
Storytelling of Myocardial Biopsy


Department of Cardiac, Thoracic, Vascular Sciences and Public Health, University of Padua, Via A. Gabelli, 86-35121 Padova, Italy
Biology 2025, 14(3), 306; https://doi.org/10.3390/biology14030306
Submission received: 21 February 2025
/
Revised: 14 March 2025
/
Accepted: 17 March 2025
/
Published: 18 March 2025
(This article belongs to the Special Issue Experimental Biology 100 Years After the Foundation of the Italian Society: A Celebratory Special Issue)
Simple Summary
Biopsy is the piece of tissue taken from a living patient. As far as the heart, the current practice is to remove myocardium from the endocardium of the right ventricle, via a venous pathway, by a catheter with a bioptome at the extremity, able to catch endomyocardium. Inflammatory, storage, fibrotic, neoplastic tissues are the targets. With cardiac transplantation, the whole heart of the recipient is available as a big biopsy. Various pathological investigation techniques may be used: histology, immunohistochemistry electron microscopy and even molecular, the latter in search of infective organisms or gene mutations. Transplantation gives the opportunity to study the whole heart of the recipient, with the possibility to study the basic cardiac disease and even discover new morbid entities. A chance that in the past was reserved only to autopsy. Moreover, periodically performed endomyocardial biopsy allows to check the occurrence of rejection, to be treated by life saving drug therapy.
Abstract
A biopsy involves the removal of a piece or an entire organ from a living patient. The former began with open heart surgery (surgical pathology) and the latter with the recipient heart in cardiac transplantation. Transvenous or transarterial catheterization is the current procedure to performed endomyocardial biopsy with bioptome from the ventricles. This manoeuvre was first carried out by Werner Forssmann through a urological catheter in 1929, which he introduced into his radial left vein until it reached the RV. Then, in London in 1974, Richardson invented a new technique with a catheter via the right femoral vein, which he applied with success in patients with multiple myocardial diseases, both inflammatory and non-inflammatory. Subsequently, a transjugular endomyocardial biopsy was accomplished by Margaret Billingham to monitor heart rejection during cardiac transplantation. In the beginning, only histology for a light microscope, and rarely during electron microscopy, was employed. With the advent of molecular techniques and the discovery of polymerase chain reaction (PCR), molecular investigation became part of the gold standard for diagnosis involving EMB: histology, immunohistochemistry and molecular investigation, the latter in search of a viral cause. Nowadays, EMB is frequently employed in infiltrative (amyloidosis) and storage diseases (e.g., hemochromatosis and Fabry diseases). Diagnosis of myocarditis is now possible through Magnetic Cardiac Resonance (MCR), in place of BEM histology, thanks to oedema. With the help of ECMO, it is possible to allow the heart to rest, supporting its recovery from ejection fraction even in fulminant myocarditis. Cardiac transplantation with the pathological study of the recipient heart offers the opportunity to discover and study new diseases, like restrictive cardiomyopathy and a non-compacted left ventricle.
1. Introduction: History of Cardiac Biopsy
Biopsy means to remove a piece of or an entire organ from a living patient.
As far as the heart is concerned, needle percutaneous transthoracic biopsy was first accomplished by Casten and Marsh in 1953 [1] and by Kent et al. in 1956 [2].
Since 1954, open heart surgery with extracorporeal circulation has made it possible to perform a cardiac biopsy.
2. Cardiac Transplantation and Cardiomyopathies
With cardiac transplantation, Christiaan Barnard in 1968 and Shumway in 1969 removed the whole heart (“cardiectomy”) and implanted a donor heart. The entire heart of a living human being was sent from the surgical theatre by the surgeon to the pathologist. It was a novel opportunity to discover and investigate new cardiac morbid entities.
A particularly dilated cardiomyopathy (DCM), the most frequent indication for a heart transplant, presented the opportunity to study the so-called “cor bovinum” in depth Figure 3.
Primary restrictive cardiomyopathy (RCM) represents the paradox of a small heart requiring a transplant Figure 4a,b, because the ventricles are unable to dilate during diastole, causing severe congestive heart failure. Since the histology shows myocardial disarray and the genetic background revealed that sarcomeric proteins are involved as in hypertrophic cardiomyopathy (HCM), this condition was named “HCM without hypertrophy”.
Also during cardiac transplantation, an amazing cardiomyopathy was discovered, named “non-compact left ventricle”, accounting for poor contractility and consisting of coarse trabeculae and deep intertrabecular fissures, with the endocardium almost reaching the epicardium Figure 5. Trabeculae observed via a 2D echo may wrongly be interpreted as mural thrombi.
Hemochromatosis is a secondary cardiomyopathy with myocardium, appearing brown to the naked eye because of myocardial storage of haemoglobin iron Figure 6. Multiple blood perfusions can be the cause.
Also, primary cardiac tumours can be diagnosed for the first time during a heart transplant.
Cardiac fibroma is often located within the ventricular septum, mimicking the asymmetric septal hypertrophy of hypertrophic cardiomyopathy, which may be wrongly diagnosed by an echo prior to heart transplantation Figure 7.
3. Arrhythmogenic Cardiomyopathy
Another adventure in the history of medicine was arrhythmogenic cardiomyopathy (ACM), which was discovered by Sergio Dalla Volta in 1961 [6] Figure 8a. At angiography, the right ventricle was so enlarged that the name “auricularization of the right ventricle” was employed Figure 8b. Later, with the advent of cardiac transplantation, this patient was successfully operated on in 1989. The recipient heart showed a huge dilatation of the right ventricular cavity with thin, translucent fibro-fatty wall Figure 8c,b. Oddly enough, in 1961, the “auricolarization” of the right ventricle was considered a sequela of myocardial infarction. At that time, coronary angiography did not exist yet and coronary arteries could only be investigated during an autopsy.
4. History of Cardiac Catheterization
A milestone in the history of EMB dates back in 1929, when the German urologist Werner Forssmann [7] Figure 9a invented cardiac catheterization, successfully accessing his own right ventricle Figure 9b with a ureteral catheter inserted into his left radial vein.
The catheter of EMB reaches the trabeculae of the ventricular septum of the right ventricle, where EMB is performed Figure 10.
5. The Discovery of Microscope
6. Monitoring of Cardiac Transplant Rejection by Endomyocardial Biopsy
7. Clinical Indications of Endomyocardial Biopsy
Concerns regarding EMB were expressed in the early season by authoritative pathologists like Ferrans and Roberts, who questioned its utility [9] Table 1.
EMB proved to be of great help in the diagnosis of cardiac tumours. A mass found via 2D echo at the right atrioventricular grove underwent EMB with specific immunohistochemistry, which facilitated a suggested diagnosis of angiosarcoma [10] Figure 14.
Other examples, in our experience, of malignant neoplasms of the heart with diagnosis achieved by EMB immunohistochemistry include T cell atrial lymphoma Figure 15 [11] and cardiac fibrosarcoma Figure 16 [12].
EMB is also particularly useful for differential diagnosis of non-malignant masses, like Loeffler’s eosinophilic disease of the endocardium, known as obliterative restrictive cardiomyopathy Figure 17 [13].
Table 2 shows indications for EMB.
As far as myocardial inflammatory disease (myocarditis) is concerned, EMB plays a crucial role in ascertaining the histotype (lymphocytic, neutrophil, eosinophil, granulomatous non-caseous, and giant cells) Figure 18, which represents a fundamental source of information for therapeutic strategies [14,15].
8. The Invention of Polymerase Chain Reaction: Molecular Pathology
Lymphocytic myocarditis is usually viral. Following the invention of polymerase chain reaction (PCR) by Kary Mullis in 1983 Figure 19 [16], it is now possible to establish the type of virus by EMB [16].
Life-threatening viral myocarditis affects not only adults but also children and infants Figure 20 [17].
Accurate interpretation of EMB is currently feasible not only through histology and light microscopy (staining histologic sections, histochemistry, and immunohistochemistry) but also through electron microscopy, molecular biology with in situ hybridization, PCR, and gene sequencing. Molecular analysis is part of the diagnostic gold standard Table 3 [18].
Clinical investigation by electroanatomic mapping may be strategic for detecting scars in myocardial diseases, like in ACM, and determining where to perform EMB Figure 21.
9. Diagnosis of ACM Through Endomyocardial Biopsy and Infiltrative Disease as Amyloidosis
In vitro investigation of autopsy heart specimens of ACM Figure 22 established that a residual myocardium <59% is diagnostic, with specificity of 90% and sensitivity of 80% Figure 23 [19].
Diagnosis of infiltrative diseases like amyloidosis can easily be detected by EMB and using specific staining like Congo Red and Tioflavine staining Figure 24.
10. EMB and Electron Microscopy
11. Endomyocardial Biopsy and Myocarditis: The Invention of Extracorporeal Membrane Oxygenation and Its Efficacy
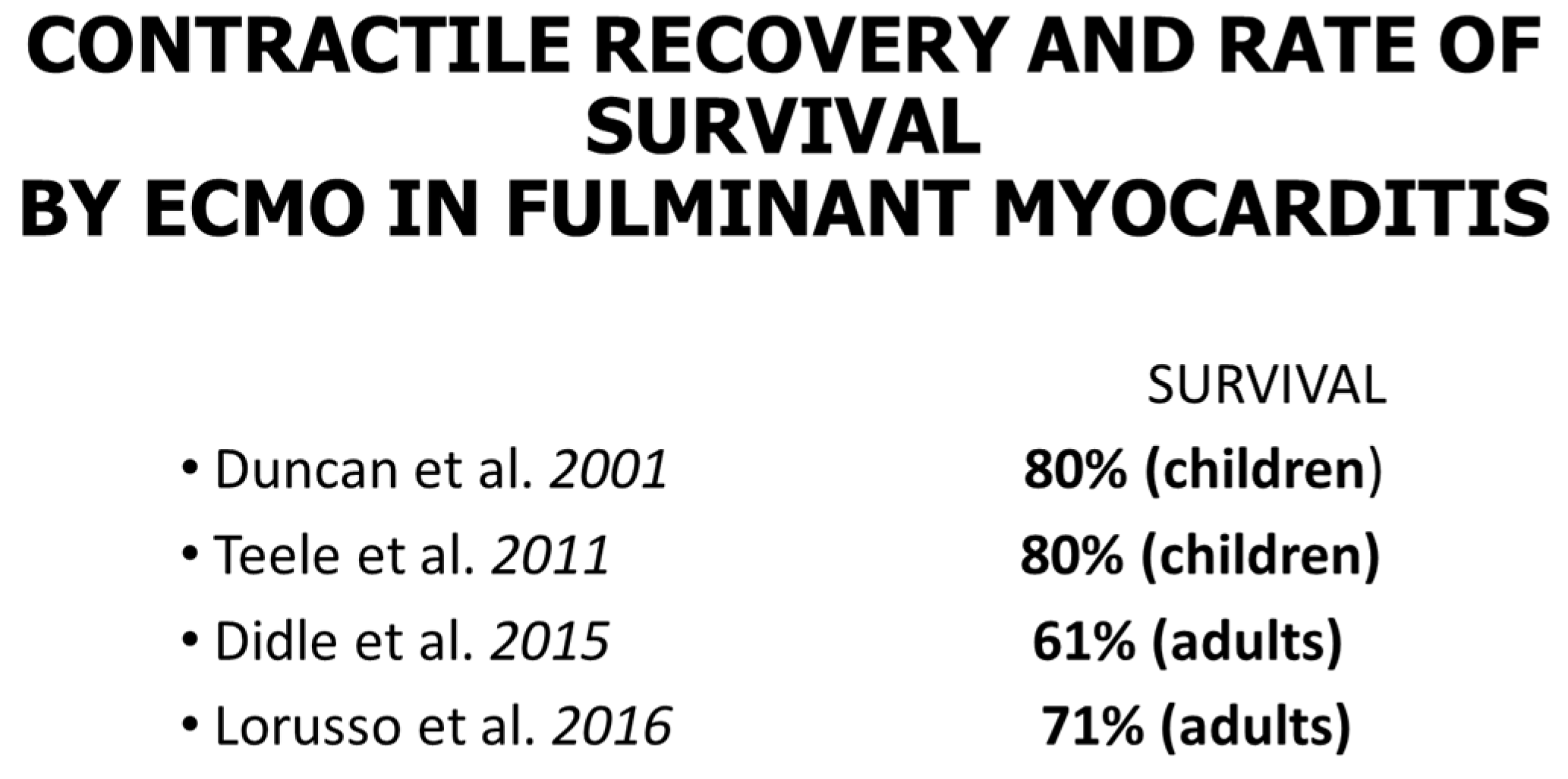
As far as myocarditis is concerned, the “Dallas Criteria” postulated that to achieve a diagnosis, [20,21,22] myocyte necrosis is the “condition sine qua non” in association with inflammatory infiltrate Figure 28. The observation of myocardial inflammation with interstitial oedema Figure 29 in the absence of myocardial necrosis [20] explains why extracorporeal membrane oxygenation (ECMO) Figure 30a, invented by Robert Bartlett (1939-) [22] Figure 30b, fulminant myocarditis, presenting with sudden onset of severe pump failure, resolves spontaneously because of reversible myocardial injury. ECMO may temporarily supply myocardial contractility until spontaneous recovery occurs. Ejection fraction may increase in fulminant myocarditis, with a high rate of survival Figure 31.
A left ventricular assistance device (LVAD) is another mechanical support therapy, and a source of large number of samples from myocardial specimens, available for in vivo histological and molecular analysis (biopsy).
12. Conclusions
EMB is the gold standard device for the diagnosis of myocarditis, cardiac rejection and infiltrative/storage disorders. The histotypes resulting from EMB can be used to inform drug therapy strategies. Molecular biology techniques should be routinely carried out as a useful complementary investigation. Sampling is fundamental (Table 4). The gold standard for diagnosis of inflammatory cardiomyopathy is a combination of histology, immunohistochemistry and molecular analysis (Table 3). EMB should be performed only if the whole “armamentarium” for pathology investigation is available.
Funding
This study was supported by the National Health system through the Veneto Region and by the ARCA research Foundation, Padua, Italy.
Acknowledgments
Giulia Vangelista performed the secretarial work.
Conflicts of Interest
The author declares no conflicts of interest.
