
Dietary Patterns and Fertility
 ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Mediterranean Diet
2.1. Typical Foods of Mediterranean Diet
2.1.1. Fats
2.1.2. Carbohydrates
2.1.3. Proteins
2.1.4. Micronutrients
2.1.5. Fruit and Vegetables
3. Western Diet
3.1. Typical Foods of the Western Diet
3.1.1. Fats
3.1.2. Carbohydrates
3.1.3. Proteins
4. Arabic Middle Eastern diet
5. Asian Diet
6. Other Dietary Patterns
6.1. Vegetarian and Vegan Diet
6.2. Ketogenic Diet
7. Conclusions
8. Take Home Message
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Infertility Workup for the Women’s Health Specialist: ACOG Committee Opinion, Number 781. Obstet. Gynecol. 2019, 133, e377–e384. [CrossRef]
- Chavarro, J.E.M.; Rich-Edwards, J.W.M.; Rosner, B.A.; Willett, W.C.M. Diet and lifestyle in the prevention of ovulatory disorder infertility. Obstet. Gynecol. 2007, 110, 1050–1058. [Google Scholar] [CrossRef] [PubMed]
- Cristodoro, M.; Dell’avanzo, M.; Ghio, M.; Lalatta, F.; Vena, W.; Lania, A.; Sacchi, L.; Bravo, M.; Bulfoni, A.; Di Simone, N.; et al. Before Is Better: Innovative Multidisciplinary Preconception Care in Different Clinical Contexts. J. Clin. Med. 2023, 12, 6352. [Google Scholar] [CrossRef] [PubMed]
- Panth, N.; Gavarkovs, A.; Tamez, M.; Mattei, J. The Influence of Diet on Fertility and the Implications for Public Health Nutrition in the United States. Front. Public Health 2018, 6, 211. [Google Scholar] [CrossRef] [PubMed]
- Lal, L.; Bharti, A.; Perween, A. To study the status of LH: FSH ratio in obese and non-obese patients of polycystic ovarian syndrome. IOSR J. Dent. Med. Sci. 2017, 16, 20–23. [Google Scholar] [CrossRef]
- Saadia, Z. Follicle Stimulating Hormone (LH: FSH) Ratio in Polycystic Ovary Syndrome (PCOS)-Obese vs. Non-Obese Women. Med. Arch. 2020, 74, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Young, J.M.; McNeilly, A.S. Theca: The forgotten cell of the ovarian follicle. Reproduction 2010, 140, 489–504. [Google Scholar] [CrossRef]
- Nestler, J.E.; Jakubowicz, D.J.; de Vargas, A.F.; Brik, C.; Quintero, N.; Medina, F. Insulin stimulates testosterone biosynthesis by human thecal cells from women with polycystic ovary syndrome by activating its own receptor and using inositolglycan mediators as the signal transduction system. J. Clin. Endocrinol. Metab. 1998, 83, 2001–2005. [Google Scholar] [CrossRef]
- Fontana, R.; Della Torre, S. The Deep Correlation between Energy Metabolism and Reproduction: A View on the Effects of Nutrition for Women Fertility. Nutrients 2016, 8, 87. [Google Scholar] [CrossRef]
- Belani, M.; Purohit, N.; Pillai, P.; Gupta, S.; Gupta, S. Modulation of steroidogenic pathway in rat granulosa cells with subclinical Cd exposure and insulin resistance: An impact on female fertility. BioMed Res. Int. 2014, 2014, 460251. [Google Scholar] [CrossRef]
