
Obesity: Treatments, Conceptualizations, and Future Directions for a Growing Problem




{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. An Overview of Obesity Treatment Options and Their Inefficiency in Isolation as Individual Treatments for Obesity
2.1. Dieting
2.2. Exercise
2.3. Probiotic/Prebiotic Supplementation
2.4. Drugs
2.5. Bariatric Surgery
2.6. Behavioral Approaches
3. An Introspective Dilemma: Anti-Obesity Treatment Supplies Causing the Obesity Boom?
4. A Growing Problem: New Thoughts!
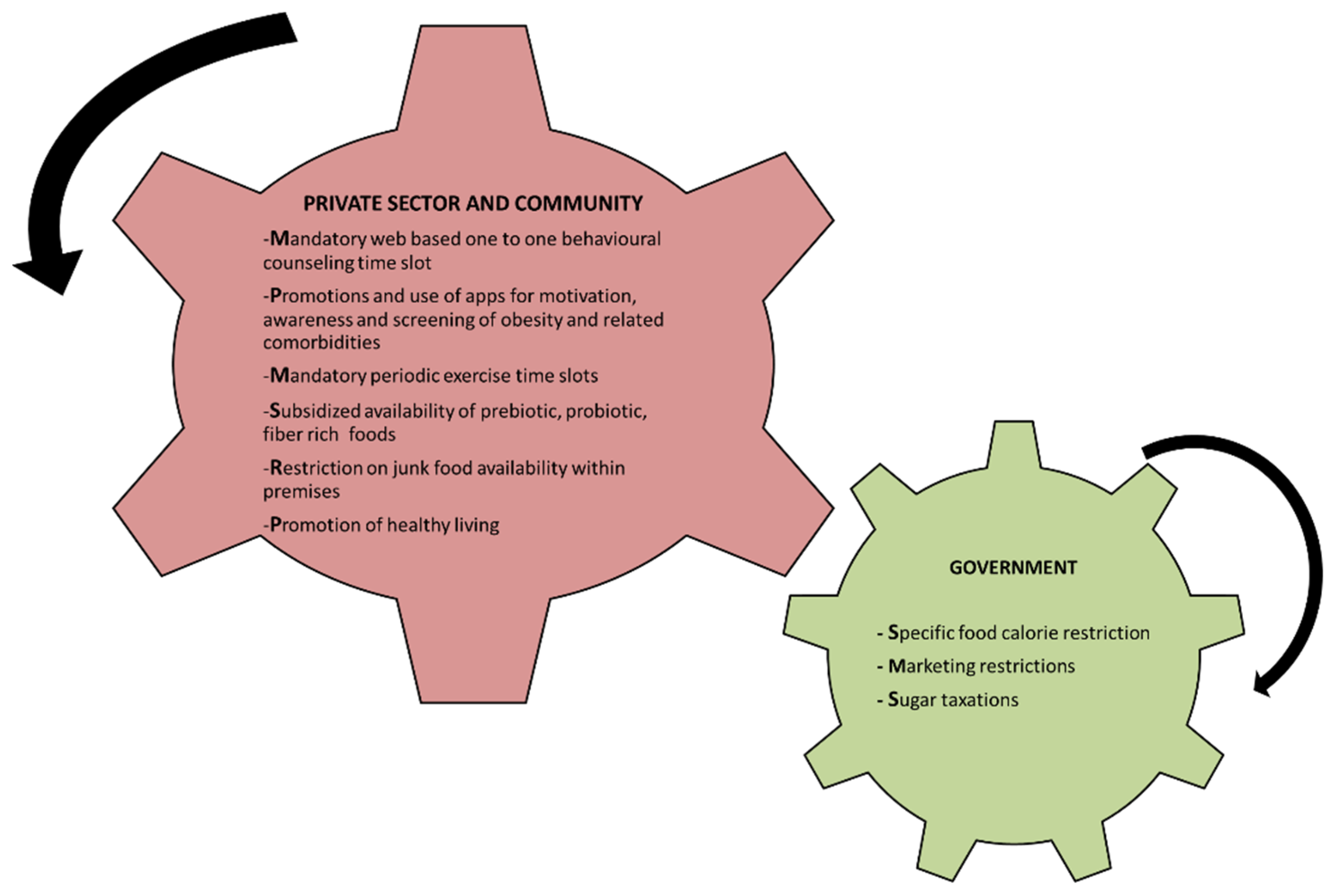
4.1. How Can the Private Sector and Community Contribute?
4.2. How Can the Government Contribute Further?
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fothergill, E.; Guo, J.; Howard, L.; Kerns, J.C.; Knuth, N.D.; Brychta, R.; Chen, K.; Skarulis, M.C.; Walter, M.; Walter, P.J.; et al. Persistent metabolic adaptation 6 years after “The Biggest Loser” competition. Obesity 2016, 24, 1612–1619. [Google Scholar] [CrossRef]
- Matarese, L.E. Diet and Obesity (Macronutrients, Micronutrients, Nutritional Biochemistry). In Metabolic Syndrome; Springer: Berling/Heidelberg, Germany, 2015; pp. 1–15. [Google Scholar] [CrossRef]
- Feinman, R.D.; Pogozelski, W.K.; Astrup, A.; Bernstein, R.K.; Fine, E.J.; Westman, E.C.; Accurso, A.; Frassetto, L.; Gower, B.A.; McFarlane, S.I.; et al. Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base. Nutrition 2015, 31, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebbeling, C.B.; Swain, J.F.; Feldman, H.A.; Wong, W.W.; Hachey, D.L.; Garcia-Lago, E.; Ludwig, D.S. Effects of Dietary Composition on Energy Expenditure During Weight-Loss Maintenance. JAMA 2012, 307, 2627–2634. [Google Scholar] [CrossRef] [Green Version]
- St-Onge, M.-P.; Ard, J.; Baskin, M.L.; Chiuve, S.E.; Johnson, H.M.; Kris-Etherton, P.; Varady, K.; on behalf of the American Heart Association Obesity Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular Disease in the Young; Council on Clinical Cardiology; et al. Meal Timing and Frequency: Implications for Cardiovascular Disease Prevention: A Scientific Statement From the American Heart Association. Circulation 2017, 135, e96–e121. [Google Scholar] [CrossRef]
- De Cabo, R.; Mattson, M.P. Effects of intermittent fasting on health, aging, and disease. N. Engl. J. Med. 2019, 381, 2541–2551. [Google Scholar] [CrossRef] [PubMed]