Abbreviations
| ACM | Arrhythmogenic right ventricular cardiomyopathy. |
| DCM | Dilated cardiomyopathy. |
| ECMO | Extracorporeal membrane oxygenation. |
| EMB | Endomyocardial biopsy. |
| HCM | Hypertrophic cardiomyopathy. |
| MCR | Magnetic Cardiac Resonance. |
| PCR | Polymerase chain reaction. |
| RCM | Restrictive cardiomyopathy. |
| RV | Right ventricle. |
References
- Casten, G.G.; Marsh, J.B. Metabolic Studies on Cardiac Tissue Obtained by Needle Biopsy in the Intact Unanesthetized Dog. Circ. Res. 1953, 1, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Kent, G.; Sutton, D.C.; Sutton, G.C. Needle Biopsy of the Human Ventricular Myocardium. Q. Bull. Northwest Univ. Med. Sch. 1956, 30, 213–214. [Google Scholar]
- Sakakibara, S.; Konno, S. Endomyocardial Biopsy. Jpn. Heart J. 1962, 3, 537–543. [Google Scholar] [CrossRef]
- Richardson, P.J. King’s Endomyocardial Bioptome. Lancet 1974, 1, 660–661. [Google Scholar] [CrossRef]
- Valente, M.; Cocco, P.; Thiene, G.; Casula, R.; Poletti, A.; Milanesi, O.; Fasoli, G.; Livi, U. Cardiac Fibroma and Heart Transplantation. J. Thorac. Cardiovasc. Surg. 1993, 106, 1208–1212. [Google Scholar] [CrossRef] [PubMed]
- Dalla Volta, S.; Battaglia, G.; Zerbini, E. ‘Auricularization’ of Right Ventricular Pressure Curve. Am. Heart J. 1961, 61, 25–33. [Google Scholar] [CrossRef]
- Forssmann, W. Die Sondierung des rechten Herzens. Klin. Wochenschr. 1929, 8, 2085–2087. [Google Scholar] [CrossRef]
- Hooke, R. Micrographia, or, Some Physiological Descriptions of Minute Bodies Made by Magnifying Glasses with Observations and Inquiries Thereupon; Martyn, J., Allestry, J., Eds.; Royal Society: London, UK, 1665. [Google Scholar]
- Ferrans, V.J.; Roberts, W.C. Myocardial Biopsy: A Useful Diagnostic Procedure or Only a Research Tool? Am. J. Cardiol. 1978, 41, 965–967. [Google Scholar] [CrossRef]
- Poletti, A.; Cocco, P.; Valente, M.; Fasoli, G.; Chioin, R.; Thiene, G. In Vivo Diagnosis of Cardiac Angiosarcoma by Endomyocardial Biopsy. Cardiovasc. Pathol. 1993, 2, 89–91. [Google Scholar] [CrossRef]
- Testolin, L.; Basso, C.; Pittarello, D.; Casarotto, D.; Valente, M. Cardiogenic Shock Due to Metastatic Cardiac Lymphoma: Still a Diagnostic and Therapeutic Challenge. Eur. J. Cardiothorac. Surg. 2001, 19, 365–368. [Google Scholar] [CrossRef]
- Basso, C.; Stefani, A.; Calabrese, F.; Fasoli, G.; Valente, M. Primary Right Atrial Fibrosarcoma Diagnosed by Endocardial Biopsy. Am. Heart J. 1996, 131, 399–402. [Google Scholar] [CrossRef] [PubMed]
- Perazzolo Marra, M.; Thiene, G.; Rizzo, S.; De Lazzari, M.; Carturan, E.; Tona, F.; Caforio, A.L.; Cacciavillani, L.; Marcolongo, R.; Tarantini, G.; et al. Cardiac Magnetic Resonance Features of Biopsy-Proven Endomyocardial Diseases. JACC Cardiovasc. Imaging 2014, 7, 309–312. [Google Scholar] [CrossRef]
- Leone, O.; Veinot, J.P.; Angelini, A.; Baandrup, U.T.; Basso, C.; Berry, G.; Bruneval, P.; Burke, M.; Butany, J.; Calabrese, F.; et al. 2011 Consensus Statement on Endomyocardial Biopsy from the Association for European Cardiovascular Pathology and the Society for Cardiovascular Pathology. Cardiovasc. Pathol. 2012, 21, 245–274. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.T.; Baughman, K.L.; Feldman, A.M.; Frustaci, A.; Jessup, M.; Kuhl, U.; Levine, G.N.; Narula, J.; Starling, R.C.; Towbin, J.; et al. The Role of Endomyocardial Biopsy in the Management of Cardiovascular Disease: A Scientific Statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation 2007, 116, 2216–2233. [Google Scholar] [CrossRef]
- Mullis, K.B.; Erlich, H.A.; Gelfand, D.H.; Horn, G.; Saiki, R.K. Process for Amplifying, Detecting, and/or Cloning Nucleic Acid Sequences. U.S. Patent 4,683,195, 7 February 1986. [Google Scholar]
- Basso, C.; Calabrese, F.; Angelini, A.; Carturan, E.; Thiene, G. Classification and Histological, Immunohistochemical, and Molecular Diagnosis of Inflammatory Myocardial Disease. Heart Fail. Rev. 2013, 18, 673–681. [Google Scholar] [CrossRef]
- Thiene, G.; Bruneval, P.; Veinot, J.; Leone, O. Diagnostic Use of the Endomyocardial Biopsy: A Consensus Statement. Virchows Arch. 2013, 463, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Basso, C.; Ronco, F.; Marcus, F.; Abudureheman, A.; Rizzo, S.; Frigo, A.C.; Bauce, B.; Maddalena, F.; Nava, A.; Corrado, D.; et al. Quantitative Assessment of Endomyocardial Biopsy in Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia: An In Vitro Validation of Diagnostic Criteria. Eur. Heart J. 2008, 29, 2760–2771. [Google Scholar] [CrossRef]
- Aretz, H.T.; Billingham, M.E.; Edwards, W.D.; Factor, S.M.; Fallon, J.T.; Fenoglio, J.J., Jr.; Olsen, E.G.; Schoen, F.J. Myocarditis: A Histopathologic Definition and Classification. Am. J. Cardiovasc. Pathol. 1987, 1, 3–14. [Google Scholar]
- Baughman, K.L. Diagnosis of Myocarditis: Death of Dallas Criteria. Circulation 2006, 113, 593–595. [Google Scholar] [CrossRef]
- Bartlett, R.H.; Kittredge, D.; Noyes, B.S., Jr.; Willard, R.H., III; Drinker, P.A. Development of a Membrane Oxygenator: Overcoming Blood Diffusiolimitation. J. Thorac. Cardiovasc. Surg. 1969, 58, 795–800. [Google Scholar] [CrossRef]
- Duncan, B.W.; Bohn, D.J.; Atz, A.M.; French, J.W.; Laussen, P.C.; Wessel, D.L. Mechanical Circulatory Support for the Treatment of Children with Acute Fulminant Myocarditis. J. Thorac. Cardiovasc. Surg. 2001, 122, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Teele, S.A.; Allan, C.K.; Laussen, P.C.; Newburger, J.W.; Gauvreau, K.; Thiagarajan, R.R. Management and Outcomes in Pediatric Patients Presenting with Acute Fulminant Myocarditis. J. Pediatr. 2011, 158, 638–643.e1. [Google Scholar] [CrossRef] [PubMed]
- Diddle, J.W.; Almodovar, M.C.; Rajagopal, S.K.; Rycus, P.T.; Thiagarajan, R.R. Extracorporeal Membrane Oxygenation for the Support of Adults with Acute Myocarditis. Crit. Care Med. 2015, 43, 1016–1025. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, R.; Centofanti, P.; Gelsomino, S.; Barili, F.; Di Mauro, M.; Orlando, P.; Milazzo, F.; Dato, G.A.; Casabona, R.; Casali, G.; et al. Venoarterial Extracorporeal Membrane Oxygenation for Acute Fulminant Myocarditis in Adult Patients: A 5-Year Multi-Institutional Experience. Ann. Thorac. Surg. 2016, 101, 919–926. [Google Scholar] [CrossRef]
Figure 1.
Instrument used for endomyocardial biopsy by Konno (a). The technique of transvenous endomyocardial biopsy (EMB), introduced in Japan by Sakakibara and Konno in 1963 [3], with the bioptome at the extremity of the catheter (b).
Figure 1.
Instrument used for endomyocardial biopsy by Konno (a). The technique of transvenous endomyocardial biopsy (EMB), introduced in Japan by Sakakibara and Konno in 1963 [3], with the bioptome at the extremity of the catheter (b).

Figure 2.
Endomyocardial biopsy (EMB) performed via a transfemoral venous approach (a) with endomyocardial fragments (b) [4].
Figure 2.
Endomyocardial biopsy (EMB) performed via a transfemoral venous approach (a) with endomyocardial fragments (b) [4].
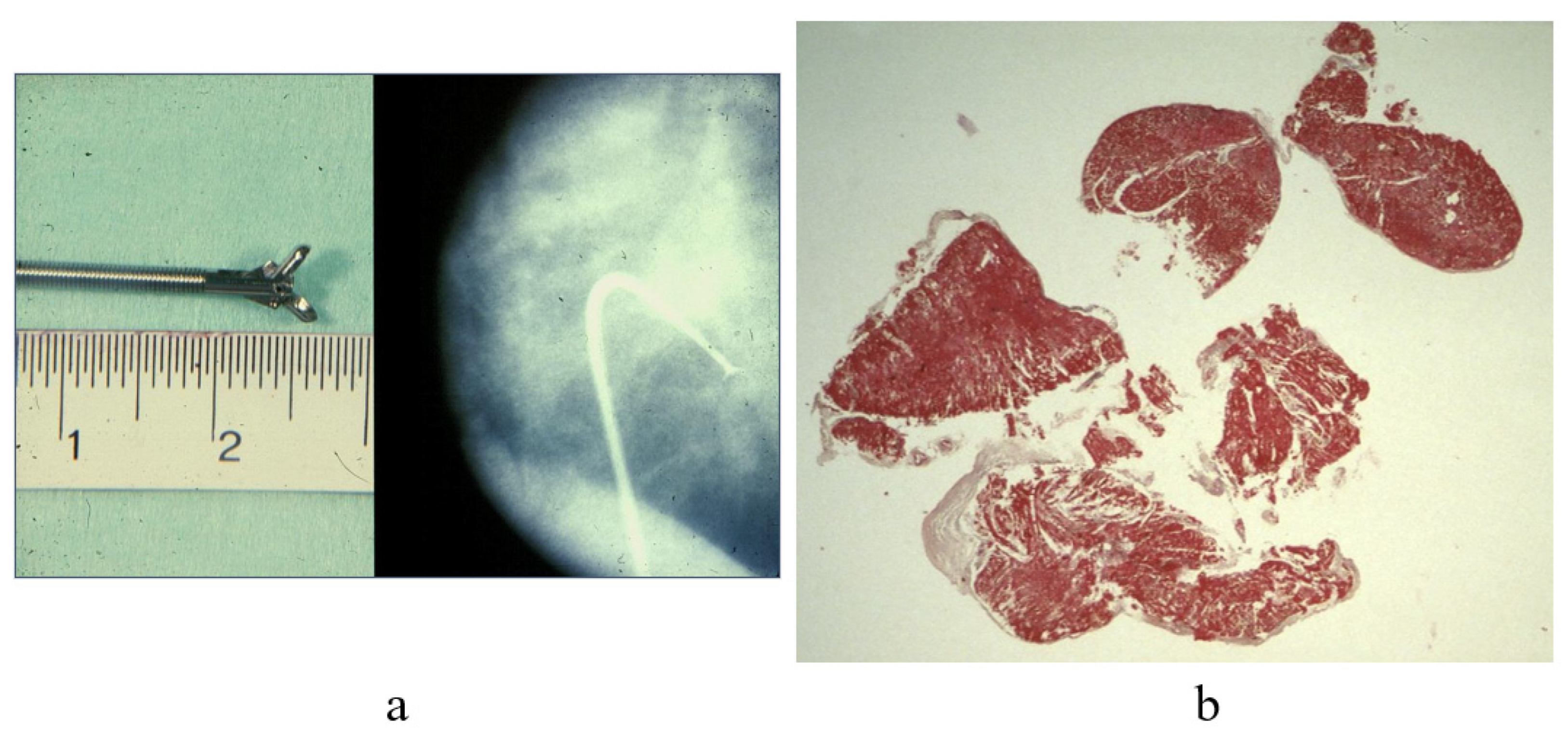
Figure 3.
Cor bovinum and dilated cardiomyopathy in the first cardiac transplantation in Italy. (a) Gross view of the heart; (b) histology with myocytolysis performed using Hematoxylin–Eosin stain.
Figure 3.
Cor bovinum and dilated cardiomyopathy in the first cardiac transplantation in Italy. (a) Gross view of the heart; (b) histology with myocytolysis performed using Hematoxylin–Eosin stain.
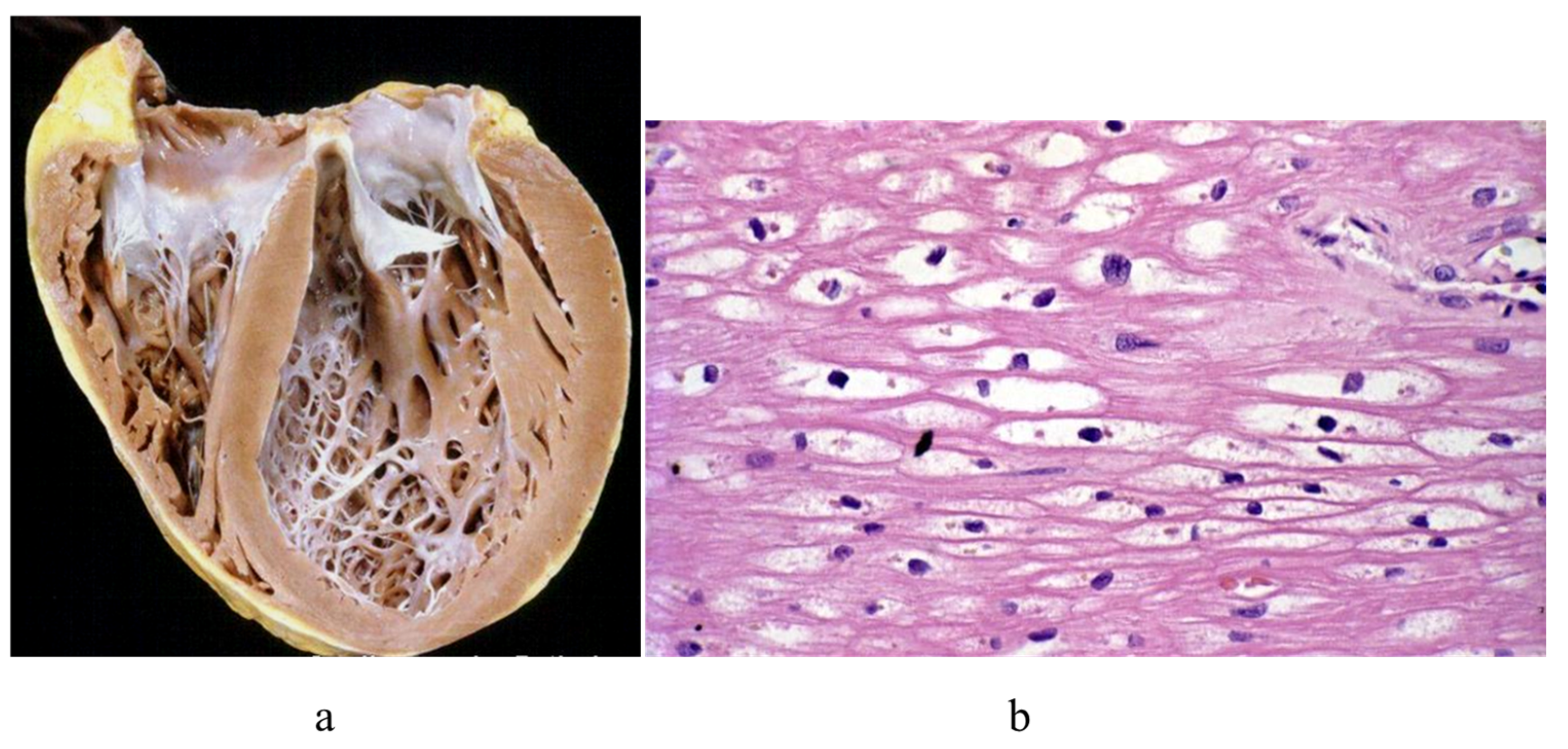
Figure 4.
Restrictive cardiomyopathy. (a) Comparison between dilated vs. restrictive cardiomyopathies. (b) Histology of the myocardium in restrictive cardiomyopathy with disarray. Azan Mallory staining.
Figure 4.
Restrictive cardiomyopathy. (a) Comparison between dilated vs. restrictive cardiomyopathies. (b) Histology of the myocardium in restrictive cardiomyopathy with disarray. Azan Mallory staining.