- Baer, D.J.; Judd, J.T.; Clevidence, B.A.; Tracy, R.P. Dietary fatty acids affect plasma markers of inflammation in healthy men fed controlled diets: A randomized crossover study. Am. J. Clin. Nutr. 2004, 79, 969–973. [Google Scholar] [CrossRef] [PubMed]
- Wise, L.A.; Wesselink, A.K.; Tucker, K.L.; Saklani, S.; Mikkelsen, E.M.; Cueto, H.; Riis, A.H.; Trolle, E.; McKinnon, C.J.; Hahn, K.A.; et al. Dietary Fat Intake and Fecundability in 2 Preconception Cohort Studies. Am. J. Epidemiol. 2017, 187, 60–74. [Google Scholar] [CrossRef] [PubMed]
- Chavarro, J.E.; Rich-Edwards, J.W.; Rosner, B.A.; Willett, W.C. Dietary fatty acid intakes and the risk of ovulatory infertility. Am. J. Clin. Nutr. 2007, 85, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Moran, L.J.; Tsagareli, V.; Noakes, M.; Norman, R. Altered Preconception Fatty Acid Intake Is Associated with Improved Pregnancy Rates in Overweight and Obese Women Undertaking in Vitro Fertilisation. Nutrients 2016, 8, 10. [Google Scholar] [CrossRef]
- Mumford, S.L.; Browne, R.W.; Kim, K.; Nichols, C.; Wilcox, B.; Silver, R.M.; Connell, M.T.; Holland, T.L.; Kuhr, D.L.; Omosigho, U.R.; et al. Preconception Plasma Phospholipid Fatty Acids and Fecundability. J. Clin. Endocrinol. Metab. 2018, 103, 4501–4510. [Google Scholar] [CrossRef]
- Chiu, Y.H.; Karmon, A.E.; Gaskins, A.J.; Arvizu, M.; Williams, P.L.; Souter, I.; Rueda, B.R.; Hauser, R.; Chavarro, J.E.; EARTH Study Team. Serum omega-3 fatty acids and treatment outcomes among women undergoing assisted reproduction. Hum. Reprod. 2017, 33, 156–165. [Google Scholar] [CrossRef]
- Lanzone, A.; Fulghesu, A.; Fortini, A.; Cutillo, G.; Cucinelli, F.; Simone, N.; Caruso, A.; Mancuso, S. Effect of opiate receptor blockade on the insulin response to oral glucose load in polycystic ovarian disease. Hum. Reprod. 1991, 6, 1043–1049. [Google Scholar] [CrossRef]
- Guarano, A.; Capozzi, A.; Cristodoro, M.; Di Simone, N.; Lello, S. Alpha Lipoic Acid Efficacy in PCOS Treatment: What Is the Truth? Nutrients 2023, 15, 3209. [Google Scholar] [CrossRef]
- Chavarro, J.E.; Rich-Edwards, J.W.; Rosner, B.A.; Willett, W.C. Protein intake and ovulatory infertility. Am. J. Obstet. Gynecol. 2008, 198, 210.e1–210.e7. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.A.; Hickey, M. Reproduction in a changing world. Fertil. Steril. 2022, 120 Pt 1, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.H.; Raftery, A.E. How Do Education and Family Planning Accelerate Fertility Decline? Popul. Dev. Rev. 2020, 46, 409–441. [Google Scholar] [CrossRef] [PubMed]
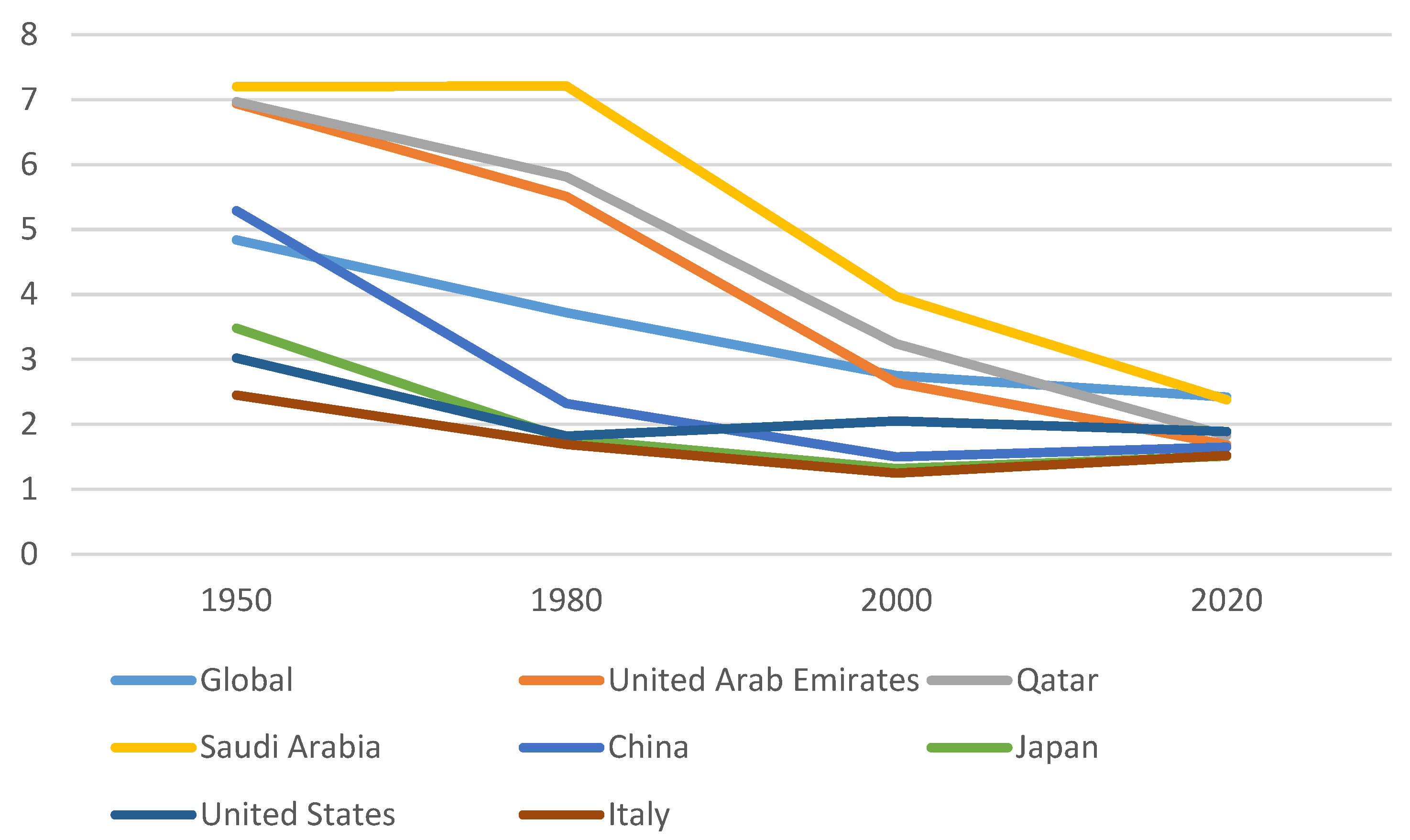
- Fertility Rate: Children per Woman—Gapminder. In Gapminder (2017)—With Minor Processing by Our World in Data. Available online: https://ourworldindata.org/grapher/children-born-per-woman (accessed on 14 January 2024).