- Bahr, L.S.; Franz, K.; Mähler, A. Assessing the (anti)-inflammatory potential of diets. Curr. Opin. Clin. Nutr. Metab. Care 2021, 24, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, C.; Depres, J.-P.; Tremblay, A. Exercise and Obesity. Obes. Res. 1993, 1, 133–147. [Google Scholar] [CrossRef] [PubMed]
- Slentz, C.A.; Aiken, L.B.; Houmard, J.A.; Bales, C.W.; Johnson, J.L.; Tanner, C.J.; Duscha, B.D.; Kraus, W.E. Inactivity, exercise, and visceral fat. STRRIDE: A randomized, controlled study of exercise intensity and amount. J. Appl. Physiol. 2005, 99, 1613–1618. [Google Scholar] [CrossRef] [Green Version]
- Vettor, R.; Di Vincenzo, A.; Maffei, P.; Rossato, M. Regulation of energy intake and mechanisms of metabolic adaptation or maladaptation after caloric restriction. Rev. Endocr. Metab. Disord. 2020, 21, 399–409. [Google Scholar] [CrossRef]
- Friedman, M.I.; Appel, S. Energy expenditure and body composition changes after an isocaloric ketogenic diet in overweight and obese men: A secondary analysis of energy expenditure and physical activity. PLoS ONE 2019, 14, e0222971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerdó, T.; García-Santos, J.A.; Bermúdez, M.G.; Campoy, C. The Role of Probiotics and Prebiotics in the Prevention and Treatment of Obesity. Nutrients 2019, 11, 635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NIH. Prescription Medications to Treat Overweight & Obesity. 2021. Available online: https://www.niddk.nih.gov/health-information/weight-management/prescription-medications-treat-overweight-obesity (accessed on 19 October 2021).
- Wilding, J.P.H.; Batterham, R.L.; Calanna, S.; Davies, M.; Van Gaal, L.F.; Lingvay, I.; McGowan, B.M.; Rosenstock, J.; Tran, M.T.; Wadden, T.A.; et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N. Engl. J. Med. 2021, 384, 989–1002. [Google Scholar] [CrossRef] [PubMed]
- Lupoli, R.; Lembo, E.; Saldalamacchia, G.; Avola, C.K.; Angrisani, L.; Capaldo, B. Bariatric surgery and long-term nutritional issues. World J. Diabetes 2017, 8, 464–474. [Google Scholar] [CrossRef] [PubMed]
- Endocrine News. Unforeseen Consequences: Bariatric Surgery Side Effects. 2018. Available online: https://endocrinenews.endocrine.org/unforeseen-consequences-bariatric-surgery-side-effects/ (accessed on 19 October 2021).