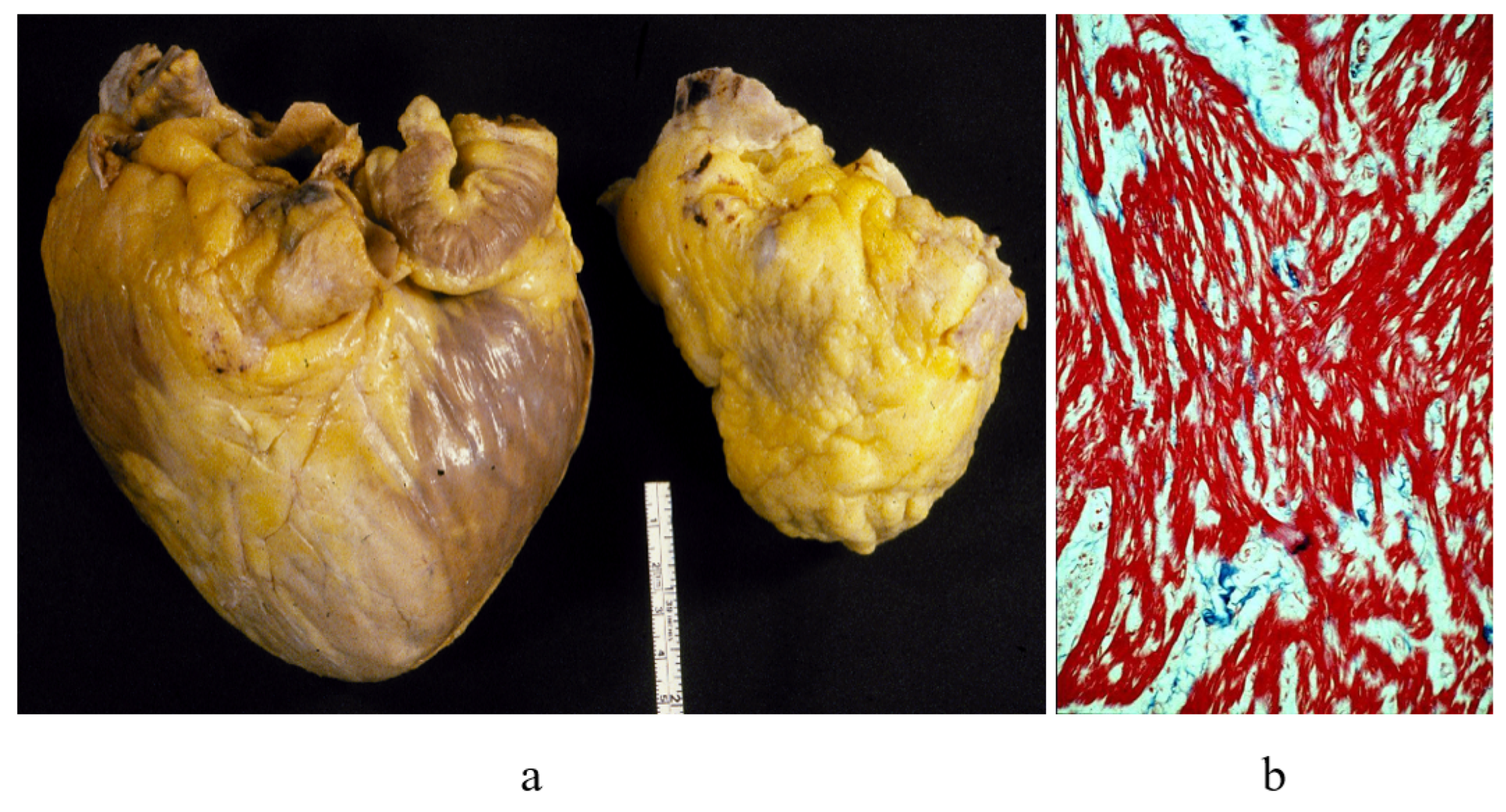
Figure 5.
(a) Non-compact left ventricle; (b) coarse trabeculae, wrongly interpreted as thrombi by ECO.
Figure 5.
(a) Non-compact left ventricle; (b) coarse trabeculae, wrongly interpreted as thrombi by ECO.
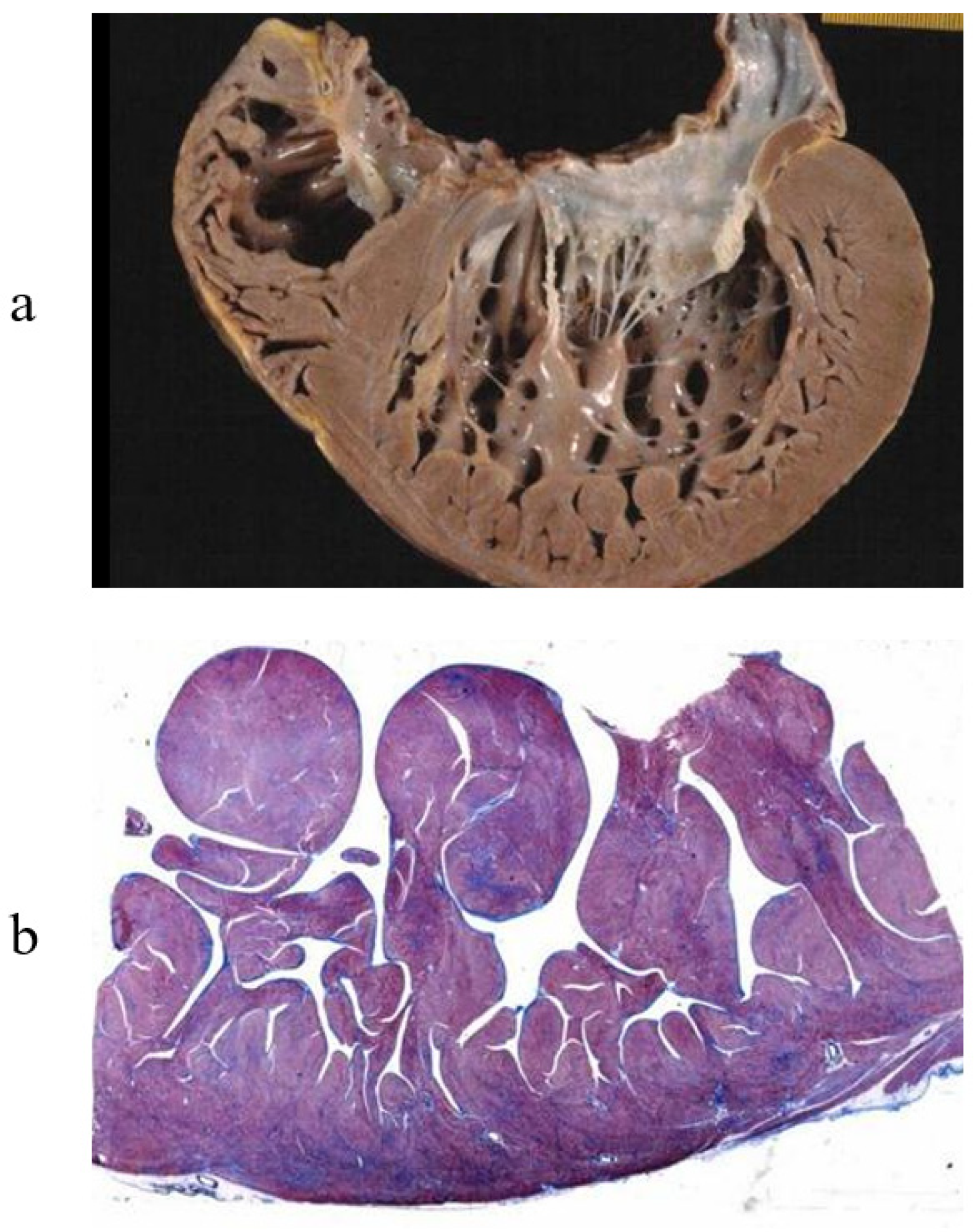
Figure 6.
Hemochromatosis in a heart specimen. (a) Brown myocardium at gross examination. (b) Storage of iron within the cardiomyocytes. (c,d) Endomyocardial biopsy with iron storage in cardiomyocytes.
Figure 6.
Hemochromatosis in a heart specimen. (a) Brown myocardium at gross examination. (b) Storage of iron within the cardiomyocytes. (c,d) Endomyocardial biopsy with iron storage in cardiomyocytes.
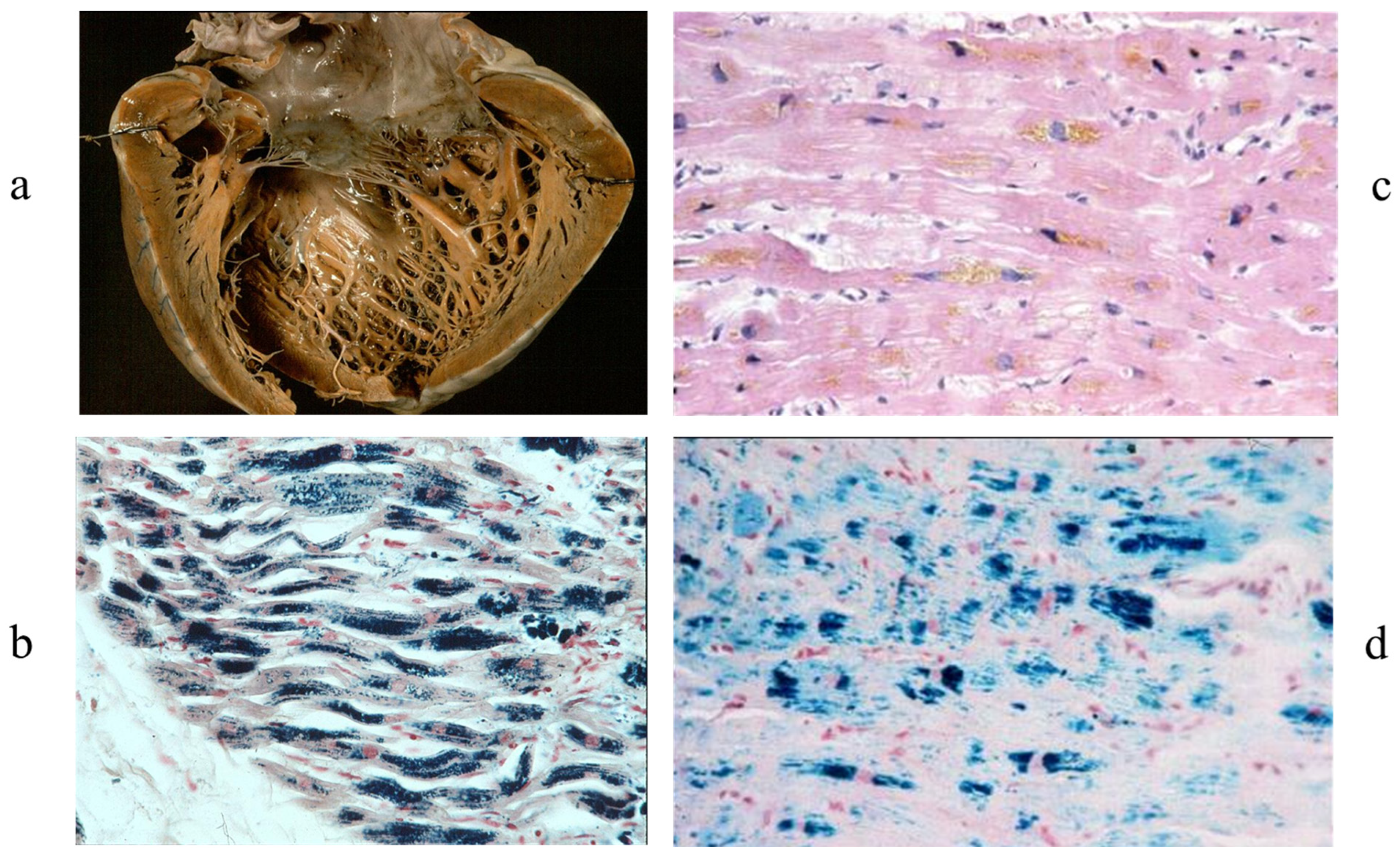
Figure 7.
Huge cardiac fibroma. (a) Gross view shows involvement of the ventricular septum mimicking hypertrophic cardiomyopathy [5]. (b) At histology, the mass consists of collagen. Azan Mallory staining was used [5].
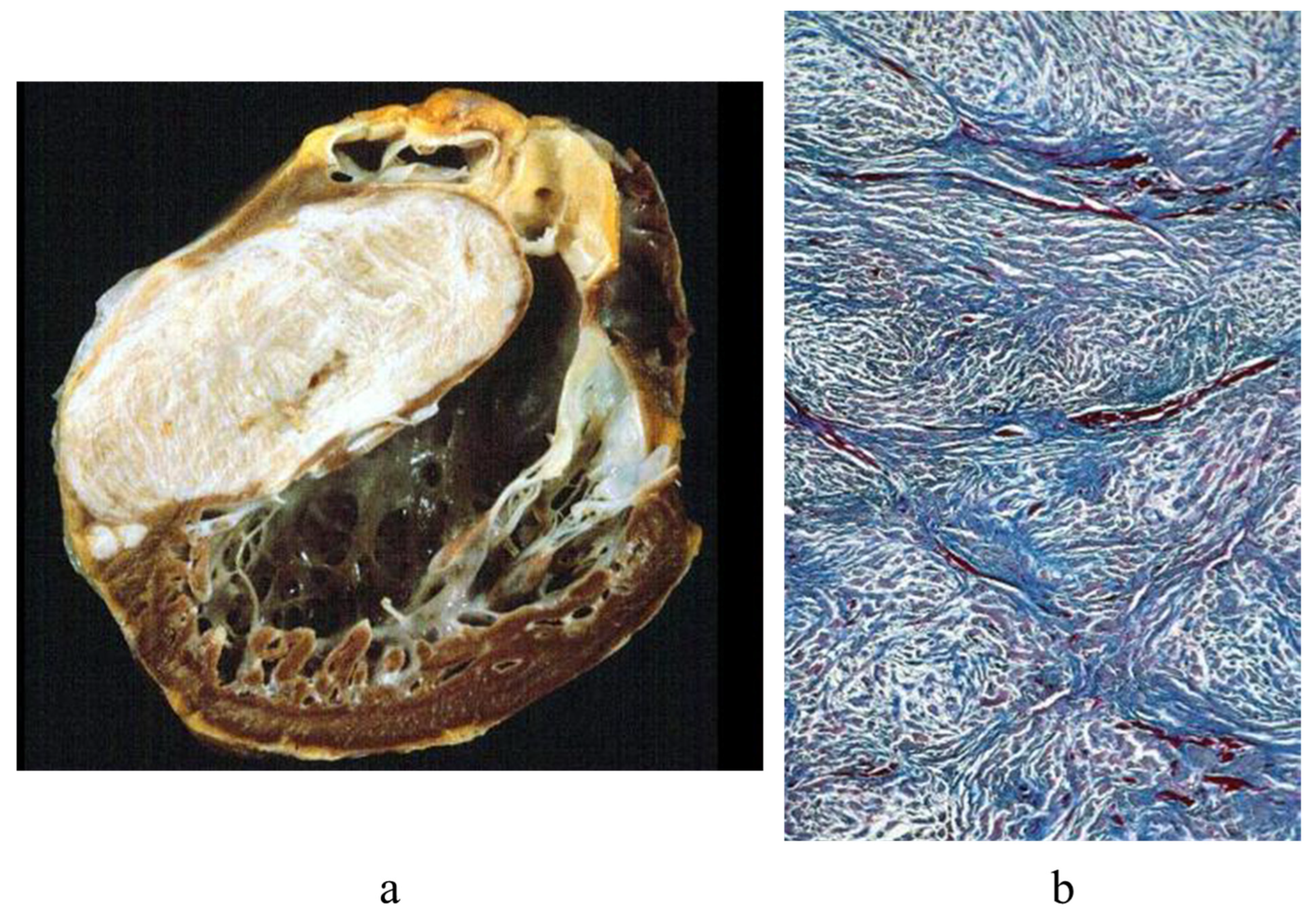
Figure 8.