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; A Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [PubMed]
- Keys, A.; Mienotti, A.; Karvonen, M.J.; Aravanis, C.; Blackburn, H.; Buzina, R.; Djordjevic, B.S.; Dontas, A.S.; Fidanza, F.; Keys, M.H.; et al. The diet and 15-year death rate in the seven countries study. Am. J. Epidemiol. 1986, 124, 903–915. [Google Scholar] [CrossRef]
- Rosato, V.; Temple, N.J.; La Vecchia, C.; Castellan, G.; Tavani, A.; Guercio, V. Mediterranean diet and cardiovascular disease: A systematic review and meta-analysis of observational studies. Eur. J. Nutr. 2017, 58, 173–191. [Google Scholar] [CrossRef]
- Gaskins, A.J.; Nassan, F.L.; Chiu, Y.-H.; Arvizu, M.; Williams, P.L.; Keller, M.G.; Souter, I.; Hauser, R.; Chavarro, J.E.; EARTH Study Team. Dietary patterns and outcomes of assisted reproduction. Am. J. Obstet. Gynecol. 2019, 220, 567.e1–567.e18. [Google Scholar] [CrossRef]
- Sun, H.; Lin, Y.; Lin, D.; Zou, C.; Zou, X.; Fu, L.; Meng, F.; Qian, W. Mediterranean diet improves embryo yield in IVF: A prospective cohort study. Reprod. Biol. Endocrinol. 2019, 17, 73. [Google Scholar] [CrossRef]
- Vujkovic, M.; de Vries, J.H.; Lindemans, J.; Macklon, N.S.; van der Spek, P.J.; Steegers, E.A.; Steegers-Theunissen, R.P. The preconception Mediterranean dietary pattern in couples undergoing in vitro fertilization/intracytoplasmic sperm injection treatment increases the chance of pregnancy. Fertil. Steril. 2010, 94, 2096–2101. [Google Scholar] [CrossRef]
- Yang, J.; Song, Y.; Gaskins, A.J.; Li, L.-J.; Huang, Z.; Eriksson, J.G.; Hu, F.B.; Chong, Y.S.; Zhang, C. Mediterranean diet and female reproductive health over lifespan: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2023, 229, 617–631. [Google Scholar] [CrossRef]
- Salas-Huetos, A.; Mitsunami, M.; Wang, S.; Mínguez-Alarcón, L.; Ribas-Maynou, J.; Yeste, M.; Souter, I.; Chavarro, J.E.; EARTH Study Team; Hauser, R.; et al. Women’s Adherence to Healthy Dietary Patterns and Outcomes of Infertility Treatment. JAMA Netw. Open 2023, 6, e2329982. [Google Scholar] [CrossRef]
- Toledo, E.; Lopez-Del Burgo, C.; Ruiz-Zambrana, A.; Donazar, M.; Navarro-Blasco, I.; Martinez-Gonzalez, M.A.; DE Irala, J. Dietary patterns and difficulty conceiving: A nested case–control study. Fertil. Steril. 2011, 96, 1149–1153. [Google Scholar] [CrossRef] [PubMed]
- Su, P.-Y.; Cao, L.-L.; Chang, J.-J.; Wang, S.-J.; Li, Y.-H.; Yuan, M.-Y.; Wang, G.-F. The effect of healthy dietary patterns on male semen quality: A systematic review and meta-analysis. Asian J. Androl. 2022, 24, 549–557. [Google Scholar] [CrossRef]
- Montano, L.; Ceretti, E.; Donato, F.; Bergamo, P.; Zani, C.; Viola, G.C.V.; Notari, T.; Pappalardo, S.; Zani, D.; Ubaldi, S.; et al. Effects of a Lifestyle Change Intervention on Semen Quality in Healthy Young Men Living in Highly Polluted Areas in Italy: The FASt Randomized Controlled Trial. Eur. Urol. Focus 2021, 8, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Petre, G.C.; Francini-Pesenti, F.; Di Nisio, A.; De Toni, L.; Grande, G.; Mingardi, A.; Cusmano, A.; Spinella, P.; Ferlin, A.; Garolla, A. Observational Cross-Sectional Study on Mediterranean Diet and Sperm Parameters. Nutrients 2023, 15, 4989. [Google Scholar] [CrossRef]
- Mantzioris, E.; Muhlhausler, B.S.; Villani, A. Impact of the Mediterranean Dietary pattern on n-3 fatty acid tissue levels–A systematic review. Prostaglandins Leukot. Essent. Fat. Acids 2021, 176, 102387. [Google Scholar] [CrossRef]
- Calder, P.C. Omega-3 fatty acids and inflammatory processes: From molecules to man. Biochem. Soc. Trans. 2017, 45, 1105–1115. [Google Scholar] [CrossRef]
- Molina, N.M.; Jurado-Fasoli, L.; Sola-Leyva, A.; Sevilla-Lorente, R.; Canha-Gouveia, A.; Ruiz-Durán, S.; Fontes, J.; Aguilera, C.M.; Altmäe, S. Endometrial whole metabolome profile at the receptive phase: Influence of Mediterranean Diet and infertility. Front. Endocrinol. 2023, 14, 1120988. [Google Scholar] [CrossRef]
- Hammiche, F.; Vujkovic, M.; Wijburg, W.; de Vries, J.H.; Macklon, N.S.; Laven, J.S.; Steegers-Theunissen, R.P. Increased preconception omega-3 polyunsaturated fatty acid intake improves embryo morphology. Fertil. Steril. 2011, 95, 1820–1823. [Google Scholar] [CrossRef] [PubMed]
- Falsig, A.-M.L.; Gleerup, C.S.; Knudsen, U.B. The influence of omega-3 fatty acids on semen quality markers: A systematic PRISMA review. Andrology. 2019, 7, 794–803. [Google Scholar] [CrossRef] [PubMed]
- Collodel, G.; Moretti, E.; Noto, D.; Corsaro, R.; Signorini, C. Oxidation of Polyunsaturated Fatty Acids as a Promising Area of Research in Infertility. Antioxidants 2022, 11, 1002. [Google Scholar] [CrossRef]
- Kermack, A.J.; Lowen, P.; Wellstead, S.J.; Fisk, H.L.; Montag, M.; Cheong, Y.; Osmond, C.; Houghton, F.D.; Calder, P.C.; Macklon, N.S. Effect of a 6-week “Mediterranean” dietary intervention on in vitro human embryo development: The Preconception Dietary Supplements in Assisted Reproduction double-blinded randomized controlled trial. Fertil. Steril. 2020, 113, 260–269. [Google Scholar] [CrossRef]
