober, C.W. Structural and Functional Changes of Normal Aging Skin. J. Am. Acad. Dermatol. 1986, 15, 571–585. [Google Scholar] [CrossRef]
- Levine, J.M. Unavoidable Pressure Injuries, Terminal Ulceration, and Skin Failure: In Search of a Unifying Classification System. Adv. Ski. Wound Care 2017, 30, 200–202. [Google Scholar] [CrossRef] [PubMed]
- Dyer, J.M.; Miller, R.A. Chronic Skin Fragility of Aging: Current Concepts in the Pathogenesis, Recognition, and Management of Dermatoporosis. J. Clin. Aesthet. Dermatol. 2018, 11, 13–18. [Google Scholar] [PubMed]
- McKnight, A.; Momoh, A.; Bullocks, J. Variations of Structural Components: Specific Intercultural Differences in Facial Morphology, Skin Type, and Structures. Semin. Plast. Surg. 2009, 23, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Brissett, A.; Naylor, M. The Aging African-American Face. Facial Plast. Surg. 2010, 26, 154–163. [Google Scholar] [CrossRef]
- Taylor, S.C. Skin of Color: Biology, Structure, Function, and Implications for Dermatologic Disease. J. Am. Acad. Dermatol. 2002, 46, S41–S62. [Google Scholar] [CrossRef]
- Montagna, W.; Carlisle, K. The Architecture of Black and White Facial Skin. J. Am. Acad. Dermatol. 1991, 24, 929–937. [Google Scholar] [CrossRef]
- Alexis, A.F.; Obioha, J.O. Ethnicity and Aging Skin. J. Drugs Dermatol. 2017, 16, s77–s80. [Google Scholar]
- Vashi, N.A.; de Castro Maymone, M.B.; Kundu, R.V. Aging Differences in Ethnic Skin. J. Clin. Aesthet. Dermatol. 2016, 9, 31–38. [Google Scholar]
- Liew, S. Ethnic and Gender Considerations in the Use of Facial Injectables: Asian Patients. Plast. Reconstr. Surg. 2015, 136, 22S–27S. [Google Scholar] [CrossRef]
- Porter, J.P.; Olson, K.L. Anthropometric Facial Analysis of the African American Woman. Arch. Facial Plast. Surg. 2001, 3, 191–197. [Google Scholar] [CrossRef]
- Talakoub, L.; Wesley, N.O. Differences in Perceptions of Beauty and Cosmetic Procedures Performed in Ethnic Patients. Semin. Cutan. Med. Surg. 2009, 28, 115–129. [Google Scholar] [CrossRef] [PubMed]
- Férnandez-Guarino, M.; Naharro-Rodriguez, J.; Bacci, S. Disturbances in the Skin Homeostasis: Wound Healing, an Undefined Process. Cosmetics 2024, 11, 90. [Google Scholar] [CrossRef]
- Arnal-Forné, M.; Molina-García, T.; Ortega, M.; Marcos-Garcés, V.; Molina, P.; Ferrández-Izquierdo, A.; Sepulveda, P.; Bodí, V.; Ríos-Navarro, C.; Ruiz-Saurí, A. Changes in Human Skin Composition Due to Intrinsic Aging: A Histologic and Morphometric Study. Histochem. Cell Biol. 2024, 162, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Bonta, M.; Daina, L.; Muţiu, G. The Process of Ageing Reflected by Histological Changes in the Skin. Rom. J. Morphol. Embryol. 2013, 54, 797–804. [Google Scholar]
- Harris, J.R.; Korolchuk, V.I. Biochemistry and Cell Biology of Ageing: Part II Clinical Science; Subcellular Biochemistry; Springer Nature: Singapore, 2019; Volume 91, ISBN 9789811336805. [Google Scholar]
- Lee, H.; Hong, Y.; Kim, M. Structural and Functional Changes and Possible Molecular Mechanisms in Aged Skin. Int. J. Mol. Sci. 2021, 22, 12489. [Google Scholar] [CrossRef]
- Berry, K.; Hallock, K.; Lam, C. Photoaging and Topical Rejuvenation. Clin. Plast. Surg. 2023, 50, 381–390. [Google Scholar] [CrossRef]
- Draelos, Z.; Bogdanowicz, P.; Saurat, J.-H. Top Weapons in Skin Aging and Actives to Target the Consequences of Skin Cell Senescence. J. Eur. Acad. Dermatol. Venereol. 2024, 38, 15–22. [Google Scholar] [CrossRef]