An image of a female with ACM published by Sergio Dalla Volta (a) in 1961 [6] (b), showing huge dilatation of the right ventricular cavity and paper-thin free wall (c,d). In 1996, she underwent a successful cardiac transplantation due to congestive heart failure.
Figure 8.
An image of a female with ACM published by Sergio Dalla Volta (a) in 1961 [6] (b), showing huge dilatation of the right ventricular cavity and paper-thin free wall (c,d). In 1996, she underwent a successful cardiac transplantation due to congestive heart failure.
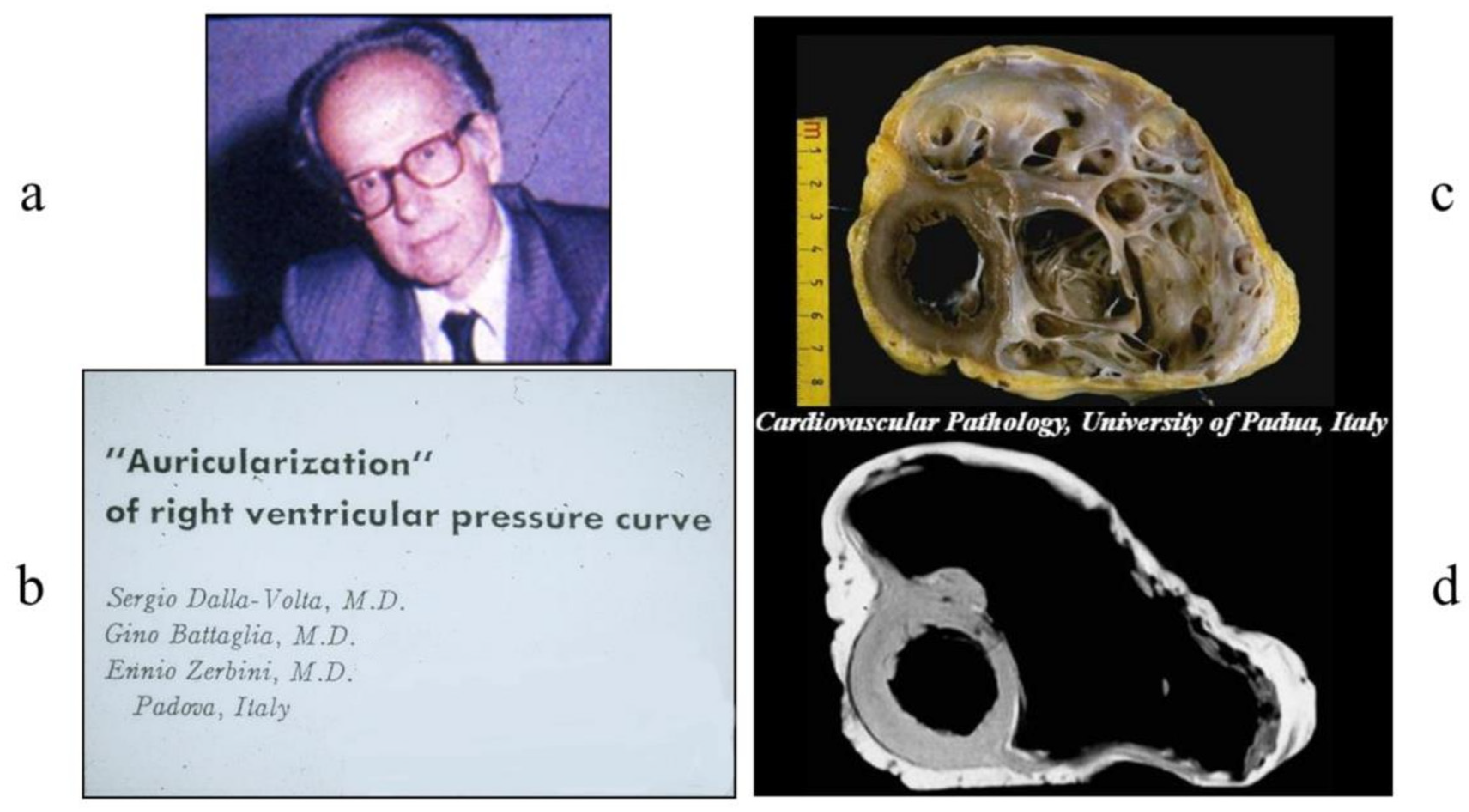
Figure 9.
Unlike skeletal muscle, once, the myocardium could be investigated only at autopsy. With the advent of cardiac catheterization in 1929 by the German urologist Werner Forssmann (1904–1979) (a), it became feasible to safely reach the right ventricle in vivo (b) [7].
Figure 9.
Unlike skeletal muscle, once, the myocardium could be investigated only at autopsy. With the advent of cardiac catheterization in 1929 by the German urologist Werner Forssmann (1904–1979) (a), it became feasible to safely reach the right ventricle in vivo (b) [7].
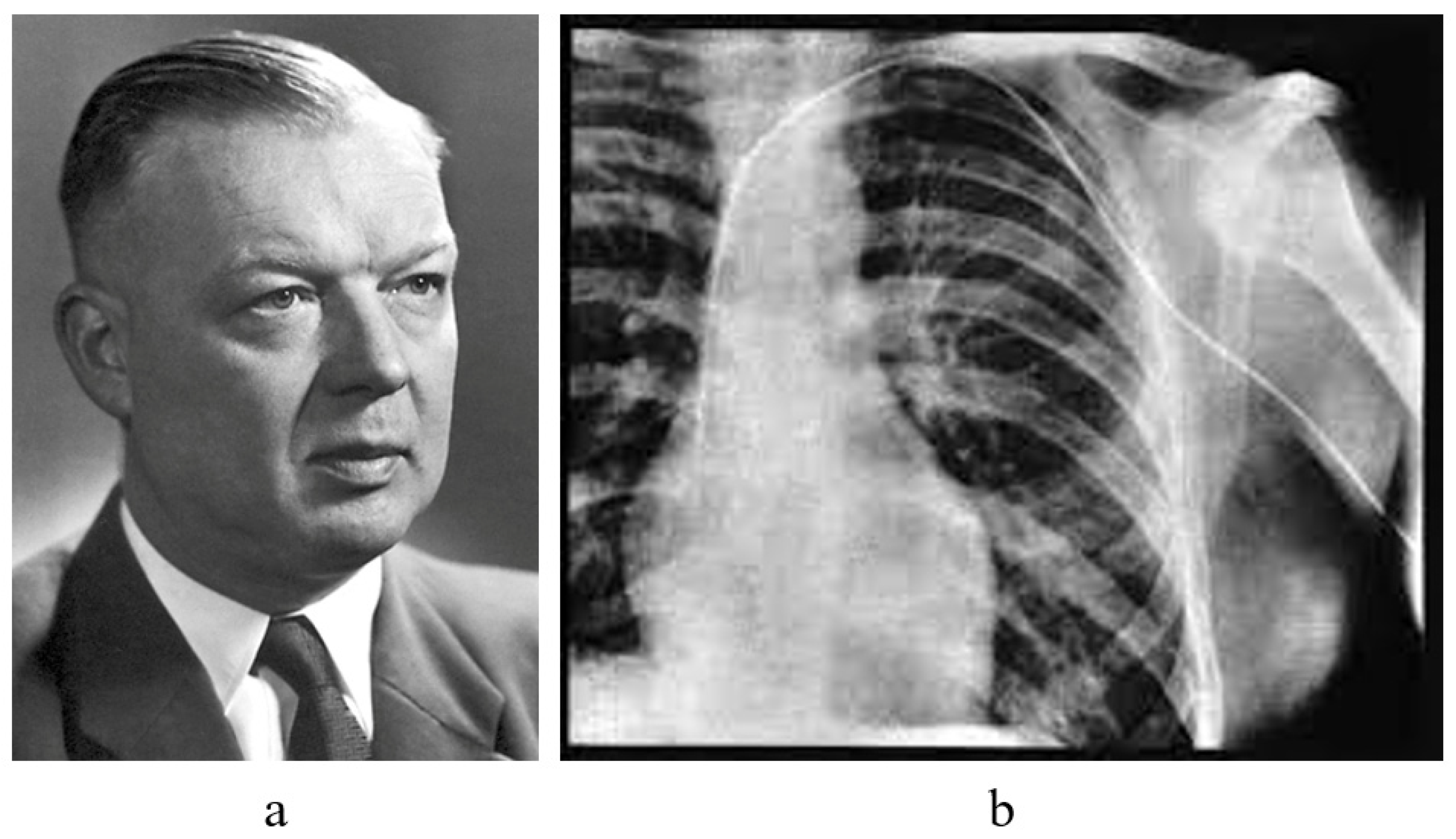
Figure 10.
A catheter with a bioptome within the right ventricle (a) and septal trabeculae (b), where endomyocardial biopsy is performed.
Figure 10.
A catheter with a bioptome within the right ventricle (a) and septal trabeculae (b), where endomyocardial biopsy is performed.
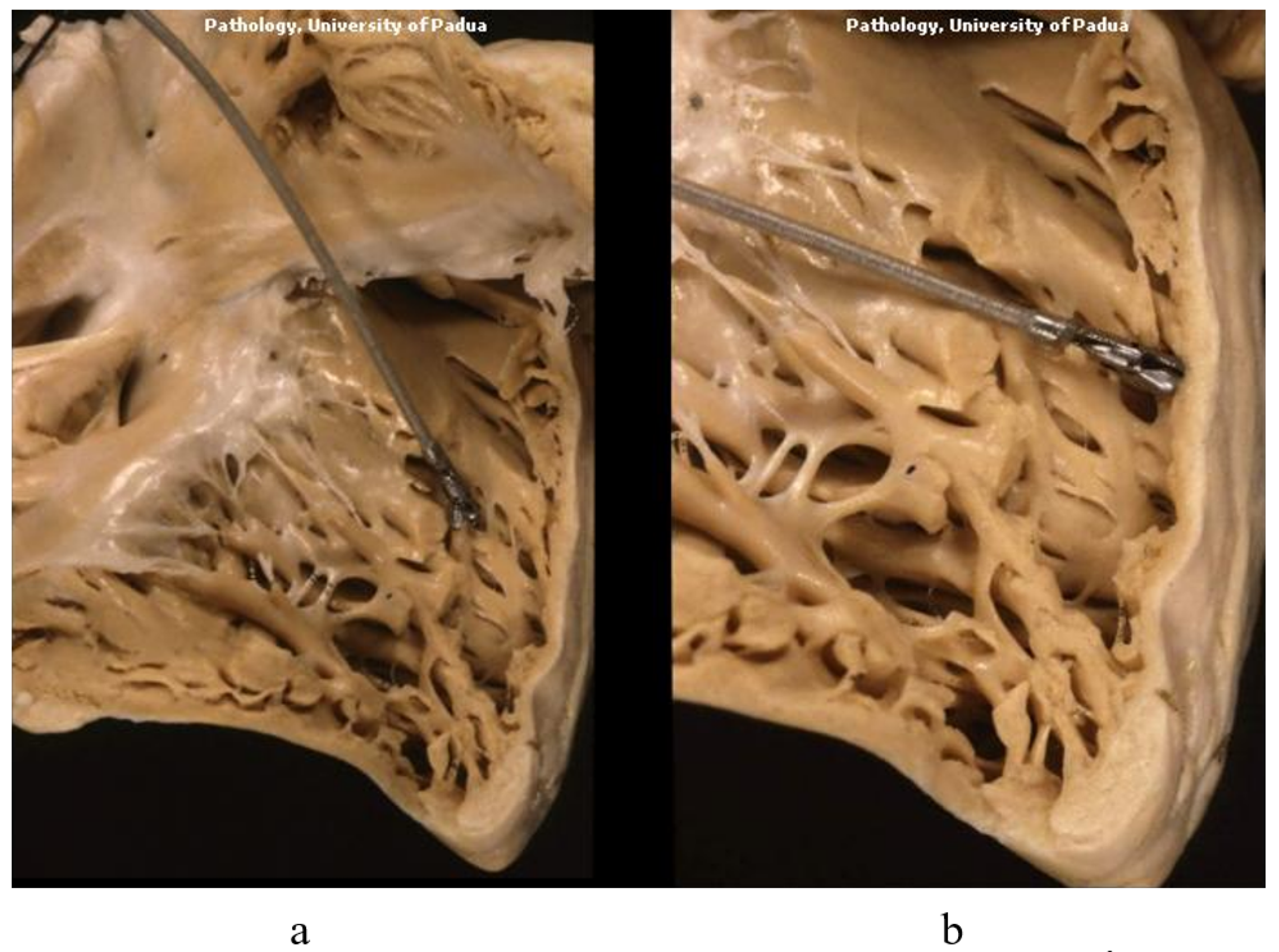
Figure 11.
Robert Hooke (1635–1703) invented the microscope in 1665, to make micrographia of minute bodies [8].
Figure 11.
Robert Hooke (1635–1703) invented the microscope in 1665, to make micrographia of minute bodies [8].

Figure 12.
Rejection of the heart. (a) T lymphocytes within the blood circulation. (b) Myocardium infiltrated with T lymphocytes.
Figure 12.
Rejection of the heart. (a) T lymphocytes within the blood circulation. (b) Myocardium infiltrated with T lymphocytes.
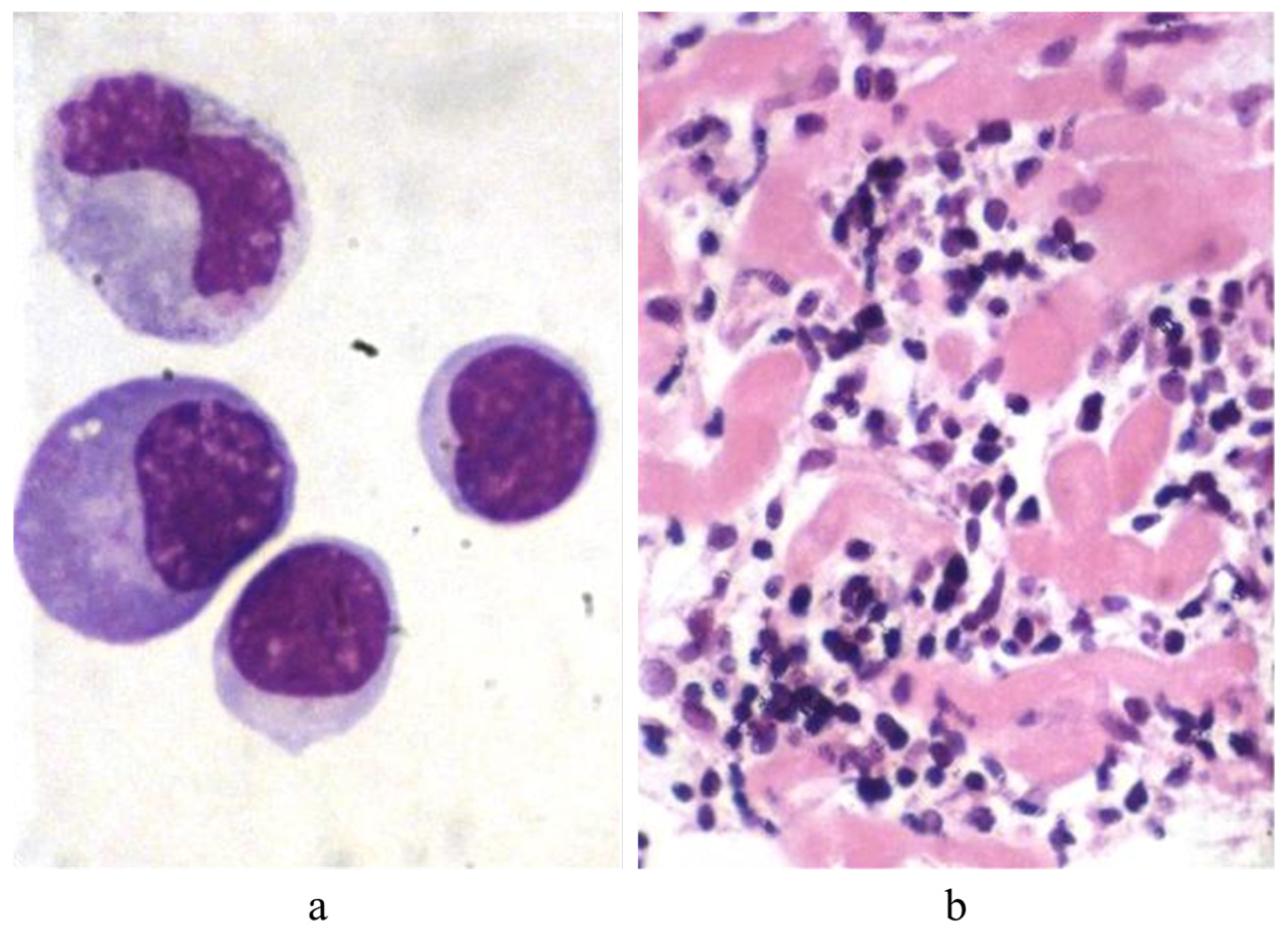
Figure 13.