- Gaskins, A.J.; Chiu, Y.-H.; Williams, P.L.; Keller, M.G.; Toth, T.L.; Hauser, R.; Chavarro, J.E.; EARTH Study Team. Maternal whole grain intake and outcomes of in vitro fertilization. Fertil. Steril. 2016, 105, 1503–1510.e4. [Google Scholar] [CrossRef]
- Noli, S.A.; Ricci, E.; Cipriani, S.; Ferrari, S.; Castiglioni, M.; La Vecchia, I.; Somigliana, E.; Parazzini, F. Dietary Carbohydrate Intake, Dietary Glycemic Load and Outcomes of In Vitro Fertilization: Findings from an Observational Italian Cohort Study. Nutrients 2020, 12, 1568. [Google Scholar] [CrossRef]
- Corsetti, V.; Notari, T.; Montano, L. Effects of the low-carb organic Mediterranean diet on testosterone levels and sperm DNA fragmentation. Curr. Res. Food Sci. 2023, 7, 100636. [Google Scholar] [CrossRef]
- Skoracka, K.; Ratajczak, A.E.; Rychter, A.M.; Dobrowolska, A.; Krela-Kaźmierczak, I. Female Fertility and the Nutritional Approach: The Most Essential Aspects. Adv. Nutr. Int. Rev. J. 2021, 12, 2372–2386. [Google Scholar] [CrossRef]
- Nassan, F.L.; Chiu, Y.-H.; Vanegas, J.C.; Gaskins, A.J.; Williams, P.L.; Ford, J.B.; Attaman, J.; Hauser, R.; Chavarro, J.E. EARTH Study Team. Intake of protein-rich foods in relation to outcomes of infertility treatment with assisted reproductive technologies. Am. J. Clin. Nutr. 2018, 108, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Braga, D.P.A.F.; Halpern, G.; Setti, A.S.; Figueira, R.C.S.; Iaconelli, A.; Borges, E. The impact of food intake and social habits on embryo quality and the likelihood of blastocyst formation. Reprod. Biomed. Online 2015, 31, 30–38. [Google Scholar] [CrossRef]
- Kohil, A.; Chouliaras, S.; Alabduljabbar, S.; Lakshmanan, A.P.; Ahmed, S.H.; Awwad, J.; Terranegra, A. Female infertility and diet, is there a role for a personalized nutritional approach in assisted reproductive technologies? A Narrative Review. Front. Nutr. 2022, 9, 927972. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Lowe, G.D.; Rumley, A.; Bruckdorfer, K.R.; Whincup, P.H. Associations of vitamin C status, fruit and vegetable intakes, and markers of inflammation and hemostasis. Am. J. Clin. Nutr. 2006, 83, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Cyrus, A.; Kabir, A.; Goodarzi, D.; Moghimi, M. The effect of adjuvant vitamin C after varicocele surgery on sperm quality and quantity in infertile men: A double blind placebo controlled clinical trial. Int. Braz. J. Urol. 2015, 41, 230–238. [Google Scholar] [CrossRef]
- Aly, H.A.; El-Beshbishy, H.A.; Banjar, Z.M. Mitochondrial dysfunction induced impairment of spermatogenesis in LPS-treated rats: Modulatory role of lycopene. Eur. J. Pharmacol. 2011, 677, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Ricker, M.A.; Haas, W.C. Anti-Inflammatory Diet in Clinical Practice: A Review. Nutr. Clin. Pract. 2017, 32, 318–325. [Google Scholar] [CrossRef]
- Yahfoufi, N.; Alsadi, N.; Jambi, M.; Matar, C. The Immunomodulatory and Anti-Inflammatory Role of Polyphenols. Nutrients 2018, 10, 1618. [Google Scholar] [CrossRef]
- Montano, L.; Maugeri, A.; Volpe, M.G.; Micali, S.; Mirone, V.; Mantovani, A.; Navarra, M.; Piscopo, M. Mediterranean Diet as a Shield against Male Infertility and Cancer Risk Induced by Environmental Pollutants: A Focus on Flavonoids. Int. J. Mol. Sci. 2022, 23, 1568. [Google Scholar] [CrossRef]
- Liu, R.H. Health-Promoting Components of Fruits and Vegetables in the Diet. Adv. Nutr. Int. Rev. J. 2013, 4, 384S–392S. [Google Scholar] [CrossRef]
- Nassan, F.L.; Chavarro, J.E.; Tanrikut, C. Diet and men’s fertility: Does diet affect sperm quality? Fertil. Steril. 2018, 110, 570–577. [Google Scholar] [CrossRef]
- Grieger, J.A.; Grzeskowiak, L.E.; Bianco-Miotto, T.; Jankovic-Karasoulos, T.; Moran, L.J.; Wilson, R.L.; Leemaqz, S.Y.; Poston, L.; McCowan, L.; Kenny, L.C.; et al. Pre-pregnancy fast food and fruit intake is associated with time to pregnancy. Hum. Reprod. 2018, 33, 1063–1070. [Google Scholar] [CrossRef]
- Qu, Y.; Chen, S.; Pan, H.; Zhu, H.; Yan, C.; Zhang, S.; Jiang, Y. Risk factors of stillbirth in rural China: A national cohort study. Sci. Rep. 2019, 9, 365. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.; Melo, P.; Pickering, O.; Dhillon-Smith, R.; Coomarasamy, A.; Devall, A. The association between dietary patterns and risk of miscarriage: A systematic review and meta-analysis. Fertil. Steril. 2023, 120, 333–357. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Wu, J.; Xun, N. Role of maternal nutrition in the health outcomes of mothers and their children: A retrospective analysis. J. Pharmacol. Exp. Ther. 2019, 25, 4430–4437. [Google Scholar] [CrossRef] [PubMed]
- Amini, S.; Jafarirad, S.; Mohseni, H.; Ehsani, H.; Hejazi, L.; Feghhi, N. Comparison of food intake and body mass index before pregnancy between women with spontaneous abortion and women with successful pregnancy. IJOGI 2017, 20, 35–42. [Google Scholar] [CrossRef]