- DiNatale, L.; Idkowiak-Baldys, J.; Zhuang, Y.; Gonzalez, A.; Stephens, T.J.; Jiang, L.I.; Li, W.; Basson, R.; Bayat, A. Novel Rotational Combination Regimen of Skin Topicals Improves Facial Photoaging: Efficacy Demonstrated in Double-Blinded Clinical Trials and Laboratory Validation. Front. Med. 2021, 8, 724344. [Google Scholar] [CrossRef]
- Tang, S.-C.; Yang, J.-H. Dual Effects of Alpha-Hydroxy Acids on the Skin. Molecules 2018, 23, 863. [Google Scholar] [CrossRef]
- Schulte, B.C.; Wu, W.; Rosen, T. Azelaic Acid: Evidence-Based Update on Mechanism of Action and Clinical Application. J. Drugs Dermatol. 2015, 14, 964–968. [Google Scholar]
- Feng, X.; Shang, J.; Gu, Z.; Gong, J.; Chen, Y.; Liu, Y. Azelaic Acid: Mechanisms of Action and Clinical Applications. Clin. Cosmet. Investig. Dermatol. 2024, 17, 2359–2371. [Google Scholar] [CrossRef] [PubMed]
- Boo, Y.C. Mechanistic Basis and Clinical Evidence for the Applications of Nicotinamide (Niacinamide) to Control Skin Aging and Pigmentation. Antioxidants 2021, 10, 1315. [Google Scholar] [CrossRef] [PubMed]
- Marques, C.; Hadjab, F.; Porcello, A.; Lourenço, K.; Scaletta, C.; Abdel-Sayed, P.; Hirt-Burri, N.; Applegate, L.A.; Laurent, A. Mechanistic Insights into the Multiple Functions of Niacinamide: Therapeutic Implications and Cosmeceutical Applications in Functional Skincare Products. Antioxidants 2024, 13, 425. [Google Scholar] [CrossRef] [PubMed]
- Madaan, P.; Sikka, P.; Malik, D.S. Cosmeceutical Aptitudes of Niacinamide: A Review. Recent Adv. Anti-Infect. Drug Discov. 2021, 16, 196–208. [Google Scholar] [CrossRef]
- Pour Mohammad, A.; Gholizadeh Mesgarha, M.; Seirafianpour, F.; Karimi, Y.; Sodagar, S.; Afraie, M.; Goodarzi, A. A Systematic Review and Meta-Analysis of Efficacy, Safety, and Satisfaction Rates of Laser Combination Treatments vs Laser Monotherapy in Skin Rejuvenation Resurfacing. Lasers Med. Sci. 2023, 38, 228. [Google Scholar] [CrossRef]
- Seirafianpour, F.; Pour Mohammad, A.; Moradi, Y.; Dehghanbanadaki, H.; Panahi, P.; Goodarzi, A.; Mozafarpoor, S. Systematic Review and Meta-Analysis of Randomized Clinical Trials Comparing Efficacy, Safety, and Satisfaction between Ablative and Non-Ablative Lasers in Facial and Hand Rejuvenation/Resurfacing. Lasers Med. Sci. 2022, 37, 2111–2122. [Google Scholar] [CrossRef]
- Mani, N.; Pajk, F.; Vizintin, Z. Full-Face Skin Resurfacing Using a Combination of Fractional and Full Spot Ablative 2940 Nm Erbium Laser. J. Cosmet. Dermatol. 2021, 20, 110–115. [Google Scholar] [CrossRef]
- Yim, S.; Lee, Y.H.; Choi, Y.-J.; Kim, W.-S. Split-Face Comparison of the Picosecond 1064-Nm Nd:YAG Laser Using a Microlens Array and the Quasi-Long-Pulsed 1064-Nm Nd:YAG Laser for Treatment of Photoaging Facial Wrinkles and Pores in Asians. Lasers Med. Sci. 2020, 35, 949–956. [Google Scholar] [CrossRef]
- Ross, E.V.; Tidwell, W.J.; Guss, L.; Sutton, A.V. Study of a 532/1064 Fractional Picosecond Laser for Facial Rejuvenation. Dermatol. Surg. 2022, 48, 109–113. [Google Scholar] [CrossRef]