In 1970, Margaret Billingham (a) (1930–2009) invents EMB through the jugular vein for monitoring cardiac rejection; (b) a transjugular venous approach.
Figure 13.
In 1970, Margaret Billingham (a) (1930–2009) invents EMB through the jugular vein for monitoring cardiac rejection; (b) a transjugular venous approach.

Figure 14.
EMB of a mass at RV grove (a). Immunohistochemistry revealed the mass to be an angiosarcoma (b–d) [10].
Figure 14.
EMB of a mass at RV grove (a). Immunohistochemistry revealed the mass to be an angiosarcoma (b–d) [10].
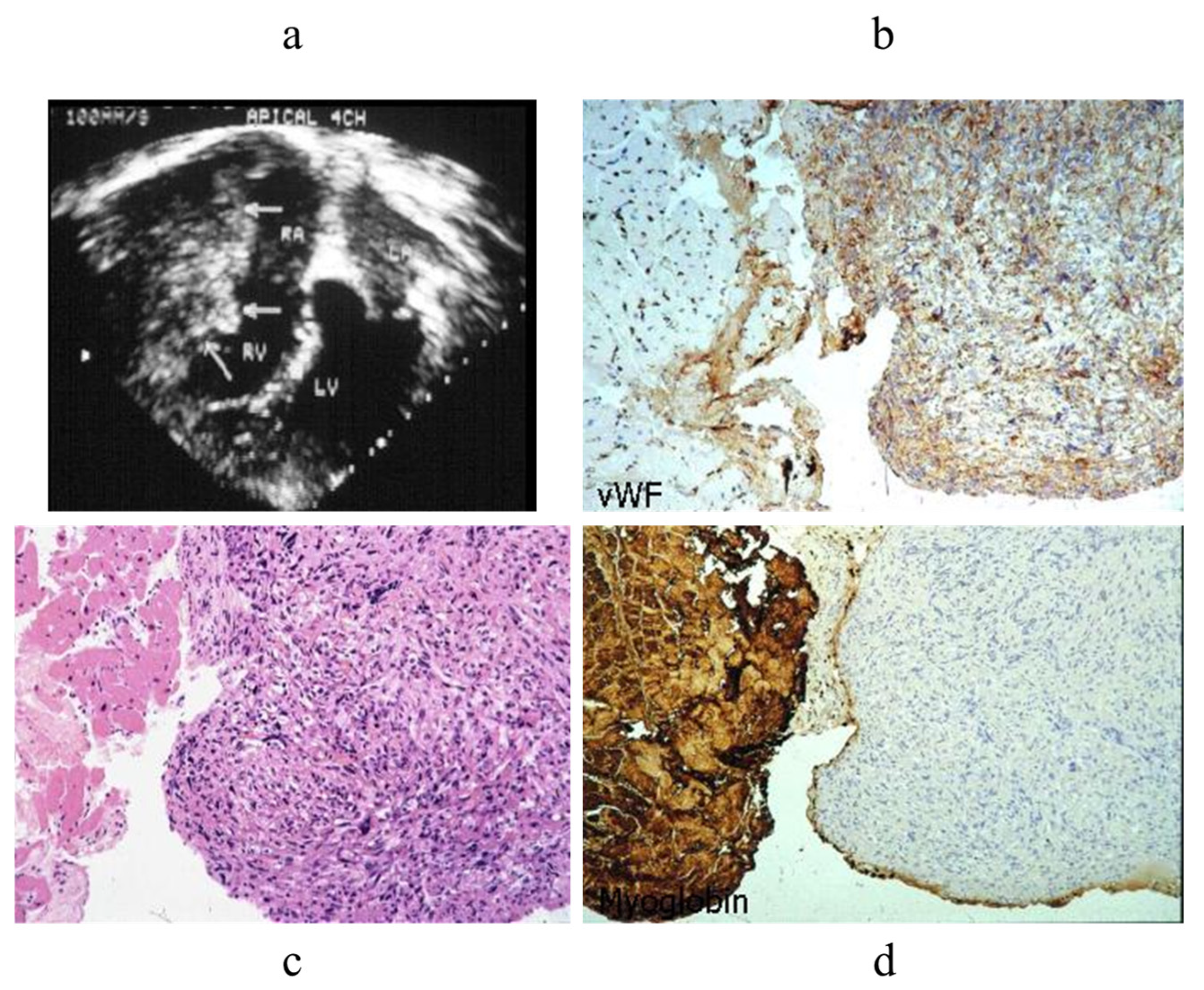
Figure 15.
EMB of an atrial lymphoma diagnosed by immunohistochemistry [11].
Figure 15.
EMB of an atrial lymphoma diagnosed by immunohistochemistry [11].
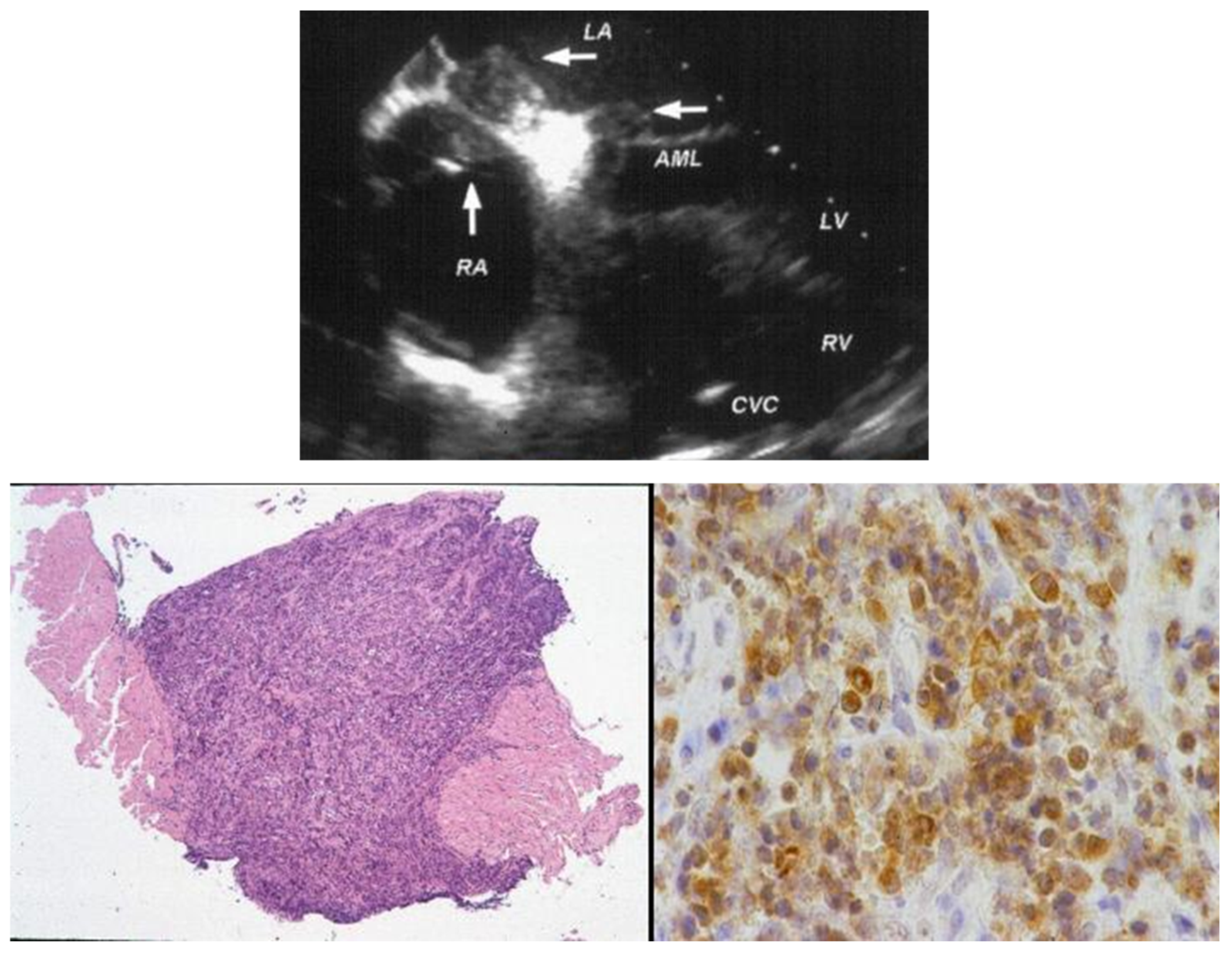
Figure 16.
EMB of a cardiac fibrosarcoma diagnosed by immunohistochemistry [12].
Figure 16.
EMB of a cardiac fibrosarcoma diagnosed by immunohistochemistry [12].
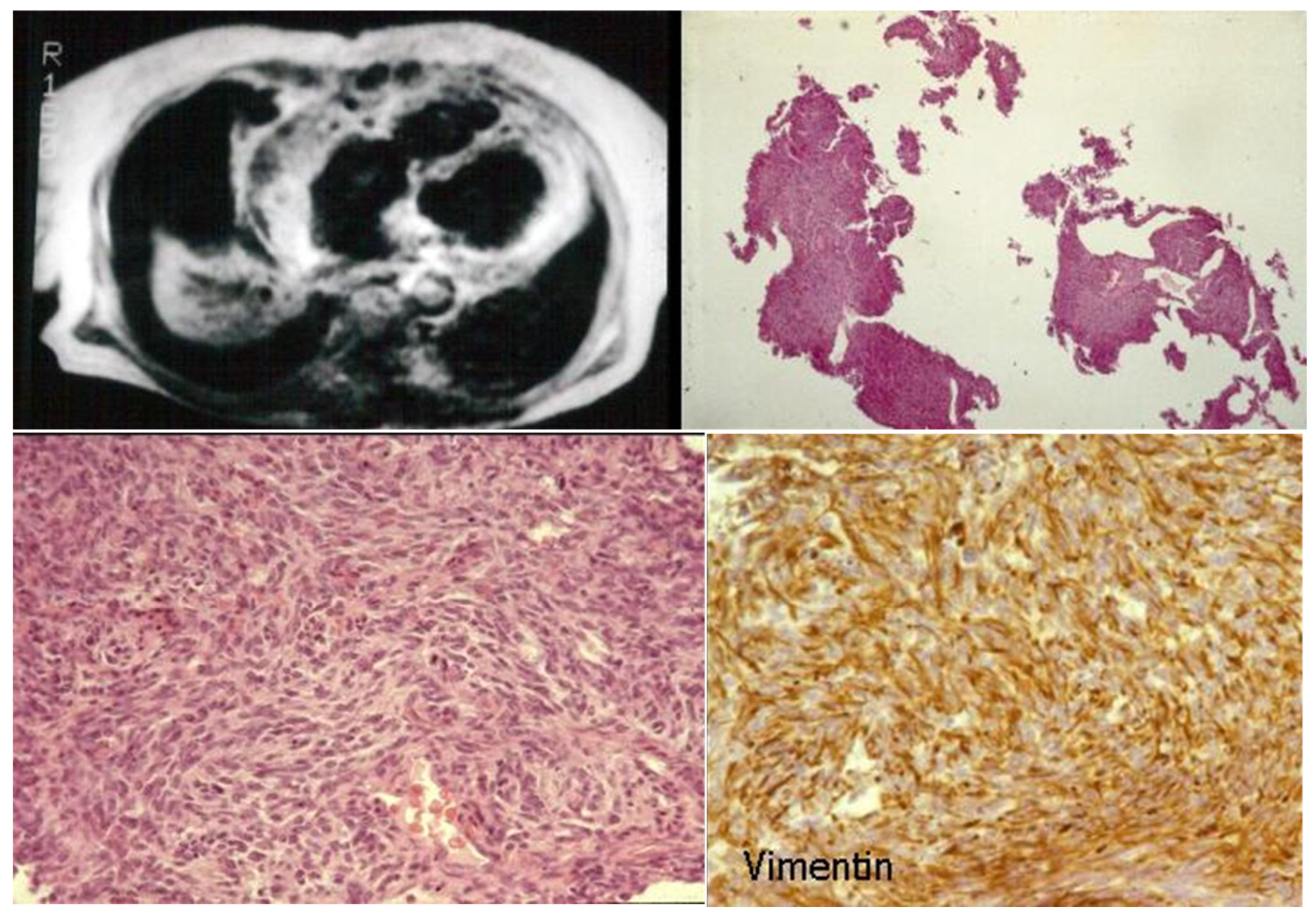
Figure 17.
EMB in obliterative cardiomyopathy of Loeffler disease (a–c) with eosinophil infiltrates (d) [13].
Figure 17.
EMB in obliterative cardiomyopathy of Loeffler disease (a–c) with eosinophil infiltrates (d) [13].