- Revonta, M.; Raitanen, J.; Sihvo, S.; Koponen, P.; Klemetti, R.; Männistö, S.; Luoto, R. Health and life style among infertile men and women. Sex. Reprod. Health 2010, 1, 91–98. [Google Scholar] [CrossRef]
- Chiu, Y.-H.; Williams, P.L.; Gillman, M.W.; Gaskins, A.J.; Mínguez-Alarcón, L.; Souter, I.; Toth, T.L.; Ford, J.B.; Hauser, R.; Chavarro, J.E.; et al. Association Between Pesticide Residue Intake From Consumption of Fruits and Vegetables and Pregnancy Outcomes Among Women Undergoing Infertility Treatment With Assisted Reproductive Technology. JAMA Intern. Med. 2018, 178, 17–26. [Google Scholar] [CrossRef]
- Halton, T.L.; Willett, W.C.; Liu, S.; Manson, J.E.; Stampfer, M.J.; Hu, F.B. Potato and french fry consumption and risk of type 2 diabetes in women. Am. J. Clin. Nutr. 2006, 83, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Malesza, I.J.; Malesza, M.; Walkowiak, J.; Mussin, N.; Walkowiak, D.; Aringazina, R.; Bartkowiak-Wieczorek, J.; Mądry, E. High-Fat, Western-Style Diet, Systemic Inflammation, and Gut Microbiota: A Narrative Review. Cells 2021, 10, 3164. [Google Scholar] [CrossRef] [PubMed]
- Cordain, L.; Eaton, S.B.; Sebastian, A.; Mann, N.; Lindeberg, S.; Watkins, B.A.; O’Keefe, J.H.; Brand-Miller, J. Origins and evolution of the Western diet: Health implications for the 21st century. Am. J. Clin. Nutr. 2005, 81, 341–354. [Google Scholar] [CrossRef] [PubMed]
- Skoracka, K.; Eder, P.; Łykowska-Szuber, L.; Dobrowolska, A.; Krela-Kaźmierczak, I. Diet and nutritional factors in male (in)fertility—Underestimated factors. J. Clin. Med. 2020, 9, 1400. [Google Scholar] [CrossRef] [PubMed]
- Silvestris, E.; de Pergola, G.; Rosania, R.; Loverro, G. Obesity as disruptor of the female fertility. Reprod. Biol. Endocrinol. 2018, 16, 22. [Google Scholar] [CrossRef] [PubMed]
- Psilopanagioti, A.; Papadaki, H.; Kranioti, E.F.; Alexandrides, T.K.; Varakis, J.N. Expression of adiponectin and adiponectin receptors in human pituitary gland and brain. Neuroendocrinology 2008, 89, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chua, S., Jr. Leptin Function and Regulation. Compr. Physiol. 2017, 8, 351–369. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, L.; Pereira, J.A.d.S.; Palhinha, L.; Moraes-Vieira, P.M.M. Leptin in the regulation of the immunometabolism of adipose tissue-macrophages. J. Leukoc. Biol. 2019, 106, 703–716. [Google Scholar] [CrossRef]
- Wu, X.; Tao, Y.; Ren, Y.; Zhang, Z.; Zhao, Y.; Tian, Y.; Li, Y.; Hou, M.; Guo, Y.; Gong, Y.; et al. Adiponectin inhibits GnRH secretion via activating AMPK and PI3K signaling pathways in chicken hypothalamic neuron cells. Poult. Sci. 2023, 102, 103028. [Google Scholar] [CrossRef]
- Limonta, P.; Marelli, M.M.; Moretti, R.; Marzagalli, M.; Fontana, F.; Maggi, R. GnRH in the Human Female Reproductive Axis. Vitam. Horm. 2018, 107, 27–66. [Google Scholar] [CrossRef]
- Brannian, J.D.; Zhao, Y.; McElroy, M. Leptin inhibits gonadotrophin-stimulated granulosa cell progesterone production by antagonizing insulin action. Hum. Reprod. 1999, 14, 1445–1448. [Google Scholar] [CrossRef]
- Bachir, B.G.; Jarvi, K. Infectious, inflammatory, and immunologic conditions resulting in male infertility. Urol. Clin. N. Am. 2014, 41, 67–81. [Google Scholar] [CrossRef]
- Chianese, R.; Pierantoni, R. Mitochondrial Reactive Oxygen Species (ROS) production alters sperm quality. Antioxidants 2021, 10, 92. [Google Scholar] [CrossRef]
- Ferramosca, A.; Provenzano, S.P.; Montagna, D.D.; Coppola, L.; Zara, V. Oxidative stress negatively affects human sperm mitochondrial respiration. Urology 2013, 82, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Daniels, J.L.; Bloomer, R.J.; van der Merwe, M.; Davis, S.L.; Buddington, K.K.; Buddington, R.K. Intestinal adaptations to a combination of different diets with and without endurance exercise. J. Int. Soc. Sports Nutr. 2016, 13, 35. [Google Scholar] [CrossRef] [PubMed]
- Saez, F.; Drevet, J.R. Dietary Cholesterol and Lipid Overload: Impact on Male Fertility. Oxidative Med. Cell. Longev. 2019, 2019, 4521786. [Google Scholar] [CrossRef]
- Mihalca, R.; Fica, S. The impact of obesity on the male reproductive axis. J. Med. Life 2014, 7, 296–300. [Google Scholar] [PubMed]
- Piomboni, P.; Focarelli, R.; Stendardi, A.; Ferramosca, A.; Zara, V. The role of mitochondria in energy production for human sperm motility. Int. J. Androl. 2011, 35, 109–124. [Google Scholar] [CrossRef]
- Yu, C.; Jiang, F.; Zhang, M.; Luo, D.; Shao, S.; Zhao, J.; Gao, L.; Zuo, C.; Guan, Q. HC diet inhibited testosterone synthesis by activating endoplasmic reticulum stress in testicular Leydig cells. J. Cell. Mol. Med. 2019, 23, 3140–3150. [Google Scholar] [CrossRef] [PubMed]