- Berna-Rico, E.; Lluch-Galcera, J.J.; Pérez-García, B.; Naharro-Rodríguez, J.; Azcárraga-Llobet, C.; Company-Quiroga, J.; Boixeda, P. Assessing the Safety and Efficacy of a New 532-Nm and 1064-Nm Laser Device with Variable Sequencing and Cryogen Spray Cooling for Rosacea Treatment. Actas Dermosifiliogr. 2025, in press. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, W.; Wang, Q. Positive Effects of Low-Dose Photodynamic Therapy with Aminolevulinic Acid or Its Methyl Ester in Skin Rejuvenation and Wound Healing: An Update. J. Biophoton. 2023, 16, e202200293. [Google Scholar] [CrossRef] [PubMed]
- Panova, O.S.; Dubensky, V.V.; Petunina, V.V.; Beimanova, M.A.; Sanches, E.A.; Gelfond, M.L.; Shilov, B.V.; Belkharoeva, R.K. Photodynamic reparative skin regeneration using application of photosensitizer gel based on chlorin e6. Biomed. Photon. 2021, 10, 4–11. [Google Scholar] [CrossRef]
- Papayan, G.V.; Podoplekina, N.D.; Glagoleva, E.N.; Petrishchev, N.N.; Galagudza, M.M. Autofluorescence Spectroscopy in Photodynamic Therapy for Skin Rejuvenation: A Theranostic Approach in Aesthetic Medicine. Photodiagn. Photodyn. Ther. 2024, 45, 103948. [Google Scholar] [CrossRef] [PubMed]
- Moubayed, S.P.; Desroches, M.-L.; Deane, E.C. Nonsurgical Facial Esthetic Procedures. Otolaryngol. Clin. N. Am. 2025, 58, 659–670. [Google Scholar] [CrossRef]
- Li, K.; Lin, Z.; Zhang, Z.; Xie, S.; Xie, G. Comparing the Effectiveness of Platelet-Rich Plasma Alone Versus Combined With Microneedles or Radiofrequency for Neck Wrinkle Treatment. J. Cosmet. Dermatol. 2025, 24, e16651. [Google Scholar] [CrossRef]
- Erlich, G.; Skorochod, R.; Sabo, E.; Saigal, R.; Dahan, E.; Wolf, Y. The Efficacy of Thermal Mechanical Fractional Injury System for Facial Rejuvenation: Subjective, Objective and Image Analysis Study. J. Cosmet. Dermatol. 2025, 24, e70063. [Google Scholar] [CrossRef]
- Manuskiatti, W.; Wannawittayapa, T.; Buranaporn, P.; Wanitphadeedecha, R.; Lizarondo, F.P.J.; Nokdhes, Y. The Efficacy and Safety of Synchronized Radiofrequency and High Intensity Facial Electrical Stimulation in Improving Facial Skin Laxity and Quality in Asians. Lasers Surg. Med. 2025, 57, 177–186. [Google Scholar] [CrossRef]
- Lv, X.; Xiang, C.; Zheng, Y.; Zhou, W.-X.; Lv, X.-L. Recent Developments in Using Microneedle Patch Technology as a More Efficient Drug Delivery System for Treating Skin Photoaging. Clin. Cosmet. Investig. Dermatol. 2024, 17, 2417–2426. [Google Scholar] [CrossRef]
- Boca, A.; Fanian, F.; Smit, R.; Redaelli, A.; Goorochurn, R.; Issa, H.; Sukmanskaya, N.; Philippon, V.; Dell’ Avanzato, R. Evaluation of the Performance and Safety of a New Micro-Needle Technology in Comparison With the Classic Needle on the Antiaging Effects of a Biorevitalizing Solution: A Randomized Split Face/Neck Study. J. Cosmet. Dermatol. 2024, 23, 3974–3985. [Google Scholar] [CrossRef]
- Kubiak, M.; Mucha, P.; Rotsztejn, H. Comparative Study of 15% Trichloroacetic Acid Peel Combined with 70% Glycolic Acid and 35% Trichloroacetic Acid Peel for the Treatment of Photodamaged Facial Skin in Aging Women. J. Cosmet. Dermatol. 2020, 19, 137–146. [Google Scholar] [CrossRef]
- Manjhi, M.; Sagar, V.; Yadav, P.; Dabas, G.; Gupta, A.; Pratap, P. A Comparative Study of 70% Glycolic Acid and 30% Trichloroacetic Acid Peel in the Treatment of Facial Atrophic Acne Scars: A Split-Face Study. J. Cutan. Aesthet. Surg. 2024, 17, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, S.; Baker, M.R.; Chatterjee, S.; Kumar, H. Botulinum Toxin: An Update on Pharmacology and Newer Products in Development. Toxins 2021, 13, 58. [Google Scholar] [CrossRef] [PubMed]