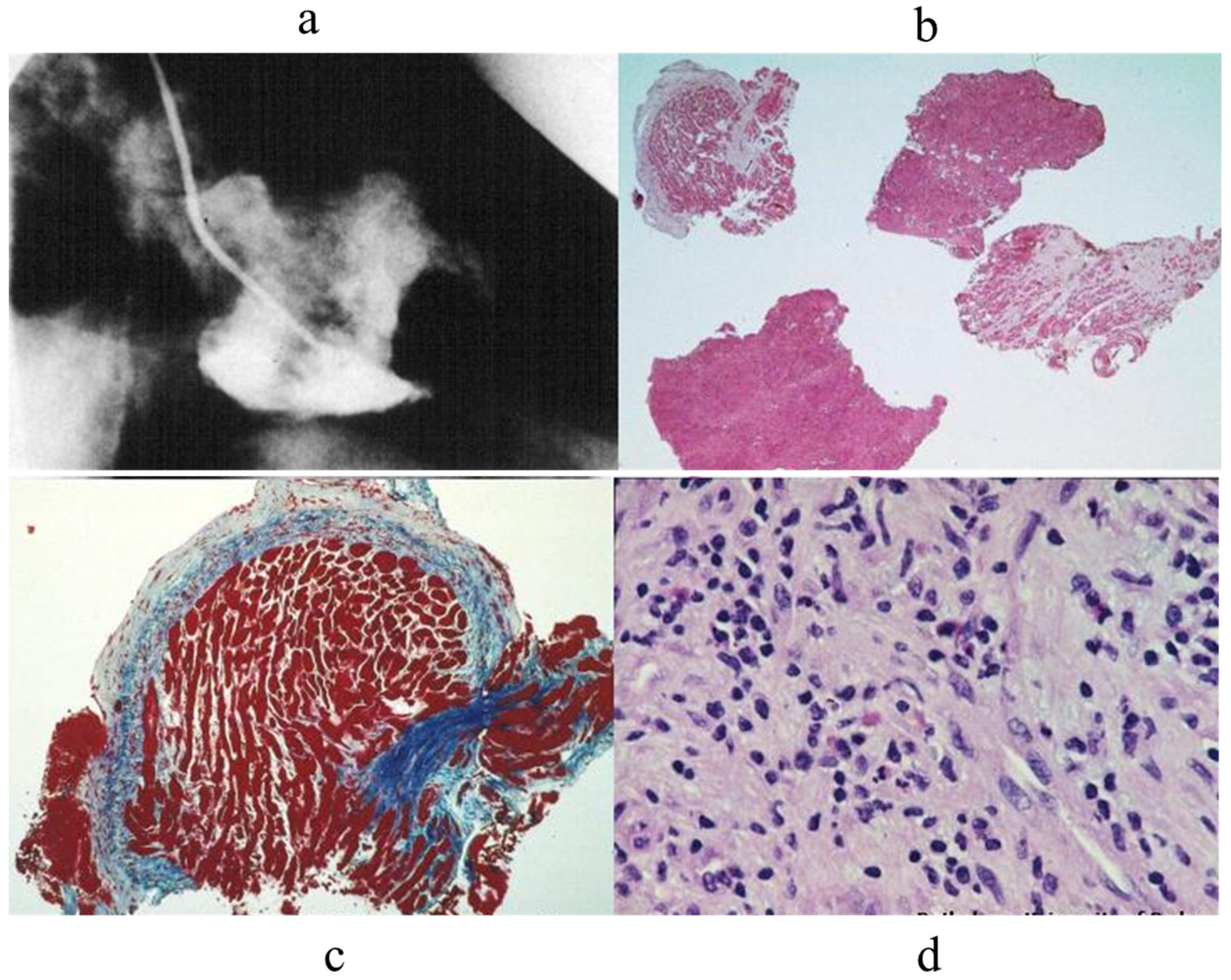
Figure 18.
Multiple histotypes of myocarditis: lymphocyte, neutrophil, eosinophil, and giant cells [14,15].
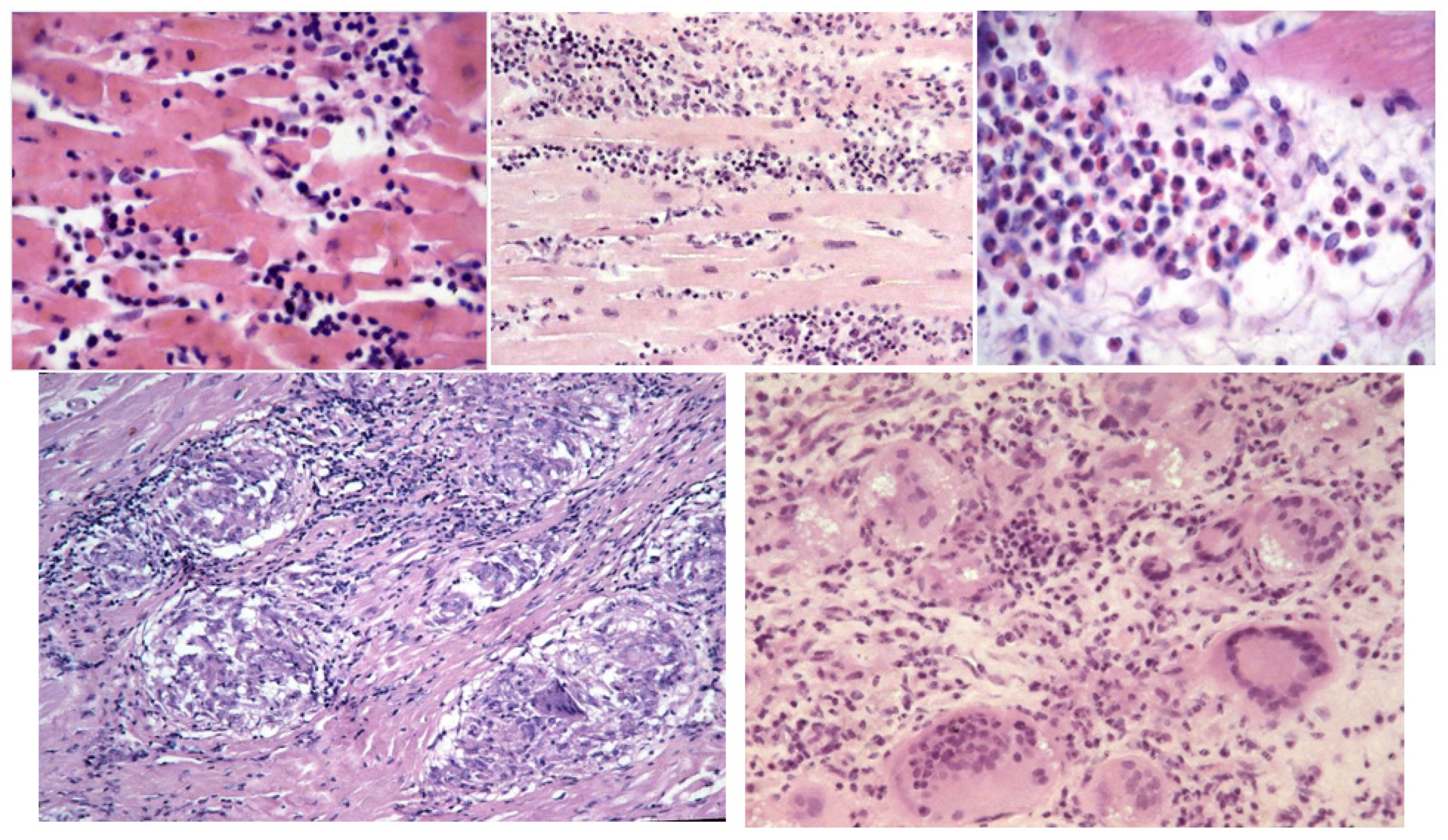
Figure 19.
In 1983, Kary Mullis (a) invents the polymerase chain reaction (PCR) (b) [16].
Figure 19.
In 1983, Kary Mullis (a) invents the polymerase chain reaction (PCR) (b) [16].
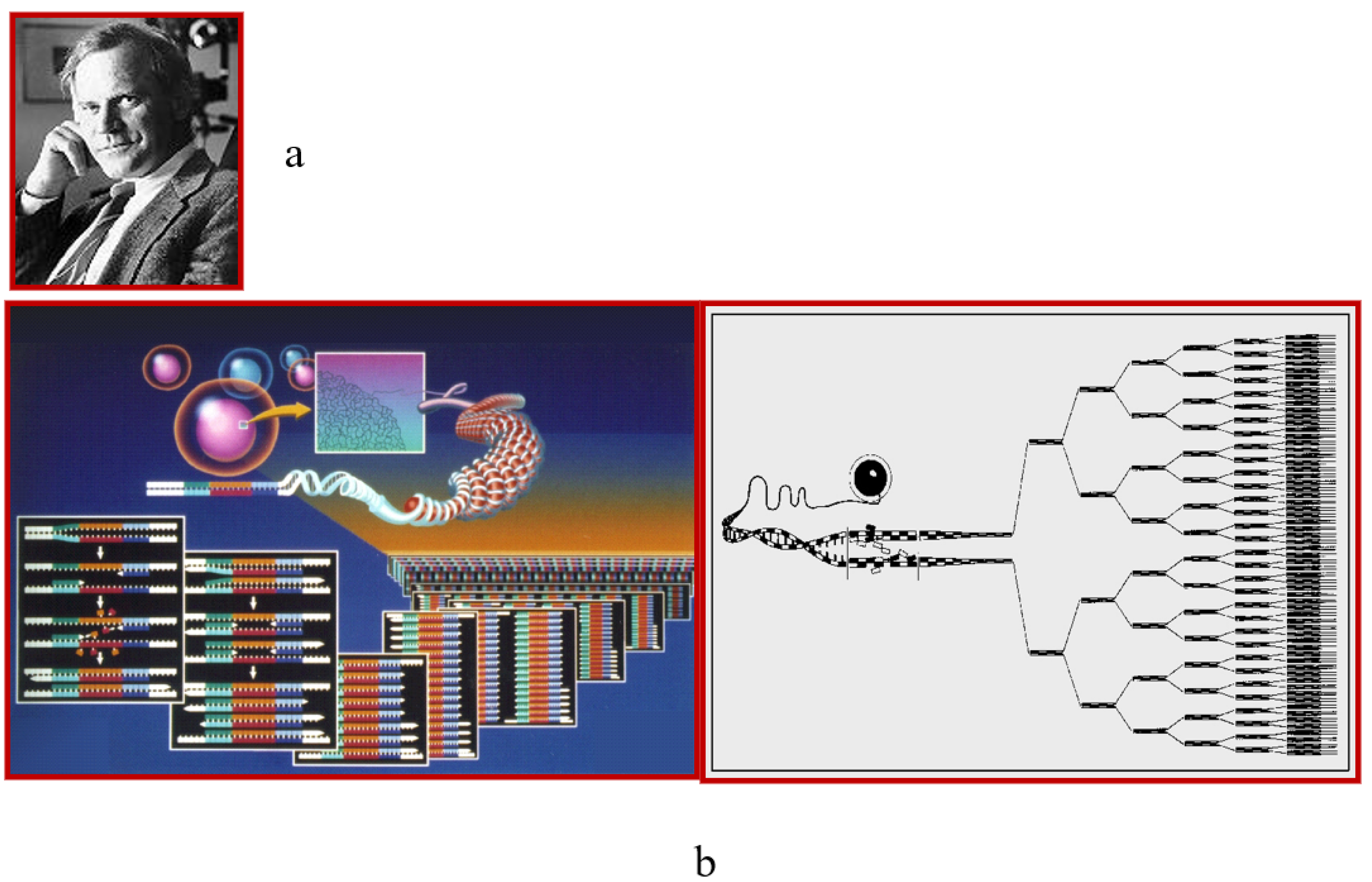
Figure 20.
Viral PCR-proven myocarditis both in children (a) and adults (b) [17].
Figure 20.
Viral PCR-proven myocarditis both in children (a) and adults (b) [17].
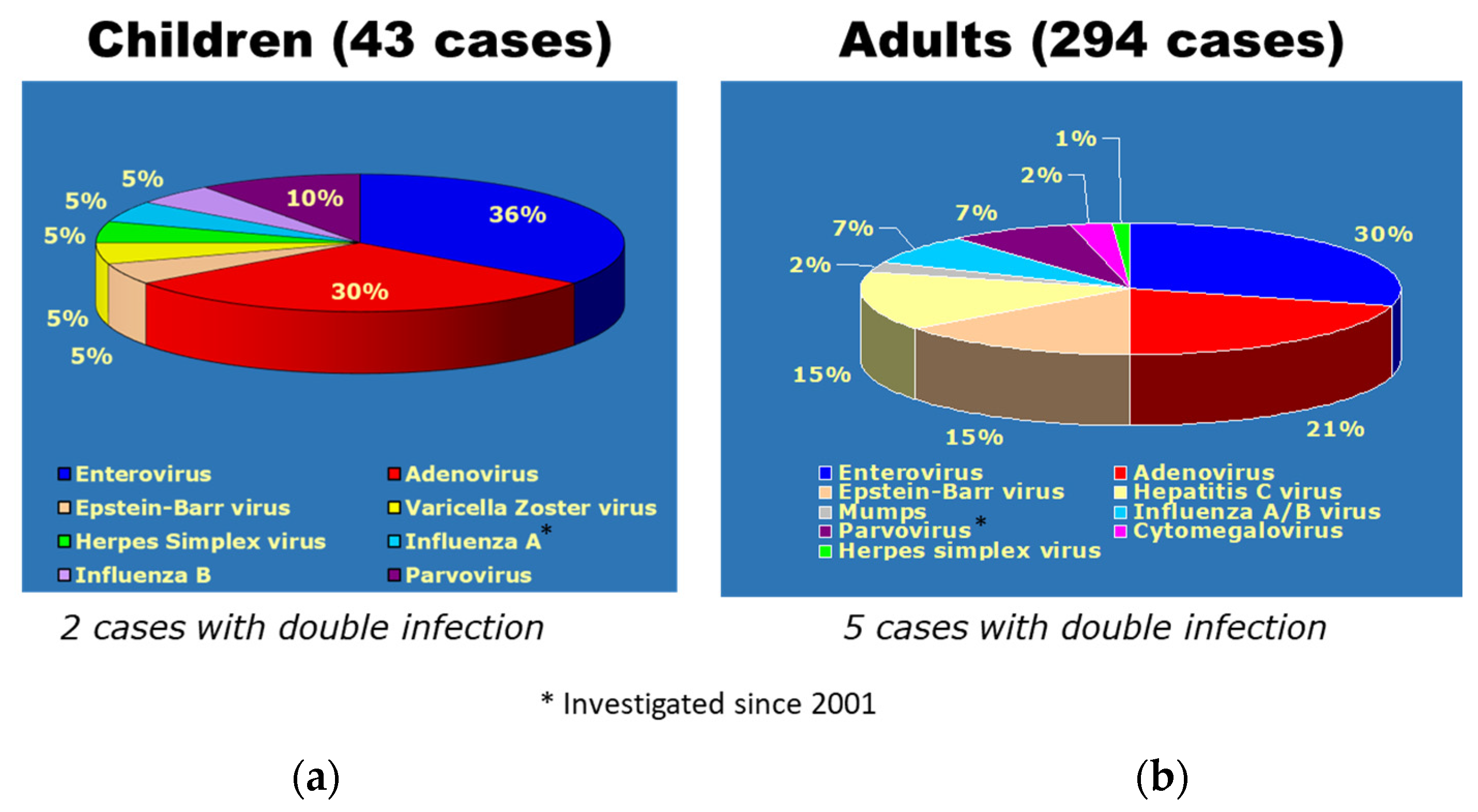
Figure 21.
EMB in ACM. (a) Electroanatomic mapping with electric scar; (b) fibroadiposis (Azan Mallory stain); (c) ventricular tachycardia.
Figure 21.
EMB in ACM. (a) Electroanatomic mapping with electric scar; (b) fibroadiposis (Azan Mallory stain); (c) ventricular tachycardia.