- Ferramosca, A.; Conte, A.; Moscatelli, N.; Zara, V. A high-fat diet negatively affects rat sperm mitochondrial respiration. Andrology 2016, 4, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Çekici, H.; Akdevelioğlu, Y. The association between trans fatty acids, infertility and fetal life: A review. Hum. Fertil. 2018, 22, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Jurczewska, J.; Szostak-Węgierek, D. The Influence of Diet on Ovulation Disorders in Women—A Narrative Review. Nutrients 2022, 14, 1556. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Manson, J.; Liu, S. Glycemic index, glycemic load, and risk of type 2 diabetes. Am. J. Clin. Nutr. 2002, 76, 274S–280S. [Google Scholar] [CrossRef] [PubMed]
- Lampiao, F.; Du Plessis, S.S. Insulin and leptin enhance human sperm motility, acrosome reaction and nitric oxide production. Asian J. Androl. 2008, 10, 799–807. [Google Scholar] [CrossRef]
- Plymate, S.R.; Matej, L.A. Inhibition of sex hormone-binding globulin production in the human hepatoma (Hep G2) cell line by insulin and prolactin. J. Clin. Endocrinol. Metab. 1988, 67, 460–464. [Google Scholar] [CrossRef]
- Zhao, J.; Zhai, L.; Liu, Z.; Wu, S.; Xu, L. Leptin level and oxidative stress contribute to obesity-induced low testosterone in murine testicular tissue. Oxidative Med. Cell. Longev. 2014, 2014, 190945. [Google Scholar] [CrossRef]
- Dias, T.R.; Alves, M.G.; Silva, B.M.; Oliveira, P.F. Sperm glucose transport and metabolism in diabetic individuals. Mol. Cell. Endocrinol. 2014, 396, 37–45. [Google Scholar] [CrossRef]
- Ferramosca, A.; Zara, V. Bioenergetics of mammalian sperm capacitation. BioMed Res. Int. 2014, 2014, 902953. [Google Scholar] [CrossRef]
- Xu, Y.; Qiao, J. Association of Insulin Resistance and Elevated Androgen Levels with Polycystic Ovarian Syndrome (PCOS): A Review of Literature. J. Health Eng. 2022, 2022, 9240569. [Google Scholar] [CrossRef]
- Poretsky, L.; Grigorescu, F.; Seibel, M.; Moses, A.C.; Flier, J.S. Distribution and characterization of insulin and insulin-like growth factor 1 receptors in normal human ovary. J. Clin. Endocrinol. Metab. 1985, 61, 728–734. [Google Scholar] [CrossRef]
- Escobar-Morreale, H.F.; Serrano-Gotarredona, J.; García-Robles, R.; Varela, C.; Sancho, J.M. Abnormalities in the serum insulin-like growth factor-1 axis in women with hyperandrogenism. Fertil. Steril. 1998, 70, 1090–1100. [Google Scholar] [CrossRef]
- Inversetti, A.; Zambella, E.; Guarano, A.; Dell’avanzo, M.; Di Simone, N. Endometrial Microbiota and Immune Tolerance in Pregnancy. Int. J. Mol. Sci. 2023, 24, 2995. [Google Scholar] [CrossRef]
- Hillier, S. Current concepts of the roles of follicle stimulating hormone and luteinizing hormone in folliculogenesis. Hum. Reprod. 1994, 9, 188–191. [Google Scholar] [CrossRef]
- Franks, S.; Robinson, S.; Willis, D. Nutrition, insulin and polycystic ovary syndrome. Rev. Reprod. 1996, 1, 47–53. [Google Scholar] [CrossRef]
- Ajuogu, P.K.; Al-Aqbi, M.A.; Hart, R.A.; Wolden, M.; Smart, N.A.; McFarlane, J.R. The effect of dietary protein intake on factors associated with male infertility: A systematic literature review and meta-analysis of animal clinical trials in rats. Nutr. Health 2020, 26, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Kemp, B.; Grooten, H.; Hartog, L.D.; Luiting, P.; Verstegen, M. The effect of a high protein intake on sperm production in boars at two semen collection frequencies. Anim. Reprod. Sci. 1988, 17, 103–113. [Google Scholar] [CrossRef]
- Holmes, M.D.; Pollak, M.N.; Willett, W.C.; Hankinson, S.E. Dietary correlates of plasma insulin-like growth factor I and insulin-like growth factor binding protein 3 concentrations. Cancer Epidemiol. Biomark. Prev. 2002, 11, 852–861. [Google Scholar] [PubMed]
- Zhang, B.; Zhou, W.; Shi, Y.; Zhang, J.; Cui, L.; Chen, Z.-J. Lifestyle and environmental contributions to ovulatory dysfunction in women of polycystic ovary syndrome. BMC Endocr. Disord. 2020, 20, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Chavarro, J.E.; Rich-Edwards, J.W.; Rosner, B.; Willett, W.C. A prospective study of dairy foods intake and anovulatory infertility. Hum. Reprod. 2007, 22, 1340–1347. [Google Scholar] [CrossRef]
- Musaiger, A.O. Diet and prevention of coronary heart disease in the Arab Middle East countries. Med. Princ. Pract. 2002, 11 (Suppl. S2), 9–16. [Google Scholar] [CrossRef]
- Badran, M.; Laher, I. Obesity in Arabic-Speaking Countries. J. Obes. 2011, 2011, 686430. [Google Scholar] [CrossRef]
- Samara, A.; Andersen, P.T.; Aro, A.R. Health Promotion and Obesity in the Arab Gulf States: Challenges and Good Practices. J. Obes. 2019, 2019, 4756260. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, M.M. Gestational Diabetes in the Arab Gulf Countries: Sitting on a Land-Mine. Int. J. Environ. Res. Public Health 2020, 17, 9270. [Google Scholar] [CrossRef] [PubMed]
- Mabry, R.; Koohsari, M.J.; Bull, F.; Owen, N. A systematic review of physical activity and sedentary behaviour research in the oil-producing countries of the Arabian Peninsula. BMC Public Health 2016, 16, 1003. [Google Scholar] [CrossRef] [PubMed]