- Trinh, L.N.; Gupta, A. Hyaluronic Acid Fillers for Midface Augmentation: A Systematic Review. Facial Plast. Surg. 2021, 37, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Rostkowska, E.; Poleszak, E.; Wojciechowska, K.; Dos Santos Szewczyk, K. Dermatological Management of Aged Skin. Cosmetics 2023, 10, 55. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Feature | Fitzpatrick Skin Types V–VI | Asian Skin | Caucasian Skin |
|---|---|---|---|
| Dermis structure | Thick dermis and stratum corneum | Thick dermis, intermediate melanin | Thin dermis and epidermis |
| Melanin and pigmentation | High melanin, large dispersed melanosomes | Moderate melanin, prone to pigment retention | Low melanin, higher UV sensitivity |
| Wrinkle onset | Delayed (5th decade) | Delayed (late 4th to 5th decade) | Early (3rd–4th decade) |
| Periorbital aging | Less pronounced | Pronounced wrinkling and hollowing | Crow’s feet and forehead lines |
| Midface aging | Marked malar fat pad descent, infraorbital hollowing | Early malar descent, flat midface | Visible volume loss, deeper folds |
| Perioral aging | Minimal volume loss, fewer perioral wrinkles | Moderate perioral aging | Marked lip volume loss, rhytids |
| Neck/jawline changes | Submental fullness, obtuse cervicomental angle | Less defined jawline with aging | Sagging and jowls common |
| Pigmentary disorders | Frequent lentigines and uneven pigmentation | Melasma, lentigines, seborrheic keratoses | Solar lentigines, telangiectasias |
| Skin Layer | Change with Aging | Approx. Age of Onset | Clinical Implications |
|---|---|---|---|
| Epidermis | Thinning and flattening of dermoepidermal junction | 30–40 years | Fragile skin, increased permeability |
| Epidermis | Reduced turnover and delayed wound healing | 40+ years | Delayed regeneration and poor healing |
| Dermis | Collagen and elastin fragmentation | 40–50 years | Loss of firmness, wrinkles |
| Dermis | Reduced fibroblast activity and ECM remodeling | 50+ years | Loss of elasticity, thinning |
| Vasculature | Capillary rarefaction and decreased diameter | 50–60 years | Reduced oxygenation, pallor |
| Vasculature | Vascular wall degeneration and risk of stasis | 60+ years | Edema, sluggish healing |
| Annexes | Sebaceous and sweat gland atrophy | 50+ years | Dryness, impaired thermoregulation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naharro-Rodriguez, J.; Bacci, S.; Hernandez-Bule, M.L.; Perez-Gonzalez, A.; Fernandez-Guarino, M. Decoding Skin Aging: A Review of Mechanisms, Markers, and Modern Therapies. Cosmetics 2025, 12, 144. https://doi.org/10.3390/cosmetics12040144
Naharro-Rodriguez J, Bacci S, Hernandez-Bule ML, Perez-Gonzalez A, Fernandez-Guarino M. Decoding Skin Aging: A Review of Mechanisms, Markers, and Modern Therapies. Cosmetics. 2025; 12(4):144. https://doi.org/10.3390/cosmetics12040144
Chicago/Turabian StyleNaharro-Rodriguez, Jorge, Stefano Bacci, Maria Luisa Hernandez-Bule, Alfonso Perez-Gonzalez, and Montserrat Fernandez-Guarino. 2025. "Decoding Skin Aging: A Review of Mechanisms, Markers, and Modern Therapies" Cosmetics 12, no. 4: 144. https://doi.org/10.3390/cosmetics12040144
APA StyleNaharro-Rodriguez, J., Bacci, S., Hernandez-Bule, M. L., Perez-Gonzalez, A., & Fernandez-Guarino, M. (2025). Decoding Skin Aging: A Review of Mechanisms, Markers, and Modern Therapies. Cosmetics, 12(4), 144. https://doi.org/10.3390/cosmetics12040144