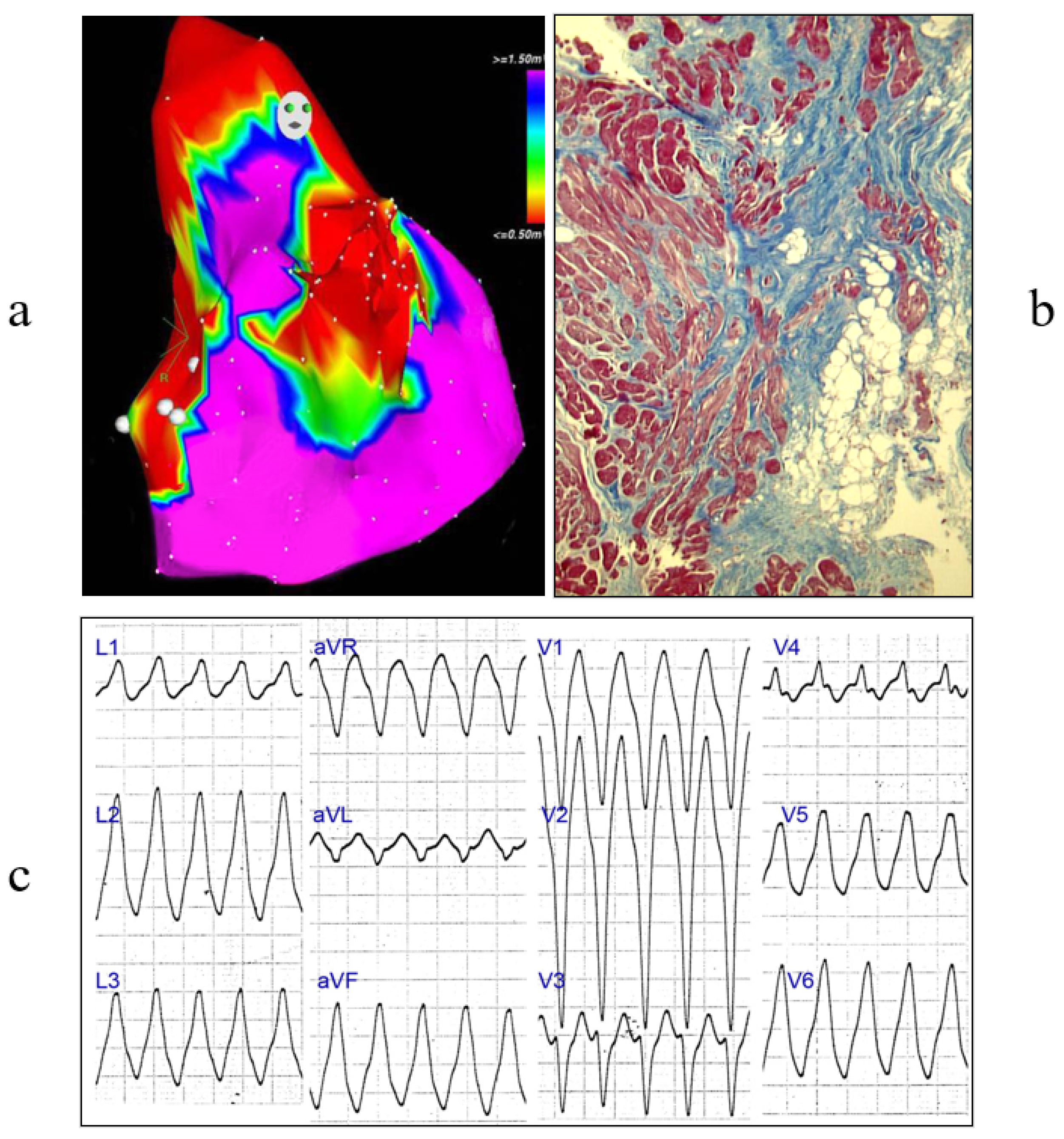
Figure 22.
EMB in ACM with in vitro investigation of specimens at autopsy. Right ventricle with fibroadiposis of the free wall (A,B). The catheter with the bioptome simulating endomyocardial biopsy (C). Other pictures of the right ventricle and the catheter with the bioptome (D,E).
Figure 22.
EMB in ACM with in vitro investigation of specimens at autopsy. Right ventricle with fibroadiposis of the free wall (A,B). The catheter with the bioptome simulating endomyocardial biopsy (C). Other pictures of the right ventricle and the catheter with the bioptome (D,E).
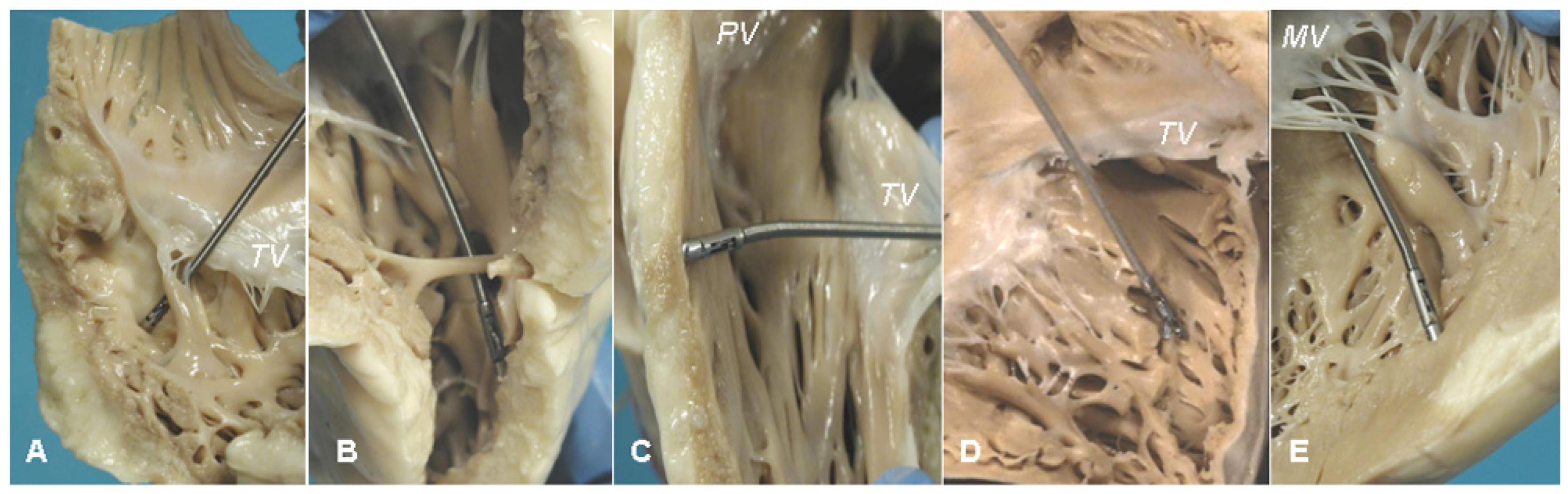
Figure 23.
Specificity (90%) and sensitivity (80%) of the residual myocardium (<59%) in the diagnosis of arrhythmogenic cardiomyopathy [19].
Figure 23.
Specificity (90%) and sensitivity (80%) of the residual myocardium (<59%) in the diagnosis of arrhythmogenic cardiomyopathy [19].
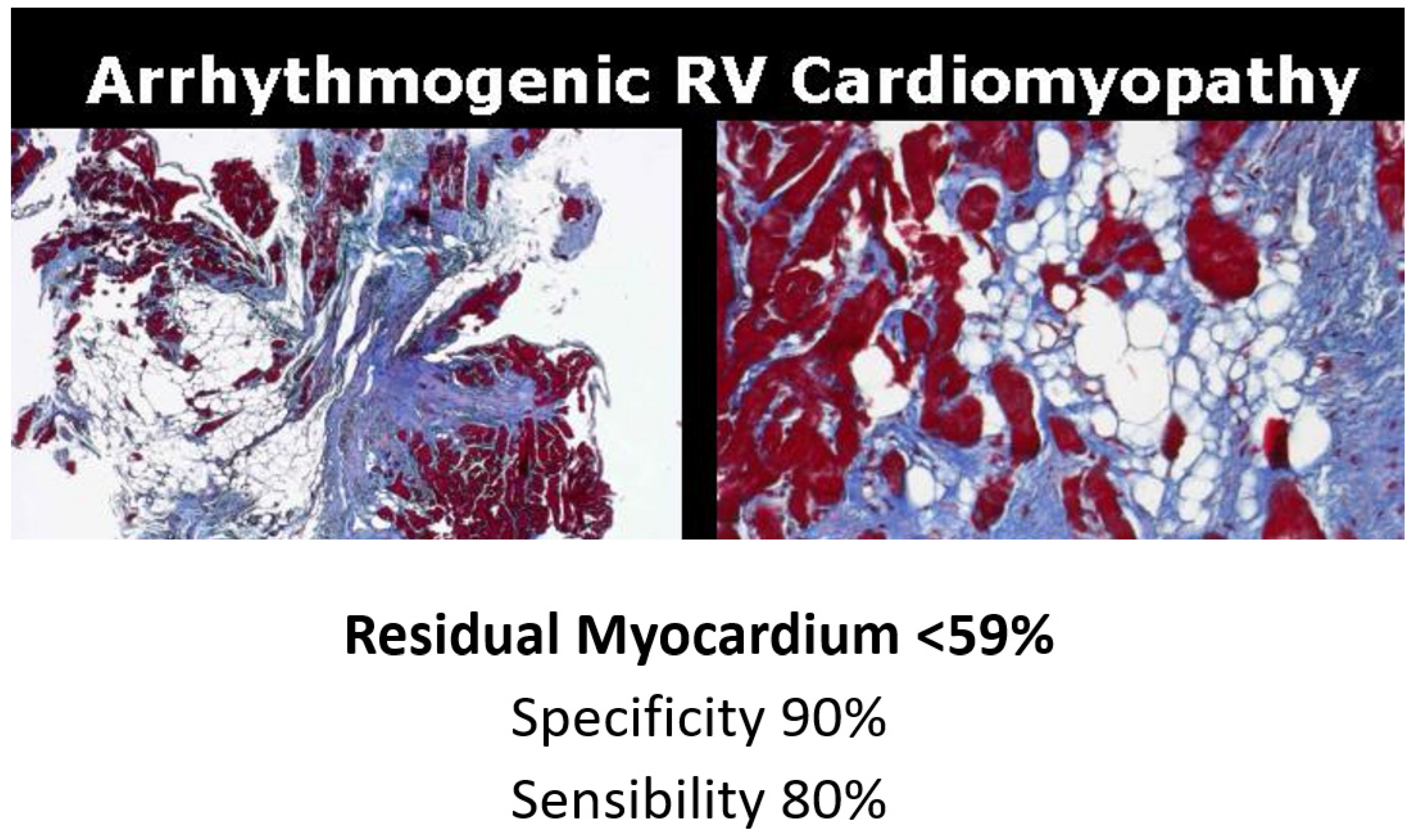
Figure 24.
Diagnosis of amyloidosis by EMB as infiltrative diseases of the myocardial interstitium with specific stems.
Figure 24.
Diagnosis of amyloidosis by EMB as infiltrative diseases of the myocardial interstitium with specific stems.
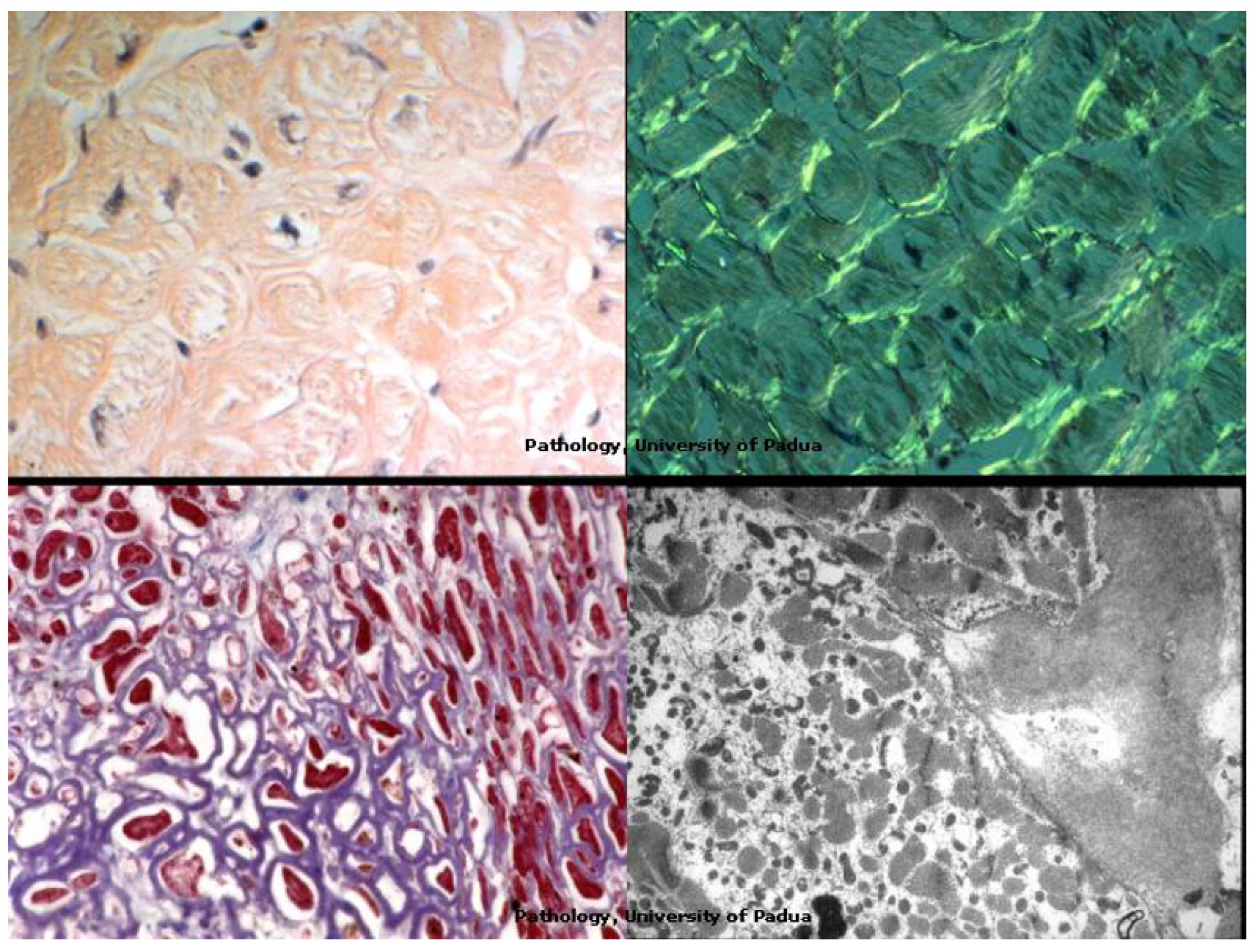
Figure 25.
Fabry disease: a secondary hypertrophic cardiomyopathy diagnosed by electron microscopy.