- Kreidieh, D.; Itani, L.; El Kassas, G.; El Masri, D.; Calugi, S.; Grave, R.D.; El Ghoch, M.; Khreidieh, D. Long-term Lifestyle-modification Programs for Overweight and Obesity Management in the Arab States: Systematic Review and Meta-analysis. Curr. Diabetes Rev. 2018, 14, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Sharara, E.; Akik, C.; Ghattas, H.; Obermeyer, C.M. Physical inactivity, gender and culture in Arab countries: A systematic assessment of the literature. BMC Public Health 2018, 18, 639. [Google Scholar] [CrossRef] [PubMed]
- Benajiba, N.; Mahrous, L.; Janah, K.; Alqabbani, S.F.; Chavarria, E.A.; Aboul-Enein, B.H. Physical activity interventions promoted in the Arabic-speaking region: A review of the current literature. Obes. Rev. 2020, 21, e13032. [Google Scholar] [CrossRef]
- Tariq, M.N.M.; Stojanovska, L.; Al Dhaheri, A.S.; Ismail, L.C.; Apostolopoulos, V.; Ali, H.I. Lifestyle Interventions for Prevention and Management of Diet-Linked Non-Communicable Diseases among Adults in Arab Countries. Healthcare 2022, 11, 45. [Google Scholar] [CrossRef] [PubMed]
- Misra, A.; Singhal, N.; Khurana, L. Obesity, the metabolic syndrome, and type 2 diabetes in developing countries: Role of dietary fats and oils. J. Am. Coll. Nutr. 2010, 29, 289S–301S. [Google Scholar] [CrossRef]
- Popkin, B.M. Global nutrition dynamics: The world is shifting rapidly toward a diet linked with noncommunicable diseases. Am. J. Clin. Nutr. 2006, 84, 289–298. [Google Scholar] [CrossRef]
- Luo, Y.; Sun, L.; Wu, Q.; Song, B.; Wu, Y.; Yang, X.; Zhou, P.; Niu, Z.; Zheng, H.; Li, H.; et al. Diet-Related Lipidomic Signatures and Changed Type 2 Diabetes Risk in a Randomized Controlled Feeding Study With Mediterranean Diet and Traditional Chinese or Transitional Diets. Diabetes Care 2023, 46, 1691–1699. [Google Scholar] [CrossRef] [PubMed]
- Rai, S.K.; Gortmaker, S.L.; Hu, F.B.; Kanaya, A.M.; Kandula, N.R.; Sun, Q.; Bhupathiraju, S.N. A South Asian Mediterranean-style diet is associated with favorable adiposity measures and lower diabetes risk: The MASALA cohort. Obesity 2023, 31, 1697–1706. [Google Scholar] [CrossRef]
- Misra, A.; Khurana, L.; Isharwal, S.; Bhardwaj, S. South Asian diets and insulin resistance. Br. J. Nutr. 2008, 101, 465–473. [Google Scholar] [CrossRef]
- Garduño-Diaz, S.D.; Khokhar, S. South Asian dietary patterns and their association with risk factors for the metabolic syndrome. J. Hum. Nutr. Diet. 2012, 26, 145–155. [Google Scholar] [CrossRef]
- Ferreira, S.R.; Lerario, D.D.; Gimeno, S.G.; Sanudo, A.; Franco, L.J. Japanese-Brazilian Diabetes Study Group Obesity and central adiposity in Japanese immigrants: Role of the Western dietary pattern. J. Epidemiol. 2002, 12, 431–438. [Google Scholar] [CrossRef]
- Shimabukuro, M.; Higa, M.; Kinjo, R.; Yamakawa, K.; Tanaka, H.; Kozuka, C.; Yabiku, K.; Taira, S.-I.; Sata, M.; Masuzaki, H. Effects of the brown rice diet on visceral obesity and endothelial function: The BRAVO study. Br. J. Nutr. 2013, 111, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Krittanawong, C.; Tunhasiriwet, A.; Zhang, H.; Prokop, L.J.; Chirapongsathorn, S.; Sun, T.; Wang, Z. Is white rice consumption a risk for metabolic and cardiovascular outcomes? A systematic review and meta-analysis. Hearth Asia 2017, 9, e010909. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Paik, H.Y.; Song, W.O.; Song, Y. Metabolic syndrome risk factors are associated with white rice intake in Korean adolescent girls and boys. Br. J. Nutr. 2015, 113, 479–487. [Google Scholar] [CrossRef]
- Samimisedeh, P.; Afshar, E.J.; Ejtahed, H.; Qorbani, M. The impact of vegetarian diet on sperm quality, sex hormones levels and fertility: A systematic review and meta-analysis. J. Hum. Nutr. Diet. 2023, 37, 57–78. [Google Scholar] [CrossRef] [PubMed]
- Orzylowska, E.M.; Jacobson, J.D.; Bareh, G.M.; Ko, E.Y.; Corselli, J.U.; Chan, P.J. Food intake di-et and sperm characteristics in a blue zone: A Loma Linda Study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 203, 112–115. [Google Scholar] [CrossRef] [PubMed]
- Purkayastha, N.; Sharma, H. Prevalence and potential determinants of primary infertility in India: Evidence from Indian demographic health survey. Clin. Epidemiol. Glob. Health 2020, 9, 162–170. [Google Scholar] [CrossRef]
- West, M.C.L.; Anderson, L.; Mcclure, N.; Lewis, S.E.M. Dietary oestrogens and male fertility potential. Hum. Fertil. 2005, 8, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Kljajic, M.; Hammadeh, M.; Wagenpfeil, G.; Baus, S.; Sklavounos, P.; Solomayer, E.-F.; Kasoha, M. Impact of the vegan diet on sperm quality and sperm oxidative stress values: A prelim-inary study. J. Hum. Reprod. Sci. 2021, 14, 365. [Google Scholar] [CrossRef]
- Hilton, L. Unhealthy diet associated with poor semen quality. Urol. Times 2020, 48. Available online: https://www.urologytimes.com/view/unhealthy-diet-associated-poor-semen-quality (accessed on 14 January 2024).