- Sogg, S.; Lauretti, J.; West-Smith, L. Recommendations for the presurgical psychosocial evaluation of bariatric surgery patients. Surg. Obes. Relat. Dis. 2016, 12, 731–749. [Google Scholar] [CrossRef]
- The Weight Control and Diabetes Research Center. Rationale and Design for a Pragmatic Effectiveness-Implementation Trial of Online Behavioral Obesity Treatment in Primary Care. 2019. Available online: http://weightresearch.org/ (accessed on 18 October 2021).
- Olson, K.; Bond, D.; Wing, R.R. Behavioral Approaches to the Treatment of Obesity. Rhode Island Med. J. 2017, 21–24. [Google Scholar]
- Thomas, J.G.; Bond, D.S. Review of Innovations in Digital Health Technology to Promote Weight Control. Curr. Diabetes Rep. 2014, 14, 485. [Google Scholar] [CrossRef] [PubMed]
- Forman, E.M.; Manasse, S.M.; Butryn, M.L.; Crosby, R.D.; Dallal, D.H.; Crochiere, R.J. Long-Term Follow-up of the Mind Your Health Project: Acceptance-Based versus Standard Behavioral Treatment for Obesity. Obesity 2019, 27, 565–571. [Google Scholar] [CrossRef] [PubMed]
- World Obesity Federation. Calculating the Costs of the Consequences of Obesity. 2017. Available online: https://www.worldobesity.org/resources/resource-library/calculating-the-costs-of-the-consequences-of-obesity (accessed on 18 October 2021).
- Yarborough, C.M.; Brethauer, S.; Burton, W.N.; Fabius, R.J.; Hymel, P.; Kothari, S.; Kushner, R.F.; Morton, J.M.; Mueller, K.; Pronk, N.P.; et al. Obesity in the Workplace. J. Occup. Environ. Med. 2018, 60, 97–107. [Google Scholar] [CrossRef]
- Bajorek, Z.; Bevan, S. Obesity and Work: Challenging Stigma and Discrimination; Report 526; Institute for Employment Studies: Brighton, UK, 2019; Available online: https://www.employment-studies.co.uk/system/files/resources/files/526.pdf (accessed on 19 December 2021).
- Barber, J.; Hillier, S.E.; Middleton, G.; Keegan, R.; Henderson, H.; Lavin, J. Providing weight management via the workplace. Int. J. Work. Health Manag. 2015, 8, 230–243. [Google Scholar] [CrossRef] [Green Version]
- Suojanen, L.-U.; Ahola, A.; Kupila, S.; Korpela, R.; Pietiläinen, K. Effectiveness of a web-based real-life weight management program: Study design, methods, and participants’ baseline characteristics. Contemp. Clin. Trials Commun. 2020, 19, 100638. [Google Scholar] [CrossRef] [PubMed]
- Marmett, B.; Carvalho, R.B.; Fortes, M.S.; Cazella, S.C. Artificial Intelligence technologies to manage obesity. Vittalle Rev. Cienc. Saude 2018, 30, 73–79. [Google Scholar] [CrossRef]
- Leeds Beckett University. What Are the Government Doing to Tackle Obesity? 2019. Available online: https://www.leedsbeckett.ac.uk/blogs/expert-opinion/2019/01/0118-obesity-awareness-week-whole-systems/ (accessed on 25 October 2021).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baker, J.S.; Supriya, R.; Dutheil, F.; Gao, Y. Obesity: Treatments, Conceptualizations, and Future Directions for a Growing Problem. Biology 2022, 11, 160. https://doi.org/10.3390/biology11020160
Baker JS, Supriya R, Dutheil F, Gao Y. Obesity: Treatments, Conceptualizations, and Future Directions for a Growing Problem. Biology. 2022; 11(2):160. https://doi.org/10.3390/biology11020160
Chicago/Turabian StyleBaker, Julien S., Rashmi Supriya, Frédéric Dutheil, and Yang Gao. 2022. "Obesity: Treatments, Conceptualizations, and Future Directions for a Growing Problem" Biology 11, no. 2: 160. https://doi.org/10.3390/biology11020160
APA StyleBaker, J. S., Supriya, R., Dutheil, F., & Gao, Y. (2022). Obesity: Treatments, Conceptualizations, and Future Directions for a Growing Problem. Biology, 11(2), 160. https://doi.org/10.3390/biology11020160