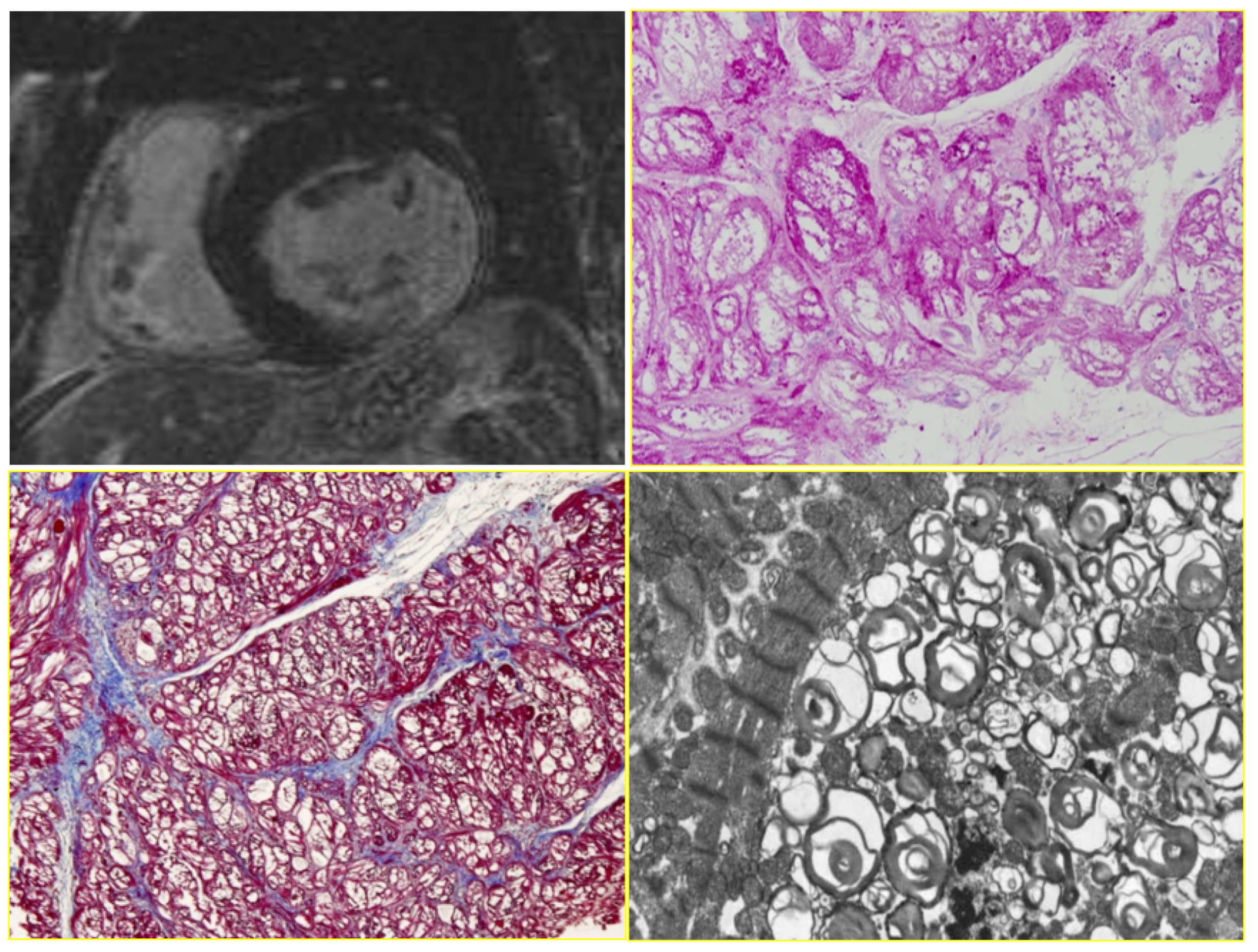
Figure 26.
Electron microscopy of myocardial apoptosis in ACM. Original magnification, ×14,500.

Figure 27.
Electron microscopy in ACM. Transmission electron microscopy shows a disrupted intercalated disc (b) compared to normal desmosome (a). Original magnification, (a) ×30,000; (b) ×50,000. Rectangular block includes a normal desmosome (a), whereas the arrow indicates disrupted desmosomes in AC (b).
Figure 27.
Electron microscopy in ACM. Transmission electron microscopy shows a disrupted intercalated disc (b) compared to normal desmosome (a). Original magnification, (a) ×30,000; (b) ×50,000. Rectangular block includes a normal desmosome (a), whereas the arrow indicates disrupted desmosomes in AC (b).
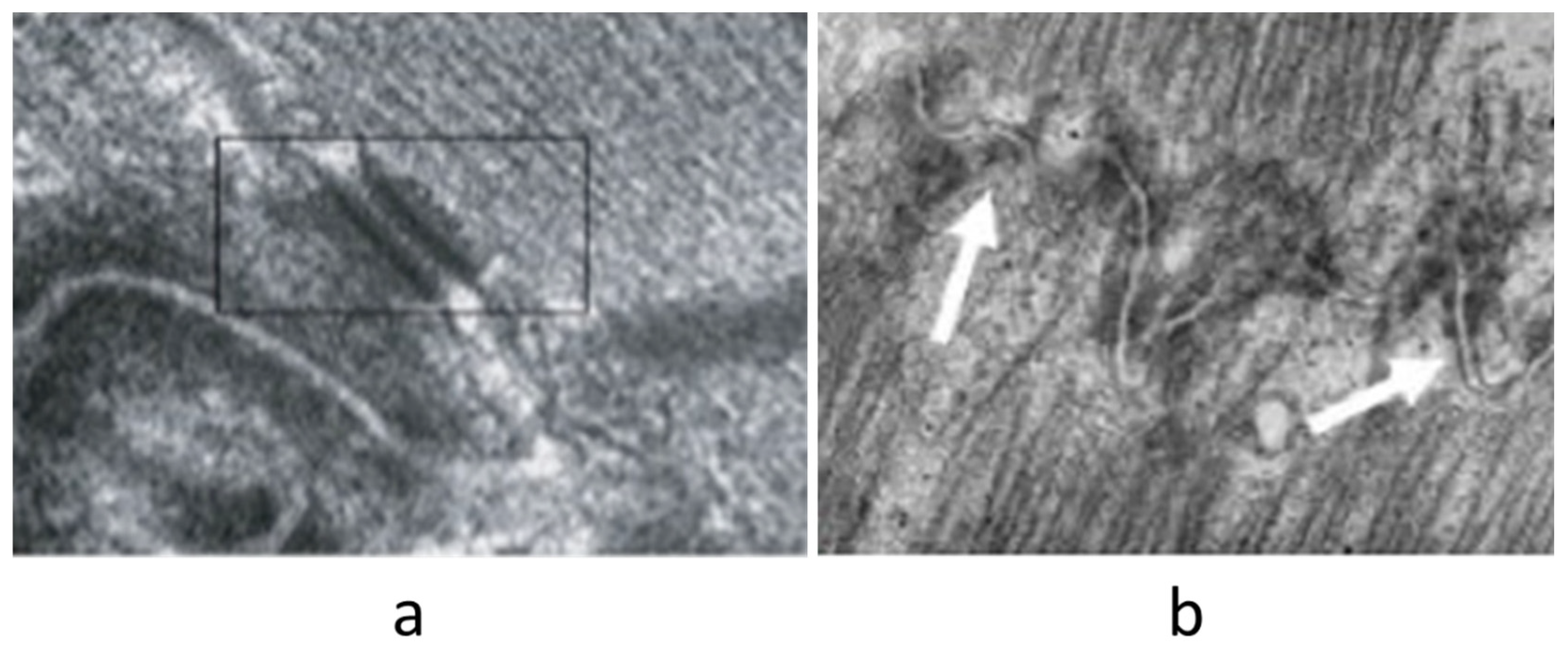
Figure 28.
Dallas Criteria. Active myocarditis was possible to detect in vivo by EMB and diagnostic histologic criteria were put forward in Dallas by the Society for Cardiovascular Pathology in 1985, based upon microscopic observation of inflammatory infiltrates associated with myocardial death (“Dallas Criteria”). (a) Active myocarditis. Inflammatory cellular infiltrate with evidence of myocyte necrosis. (b) Borderline myocarditis. Inflammatory cellular infiltration without evidence of myocyte injury. Hematoxylin–Eosin staining was used [20].
Figure 28.
Dallas Criteria. Active myocarditis was possible to detect in vivo by EMB and diagnostic histologic criteria were put forward in Dallas by the Society for Cardiovascular Pathology in 1985, based upon microscopic observation of inflammatory infiltrates associated with myocardial death (“Dallas Criteria”). (a) Active myocarditis. Inflammatory cellular infiltrate with evidence of myocyte necrosis. (b) Borderline myocarditis. Inflammatory cellular infiltration without evidence of myocyte injury. Hematoxylin–Eosin staining was used [20].
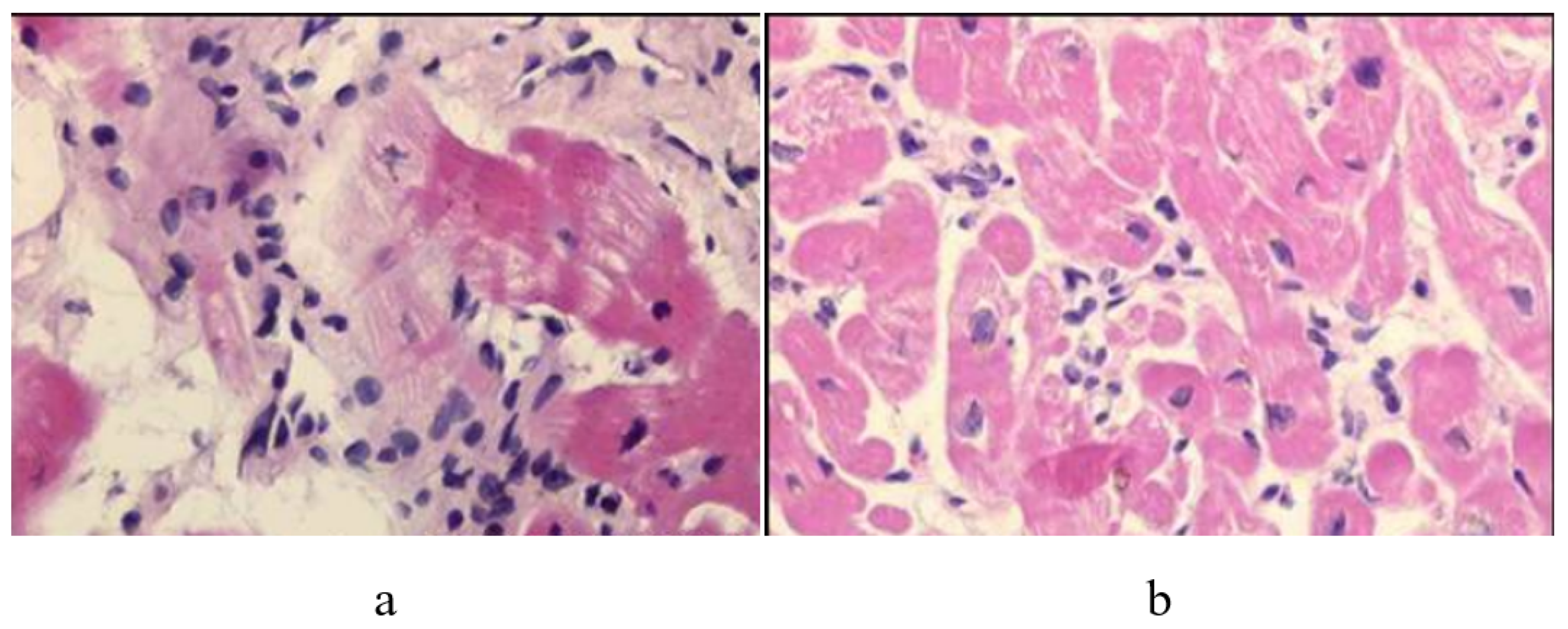
Figure 29.
Lymphocytic myocarditis with inflammatory infiltrate and the oedematous interstitium, without cardiomyocytes necrosis.
Figure 29.
Lymphocytic myocarditis with inflammatory infiltrate and the oedematous interstitium, without cardiomyocytes necrosis.
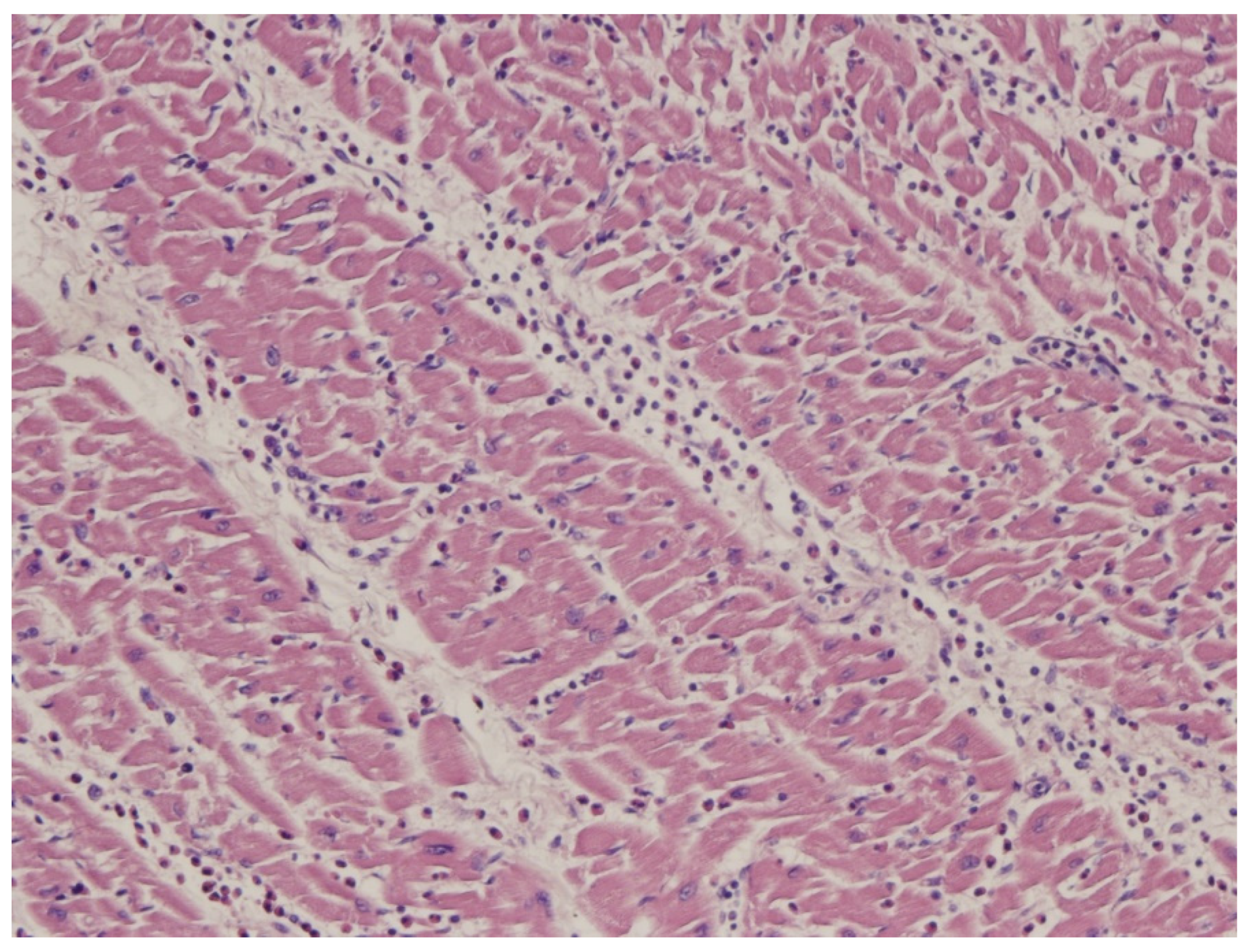
Figure 30.
Robert Bartlett (1939-) (b) developed the tool (a) of extracorporeal membrane oxygenation (ECMO) [22].
Figure 30.
Robert Bartlett (1939-) (b) developed the tool (a) of extracorporeal membrane oxygenation (ECMO) [22].

Figure 31.
Contractile recovery and rate of survival achieved when employing ECMO in fulminant myocarditis (both in children and adults) [23,24,25,26].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Questioning the utility of EMB [9].
Table 1.
Questioning the utility of EMB [9].
|
|
|
Table 2.
Indications for EMB.
|
|
|
|
|
Table 3.
Inflammatory cardiomyopathy. Endomyocardial biopsy [18].
Table 3.
Inflammatory cardiomyopathy. Endomyocardial biopsy [18].
| Molecular Analysis | Histology | Immunohistochemistry |
|---|---|---|
| ↘ | ↓ | ↙ |
| Gold Standard |
Table 4.
EMB sampling.
|
|
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Thiene, G. Storytelling of Myocardial Biopsy. Biology 2025, 14, 306. https://doi.org/10.3390/biology14030306
AMA Style
Thiene G. Storytelling of Myocardial Biopsy. Biology. 2025; 14(3):306. https://doi.org/10.3390/biology14030306
Chicago/Turabian StyleThiene, Gaetano. 2025. "Storytelling of Myocardial Biopsy" Biology 14, no. 3: 306. https://doi.org/10.3390/biology14030306
APA StyleThiene, G. (2025). Storytelling of Myocardial Biopsy. Biology, 14(3), 306. https://doi.org/10.3390/biology14030306
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.