- Berkow, S.E.; Barnard, N. Vegetarian diets and weight status. Nutr Res. 2006, 64, 175–188. [Google Scholar] [CrossRef]
- Freeman, J.M.; Kossoff, E.H.; Hartman, A.L. The ketogenic diet: One decade later. Pediatrics 2007, 119, 535–543. [Google Scholar] [CrossRef]
- Masucci, L.; D’ippolito, S.; De Maio, F.; Quaranta, G.; Mazzarella, R.; Bianco, D.M.; Castellani, R.; Inversetti, A.; Sanguinetti, M.; Gasbarrini, A.; et al. Celiac Disease Predisposition and Genital Tract Microbiota in Women Affected by Recurrent Pregnancy Loss. Nutrients 2023, 15, 221. [Google Scholar] [CrossRef]
- Gasior, M.; Rogawski, M.A.; Hartman, A.L. Neuroprotective and disease-modifying effects of the ketogenic diet. Behav. Pharmacol. 2006, 17, 431–439. [Google Scholar] [CrossRef]
- Mavropoulos, J.C.; Yancy, W.S.; Hepburn, J.; Westman, E.C. The effects of a low-carbohydrate, ketogenic diet on the polycystic ovary syndrome: A pilot study. Nutr. Metab. 2005, 2, 35. [Google Scholar] [CrossRef]
- Paoli, A.; Mancin, L.; Giacona, M.C.; Bianco, A.; Caprio, M. Effects of a ketogenic diet in overweight women with polycystic ovary syndrome. J. Transl. Med. 2020, 18, 104. [Google Scholar] [CrossRef]
- Cincione, R.I.; Losavio, F.; Ciolli, F.; Valenzano, A.; Cibelli, G.; Messina, G.; Polito, R. Effects of mixed of a ketogenic diet in overweight and obese women with polycystic ovary syndrome. Int. J. Environ. Res. Public Health 2021, 18, 12490. [Google Scholar] [CrossRef] [PubMed]
- Palafox-Gómez, C.; Ortiz, G.; Madrazo, I.; López-Bayghen, E. Adding a ketogenic dietary intervention to IVF treatment in patients with polycystic ovary syndrome improves implantation and pregnancy. Reprod. Toxicol. 2023, 119, 108420. [Google Scholar] [CrossRef] [PubMed]
- Hunter, J.E. Dietary trans fatty acids: Review of recent human studies and food industry responses. Lipids 2006, 41, 967–992. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.L.-Y.; Dunning, K.R.; Yang, X.; Russell, D.L.; Lane, M.; Norman, R.J.; Robker, R.L. High-fat diet causes lipotoxicity responses in cumulus-oocyte complexes and decreased fertilization rates. Endocrinology 2010, 151, 5438–5445. [Google Scholar] [CrossRef]
- Masood, W.; Annamaraju, P.; Khan Suheb, M.Z.; Uppaluri, K.R. Ketogenic Diet. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]


{kind=link}
| Mediterranean Diet | Western Diet | Arab Middle Eastern Diet | Asian Diet |
|---|---|---|---|
PUFA:
| SFA:
| SFA:
| SFA e TFA:
|
Carbohydrates:
| Carbohydrates:
| Carbohydrates:
| Carbohydrates:
|
Protein:
| Protein:
| ||
Micronutrients:
| Cholesterol:
| ||
Fruits & vegetables:
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cristodoro, M.; Zambella, E.; Fietta, I.; Inversetti, A.; Di Simone, N. Dietary Patterns and Fertility. Biology 2024, 13, 131. https://doi.org/10.3390/biology13020131
Cristodoro M, Zambella E, Fietta I, Inversetti A, Di Simone N. Dietary Patterns and Fertility. Biology. 2024; 13(2):131. https://doi.org/10.3390/biology13020131
Chicago/Turabian StyleCristodoro, Martina, Enrica Zambella, Ilaria Fietta, Annalisa Inversetti, and Nicoletta Di Simone. 2024. "Dietary Patterns and Fertility" Biology 13, no. 2: 131. https://doi.org/10.3390/biology13020131
APA StyleCristodoro, M., Zambella, E., Fietta, I., Inversetti, A., & Di Simone, N. (2024). Dietary Patterns and Fertility. Biology, 13(2), 131. https://doi.org/10.3390/biology13020131